ABSTRACT
OBJECTIVES: to evaluate the associated factors in the participation of educational activities and the indication of maternity reference of the birth given for the women during prenatal. Methods: A multicenter longitudinal study was conducted in three maternity hospitals. The interview was carried out soon after the childbirth and the outcomes evaluated were the participation of educational activities during the prenatal and the indication of birth maternity reference. The Poisson regression was used in the analysis of the proposed hierarchical model.
RESULTS: Of the 3438 women, 23.2% participated in the educative activities and 61.2% had the childbirth linked to a reference maternity. The women with higher household income (PR= 1.36; CI95%= 1.04-1.77), increase in age by one year (PR= 1.02; CI95%= 1.01-1.04), first pregnancy (PR= 1.84; CI95%= 1.56-2.17), and who practiced physical activity (PR= 1.28; CI95%= 1.09-1.50) had higher prevalence in the participation on the educational activities. The indication of maternity reference was more frequent between the women with higher household income (PR= 1.15; CI95%= 1.01-1.30), education (PR= 1.01; CI95%= 1.00-1.02), non-smoker (PR= 1.31; CI95%= 1.07-1.61), and drug user (PR= 1.44; CI95%= 1.17-1.77).
CONCLUSIONS: despite the wide coverage, the prenatal still has flaws in the actions of education and in the indication of the reference maternity hospital.
Keywords:
Prenatal care, Health education, Quality of health care, Maternal and child health, Perinatal care
RESUMO
OBJETIVOS: analisar os fatores associados à participação das gestantes em atividades educativas e sua indicação à maternidade de referência ao parto durante o pré-natal.
MÉTODOS: estudo longitudinal multicêntrico realizado em três maternidades. Utilizou-se entrevista realizada logo após o parto e os desfechos avaliados foram a participação em atividade educativa no pré-natal e a indicação da maternidade de referência ao parto. Utilizou-se Regressão de Poisson na análise do modelo hierárquico proposto.
RESULTADOS: das 3438 participantes, 23,2% participaram de atividades educativas e 61,2% tiveram o parto referenciadoà uma maternidade. As mulheres com maior renda familiar (RP= 1,36; IC95%= 1,04–1,77), com aumento em um ano na idade (RP= 1,02; IC95%= 1,01–1,04), primeira gestação (RP= 1,84; IC95%= 1,56–2,17) e que praticavam atividade física (RP= 1,28; IC95%= 1,09–1,50) tiveram maior prevalência de participação nas atividades educativas. A indicação da maternidade foi mais frequente entre as mulheres com maior renda familiar (RP= 1,15; IC95%= 1,01–1,30), escolaridade (RP= 1,01; IC95%=1,00–1,02), não tabagistas (RP= 1,31; IC95%= 1,07–1,61) e usuárias de drogas (RP= 1,44; IC95%= 1,17–1,77).
CONCLUSÕES: apesar da ampla cobertura, o pré-natal ainda apresenta falhas nas ações educativas e na indicação da maternidade de referência.
Palavras-chave:
Cuidado pré-natal, Educação em saúde, Qualidade da assistência à saúde, Saúde materno-infantil, Assistência perinatal
IntroductionFor decades, the development and enhancement of public programs and policies has played an important role in the organization of prenatal and child care in Brazil.
1 In 2000, the Ministry of Health created the Program of Humanization of Delivery and Birth (PHPN – Portuguese acronym) for the development of actions of promotion, prevention and assistance to the health of pregnant women and newborns.
2 In 2004, it established the Agenda of Compromises for Integrative Health of Children and Reduction of Infant Mortality, which encourages actions of orientation to mothers about the importance of breastfeeding, heel prick test, umbilical cord care, immunization and first consultation.
3 In 2011, the Stork Network was implemented, another policy that prioritizes the quality of prenatal care and assistance to delivery and birth, including the integrative follow-up of children up to 24 months of life.
4In this scenario, it is known that neonatal deaths are generally associated with flaws in the assistance provided to both mother and newborn during the prenatal and postpartum period and these deaths are considered avoidable by means of the provision of integrative healthcare, including educational activities.
5 There is consistent evidence that educational approaches during pregnancy have a potential impact in the reduction of neonatal mortality.
4 These processes include guidelines for breastfeeding, infant and maternal immunization, umbilical cord care, neonatal screening by means of the “heel prick test”, preventive measures and signs of alert for mother and baby and the first consultation of the newborn in the first week of life.
7 A systematic review on the impact of educational activities developed in low risk prenatal care in obstetric outcomes observed that educational practices during prenatal contribute to favorable obstetric results, since they minimize doubts and the anxiety of women during pregnancy, preparing her for the delivery and postpartum.
8In addition to educational practices, the indication of the maternity hospital during pregnancy promotes the bond of pregnant women with the maternity, averting the pilgrimage of the mother during labor and risks for their health and that of newborns.
