ABSTRACT
Abstract
OBJECTIVES: to identify the scientific evidence on excessively resistant and multidrug resistant tuberculosis in pediatric patients.
METHODS: this is a scope review of the literature, with a guiding question: "What is the scientific evidence on multidrug-resistant tuberculosis (MDR-TB) and extensively drug-resistant tuberculosis in pediatric patients?". The research used the descriptors: "extensively drug-resistant tuberculosis" OR "multidrug-resistant tuberculosis" AND "pediatrics". The research was carried out in a double-blind manner in the following databases of the Medical Literature Analysis and Retrieval System Online, Regional Office for the Western Pacific's Institutional Repository for Information Sharing, Embase/Elsevier and International Clinical Trials Registry Platform, with a temporal cut-off from 2011 to 2021, sending a final synthesized sample of 18 articles, which evaluated the methodological content through the level of evidence.
RESULTS: the results show the lack of research with a high level of evidence related to MDR-TB in children, the lack of adequate dosage of second-line drugs for the pediatric population and the importance of drug sensitivity testing for the cases of treatment
CONCLUSIONS: it was identified that the obstacles to MDR-TB treatment were concentrated in the lack of detailed protocols, safe drug dosages with a low side effect, and mainly in the social health determinants and disease process involving MDR-TB.
Keywords:
Multidrug-resistant tuberculosis, Extensively drug-resistant tuberculosis, Pediatrics, Social determinants of health
RESUMO
OBJETIVOS: identificar as evidências científicas sobre tuberculose excessivamente resistente e multidroga resistente em pacientes pediátricos.
MÉTODOS: trata-se de uma revisão de escopo da literatura, tendo como questão norteadora: "Quais as evidências científicas sobre tuberculose multidroga-resistente (TB-MDR) e tuberculose extensivamente resistente em pacientes pediátricos?" A pesquisa usou os descritores: "tuberculose extensivamente resistente a medicamentos" OR "tuberculose resistente a múltiplos medicamentos" AND "pediatria". A pesquisa foi realizada de modo duplo-cego nas bases de dados Medical Literature Analysis and Retrieval System Online, Regional Office for the Western Pacific's Institutional Repository for Information Sharing, Embase/Elsevier e International Clinical Trials Registry Platform, com um corte temporal de 2011 a 2021, sendo a amostra final sintetizada de 18 artigos, nos quais avaliou-se o conteúdo metodológico por meio do nível de evidência.
RESULTADOS: os resultados mostraram a escassez de pesquisas de alto nível de evidência relacionadas à TB-MDR em crianças, ausência de posologia adequada das drogas de segunda linha para o público pediátrico e a importância do teste de sensibilidade a drogas para o tratamento dos casos.
CONCLUSÕES: identificou-se que os obstáculos do tratamento TB-MDR se concentraram na ausência de protocolos detalhados, de dosagens medicamentosas seguras e com menor efeito colateral, e, principalmente, nos determinantes sociais do processo saúde e doença que envolvem a TB-MDR.
Palavras-chave:
Tuberculose multidroga resistente, Tuberculose extensivamente resistente a drogas, Pediatria, Determinantes sociais de saúde
IntroductionTuberculosis (TB) is a global disease and one of the ten leading causes of death in the world, ranking first in deaths from a single infectious agent, and in terms of numbers, the Human Immunodeficiency Virus (HIV) surpasses deaths. Worldwide, it is estimated that in 2019, ten million people would have TB, of which 12% were children and adolescents under the age of 15.
1 According to the Ministry of Health, between 2017 and 2019 there was an increase in cases of TB in Brazil, however, in 2020 there was a sharp decrease in this number adding to an increase of cases in abandoning the treatment, totaling 66,819 new cases of TB.
2Multidrug-resistant TB (MDR-TB) represents a challenge to the success of controlling global tuberculosis due to the high incidence of cases,
3,4 and consisting of infection by Mycobacterium tuberculosis resistant to two or more drugs, usually rifampicin and isoniazid. The prevalence of MDR-TB increased from 50,000 cases in 2009 to over 150,000 cases in 2017.
5Regarding to children, in 2018, tuberculosis in children under 15 years old accounted for 11% of the cases in the global context, and the number of children starting TB treatment was 349,487, which represented an increase of 20% compared to 2017. Estimates suggest that from 2018 to 2022 the number of people diagnosed and treated for TB would be 40 million, of which 3.5 million would be children.
6 Currently, in areas with high numbers of new cases, TB is among the top ten diseases responsible for the death of children under five years old.
