ABSTRACT
OBJECTIVES: to analyze the magnitude and temporal distribution of congenital syphilis, according to sociodemographic characteristics and prenatal care in the three most populous municipalities of Baixada Fluminense-RJ (2015-2024).
METHODS: ecological time series study. Data from the Notifiable Diseases Information System and the Live Birth Information System. Incidences and temporal trends were calculated considering sociodemographic and prenatal variables. For temporal analysis, the Joinpoint Regression program was used.
RESULTS: 8961 cases of congenital syphilis were registered. Belford Roxo presented the highest incidence, reaching 28.5/1,000 LB in 2024, followed by Duque de Caxias -24.1, and Nova Iguaçu - 9.7, with stagnation in the rates in the first and growth in the last two, from 2015 to 2021, with a reduction in recent years, without reversing the magnitude of disease. COVID-19 pandemics altered trends, with joinpoints in 2021. Inequalities in the magnitude and trend of CS were identified, with higher incidences and stability/increase among adolescents, brown women, and those with low education. Women who did not undergo prenatal care had higher incidences, stable or increasing.
CONCLUSION: the incidences of CS were high, uneven and predominantly stationary or increasing, especially in more vulnerable groups. It is necessary to offer more equitable and qualified prenatal care in these municipalities.
Keywords:
Congenital syphilis, Measuring health inequalities, Prenatal care, Health information systems, Time series studies
RESUMO
OBJETIVOS: analisar a magnitude e distribuição temporal da sífilis congênita, segundo características sociodemográficas e pré-natal, nos três municípios mais populosos da Baixada Fluminense do RJ (2015-2024).
MÉTODOS: estudo ecológico de série temporal. Dados do Sistema de Informação de Agravos de Notificação e do Sistema de Informações sobre Nascidos Vivos. Incidências e tendência temporal foram calculadas considerando variáveis sociodemográficas e pré-natal. Para análise temporal, utilizou-se o programa Joinpoint Regression.
RESULTADOS: registraram-se 8961 casos de sífilis congênita. Belford Roxo apresentou a maior incidência, atingindo em 2024, 28,5/1000 NV, seguido por Duque de Caxias - 24,1, e Nova Iguaçu - 9,7, com estagnação das taxas no primeiro e crescimento nos dois últimos municípios, de 2015 a 2021, com redução nos últimos anos, sem reversão da magnitude do agravo. Observou-se influência da pandemia de COVID-19, com pontos de inflexão em 2021. Identificaram-se desigualdades na magnitude e tendência da sífilis congênita, predominando maiores incidências e estabilidade e/ou crescimento entre adolescentes, pardas e com baixa escolaridade. Mulheres que não realizaram pré-natal apresentaram incidências mais elevadas, estacionárias ou crescentes.
CONCLUSÃO: as incidências de sífilis congênita se mostraram elevadas, desiguais e predominantemente estacionárias ou crescentes, principalmente em grupos mais vulneráveis. É necessário oferecer um pré-natal mais equânime e qualificado nesses municípios.
Palavras-chave:
Sífilis congênita, Mensuração das desigualdades em saúde, Cuidado pré-natal, Sistemas de informação em saúde, Estudos de séries temporais
IntroductionSyphilis is a systemic, chronic and curable bacterial infection exclusive to humans, which remains a major public health problem in Brazil and globally.
1,2 Placental transmission may occur at any point during pregnancy or at any clinical stage of pregnant women who have been inadequately treated. Congenital syphilis (CS) is a significant cause of morbimortality, particularly in infants under one year of age,
2 and serves as a sentinel event for the quality of the prenatal care.
1-3CS is a recurrent target of public policies in Brazil.
3 However, the country is still far from the goal proposed by the World Health Organization (WHO), of ≤0.5 cases per 1,000 live births (LB).
3In 2023, Brazil's incidence reached 9.9 per 1,000 LB, 20 times the recommended rate.
1 In the same year, 25,002 cases of congenital syphilis were recorded. The state of Rio de Janeiro (ERJ – Portuguese acronym) had the highest incidence at 18.5 per 1,000 LB, followed by the states of Tocantins, Roraima and Espírito Santo.
1In the ERJ, the highest incidences are observed in the Metropolitan Region I, which, in addition to the capital city, encompasses peripheral municipalities with diverse population profiles.
4 In this region, studies focusing on the capital city, Rio de Janeiro, are particularly common. They show high and increasing CS rates, reaching an incidence of 18.6 per 1,000 live births in 2020.