4In spite of the increase of prenatal care’s coverage in the country, a study of national basis demonstrated that only a fifth of women had adequate prenatal care and such result is related to regional and social inequalities.
9 The National Health Survey (PNS – Portuguese acronym) identified that 86.6% of women started prenatal before the 13
th week of pregnancy, that 88.8% of women aged 15 or more and with term or post-term births had six or more prenatal consultations and 70.1% had prenatal care in public health facilities, mostly Basic Health Units.
10 Impaired access, unfavorable socioeconomic conditions, low maternal schooling
11 and prenatal pilgrimage
12 were other factors associated with inadequate prenatal care.
The understanding of factors related to the non-participation in educational activities and the non-referral of the pregnant women to the maternity hospital of reference by the public managers may favor the development of effective health actions that, consequently, may contribute to the prevention of complications for both women and newborns. Given the above, the present study analyzed factors associated with the participation in educational activities and the indication of a maternity of reference for birth provided to women during prenatal.
MethodsWe evaluated data from a multicenter cross-sectional study, entitled “
Projeto Viver”, carried out with 3438 puerperal women and newborns from three maternity hospitals of the state of Espírito Santo in the period between August 2019 and March 2020.
The maternity hospitals, located in two health regions of the state (Metropolitan and North), were chosen considering two aspects: (1) to concentrate the highest number of births in the region; (2) to possess variety of assistance, with coverage of 80 to 100% of the Unified Health System (SUS – Portuguese acronym) and 100% private or by supplementary health insurance.
Data collection of mothers and children that did not die after the period from delivery to hospital discharge included interviews of three moments: in person at the maternity hospital, right after birth; on the seventh and 27
th days of the child’s life, when completed the neonatal period, both by phone. In an attempt to reduce losses of follow-up, we performed the second follow-up between the seventh and tenth day after birth; and the third between the 27
th and the 30
th day.
In order to assure the quality of the research, data collection was performed by a properly trained team and using standardized forms. We elaborated an orientation manual about fulfillment of tools and made it available for each team member.
In order to analyze factors associated with the dependent variables (educational activity at prenatal and indication of maternity of reference at birth), we used a hierarchized model divided into three levels, containing demographic and socioeconomic information, as well as behavioral habits and prenatal assistance.
The first level comprises socioeconomic and demographic information of the mother, such as: schooling (complete regular education); family income (categorized into quintiles); marital status (with a partner; without a partner); if the woman had a paid employment (yes; no); amount of inhabitants per room, excluding bathrooms.
In the second level, we used demographic and reproductive information and behavioral habits of the mother during pregnancy: age (years); parity (0;>1); alcohol consumption (yes; no); tobacco consumption (yes; no); drug use (yes; no); physical activity (yes; no); victim of violence (yes; no).
The third level included the gestational variables: model of the health service in which prenatal consultations were performed (public; private); gestational week of onset of prenatal; number of prenatal consultations (<7; ≥7); classification of gestational risk by a health professional (low; average; high; very high); health problems occurred during pregnancy (yes; no).
For the analysis and statistical validation of associations, we used the Stata 16.0 software. In the descriptive analysis, we presented all absolute and relative values of all categorical variables, using Pearson’s chi square test for testing the dependent variables with the independent variables. In the hierarchized model, we used Poisson regression with robust variance adjustment to estimate the ratio of prevalence within women who participated in educational activities in prenatal and those who received orientations about the maternity of reference for delivery. For all analyses, the 5% significance level was used.
Initially, we performed the analysis of each independent variable, using the Akaike Information Criterion (AIC), the Bayesian information criterion (BIC) and adjusted R2 to verify what format (categorical or continuous) would adjust better to the model. Posteriorly, we performed the univariate analysis to retrieve from the model those who presented values
p>0.20. All variables proposed in the hierarchic model had
p<0.07 values.
The multivariate analysis started with the inclusion of all variables of the first level, maintaining those that presented values
p<0.05. Afterwards, variables of the second level were added and those with values
p>0.05 were excluded from the model. The variables of the first level were maintained, regardless of the
p value, after the inclusion of variables of the second level. Subsequently, the variables of the third level were included and those that had
p<0.05 value remained in the model, maintaining the variables of previous levels, regardless of their
p value.
The research was approved by the Research Ethics Committee of the University Vila Velha (UVV), under opinion number 3044870, of Unimed, number 3269032 and Santa Casa de Vitória, number 3356606.
ResultsIn the maternity hospital, 3438 parturient women were interviewed (82.7%) and there was a positive relationship between those who declared having participated in the educational activity during prenatal and age, schooling and family income (
p<0.001). The prevalence of participation in educational activities was higher among women who had partners (24.6%) and those who had paid employment (27.1%) (Table1). However, the prevalence of these activities, in general, was low, since two out of ten women participated in educational activities during prenatal, on average.