7 In most cases, a child suspected of having TB is when they have a recurrent respiratory illness. A study carried out in 2018 indicated that approximately 32,000 children worldwidely has MDR-TB every year, and these cases are even more neglected in terms of diagnosis and treatment.
8,9MDR-TB in children is extremely challenging. In addition to obstacles regarding the quality of samples in children in obtaining diagnoses and those who have negative bacilloscopy have paucibacillary, there is the prolonged treatment, which ranges from 18 to 20 months.
9 Nevertheless, health services are not prepared to manage the cases mentioned, which is due to limited public health policies in the area, insufficient research and lack of access to adequate drug therapy, culminating in inadequate health care.
10In this context, given the substantial lack of research in the area and the negligence involving the disease in this vulnerable population, it is essential to discuss the diagnosis, of the treatment and managing childhood MDR-TB cases. This article aimed to carry out a scope review of the scientific evidence found in the literature on extensively resistant TB and MDR-TB in pediatric patients.
MethodsThis literature review was conducted using the scope review method, which provides a mapping of the available evidence, allowing to identify knowledge gaps.
11To define the guiding question, the acronym PECO (Population/Exposure/Comparison/Outcomes) was used, considering Population = (Pediatric patients with multidrug-resistant TB), Exposure = (Anti-tuberculosis antimicrobials), Comparison = (Pediatric patients with non-multidrug-resistant TB) and Outcome = (Prognosis).
12,13 Thus, the guiding question was: "What is the scientific evidence on MDR-TB and extensively resistant TB in pediatric patients?". The Preferred Reporting Items for Systematic Review and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) statement was used to summarize the study selection process and its stages, as shown in Figure 1.
11 The MEDLINE/PubMed (Medical Literature Analysis and Retrieval System Online), Regional Office for the Western Pacific's Institutional Repository for Information Sharing (WHO IRIS), Embase/Elsevier and International Clinical Trials Registry Platform (ICTRP) databases were used. The search strategy was designed and conducted by two experienced authors, independently, using the Health Sciences Descriptors (DeCS) and translated into the Medical Subject Headings (MeSH): "Extensively Drug-Resistant Tuberculosis" OR "Tuberculosis Resistant to Multiple Drugs" AND "Pediatrics" // "Extensively Drug-Resistant Tuberculosis" OR "Tuberculosis, Multidrug-Resistant" AND "Pediatrics"
Inclusion criteria included: publications from 2011 to 2021, in English, Spanish and Portuguese, full text available or not, and case reports, original articles, clinical trials, meta-analyses, randomized controlled trials and systematic reviews. The target public for the study was the pediatric population aged between zero to ten, excluding adolescents. Next, the studies to be used were identified by selecting title, abstract and complete reading, using Mendeley - Reference Management Software, thus removing duplicate articles and increasing the reliability of the research. Articles that did not address the guiding question described were excluded, as well as articles classified as books, documents, preprints, editor's comments and integrative review articles.
After reading and selecting the articles, they were summarized in a Microsoft Word Office 365 document, containing: year of publication, authors' names, publication title, language, database and a brief conclusion about the article's content. It also contains the main information on the level of evidence and contribution to clinical practice, as well as the impact factor of the journals.
In order to fulfill the requirement of a scope review and promote greater robustness and quality of production, our study evaluated the level of evidence (LE) identifying according to the hierarchy, chosen because it is widely used and effective for classifying evidence for literature reviews: NE I - Systematic reviews or meta-analyses of randomized clinical trials; NE II - Well-designed randomized controlled clinical trial; NE III - Well-designed controlled clinical trial without randomization; NE IV - Well-designed cohort, case-control, cross-sectional study; NE V - Systematic review of qualitative studies and descriptive studies; NE VI - Single descriptive or qualitative study; NE VII - Authority opinion and/or expert report.
ResultsEighteen articles were selected according to the inclusion criteria presented. All the articles were originally published in English and 38.8% of them took place in the Asian continent. Of the total number selected, 94.4% were obtained from the MEDLINE/PubMed database and only 5.6% were selected from the Embase/Elsevier and International Clinical Trials Registry Platform (ICTRP) databases.