5 The most affected population is one with higher social vulnerabilities (black and adolescent women with low educational attainment and who did not receive prenatal care). There is a geographic concentration in the central, suburban North and West areas of the city, which have worse life conditions.
5,6In the Metropolitan Region II, São Gonçalo, the second most populous municipality in the ERJ, showed increasing rates between 2010 and 2018, reaching 41.6 per 1,000 LB in 2018.
7 And Niterói, a municipality with the 7
th highest Municipal Human Development Index (MHDI) in the country, also had an increasing trend of the problem (16% per year), reaching 23.2 cases per 1,000 live births in 2016.
8Some recent studies have evaluated the evolution of CS with time-series analysis, both at the local and national levels.
7-10 All of them show an increasing trend in the problem, with differences in magnitude. No population-based articles on CS were found in municipalities of the
Baixada Fluminense, which is located in the peripheral area of the ERJ's Metropolitan Region I and has a large population.
This study aims to describe the magnitude and the epidemiological characteristics of CS and to analyze its temporal distribution by sociodemographic and prenatal care characteristics in the three most populous municipalities of the
Baixada Fluminense.
MethodsThis was an ecological time-series study. The study population was from the three municipalities that accounts for 58% of the
Baixada Fluminense population, according to the 2022 Census (Guapimirim, Magé, Duque de Caxias, Nova Iguaçu, São João de Meriti, Nilópolis, Belford Roxo, Mesquita, Queimados, Japeri, Paracambi, Seropédica e Itaguaí). The municipality of Duque de Caixias has 808,152 inhabitants and a 0.711 MHDI. Nova Iguaçu, in turn, has 785,882 inhabitants and a 0.713 MHDI. Finally, Belford Roxo has 483,087 inhabitants and a 0.684 MHDI.
11 According to the e-management platform for basic care (BS) of the Secretariat of Primary Health Care, Ministry of Health, BC coverage in 2020 corresponded to 45.4%, 69.5% and 32.1%, respectively.
12We used secondary data related on confirmed cases of CS, from 2015 to 2024, sourced from the Notifiable Diseases Information System (SINAN – Portuguese acronym), which was accessed through the website of the Rio de Janeiro State Health Secretariat.
13 SINAN is a universal system that compiles and processes information from notification/investigation forms across the country.
For the population-based calculation, the source was the Live Births Information System (SINASC – Portuguese acronym).
13 This information system, universal as well, is fed by the live birth statements (DN – Portuguese acronym).
For the calculation of CS incidence, we used the number of new cases confirmed annually, divided by the number of live births in the same year, and multiplied by 1,000. Rates were calculated globally, according to the sociodemographic variables. The analyzed variables, from SINAN and SINASC, were: maternal age, categorized into adolescents (up to 19 years), 20 to 34 years and 35 years or more; maternal schooling, categorized into low (less than eight years of schooling), medium (eight to 11 years) and high (12 years or more); skin color/race, categorized according to the DN and CS notification form fields into White, Black, Yellow, Brown and Indigenous; prenatal care, categorized dichotomously (performed or not).
Additionally, relative frequencies of the clinic variables of the notification form were described as follows: timing of diagnosis (during prenatal care, at delivery or D&C, after childbirth or not performed); maternal treatment (adequate, inadequate or not performed); partner's treatment (yes or no).
The temporal trend analysis was conducted for each municipality and stratified by age group, educational attainment, and color/race of mothers and prenatal care attendance, using the abovementioned strata. The Joinpoint Regression software (National Cancer Institute, Bethesda, Maryland, USA), version 5.3.3.0.0 was used, which allows for the adjustment of a series of trend lines and its joinpoints on a logarithmic scale.
14 A joinpoint is identified when the direction of the trend is inverted or there are different trend patterns, and therefore, the periods are analyzed separately. In the absence of a variation, the entire period is analyzed. For these identified periods, annual percent changes (APC) are estimated and tested, and their respective 95% confidence intervals (95% CI) are determined. The significance test used is the Monte Carlo Permutation Method.
14This study is part of the project "
Desigualdades nos indicadores de saúde da mulher e da criança no Estado do Rio de Janeiro", approved by the Research Ethics Committee (CEP- Portuguese acronym) of the Fluminense Federal University Faculty of Medicine, under approval number 6.592.723, from December 19, 2023.
ResultsBetween 2015 and 2024, 8,961 cases of congenital syphilis were recorded in the three municipalities, with Nova Iguaçu having the highest absolute number (Table 1). Maternal characteristics were similar: 23-27% adolescents, more than 30% had low educational attainment, there was a predominance of Brown race/color and a high rate of prenatal care attendance (>70%). However, less than half received diagnosis at pregnancy, especially Nova Iguaçu (31.3%). Adequate treatment was reported in less than 7% of pregnant women, and partner's treatment, in less than 12%.