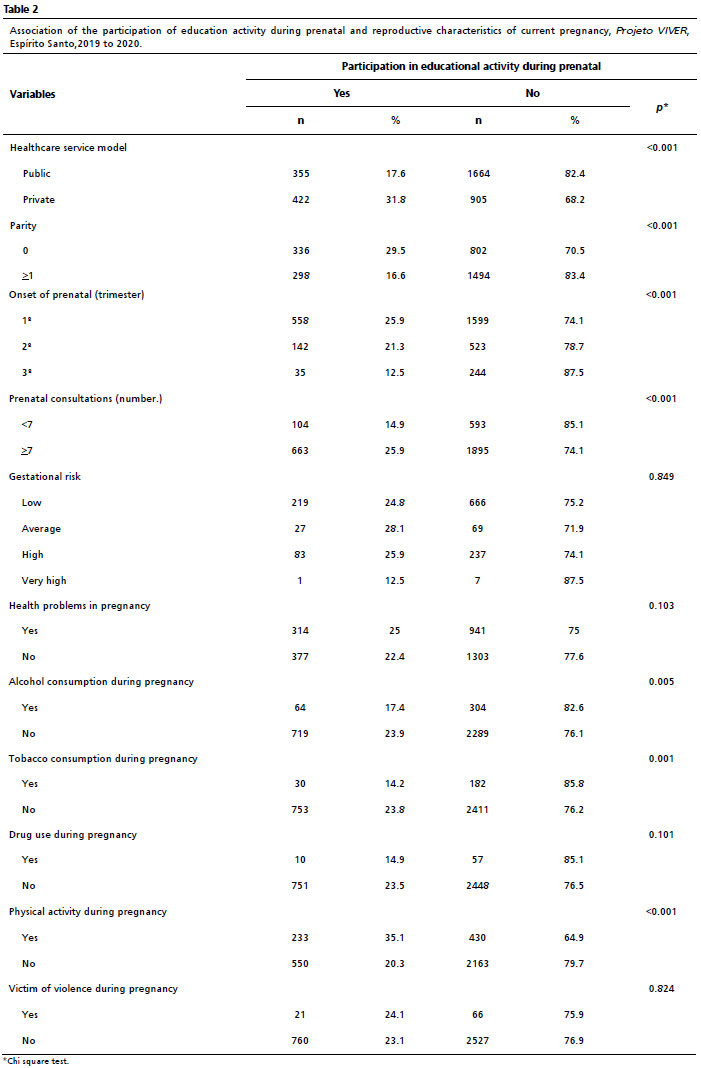
Almost the double of women assisted in supplementary healthcare (31.8%) participated in educational activities compared to those who were followed in public healthcare (17.6%) The primiparous women (29.5%) with prenatal started in the first trimester (25.9%), with more than six consultations (25.9%) and who practiced physical activity (35.1%) presented higher participation in educational activities. However, lower participation was observed in women who consumed alcohol (17.4%) and tobacco (14.2%) in pregnancy (Table 2).
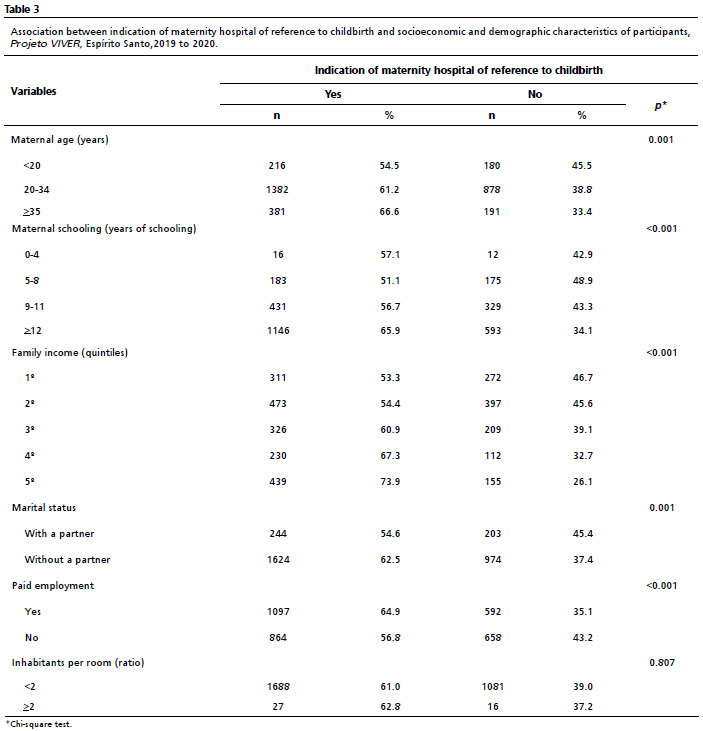
With regard to the indication of maternity hospital of reference to delivery (Table 3), 61.2% of women were informed during prenatal care. The prevalence of indication of the maternity of reference increased with age (
p=0.001), maternal schooling (
p<0.001) and family income (
p<0.001). Women with partners (62.5%) and those who had paid employment (64.9%) were those who most received orientation about maternity hospitals of reference forchildbirth.
