ABSTRACT
OBJECTIVES: compare the evaluation of breastfeeding technique between binomials who did or did not receive prenatal education orientation.
METHODS: original study based on the application of breastfeeding evaluation form on binomials in joint accommodation (JA) composing of twenty (20) Yes/No questions and the collection of bi categorized independent variables between August/2017-October/2018. Prenatal educational activities with nominal listing of those present and thus creation of the variable was: Prenatal Class Yes/No. Multivariate analysis by Logistic regression were performed with confidence interval at 95%.
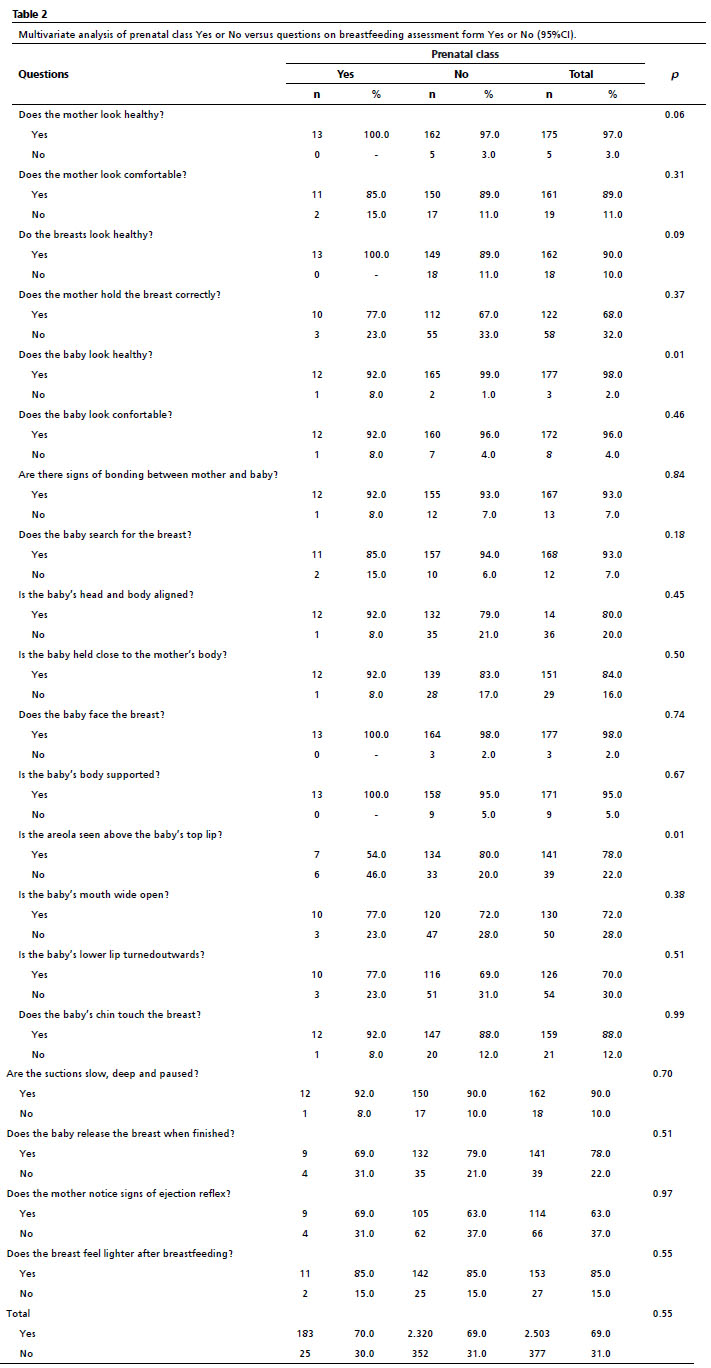
RESULTS: 180 binomials were included, of which 13 (7%) were exposed to prenatal activities and 167 (93%) were not exposed. In the exposed group, there was a predominance of married and multiparous women (p<0.05), in addition to lower educational level and higher rate of maternal pathologies and low birth weight (p<0.05). Regarding the breastfeeding evaluation, of the 20 questions observed, the exposed group was superior in 12 of them. Among the 4 questions about the Newborn's grip, the exposed group was superior in 3 (baby's mouth wide open, lip lowered and chin touching the breast), and the unexposed group was superior in the areola visualization above the upper lip with p<0.05. The limitation found in the study was attributed to quantitative and qualitative heterogeneity between groups.