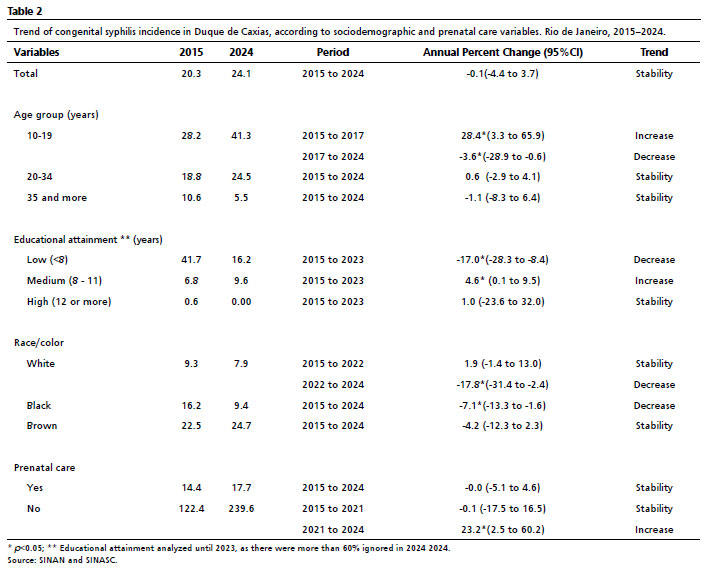
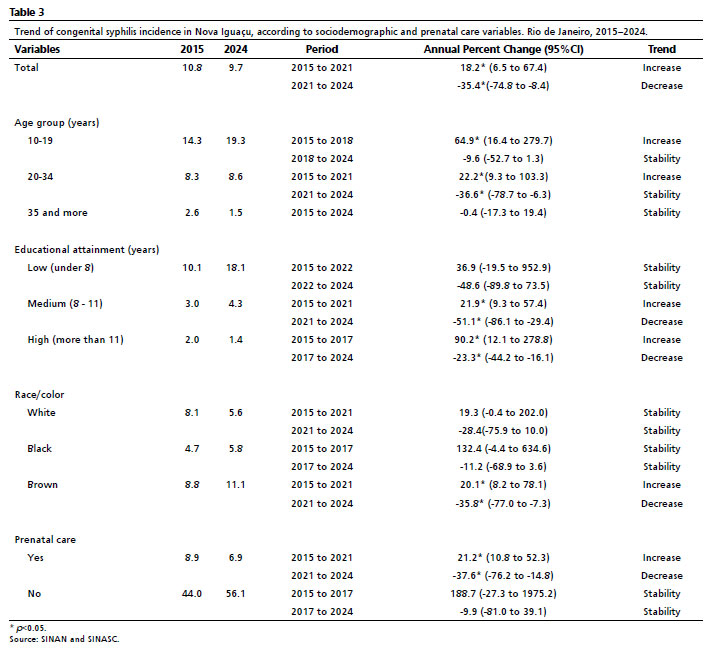
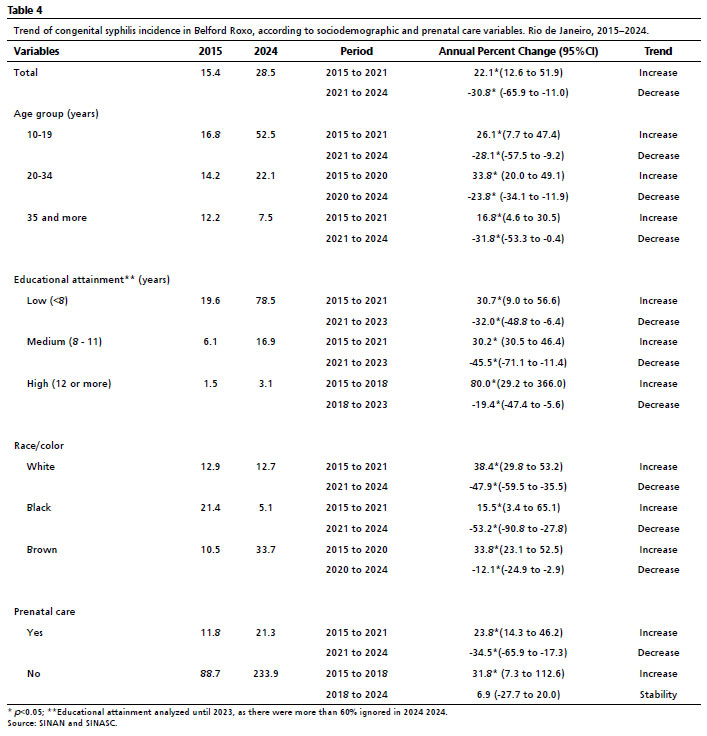
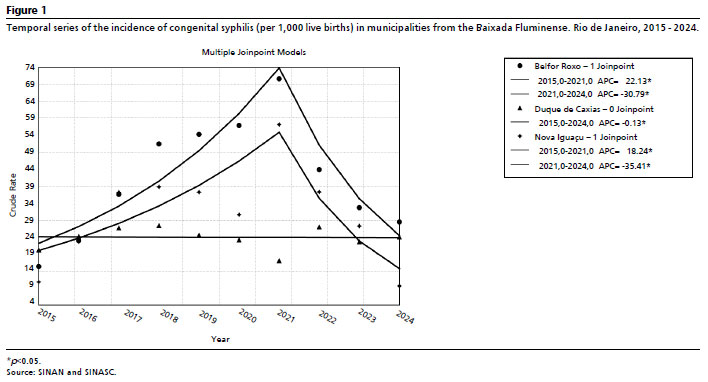
The rates of CS varied from 20.3 to 24.1 per 1,000 LB in Duque de Caxias (stability). Belford Roxo and Nova Iguaçu showed a different pattern: the rates increased from 15.4 to 28.5 per 1,000 LB and from 10.8 to 9.7 per 1,000 LB, respectively, both with a subsequent decrease after 2021. (Tables 2, 3 and 4; Figure 1).
As taxas de SC variaram de 20,3 a 24,1/1.000 NV em Duque de Caxias (estabilidade); de 15,4 a 28,5/1.000 NV em Belford Roxo e de 10,8 a 9,7/1.000 NV em Nova Iguaçu, ambos com aumento até 2021 e queda subsequente (Tabelas 2, 3 e 4; Figura 1).
In all municipalities, adolescents had the lowest rates, showing an initial increasing trend followed by a subsequent decrease or stabilization. Women aged 20-34 years showed a similar pattern in Belford Roxo and Nova Iguaçu. For women aged ≥35 years, an increase was observed only in Belford Roxo, until 2021.
The highest rates of CS were observed in mothers with low educational attainment. From 2015 to 2023, a decrease was observed in Duque de Caxias, stability in Nova Iguaçu and an increase with subsequent decrease in Belford Roxo. The mean "educational attainment" had an increasing trend in the three municipalities until 2021, with subsequent decrease. Women with high educational attainment maintained very low rates.
Regarding race/color, the highest rates were concentrated among Black and Brown women, with some exceptions. White women had a decrease in Duque de Caxias (2022-2024), stability in Nova Iguaçu and an increase followed by a subsequent decrease in Belford Roxo. Black women had a continuous decrease in Duque de Caxias, stability in Nova Iguaçu and a variation in Belford Roxo. Brown women had stability in Duque de Caxias and an increasing pattern until 2020/2021, followed by a decrease in the other municipalities.