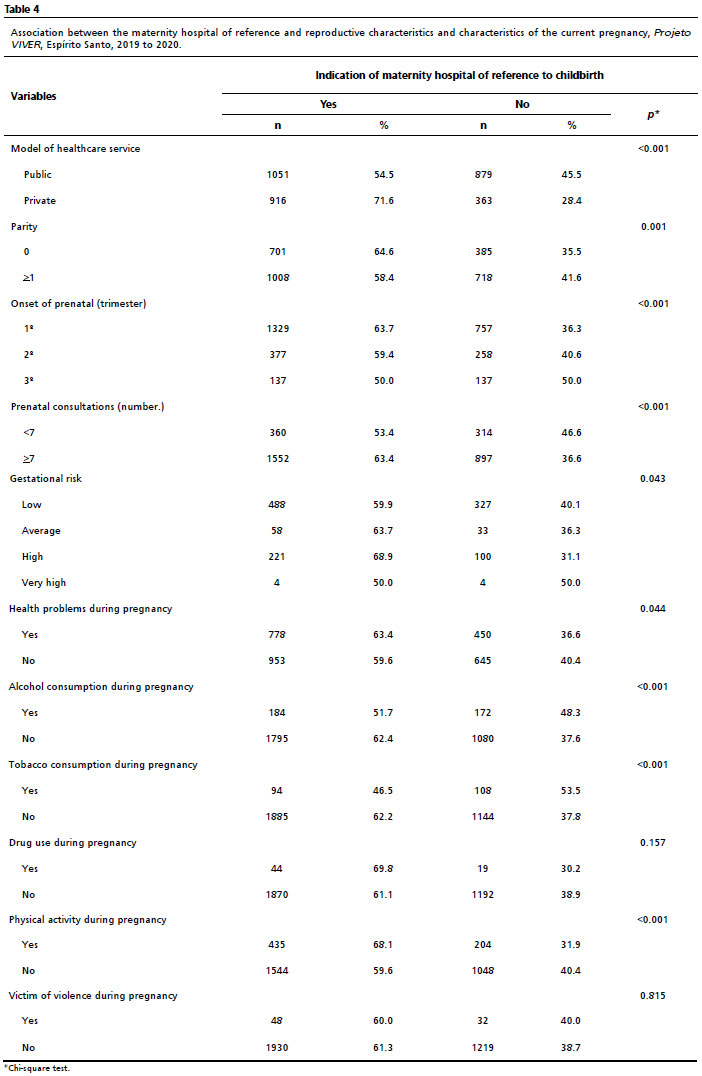
When observing reproductive and gestational characteristics of the participants (Table 4), there was higher indication of maternity hospital of reference for women followed-up in the private healthcare service (71.6%), nulliparous (64.6%), prenatal started in the first trimester (63.7%), with seven or more prenatal consultations (63.4%), of high gestational risk (68.9%), health problems in pregnancy (63.4%), those who did not use alcohol (62.4%) and tobacco (62.2%) and practiced physical activity (68.1%) in pregnancy.
For the participation in educational activities during prenatal, we used in the initial analysis only variables that presented a significance level under 20%, being: maternal schooling (
p<0.001), family income (
p<0.001), marital status (
p=0.002), paid employment (
p<0.001), ratio of inhabitants per room (
p<0.001), maternal age (
p<0.001), parity (
p<0.001), alcohol consumption (
p=0.007), tobacco consumption (
p=0.002), drug use (
p=0.123), physical activity (
p<0.001), model of healthcare service (
p<0.001), trimester of onset of prenatal (
p=0.001), number of prenatal consultations (
p<0.001) and health problems during pregnancy (
p=0.103).
In the final model of participation in educational activities, these variables remained: maternal schooling, family income, maternal age, parity and physical activity in pregnancy (Table 5). The increase in one year of maternal age added 2% in participation in educational activity (PR= 1.02; CI95%=1.01–1.04). The prevalence was 36% higher for women with higher family income than for those poorer (PR= 1.36; CI95%= 1.04–1.77), 84% higher for primiparous women than those with one or more children (PR= 1.84; CI95%= 1.56–2.17) and 28% higher for women who practiced physical activity in pregnancy (PR= 1.28; CI95%= 1.09-1.50).
In the indication of maternity of reference, the variables that presented statistical significance under 20% in the univariate analysis were: maternal schooling (
p<0.001), family income (
p<0.001), marital status (
p=0.003), paid employment (
p<0.001), ratio of inhabitants per room (
p<0.001), maternal age (
p<0.001), parity (
p<0.001), alcohol consumption (
p<0.001), tobacco consumption (
p<0.001), drug use (
p=0.110), physical activity (
p<0.001), model of healthcare service (
p<0.001), trimester of prenatal onset (
p<0.001), number of prenatal consultations (
p<0.001), gestational risk (
p=0.031) and health problems during pregnancy (
p=0.043).