CONCLUSIONS: prenatal education for breastfeeding did not alternate significantly the performance of binomials on the breastfeeding technique in this study.
Keywords:
Prenatal education, Breastfeeding, Joint accommodation, Regression analysis
RESUMO
OBJETIVOS: comparar avaliação da mamada em binômios cujas mães receberam ou não orientações educativas pré-natais.
MÉTODO: estudo original de casos realizado a partir da aplicação do formulário de avaliação da mamada junto aos binômios no alojamento conjunto (AC), composto por 20 perguntas sim ou não e coleta de variáveis independentes bi categorizadas entre agosto/2017 e outubro/2018. Atividades educacionais pré-natais com listagem nominal dos presentes e assim criação da variável: Aula pré-natal sim/não. Análises multivariadas por Regressão logística, com intervalo de confiança de 95%.
RESULTADOS: 180 binômios foram incluídos, dos quais 13 (7%) foram expostos às atividades pré-natais e 167 (93%) não expostos. No grupo de expostos, houve predomínio de mulheres casadas e multíparas (p<0,05), além de menor nível de escolaridade e maior taxa de patologias maternas e RN com baixo peso (p<0,05). Em relação a avaliação da mamada, das 20 questões observadas, o grupo exposto foi superior em 12 delas. Entre as 4 questões sobre a pega do RN, o grupo exposto foi superior em 3 (boca do bebê bem aberta, lábio evertido e queixo encosta a mama), sendo que o grupo não exposto foi superior no quesito visualização da aréola acima do lábio superior com p<0,05. A limitação encontrada no estudo foi atribuída a heterogeneidade quantitativa e qualitativa entre grupos.
CONCLUSÃO: educação pré-natal para o aleitamento não alterou significativamente o desempenho dos binômios na técnica de amamentação nesse estudo.
Palavras-chave:
Educação pré-natal, Aleitamento materno, Alojamento conjunto, Análise de regressão
IntroductionBreastfeeding is considered one of the pillars for promoting and protecting children’s health all over the world and the superiority of human breast milk as a source of food, defending against diseases and affection is inarguable.
1Therefore, the World Health Organization (WHO) proposed in 1992 the
Iniciativa Hospital Amigo da Criança (IHAC) (Child Friendly Initiative Hospital), whose objective is the implementation of Ten steps for the success of breastfeeding, a protocol that synthesizes the necessary practices to support breastfeeding in hospitals.
2Hospital Guilherme Álvaro (HGA) in Santos-SP is a tertiary center that is a reference in treating pregnant women and high-risk newborns (NB). It was the second hospital to be licensed as a Child Friendly Hospital in Brazil in 1994 and has a long tradition of supporting breastfeeding. Among the pioneer activities in this service, the promotion of breastfeeding during prenatal procedures and the monitoring of breastfeeding when in a joint accommodation (JA), are steps 3 and 5, respectively, of the ten steps of the IHAC.
2In order to accomplish step 3, since 1980, the educational activities are performed in the waiting rooms of prenatal appointments at the HGA. The baby’s first feedings during the JA are monitored to prevent the inherent difficulties in the act of breastfeeding as predicted by step5 of the IHAC.
3As a way to check this breastfeeding monitoring, an instrument was proposed by the IHAC evaluators, which is used in the accreditation of the hospital in the mother-baby binomials. This instrument assigns a score that identifies the difficulties that may affect nursing and serves, in this instance, to check the legitimacy of step 5 in the hospital.