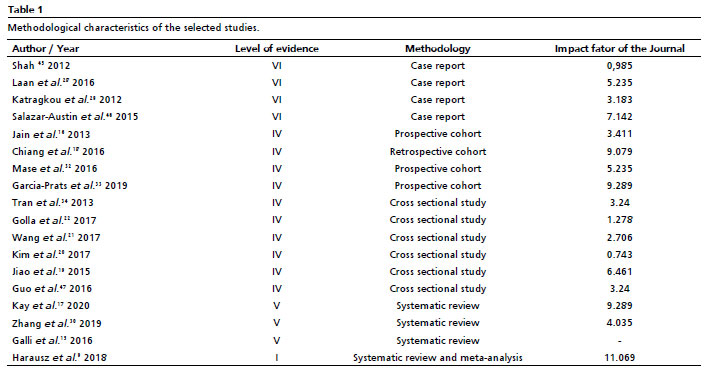
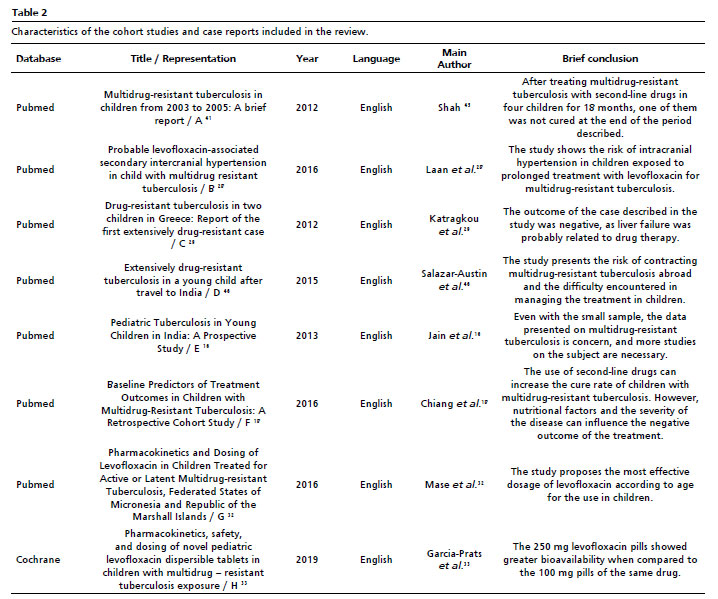
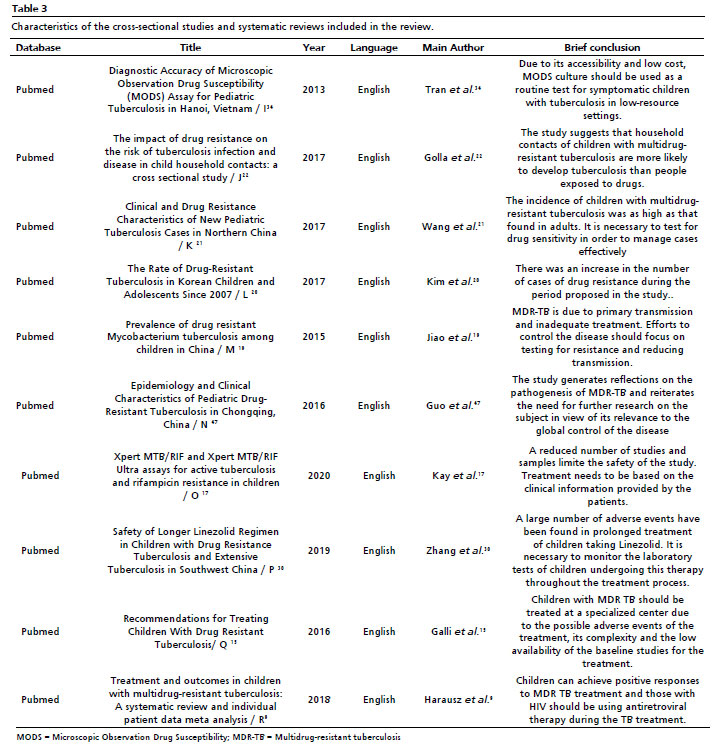
Table 1 shows the level of evidence of the articles, as well as its methodological design and the impact fator of the journal. Among the articles reviewed, four are case reports (22.2%), four cohort studies, three prospective and one retrospective (22.2%), as shown in Table 2, as well as six cross-sectional studies (33.3%), this was the most prevalent study, and four systematic reviews (22.2%) found in Table 3.
Adding up the cases presented in the four case reports reviewed, we obtained 100% of the cases of children with MDR-TB tuberculosis, among them 25% confirmed with Bacillus Calmette and Guérin (BCG) vaccination and 25% were unvaccinated. Among the remaining 50% of the children, the data was not described. In only 25% of the children there was a household with an adult case of TB or MDR-TB confirmed; 50% of the case studies had no outcome described; 25% of the children were cured; 12.5% died and the remaining 12.5% abandoned the treatment.