In the final model for the indication of maternity hospital of reference to delivery, the variables that remained were: maternal schooling, family income, alcohol, tobacco and drug consumption during pregnancy and model of healthcare service in which prenatal care was performed (Table 5). When increasing one year to maternal schooling, 1% is added in the indication of maternity hospital of reference (PR= 1.01; CI95%= 1.00-1.02). The indication of maternity hospital was 15% higher for richer women compared to poorer women (PR= 1.15; CI95%= 1.01–1.30), 31% higher for those who did not smoke during pregnancy (PR= 1.31; CI95%= 1.07–1.61), 44% higher for those who used drugs during pregnancy (PR= 1.44; CI95%= 1.17–1.77) and 13% higher for women who had prenatal at supplementary healthcare (PR= 1.13; CI95%= 1.05–1.24).
DiscussionIt is noted that the participation in educational activities during prenatal was more frequent between women with higher income, older age, without children and who practiced physical activity. The indication of the maternity of reference for delivery was more frequent for women with higher schooling, higher family income, with prenatal care provided by supplementary healthcare, but who used drugs during pregnancy.
In spite of the high coverage of prenatal care in Brazil, the quality of this assistance for pregnant women is still low
13 and such reality was reassured in this study, in which only 23% of women had participated in educational activities during prenatal, when 79% had seven or more consultations. Other surveys demonstrate similar results, in which a low proportion of women participate in any physical activity during prenatal,
14,15 demonstrating flaws in the assistance due to absence of important actions that may affect the quality of prenatal. It was also observed social inequalities in the access of women to educational activities, since the prevalence was higher between participants with higher family income, older age and primiparous. The same relationship is observed in different regional
16 and national
9 samples. This possibly occurs because most women with lower socioeconomic conditions use the public healthcare system, in which some social and economic inequalities persist within the geographic regions of the country.
17 With regard to the worse result of prenatal adequacy within multiparous women, it is probably related to the difficulty of attending to health services due to the lack of social support in the care with the other children.
18 A retrospective cohort, with 3235 Canadian medical records, observed that women with inadequate prenatal had lower schooling and higher level of unemployment.
19We highlight that the reality of health service is not always capable of meeting the demands and expectations of women during the pregnancy period, and for many times, this is a consequence of the absence of health professionals qualified for the execution of actions of health promotion by means of health education. The Family Health Strategy (ESF – Portuguese acronym) is a model of healthcare that has as one of its principles actions of health promotion and this was demonstrated in a study carried out with women in prenatal, in which the provision of education information was higher for women followed-up at ESF, by group reunions and/or home visitations.
13Health education as an important role in maternal and newborn care, affects positively the maternal, neonatal and infant health, mainly when they are performed in populations with high mortality rates and limited resources for healthcare.
20 It is known that social and regional inequalities influence the access of pregnant women to educational actions, which are supplementary to prenatal consultations, corroborating what the present study verified, that is, the prevalence of participation in educational activities was higher within women with higher socioeconomic level. Similarly, a survey conducted in Ceará verified that 15% of women had access to actions of promotion and prevention to healthcare in prenatal.
21 Another study, national based however, observed higher prevalence of these actions in the South region of the country, in municipalities with up to ten thousand or with more than 300 thousand inhabitants, and in those with higher HDI.
22A systematic review carried out in USA demonstrates that health education activities with onset in the prenatal and that continue in postpartum are more effective than methods concentrated only in education during pregnancy, presenting better results in the continuity of breastfeeding at six months, in adequate health behaviors and in the better knowledge of healthcare.
6 However, efforts of the entire health system are necessary to increase the awareness of the importance of educational actions not only during prenatal, but also during postnatal.
Surveys carried out in distinct countries have been observing that inequalities in access to healthcare systems are related to age, schooling and family income. In Ghana, the geographic location, family income and schooling are the main factors responsible for inequalities in mother-and-child healthcare.
23 In the USA, there is a strong evidence related with race and ethnicity, health insurance and education in maternal mortality and severe morbidity.
24 In Indonesia, the Demographic and Health Survey demonstrated that maternal age, schooling, number and order of birth of children, difference of age between mother and husband, occupation of husband, wealth index, access to health services and regional factors were significantly associated with the use of prenatal and postnatal care.
26With regard to the indication of maternity hospital of reference, a national hospital based study carried out with 16,220 women demonstrated that 43% did not know which maternity they should search for, being subject to the search for availability of hospital rooms for the execution of labor,
26 which corroborates the result obtained in the present study, in which 39% of women were not referred to the maternity hospital. The pilgrimage of women during labor is a factor that puts the health of both mother and baby at risk and has direct relationship with the increase of neonatal mortality, as demonstrated by a cohort that assessed the profile of neonatal mortality and assistance to pregnant women and newborns and found strong association between neonatal death and pilgrimage for childbirth, since that in 40% of deaths, mothers had roamed by more than one maternity hospital in the moment of labor.