Pregnant women who did not receive prenatal care had very higher rates of CS (above 200 per 1,000 LB in some years), with a recent increasing trend in Duque de Caxias and Belford Roxo and stability in Nova Iguaçu. Among those who had prenatal care, an increase with subsequent decrease was observed in Belford Roxo and Nova Iguaçu until 2021, and stability was observed in Duque de Caxias.
DiscussionThe present study found that in the three largest municipalities of
Baixada Fluminense, CS had elevated and unequal rates, with increasing and stationary trends being predominant. Although a decreasing trend was observed in Belford Roxo and Nova Iguaçu from 2021 to 2024, it was not enough to reverse the magnitude of the health issue.
The rates of Belford Roxo and Duque de Caxias in 2024 were higher than those observed in the municipality of Rio de Janeiro,
5 all from the Metropolitan Region 1 of the state of Rio de Janeiro. These rates also were higher than those observed in Niterói, in Metropolitan Region 2.
8 The three analyzed municipalities encompassed 20% of cases of CS in the state, in 2024.
According to the Brazil Social Progress Index 2025, which analyzes comprehensive indicators of quality of life, Belford Roxo and Duque de Caxias had the second and the third lowest scores, respectively, among Brazilian municipalities with more than 500,000 inhabitants. Among the indicators with lowest scores are health care and educational attainment, which highlights the social and health access vulnerabilities of these municipalities.