Of all the cohorts analyzed, 25% reported exposure to wood smoke as a risk factor for contracting TB as a current finding in the literature and 50% of the cohorts included a proposed dosage of levofloxacin, an antibiotic of the fluoroquinolone class, for MDR-TB treatment in pediatric patients. These are shown in Table 2.
Of the cross-sectional studies analyzed, only 33.3% indicated human immunodeficiency virus (HIV) infection as an obstacle to MDR-TB treatment. The negligence of tuberculosis programs in relation to the disease in children was pointed out in approximately 16.6% of the studies. Of the total data presented, only 16.6% showed greater resistance to ethambutol in the sample analyzed, while 33.3% showed resistance to isoniazid and 16.6% to streptomycin. The remaining 33.3% did not provide any information. In the context of the systematic reviews, all of them described HIV infection as a risk factor for having MDR-TB; 25% of the reviews emphasized HIV as a risk factor; 50% mentioned the absence of BCG vaccine and HIV as risk factors; and the last 25% described HIV infection, absence of BCG and nutritional alterations as risk factors for MDR-TB.
Only 25% of the reviews discussed the adverse effects of the treatment, identifying peripheral neuropathy, anemia and leukopenia as the most serious in children. All the articles emphasized the importance of drug sensitivity testing for the diagnosis and effective treatment on MDR-TB, but also highlighted the lack of access to this test. The details are shown in Table 3.
DiscussionThe scientific evidence on MDR-TB and extensively resistant TB in pediatric patients, summarized in this scope review in 18 articles presented in Tables 2 and 3, showed the following main findings: MDR-TB treatment is a social and economic challenge and a cure is not always achieved. In addition, they show risks arising from the treatment such as intracranial hypertension and liver failure. It is noteworthy that the 250mg dose of levofloxacin, the main drug used for the treatment, has greater bioavailability, favoring treatment. Systematic reviews and cross-sectional studies have shown that one of the biggest obstacles is the household contact of children with MDR-TB, who are more likely to develop TB than people exposed to drugs, as well as the difficulty of family and child adherence to the treatment of the disease.
Globally, drug susceptibility tests (DST), especially faster culture techniques, a unique component in managing MDR-TB cases, are not easily accessible in the health services and when they are available, there are delays in the results, as well as other obstacles such as difficulties in collecting samples from children and the fact that samples from adult cases are prioritized for analysis, all of which make it difficult to diagnose children.
14,15However, Jain
et al.16 reaffirm the challenge of obtaining a diagnosis of MDR-TB in children, pointing out the difficulty in collecting samples from children for microscopic exams and cultures, the greater likelihood of this population having the disease in its extrapulmonary form and the paucibacillary characteristic that is often present. Therefore, the treatment should start according to the known sensitivity in adults until the DST result.
9,15-22 However, children who have already had and abandoned the treatment for active TB or who have relapsed disease after first-line drug therapy are also possible sources of MDR-TB.
23In view of this, TB cases in adults are a way of screening and diagnosing child contact early, and should be carried out mainly by the
Estratégia Saúde da Família (ESF) (Family Health Strategy) through the
Programa Nacional de Controle da Tuberculose (PNCT) (National Tuberculosis Control Program).
24 In addition, investment should also be made in directly observed treatment (DOT) for the pediatric population. DOT for pediatric patients consists of a set of activities aimed to ensure planned care for children. One of these strategies is observation during medication intake, which can be done by the child's caregiver if the health professional accompanying the family is capable.
25-27 In none of the articles summarized in this review is considering DOT a strategy for children, which shows the invisibility of childrenfacing care strategies.
27Another important aspect refers to the lack of adequate dosage of second-line drugs used in treating MDR-TB in children, despite the fact that the treatment is 30% higher than in adults. However, pediatric patients face serious damage related to drug toxicity, most of which can be managed and contained when the patient is monitored and followed up. A few exceptions include hearing loss, hypothyroidism and liver failure, which are cited in the literature as effectively incapacitating for children.
28,29Cases of increased intracranial pressure have been reported
30 as an adverse effect of levofloxacin, one of the drugs of choice in MDR-TB treatment.
28 In line with adverse drug reactions. Anemia, peripheral neuropathy and leukopenia were also the main adverse effects found in MDR-TB therapies.