27Therefore, the orientation and indication of the maternity for childbirth should occur since the onset of prenatal care, facilitating the access of pregnant women in the moment of labor or in case of emergencies.
28 In this sense, the high percentage of women who did not know what maternity hospital of reference for labor reflects the absence of planning for assistance to childbirth and flaws of adequacy of the process of prenatal care, according to criteria from the Program of Humanization of Prenatal and Birth and the WHO.
2 Moreover, the access to this orientation was more frequent for women with higher schooling, who had prenatal in supplementary healthcare, non-smokers and drug users.
Concerning drug users, the prenatal of this group can be performed by the Basic Health Unit or by the team of street office, according to the guideline of the Ministry of Health. Thus, it should be assured the linking with the maternity hospital of reference, the evaluation and classification of the risk of the pregnant women, and according to each case, refer to the specialized service of high-risk prenatal, articulating the case with services of psychosocial and family support.
29 These actions may be an explanations for women that use drugs, in this study, being more aware of what maternity they should search for in the moment of labor than those who did not use drugs. Differently from our findings, a retrospective cohort carried out in Canada observed that low quality of prenatal care was more frequent for women with elevated consumption of tobacco and drugs.
19As a limitation, we consider the losses and refusals by the puerperal women at postpartum, since the interviews were performed in the maternity. In order to reduce such bias, women were contacted in, at least, two moments by another interviewer, before being considered a refusal. The dissatisfaction with pregnancy or even with the assistance provided in the maternity hospital may be a factor that contributed to the refusal in participating in the survey, and the result of this study may be underestimated, since there is a relationship of satisfaction of the user and the quality of service, as well as the profile of the user, observing that characteristics such as: being young, exclusive use of SUS, low schooling and bad self-perception of health generated more chances of dissatisfaction of users with the Brazilian health system.
30 Besides, women in postpartum period may not respond adequately to the interview, for being tired or even in situation of postpartum depression, which may be the cause of bias. When observing such a situation, the interviewer would suspend the interview and return in another moment, which may have minimized this bias.
We conclude that, in spite of the high coverage of prenatal consultations, we observed a low scope of actions of health education and the knowledge of mothers in relation to the maternity hospital of reference for childbirth, mainly for women with lower socioeconomic conditions. It is important to encourage and qualify the health team for the development of educational actions with pregnant women, both in-group and individually. The implementation of health policies emphasized in the improvement of quality of prenatal care, including educational actions in the care provided to both pregnant women and newborns is a measure that may reduce postpartum complications, as well as those related to newborn care.
References1. Mamede FV, Prudêncio PS. Contribuições de programas e políticas públicas para a melhora da saúde materna. Rev Gaucha Enferm. 2015; 36 (esp): 262-6.
2. Ministério da Saúde (BR). Portaria n° 569, de 1 de junho de 2000. Institui o Programa de Humanização no Pré-natal e Nascimento no âmbito do Sistema Único de Saúde (SUS). Brasília (DF): DOU de 1 jun 2000; Seção 1, p. 4-6. [access in 2022 Jun 14]. Available from:
https://www.mpba.mp.br/sites/default/files/biblioteca/saude/projeto-cegonha/legislacao/1_portaria_569_2000._programa_de_humanizacao_no_parto.pdf3. Ministério da Saúde (BR). Agenda de compromissos para a saúde integral da criança e redução da mortalidade infantil. Brasília (DF): Ministério da Saúde; 2004.
4. Ministério da Saúde (BR). Portaria 1.459, de 24 de junho de 2011. Institui no âmbito do Sistema Único de Saúde (SUS) a Rede Cegonha. Brasília (DF): DOU de 24 jun 2011; Seção 1, p. 61. [access in 2022 Jun 14]. Available from:
http://www.as.saude.ms.gov.br/wp-content/uploads/2016/07/Portaria-GM-MS-n%C2%BA1.459-do-dia-24-de-junho-de-2011.pdf5. United Nations. The Millennium Development Goals Report 2015 [Internet]. 2015 [access in 2022 Jun 14]. Available from:
https://www.un.org/millenniumgoals/2015_MDG_Report/pdf/MDG%202015%20rev%20(July%201).pdf6. Herval ÁM, Oliveira DPD, Gomes VE, Vargas AMD. Health education strategies targeting maternal and child health: a scoping review of educational methodologies. Medicine (Baltimore). 2019; 98 (26): e16174.