15Adolescents had higher rates than other age groups in the three cities, with a predominantly increasing trend. The elevated rates and the increase in this group can be explained by a sum of factors. The National Survey of School Health (PeNSE – Portuguese acronym) recorded a reduction in condom use from 72.55% for 59% in the period from 2009 to 2019.
16 This increased the risk of early pregnancy and sexually transmittable infections; with a particular emphasis on acquired syphilis, which is rising in Brazil, including among individuals aged 13 to 19.
1 Another contributing factor is access and use of prenatal care. Despite an increasing trend of attending seven or more prenatal consultations in both Brazil and the state of Rio de Janeiro,
17 the proportion of inadequate prenatal care is higher among adolescents. This inadequacy is particularly pronounced among those with lower educational attainment, with Black or Brown race/color and of low socioeconomic status.
18-20For the group of women of low educational attainment, with higher rates in the entire period, the exception was Duque de Caxias, where a decrease of the problem was recorded; in the other municipalities, the rates were stationary or decreased. It is known that this group is vulnerable for both inadequate prenatal care,
19,20 and sexually transmitted infections, notably syphilis.
21 High and/or increasing rates of congenital syphilis for this vulnerable group were also reported at national level,
9,10 and in other regions of the state of Rio de Janeiro.
7,8Regarding the variable maternal race/color, the results of this study confirmed the relationship between CS and the situation of social vulnerability in which Black and Brown mothers and their children are situated.
22 In the three analyzed municipalities, in 2024, the highest incidences were observed in Brown women and, only in Belford Roxo, White women had higher rates than Black women. This pattern was similar to those of studies focused on the Brazilian population,
9,22 and on other municipalities of the Rio de Janeiro Metropolitan Area, such as Niterói, São Gonçalo and the city of Rio de Janeiro.
5-8The persistence of CS reveals flaws in the healthcare network and low quality of prenatal care.
3,23 In the municipalities of
Baixada Fluminense, about 75% of women with CS had prenatal care, although the diagnosis and treatment were mostly inadequate. Flaws in prenatal care associated with high rates of CS were observed in national studies.
9,10 Similarly, data from international studies show that 88% of pregnant women had at least one prenatal consultation, but among mothers with syphilis, only 51% were adequately treated.
2Low educational attainment, low income and adolescent pregnancy are among inequalities that accumulate during prenatal care and contribute to inadequate treatment for pregnant women.
18-20 According to performance indicators from
Previne Brasil 2022, Duque de Caxias, Nova Iguaçu e Belford Roxo had, respectively, 21%, 55% and 3.0% of pregnant women tested for syphilis and HIV in the third four-month period of 2022. All of these values are below the 60% target and significantly distant from the goal recommended by the WHO and ratified by the national agreement for the elimination of vertical transmitted diseases, which states that at least 95% of pregnant women should be tested for syphilis during prenatal care.
24,25The partner's treatment is extremely important for preventing reinfections of pregnant women.
2 A study in Porto Alegre showed that the absence of treatment by partners had a statistically significant association with incidence of CS, as well as with perinatal and neonatal death outcomes.
26 In the present study, we observed that only 11% of notified CS cases had treated partners. This reinforces the need to engage partners during prenatal care for a more effective fight against syphilis and other sexually transmittable diseases. In adolescents, the difficulties in providing care to partners may be even higher, representing an additional factor to the high rates for this age group.
27Regardless of age, removing the variable "partner's treatment" as a criterion for adequate treatment for pregnant women is contradictory, as the non-treatment or inadequate treatment of partners increases the probability of reinfection and fails to interrupt the syphilis chain of infection.
26,27In Belford Roxo, a municipality with the worst indicators analyzed, we observed that the majority of variables with an increasing trend showed a joinpoint in 2021, suggesting a potential influence of the COVID-19 pandemic. It is known that health services were significantly affected in 2020 and 2021, impairing the control of diverse infectious diseases, including syphilis.
28 In a context of high socioeconomic vulnerability, such as observed in Belford Roxo, this scenario may have contributed to the increase of CS cases. This hypothesis is reinforced by national studies that identify an association between low MHDI and higher incidence of the disease.
29 It is, however, imperative to analyze the variations in prenatal care coverage, as well as other relevant factors, across the pre-pandemic and pandemic periods, in order to corroborate this hypothesis.
A recent assessment regarding gestational and congenital syphilis showed that SINAN continues to have completeness issues, particularly concerning sociodemographic variables and partner's treatment, though it has shown improvement in recent years.