30-33It is worth pointing out that there is a great deal of difficulty in accessing care for these children, and when it is finally provided, there are often many limitations in the health services, including in terms of the team's knowledge in relation to the disease in question,
18 highlighting yet another weakness in health care on MDR-TB.
18Some of the analyzed authors described higher MDR-TB morbidity in pediatric patients with nutritional deficiencies, carriers of the human immunodeficiency virus (HIV) and those who did not have the BCG vaccine.
17,18,22 Not only child malnutrition, the absence of BCG and vertical transmission of HIV are important social markers of poverty and social inequality, which reveal MDR-TB at childhood as a disease of poverty.
34Children with HIV taking antiretroviral therapy (ART) are more likely to have a positive MDR-TB treatment outcome when compared to those not taking ART.
9 Immunodeficiencies are important risk factors for becoming ill with TB, due to alterations in immune responses to pathogens, leaving the individual even more vulnerable.
31,35 Vertical transmission of HIV can be avoided, but many low-income pregnant women do not have access to prenatal care services,
35,36,37 highlighting the relationship between poverty and health inequalities.
31In regard to nutritional issues, childcare consultations should be a unique component in the follow-up of these children, since it is possible to trace the socioeconomic profile of the patients attended.
36,37 Although there is a substantial supply of food from the agriculture in Brazil, the lack of capital for a large portion of the population prevents access,
38 causing nutritional deficiencies to remain and contributing to greater morbidity from MDR-TB in pediatric patients.
38-40 By 2030, the eradication of hunger and poverty is one of the goals of the Millennium Development Goals. One strategy for achieving these goals is to eliminate malnutrition by 2030 and solve the problem in children under five Years old by 2025.
41Regarding the importance of BCG vaccination, a document published in 2018 by WHO points out that it is the only tuberculosis vaccine available, preventing the most severe forms of the disease, and that vaccination on newborns is one of the main pillars of the global tuberculosis reduction strategy.
42 With the COVID-19 pandemic and its social isolation measures, childhood vaccination has suffered a concerning decline.Estimates suggest that approximately 80 million children are left vulnerable to the infection by preventable diseases due to the reduction of the global vaccination coverage.
40-42Tuberculosis is historically associated with poverty, human settlements, poor sanitation and consequently social stigma. Thus, the disease is closely linked to an issue of social vulnerability and should be discussed based on the social determinants of health (SDH) found.
39,41-43 It should be noted that none of the articles reviewed analyzed the socio-economic impacts of the diagnosis, treatment and managing MDR-TB in pediatric patients. Some of them refer to the lack of public policies and research in the area, resulting in a lack of knowledge and fear of managing and treating the cases in this matter.
15,17,19,44-47This demonstrates the importance of SDH in planning an effective therapeutic plan for each individual suffering from TB, as well as the necessity of social support for this population, resulting in overall control of the disease.
46,47It was found that the lack of studies on MDR-TB in children is an obstacle to the diagnosis, treatment and proper management of the cases. In addition, the gap in screening household of adult patients diagnosed with MDR-TB, it becomes difficult to access health services and neglect the disease in becoming a major public health problem, reflecting negatively on the attempt to reduce overall cases of tuberculosis.
The BCG vaccine, good nutritional aspects and antiretroviral therapy for children with HIV are essential to reduce the risk of contracting MDR-TB in children. The lack of drugs with adequate dosages for pediatric patients is another important challenge, causing a major toxic effect in children, who in turn must be monitored assiduously by the health team throughout the treatment.
In short, this review has shown, through synthesized articles, that the obstacles to MDR-TB treatment have focused on the lack of detailed protocols, safe drug dosages with fewer side effects, and especially the social determinants of the health and disease process surrounding MDR-TB.
In this context, our review found evidence that corroborates the necessity to invest in clinical research, with a high level of evidence on the subject, since there are gaps in knowledge that still need to be clarified, contributing to the reduction of MDR-TB in children.
References1. World Health Organization (WHO). Global Tuberculosisis Report 2020. Geneva: WHO; 2020. [access in 2021 Abr 19]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131-eng.pdf2. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Boletim Epidemiológico Tuberculose 2021. Brasília (DF): Ministério da Saúde; 2021. [access in 2021 Abr 19]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2021/boletim-tuberculose-2021_24.033. Piubello A, Souleymane MB, Hassane-Harouna S, Yacouba A, Lempens P, Assao-Neino MM,
et al. Management of multidrug-resistant tuberculosis with shorter treatment regimen in Niger: nationwide programmatic achievements. Respir Med. Jan 2020; 161: 105844.