7. Ministério da Saúde (BR). Saúde da criança: aleitamento materno e alimentação complementar. 2ª ed. Brasília (DF): Ministério da Saúde; 2015. [access in 2022 Jun 14]. Available from:
https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/s/saude-da-crianca/publicacoes/saude-da-crianca-aleitamento-materno-e-alimentacao-complementar/view8. Silva EP, Lima RT, Osório MM. Impacto de estratégias educacionais no pré-natal de baixo risco: revisão sistemática de ensaios clínicos randomizados. Ciên Saúde Colet. 2016; 21 (9): 2935-48.
9. Domingues RMSM, Viellas EF, Veras MAB, Torres JA, Theme-Filha MM, Gama SGN,
et al. Adequação da assistência pré-natal segundo as características maternas no Brasil. Rev Panam Salud Publica. 2015; 37 (3): 140-7.
10. Ministério da Economia (BR). Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa nacional de saúde: 2019. Rio de Janeiro (RJ): IBGE; 2021. [access in 2023 Fev 6]. Available from:
https://www.pns.icict.fiocruz.br/wp-content/uploads/2021/12/liv101846.pdf11. Goudard MJF, Simões VMF, Batista RFL, Queiroz RCS, Alves MTSSB, Coimbra LC, et al. Inadequação do conteúdo da assistência pré-natal e fatores associados em uma coorte no nordeste brasileiro. Ciên Saúde Colet. 2016; 21 (4): 1227-38.
12. Mendes RB, Santos JMJ, Prado DS, Gurgel RQ, Bezerra FD, Gurgel RQ. Características maternas e tipo de assistência pré-natal associada à peregrinação no anteparto. Rev Saúde Pública. 2019; 53: 70.
13. Nunes DM, Rigo L, Boclin KLS, Malvestio LMM, Anziliero D, Horta BL, et al. Qualidade do Pré-Natal no Brasil: Pesquisa Nacional de Saúde 2013. Ciên Saúde Colet. 2019; 24 (3): 1223-32.
14. Schwab FCBS, Ferreira L, Martinelli KG, Esposti CDD, Pacheco KTDS, Oliveira AE, et al. Fatores associados à atividade educativa em saúde bucal na assistência pré-natal. Ciên Saúde Colet. 2021; 26 (3): 1115-26.
15. Gonçalves MLC, Silva HO, Oliveira TA, Rodrigues LV, Campos ALA. Perfil sociodemográfico e obstétrico de puérperas assistidas no município de Iguatu – CE. Rev Bras Prom Saúde. 2012; 25 (2 Supl.): 33-9.
16. Anversa ETR, Bastos GAN, Nunes LN, Dal Pizzol TS. Qualidade do processo da assistência pré-natal: unidades básicas de saúde e unidades de Estratégia Saúde da Família em municípios no Sul do Brasil. Cad Saúde Pública. 2012; 28 (4): 789-800.
17. Leal MC, Esteves-Pereira AP, Vilela MEA, Alves MTSSB, Neri MA, Queiroz RCS, et al. Redução das iniquidades sociais no acesso às tecnologias apropriadas ao parto na Rede Cegonha. Ciên Saúde Colet. 2021; 26 (3): 823-35.
18. Pereira L B, Vogt SE, Holzmann APF, Brito MFF, Pinho L, Silveira MF, et al. Apoio social percebido por gestantes e fatores associados: estudo transversal em coorte de base populacional. Ciên Saúde Colet. 2024. [Internet]. [access in 2024 Ago 20]. Available from:
http://cienciaesaudecoletiva.com.br/artigos/apoio-social-percebido-por-gestantes-e-fatores-associados-estudo-transversal-em-coorte-de-base-populacional/1919919. Nussey L, Hunter A, Krueger S, Malhi R, Giglia L, Seigel S, et al. Sociodemographic Characteristics and Clinical Outcomes of People Receiving Inadequate Prenatal Care: A Retrospective Cohort Study. J Obstet Gynaecol Can. 2020; 42 (5): 591-600.
20. Sacks E, Freeman PA, Sakyi K, Jennings MC, Rassekh BM, Gupta S, et al. Comprehensive review of the evidence regarding the effectiveness of community-based primary health care in improving maternal, neonatal and child health: 3. neonatal health findings. J Glob Health. 2017; 7 (1): 010903.
21. Fátima VMM, Barbosa CP, Vertamatti MAF, Tavares MNA, Oliveira CAC, Alencar APA. Acesso aos serviços públicos de saúde e atenção integral à mulher no período gravídico puerperal no Ceará, Brasil. BMC Health Serv Res. 2019; 19 (1): 851.
22. Neves RG, Flores-Quispe MDP, Facchini LA, Fassa AG, Tomasi E. Pré-natal no Brasil: estudo transversal do Programa de Melhoria do Acesso e da Qualidade da Atenção Básica, 2014. Epidemiol Serv Saúde. 2020; 29 (1): e2019019.