30This study faced limitations stemming from data incompleteness, notably in maternal sociodemographic variables and partner treatment data, as evidenced by high percentages of missing fields. These issues are consistent with findings in other municipalities and at the national level. Furthermore, the underreporting of congenital syphilis and the reliance of secondary data precluded a more in-depth analysis of local of health management strategies.
Ultimately, sociodemographic vulnerability was revealed to be a relevant factor for the occurrence and increase of CS in the
Baixada Fluminense, aggravated by flaws in diagnosis and treatment. Analyses from other national studies reinforce the intersectionality of race, educational attainment, and age in the development of health inequities, with a focus on maternal and child health outcomes.
10,22 In the case of CS, social determinants impact as early as the acquisition of the infection, which is more frequent in Black or Brown women, and those with low educational attainment.
21,22 Access to adequate prenatal care, which would prevent vertical transmission, is likewise influenced by sociodemographic variables. Adolescents, Black or Brown women, and those with low educational attainment tend to have fewer consultations, undergo fewer syphilis tests, receive fewer diagnoses during prenatal care, and are provided less adequate treatment for themselves and their partners.
3,19,20,22Public policies to combat CS are already in place, and the country has a robust healthcare system.
3 At the local management level, municipalities have implemented some action, such as the use rapid syphilis tests in primary healthcare units and professional training.
4 However, these measures proved to be insufficient in the
Baixada Fluminense, as the incidence of CS remained high or stable even among pregnant women with access to prenatal care. Other measures are a priority, such as valuing the topic in medical curricula, providing ongoing education for healthcare professionals on the diagnosis and treatment of the condition, and developing strategies for the appropriate management and treatment of partners.
3,23,29 The mandatory collection of partner information could be reincorporated into disease surveillance.
23We highlight the need to strengthen primary healthcare,
3 along with providing strategic guidance for preventive actions targeted at young Black and Brown women with low educational attainment in municipalities located in the metropolitan peripheries.
Therefore, for the
Baixada Fluminense, it is crucial to guarantee more equitable and qualified prenatal care, with timely diagnosis and adequate treatment, in addition to mitigating social inequalities. This last measure has a broad perspective, which depends on intersectoral collaboration and civil society engagement. For syphilis and other socially determined diseases, only effective changes in income distribution and healthcare financing can ensure the elimination of these conditions.
References1. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde e Ambiente. Boletim Epidemiológico. Número Especial. Outubro 2024. Sífilis. Brasília (DF): Ministério da Saúde; 2024. [access in 2025 Abr 18]. Available from:
https://www.gov.br/aids/pt-br/central-de-conteudo/boletins-epidemiologicos/2024/boletim_sifilis_2024_e.pdf/view2. Korenromp EL, Rowley J, Alonso M, Mello MB, Wijesooriya NS, Mahiané SG,
et al. Global burden of maternal and congenital syphilis and associated adverse birth outcomes—Estimates for 2016 and progress since 2012. PLoS ONE 2019; 14 (2): e0211720.
3. Miranda AE, Santos PC, Coelho RA, Pascom ARP, de Lannoy LH, Ferreira ACG,
et al. Perspectives and challenges for mother-to-child transmission of HIV, hepatitis B, and syphilis in Brazil. Front Public Health. 2023; 11: 1182386.
4. Secretaria de Saúde do Estado do Rio de Janeiro. Boletim de análise de situação de saúde - Sífilis | Rio de Janeiro; Governo do Estado do Rio de Janeiro; out.2024. [access in 2025 Abr 18]. Available from:
https://sistemas.saude.rj.gov.br/tabnetbd/docs/boletins/BASIS0304.pdf5. Paiva MFCM, Fonseca SC. Sífilis congênita no Município do Rio de Janeiro, 2016-2020: perfil epidemiológico e completude dos registros. Medicina (Ribeirão Preto). 2023; 56 (1): e-198451.
6. Reis GJ, Barcellos C, Pedroso MM, Xavier DR. Diferenciais intraurbanos da sífilis congênita: análise preditiva por bairros do Município do Rio de Janeiro, Brasil. Cad Saúde Pública. 2018; 34 (9): e00105517.
7. Morais LS de, Pimentel SVT, Kawa H, Fonseca SC. Temporal trend of congenital syphilis in the most populous municipality of metropolitan region II of Rio de Janeiro state. Rev Paul Pediatr. 2023; 41: e2021337.
8. Heringer ALS, Kawa H, Fonseca SC, Brignol SMS, Zarpellon LA, Reis AC. Desigualdades na tendência da sífilis congênita no município de Niterói, Brasil, 2007 a 2016. Rev Panam Salud Pública. 2020; 44: e8.