4. Lange C, Dheda K, Chesov D, Mandalakas AM, Udwadia Z, Horsburgh Jr CR. Management of drug-resistant tuberculosis. Lancet. 2019 Set; 394 (10202): 953-66.
5. Glanziou P. Predicted impact of the COVID-19 pandemic on global tuberculosis deaths in 2020. Medrxiv. 2020; 20 (1): 1-7.
6. World Health Organization (WHO). Global Tuberculosisis Report 2019. Geneva: WHO; 2020. [access in 2021 Abr 19]. Available from:
https://iris.who.int/bitstream/handle/10665/329368/9789241565714-eng.pdf?sequence=197. Velizarova S, Gabrovska N, Spasova A, Marais B, Harausz EP, Tiberi S,
et al. Management and outcomes of severe childhood tuberculosis in the pediatric intensive care setting: can we identify best practices? J Bras Pneumol. 2019; 45 (2): e20190043.
8. Santanna CC. Diagnóstico da tuberculose na infância e na adolescência. Pulmão RJ. 2012; 21 (1): 60-4
9. Harausz EP, Garcia-Prats AJ, Law S, Schaaf HS, Kredo T, Seddon JA,
et al. Treatment and outcomes in children with multidrug-resistant tuberculosis: a systematic review and individual patient data meta-analysis. PLOS Med. 2018 Jul; 15 (7): e1002591.
10. World Health Organization (WHO). Road map toward ending TB in children and adolescents. 2nd ed. Geneva: WHO; 2018. [access in 2021 Abr 19]. Available from:
https://www.stoptb.org/publications/roadmap-towards-ending-tb-children-and-adolescents-2nd-edition11. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D,
et al. PRISMA extension for scoping reviews (prisma-scr): checklist and explanation. Ann Intern Med. 2018 Set; 169 (7): 467.
12. Melnyk BM, Fineout-Overholt E. Evidence-Based practice in nursing & healthcare: a guide to best practice. Philadelphia: Lippincott Williams & Wilkins; 2018. 823 p.
13. Morgan RL, Whaley P, Thayer KA, Schünemann HJ. Identifying the PECO: a framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int. 2018 Dez; 121: 1027-31.
14. Reubenson G. Pediatric drug-resistant tuberculosis. Pediatric Drugs. 2011; 13 (6): 349-55.
15. Galli L, Lancella L, Garazzino S, Tadolini M, Matteelli A, Migliori GB,
et al. Recommendations for treating children with drug-resistant tuberculosis. Pharmacol Res. 2016 Mar; 105: 176-82.
16. Jain SK, Ordonez A, Kinikar A, Gupte N, Thakar M, Mave V,
et al. Pediatric tuberculosis in young children in india: a prospective study. Bio Med Res Int. 2013; 2013: 1-7.
17. Kay AW, González Fernández L, Takwoingi Y, Eisenhut M, Vu RD, Steingart KR,
et al. Xpert MTB/RIF and Xpert MTB/RIF Ultra assays for active tuberculosis and rifampicin resistance in children. Cochrane Database Syst Rev. 2020 Aug; 8 (8): CD013359.
18. Chiang SS, Starke JR, Miller AC, Cruz AT, Del Castillo H, Valdivia WJ,
et al. Baseline predictors of treatment outcomes in children with multidrug-resistant tuberculosis: a retrospective cohort study. Clin Infect Dis. 2016 Jul; 63 (8): 1063-71.
19. Jiao WW, Liu ZG, Han R, Zhao XQ, Dong F, Dong HY,
et al. Prevalence of drug resistant Mycobacterium tuberculosis among children in China. Tuberculosis. 2015 Mai; 95 (3): 315-20.
20. Kim HJ, Yoon HH, Eun BW, Ahn Y, Ryoo S, Kim HJ. The rate of drug-resistant tuberculosis in korean children and adolescents since 2007. J Korean Med Sci. 2017 Jun; 32 (6): 954-60.
21. Wang T, Dong F, Li QJ, Yin QQ, Song WQ, Mokrousov I,
et al. Clinical and drug resistance characteristics of new pediatric tuberculosis cases in northern china. Microb Drug Resist. 2018 Nov; 24 (9): 1397-403.
22. Golla V, Snow K, Mandalakas AM, Schaaf HS, Du Preez K, Hesseling AC,
et al. The impact of drug resistance on the risk of tuberculosis infection and disease in child household contacts: a cross sectional study. BMC Infect Dis. 2017 Ago; 17 (1): 593.