23. Anarwat SG, Salifu M, Akuriba MA. Equity and access to maternal and child health services in Ghana a cross-sectional study. BMC Health Serv Res. 2021; 21 (1): 864.
24. Wang E, Glazer KB, Howell EA, Janevic TM. Social Determinants of Pregnancy-Related Mortality and Morbidity in the United States: A Systematic Review. ObstetGynecol. 2020; 135 (4): 896-915.
25. Istifa MN, Efendi F, Wahyuni ED, Ramadhan K, Adnani QES, Wang JY. Analysis of antenatal care, intranatal care and postnatal care utilization: Findings from the 2017 Indonesian Demographic and Health Survey. PLoSOne. 2021; 16 (10): e0258340.
26. Bittencourt DA, Cunha EM, Domingues RMSM, Dias BAS, Dias MAB, Torrever JA, et al. Nascer no Brasil: continuity of care during pregnancy and postpartum period for women and newborns. Rev Saúde Pública. 2020; 54: 100.
27. Lansky S, Friche AAL, Silva AAM, Campos D, Bittencourt DAS, Carvalho ML et al. Pesquisa Nascer no Brasil: perfil da mortalidade neonatal e avaliação da assistência à gestante e ao recém-nascido. Cad Saúde Pública. 2014; 30 (Suppl.1): S192-S207.
28. Polgliane RBS, Leal MC, Amorim MHC, Zandonade E, Santos Neto ET. Adequação do processo de assistência pré-natal segundo critérios do Programa de Humanização do Pré-natal e Nascimento e da Organização Mundial de Saúde. Cien Saúde Colet. 2014; 19 (7): 1999-2010.
29. Ministério do Desenvolvimento Social e Combate à Fome (BR). Nota técnica conjunta sobre Diretrizes, Fluxo e Fluxograma para a atenção integral às mulheres e adolescentes em situação de rua e/ou usuárias de álcool e/ou crack/outras drogas e seus filhos recém-nascidos. Brasília (DF): Ministério da Saúde; 2016. [access in 2022 Jun 14]. Available from:
https://www.mds.gov.br/webarquivos/legislacao/bolsa_familia/nota_tecnica/nt_conjunta_01_MDS_msaude.pdf30. Gouveia GC, Souza WV, Luna CF, Souza-Júnior PRB, Szwarcwald CL. Satisfação dos usuários do sistema de saúde brasileiro: fatores associados e diferenças regionais. Rev Bras Epidemiol. 2009; 12 (3): 281-96.
Authors’ contributionPoton WL: conceptualization and design of the study, data analysis and interpretation of results.
Haddad LSP: data analysis and interpretation of results.
Bubach S, Santos AS, Horta BL, Cypreste AMZ, Souza CG, Oliveira AC, Baltar ECV, Catharino RR, Duemke LB and Santos TMR: conceptualization and design of the study.
All authors approved the final version of the article and declare no conflict of the interest.
Received on December 27, 2023
Final version presented on August 21, 2024
Approved on August 21, 2024
Associated Editor: Aurélio Costa


 ; Susana Bubach 2
; Susana Bubach 2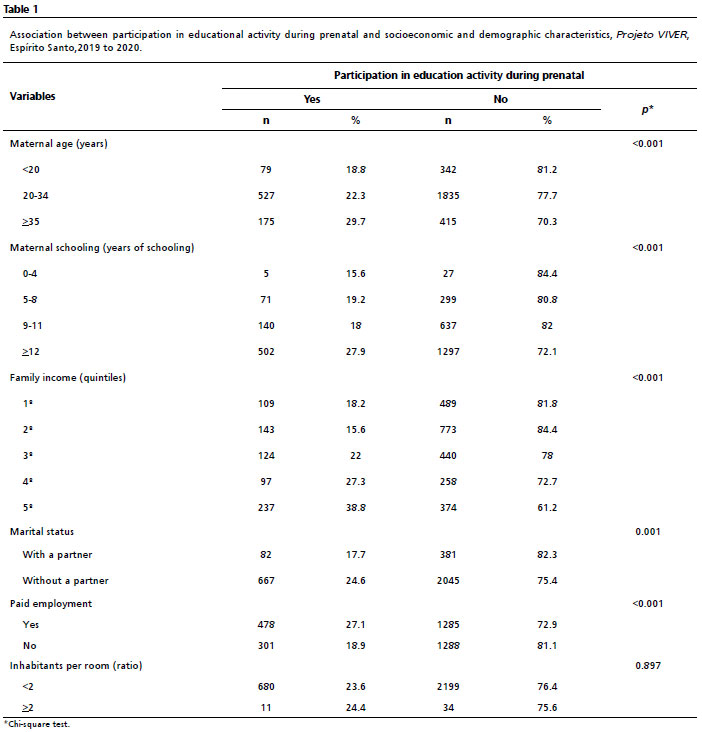







 Ler em português
Ler em português