4A lot is discussed on whether or not prenatal education is effective in protecting breastfeeding practice after birth and original studies evaluating this efficacy are always welcome.
5 Therefore, the authors have proposed to perform an original study, in which the result of the application of the breastfeeding evaluation form at the HGA in a JA can be compared between mothers who did and did not receive prenatal educational orientation at the same hospital.
MethodsThis is an original case study obtained from the application of the breastfeeding evaluation form with mother-baby binomials in a joint accommodation at the HGA in Santos (SP, Brazil). All the mothers have signed the Informed Consent Forms, and the study was approved by the Research Ethics Committee at the Institution, as well as the National Research Ethics Committee through the
Plataforma Brasil (Brazil Platform).
Between August 2017 and October 2018, 180 breastfeeding evaluations were performed observationally, without intervention, by trained and supervised students; followed by the collection of independent variables through interviews with the mothers. The inclusion criteria were: healthy mother and NB, admitted in a joint accommodation only, no more than 24 hours of separation, exclusive breastfeeding, and they have signed the Informed Consent Forms.
The 09 bi categorized independent variables according to literature were: mother’s age (above and below 18 years of age),
6,7 mother’s schooling (higher and lower than high school),
8 mother’s marital status (married and single ),
9 Parity (primiparous and multiparous),
10 Number of prenatal consultations (below and above 06),
11 Obstetric pathology (present and absent),
12 Type of childbirth (natural and C-section),
13 Newborn’s sex male and female),
10,14 and Newborn’s weight (above and below 2.500g).
15The 20 yes or no questions from the form in step 5 of the IHAC are: 1. Mother looks healthy. 2. Mother looks comfortable. 3. Breasts look healthy. 4. Mother holds the breast correctly. 5. Baby looks healthy. 6. Baby looks comfortable. 7. Signs of bonding between mother and baby. 8. Baby searches for the breast. 9. Baby’s head and body are aligned. 10. Baby is close to the mother’s body. 11. Baby is facing the breast. 12. Baby is well supported. 13. More of the areola is seen above the upper lip. 14. Baby’s mouth is wide open. 15. Lower lip is turned outwards. 16. Baby’s chin touches the breast. 17. Suckling is slow, deep and paused. 18. Baby releases the breast when finishes breastfeeding. 19. Mother perceives the ejection reflex. 20. Breasts look lighter after breastfeeding.
During the same period, prenatal educational activities were performed with emphasis on the breastfeeding technique, conducted by the students who were not participating of the evaluation at JA, trained and supervised by the nurses’ sector and, with a nominal list of pregnant women who were exposed to these activities, a variable was created: prenatal class yes or no.
The multivariate analysis through logistical regression with the Epi Info™ 7 software with a confidence interval of 95% was performed.
16,17ResultsAfter 84 prenatal activities to 345 pregnant women and 92 visits at the JA in the HGA with 180 breastfeeding evaluations, the sample reached 13 (7%) exposed binomials and 167 (93%) non-exposed binomials to the classes (Tables 1 and 2).
DiscussionIn 2012, Marra
et al.18 described the complications of babies of high-risk pregnant women at the HGA. In this study, the prevalence of low birth weight (43%), admission to intensive care unit (67%) and admissions lasting over 28 days (13%) were considerable. Taking into consideration that such complications were exclusion criteria of our study, valid to presume a considerable amount of the binomials were exposed to the classes being excluded from the JA breastfeeding evaluations.
Besides that, HGA is a state sponsored hospital of the
Sistema Único de Saúde (SUS) (Public Health System), subject to the rules of the
Central de Regulação de Oferta de Serviços de Saúde (CROSS) (Central for Regulation and Supply of Health Services) and, as described by Vilarins
et al.,
19 the CROSS regulation guarantees the balance between supply and demand, which means there is no guarantee that the pregnant woman will give birth in the same hospital where she performed her prenatal evaluations. Therefore, it is possible that part of the pregnant women who took part in the educational activities during prenatal evaluations did not give birth at the same hospital and, for this reason, were not included in this study.