23. Schaaf HS. Diagnosis and management of multidrug-resistant tuberculosis in children: a practical approach. Ind J Pediatr. 2019; 86 (8): 717-24.
24. Araújo DS, Palheta MD, Souza JC, Júnior ID, Silva FB, Araújo VD,
et al. O papel do enfermeiro na busca ativa de pacientes em abandono do tratamento de tuberculose: uma revisão integrativa da literatura. Rev Eletr Acervo Saúde. 2020 Set; 59 (Supl.): e4263.
25. Medina MG, Giovanella L, Bousquat A, Mendonça MH, Aquino R. Atenção primária à saúde em tempos de COVID-19: o que fazer? Cad Saúde Pública. 2020; 36 (8): e00149720.
26. Silva ANC, Ross JR. Tratamento diretamente observado na tuberculose. J Manag Primary Health Care. 2020; 12: 1-11.
27. Jonckheree SF, Jennifer OC. Overcoming Challenges in the Diagnosis, Prevention, and Treatment of Pediatric Drug-Resistant Tuberculosis. Expert Rev Respir Med. 2017; 5 (11): 385-94.
28. Laan LE, Schaaf HS, Solomons R, Willemse M, Mohamed N, Baboolal SO,
et al. Probable levofloxacin-associated secondary intracranial hypertension in a child with multidrug-resistant tuberculosis. Pediatr Infect Dis J. 2016 Jun; 35 (6): 706-8.
29. Katragkou A, Antachopoulos C, Hatziagorou E, Sdougka M, Roilides E, Tsanakas J. Drug-resistant tuberculosis in two children in Greece: report of the first extensively drug-resistant case. Eur J Pediatr. 2012 Ago; 172 (4): 563-7.
30. Zhang Z, Cheng Z, Liu Q, Shang T, Jiang L, Fu Z,
et al. Safety of longer linezolid regimen in children with drug-resistant tuberculosis and extensive tuberculosis in Southwest China. J Glob Antimicrob Resist. 2020 Jun; 21: 375-9.
31. Barreto ML. Desigualdades em Saúde: uma perspectiva global. Ciên Saúde Colet. 2017; 22 (7): 2097-2108.
32. Mase SR, Jereb JA, Gonzalez D, Martin F, Daley CL, Fred D,
et al. Pharmacokinetics and dosing of levofloxacin in children treated for active or latent multidrug-resistant tuberculosis, federated states of micronesia and republic of the marshall islands. Pediatr Infect Dis J. 2016 Abr; 35 (4): 414-21.
33. Garcia-Prats AJ, Purchase SE, Osman M, Draper HR, Schaaf HS, Wiesner L,
et al. Pharmacokinetics, safety, and dosing of novel pediatric levofloxacin dispersible tablets in children with multidrug-resistant tuberculosis exposure. Antimicrob Agents Chemother. 2019 Jan; 63 (4): e01865.
34. Tran ST, Renschler JP, Le HT, Dang HT, Dao TM, Pham AN,
et al. Diagnostic accuracy of microscopic observation drug susceptibility (MODS) assay for pediatric tuberculosis in hanoi, vietnam. PLoS ONE. 2013 Set; 8 (9): e72100.
35. Friedrich L, Menegotto M, Magdaleno MA, Silva OLC. Transmissão vertical do HIV: uma revisão sobre o tema. Bol Cient Pediatr. 2016; 5 (3): 81-6.
36. Tahan TT, Gabardo BM, Rossoni AM. Tuberculosis in childhood and adolescence: a view from different perspectives. J Pediatr (Rio J.). 2020 Mar; 96: 99-110.
37. Góes FG, Silva MD, Paula GK, Oliveira LP, Mello ND, Silveira SS. Nurses' contributions to good practices in child care: an integrative literature review. Rev Bras Enferm. 2018; 71 (Suppl. 6): 2808-17.
38. Ministério da Saúde (BR). Portaria nº 1130, de 05 de agosto de 2015. Institui a Política Nacional de Atenção Integral à Saúde da Criança (PNAISC) no âmbito do Sistema Único de Saúde (SUS). Brasília (DF): Ministério da Saúde; 2015. [access in 2021 Mai 6]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2015/prt1130_05_08_2015.html39. Garcia LRS, Roncalli AG. Determinantes socioeconômicos e de saúde da desnutrição infantil: uma análise da distribuição espacial. Saúde Pesq. 2020; 13 (3): 595-606.