9. Silva AAO, Leony LM, Souza WV, Freitas NEM, Daltro RT, Santos EF,
et al. Spatiotemporal distribution analysis of syphilis in Brazil: Cases of congenital and syphilis in pregnant women from 2001-2017. PLoS One. 2022; 17 (10): e0275731.
10. Dalazen CE, Souza AS, Ribeiro CJN, Marques Dos Santos M, Probst LF, Theobald MR,
et al. Space-time risk cluster and time trends of congenital syphilis in Brazil: an ecological study. Trans R Soc Trop Med Hyg. 2022; 116 (9): 822-31.
11. Programa das Nações Unidas para o Desenvolvimento (PNUD), Instituto de Pesquisa Econômica Aplicada (IPEA), Fundação João Pinheiro (FJP). Atlas do Desenvolvimento Humano no Brasil [
Internet]. Brasília: PNUD/IPEA/FJP; 2013 [access in 2025 Abr 18]. Available from:
http://www.atlasbrasil.org.br12. Ministério da saúde (BR). Atenção Primária à Saúde - Relatórios Públicos - Cobertura APS [
Internet] Brasil; 2023 [access in 2025 Mar 20]. Available from:
https://egestorab.saude.gov.br/paginas/acessoPublico/relatorios/relHistoricoCoberturaAB.xhtml13. Secretaria de Saúde (RJ). Dados SUS. [
Internet] Rio de Janeiro, Brasil, 2025 [access in 2025 Mar 20]. Available from:
https://www.saude.rj.gov.br/informacao-sus/dados-sus 14. National Cancer Institute. Division of Cancer Control & Population Sciences. Joinpoint Regression Program, Version 5.3.0.0 –Joinpoint Trend Analysis Software [
Internet] Maryland, USA; 2025 [access in 2025 Abr 18]. Available from:
https://surveillance.cancer.gov/joinpoint/15. Instituto do Homem e Meio Ambiente da Amazônia. Índice de Progresso Social Brasil 2025: Qualidade de Vida nos 5.570 municípios do Brasil. Belém, Pará: Imazon 2025. [access in 2025 Jun 28]. Available from:
https://ipsbrasil.org.br/pt 16. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa nacional de saúde do escolar (PeNSE): análise de indicadores comparáveis dos escolares do 9º ano do ensino fundamental, 2009-2019, municípios das capitais [
Internet]. 2022 [access in 2023 Jul 26]. Available from:
https://www.ibge.gov.br/estatisticas/sociais/educacao/9134-pesquisa-nacional-de-saude-do-escolar.html17. Souza DRS, Morais TNB, Costa KTDS, Andrade FB. Maternal health indicators in Brazil: A time series study. Medicine (Baltimore). 2021; 100 (44): e27118.
18. Ratowiecki J, Santos MR, Poletta F, Heisecke S, Elias D, Gili J,
et al. Inequidades sociales en madres adolescentes y la relación con resultados perinatales adversos en poblaciones sudamericanas. Cad Saúde Pública. 2021; 36 (12): e00247719.
19. Freitas CHSM, Forte FDS, Roncalli AG, Galvão MHR, Coelho AA, Dias SMF. Factors associated with prenatal care and HIV and syphilis testing during pregnancy in primary health care. Rev Saúde Pública. 2019; 53:76.
20. Esposti CDD, Santos-Neto ETD, Oliveira AE, Travassos C, Pinheiro RS. Social and geographical inequalities in the performance of prenatal care in a metropolitan area of Brazil. Ciên Saúde Colet. 2020; 25 (5): 1735-50.
21. Macêdo VC, Lira PIC, Frias PG, Romaguera LMD, Caires S de FF, Ximenes RAA. Risk factors for syphilis in women: case-control study. Rev Saúde Pública. 2017; 51:78.
22. Paixao ES, Ferreira AJF, Pescarini JM, Wong KLM, Goes E, Fiaccone R,
et al. Maternal and congenital syphilis attributable to ethnoracial inequalities: a national record-linkage longitudinal study of 15 million births in Brazil. Lancet Glob Health. 2023; 11 (11): e1734-42.
23. Figueiredo DCMM, Figueiredo AM, Souza TKB, Tavares G, Vianna RPT. Relação entre oferta de diagnóstico e tratamento da sífilis na atenção básica sobre a incidência de sífilis gestacional e congênita. Cad Saúde Pública. 2020; 36 (3): e00074519.