40. Brasil. Presidência da República. Lei nº 10.836, de 09 de janeiro de 2004. Cria o Programa Bolsa Família e dá outras providências. Brasília (DF); 2004. [access in 2021 Mai 6]. Available from:
http://www.planalto.gov.br/ccivil_03/_ato2004-2006/2004/lei/l10.836.htm 41. Organização das Nações Unidas (ONU). Objetivos de Desenvolvimento Sustentável. Transformando Nosso Mundo: A Agenda 2030 para o Desenvolvimento Sustentável. Rio de Janeiro: ONU; 2015. [access in 2021 Mai 6]. Available from:
https://brasil.un.org/sites/default/files/2020-09/agenda2030-pt-br.pdf42. World Health Organization (WHO). BCG vaccines: WHO position paper – February 2018. Releve Epidemiologique Hebdomadaire. Genebra: WHO; 2018. [access in 2021 Apr 29]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/260307/WER9308-73-96.pdf?sequence=1&isAllowed=y. 43. Ministério da Saúde (BR). Manual de Normas e Procedimentos para Vacinação. Brasília (DF): Ministério da Saúde; 2014. [access in 2021 Apr 29]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_procedimentos_vacinacao.pdf44. Sato APS. Pandemia e coberturas vacinais. Rev Saúde Pública. 2020; 54: 115.
45. Shah I. Multidrug-resistant tuberculosis in children from 2003 to 2005: a brief report. Indian J Med Microbiol. 2012; 30 (2): 208-11.
46. Salazar-Austin N, Ordonez AA, Hsu AJ, Benson JE, Mahesh M, Menachery E,
et al. Extensively drug-resistant tuberculosis in a young child after travel to India. Lancet Infect Dis. 2015 Dez; 15 (12): 1485-91.
47. Guo Q, Pan Y, Yang Z, Liu R, Xing L, Peng Z,
et al. Epidemiology and clinical characteristics of pediatric drug-resistant tuberculosis in chongqing, china. Plos One. 2016 Mar; 11 (3): e0151303.
Authors' contributions: Sobreira LB, Freitas PSS and Rezende LDA: conception and design of the study; data analysis and interpretation; writing of the manuscript; critical and intellectual review. Nascimento LCN, Vieira ACBCV, Sales CMM and Pacheco AO: manuscript drafting; critical and intellectual review.
All the authors have approved the final version of the article and declare no conflict of interest.
Received on March 10, 2023
Final version presented on October 19, 2023
Approved on November 23, 2023
Associated Editor: Pricila Mullachery


 ; Paula de Souza Silva Freitas2
; Paula de Souza Silva Freitas2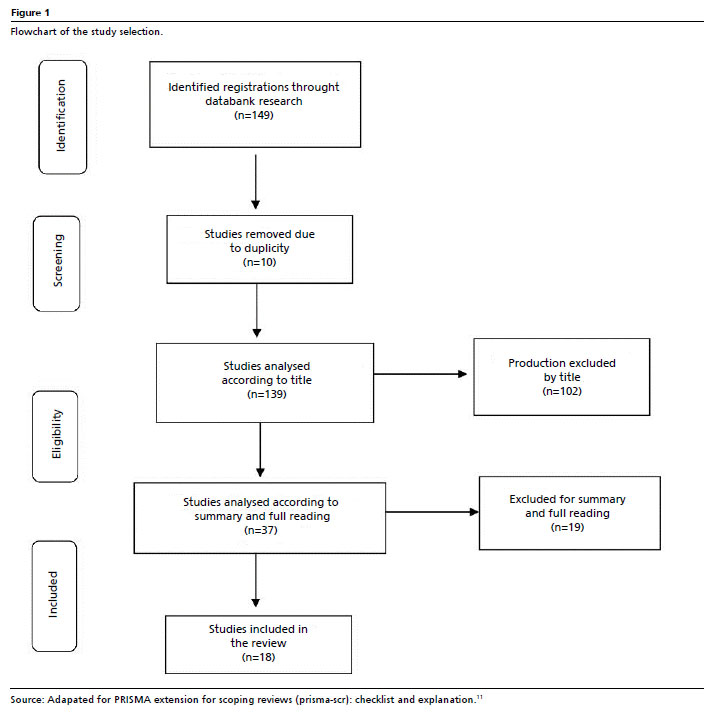






 Ler em português
Ler em português