24. Ministério da Saúde (BR) Sistema de informação em Saúde para a Atenção Básica (SISAB): Indicadores de desempenho. Brasília (DF): Ministério da Saúde; 2023. [access in 2023 Jul 26]. Available from:
https://sisab.saude.gov.br/paginas/acessoRestrito/relatorio/federal/indicadores/
indicadorPainel.xhtml;jsessionid=uziVEOSJeBYieVPFdaKx28Nu 25. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Pacto Nacional para a Eliminação da Transmissão Vertical de HIV, Sífilis, Hepatite B e Doença de Chagas como Problema de Saúde Pública. Brasília (DF): Ministério da Saúde; 2022. 1ª ed. [access in 2025 Abr 18]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/pacto_nacional_eliminacao_transmissao_vertical.pdf26. Swayze EJ, Cambou MC, Melo M, Segura ER, Raney J, Santos BR,
et al. Ineffective penicillin treatment and absence of partner treatment may drive the congenital syphilis epidemic in Brazil. AJOG Glob Rep. 2022; 2 (2): 100050.
27. Laurentino ACN, Ramos BA, Lira CDS, Lessa IF, Taquette SR. Atenção à saúde dos parceiros sexuais de adolescentes com sífilis gestacional e seus filhos: uma revisão integrativa. Ciên Saúde Colet. 2024; 29 (5): e12162023.
28. Maia CMF, Marques NP, Dias VO, Martelli DRB, Oliveira EA, Martelli-Júnior H. Epidemiological trends in notified syphilis diagnoses during the COVID-19 pandemic in Brazil. Sex Transm Infect. 2022; 98 (6): 458.
29. Costa IB, Pimenta IDSF, Aiquoc KM, Oliveira ÂGRDC. Congenital syphilis, syphilis in pregnancy and prenatal care in Brazil: An ecological study. PLoS One. 2024; 19 (6): e0306120.
30. Oliveira GL, Ferreira AJ, Santana JG, Lana RM, Cardoso AM, Teles C,
et al. A completeness indicator of gestational and congenital syphilis information in Brazil. Rev Saúde Pública. 2023; 57: 42.
Authors' contributionPimentel SVT: conceptualization and study design, database development, data analysis and interpretation, manuscript writing.
Bastos VMS and Vasconcelos GQ: database development, data analysis and interpretation, manuscript writing.
Fonseca SC: study design, data interpretation, manuscript writing.
Kawa H: conceptualization and study design, data interpretation, manuscript writing.
All authors approved the final version of the article and declared no conflicts of interest.
Data availabilityAll datasets supporting the results of this study are included in the article.
Received on October 11, 2024
Final version presented on July 15, 2025
Approved on August 15, 2025
Associated Editor: Aurélio Costa


 ; Vitória Machado Santos Bastos2
; Vitória Machado Santos Bastos2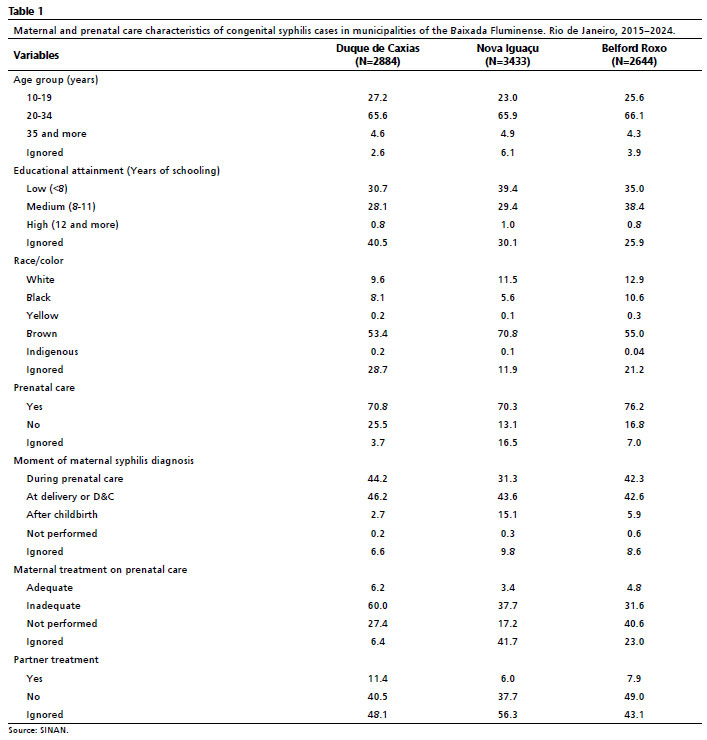






 Ler em português
Ler em português