These two factors might explain the numerical difference of 13 (7%) to 167 (93%) between the groups that were exposed and non-exposed to prenatal activities in the breastfeeding evaluations at JA .
19Furthermore, considering the significant difference between the groups of exposed and non-exposed to the classes in the variables of marital status, married (100% to 69% -
p=0.04) and multiparous (92% to 58% -
p=0.02) it is likely that there is also a qualitative discrepancy between the groups with consequent difficulty to analyze.
At the same time, it might be difficult to document the impact of the educational activities in the breastfeeding evaluation due to the fact that this study is made in a Child Friendly Hospital with good success rates in breastfeeding before the study started. To exemplify, Sanches
et al.20 in 2000
, used the breastfeeding evaluation form for the first time at HGA, using the first draft of the form, which was very similar to the current one. The authors opted to use global score percentage of positive answers which was at 60%, it was very low compared to the present data gathered. In that study, no hypothesis outcome was tested and the final values did not appear to be significantly different in any of the independent variables tested. The fact that our study achieved a much higher percentage of positive answers, 70% for the exposed group and 69% for the non-exposed group, shows that the quality of the breastfeeding support at the hospital maintained high, generating an additional difficulty in testing the outcome, given that an alteration higher than 69% is very difficult to attain using this model.
20Another factor that might contribute to a lack of significant association between the observed factors is the kind of statistical analysis performed. A second study with the same form was conducted in Brazil by Vieira
et al.,
21 and these authors opted for an analysis of 05 groups in 04 question forms that are: General observation of the mother, General observation of the baby, Baby position, grip and suckling. We did not opt for this model of outcome because the association between the low number of exposed groups in the sample and the subdivision of outcomes in groups would lead to a lower statistical coherence.
21On the other hand, Carvalhaes
et al.,
4 also performed an analysis based on groups of question and, like us, totaled a positive percentage of 78%. These authors did not test any independent variables nor any outcomes that might alter such results, which made it impossible to compare their results to ours, despite the significant percentage difference was higher.
4As for, Lumbiganon
et al.,
22 in a systematic meta-analysis of 17 studies already had indicated that the prenatal educational activities did not significantly affect the breastfeeding indices. These authors discussed the fact that prospective studies with this kind of question was difficult to conduct. This fact did occur in our study, especially because there is no guarantee that the exposed pregnant women of the educational activities would give birth at the same hospital where the breastfeeding evaluations occurred, and also because of the losses of the non-inclusion.
22Either way, the analysis of the results of our study has showed statistically feasible, and the binomials exposed to the classes obtained superior results in the number of questions (12 and 8 – 60% to 40%) and in the percentage of global positive responses (79% to 60% -
p=0.55), while the non-exposed binomials were better evaluated in the two questions: Areola is seen above the upper lip yes (80% to 54% -
p=0.01) and Baby appears healthy yes (99% to 92% -
p=0.01).
Therefore, it is possible to infer that prenatal education for breastfeeding was not capable of altering the performance of the mother-baby binomials when it comes to breastfeeding technique as measured by the breastfeeding evaluation form in this present study.
Prenatal education for breastfeeding has been performed at the HGA uninterruptedly since 1980, and several health professional teams have been trained to reproduce them since then. The value of these classes is, in our estimation, inarguable regardless of the results this study obtained. We suggest new studies to be made to continue to evaluate that these classes are indeed effective.
References1. Kummer SC, Giugliani ER, Susin LO, Folletto JL, Lermen NR, Wu VY,
et al. Evolução do padrão de aleitamento materno. Rev Saúde Pública. 2000; 34 (2): 143-8.
2. Lamounier JA. Promoção e incentivo ao aleitamento materno: iniciativa Hospital Amigo da Criança. J Pediatr (Rio J). 1996; 72 (6): 36-8.
3. Murahovschi J. Amamentação: da teoria à prática. 1
st Ed. Centro de Lactação de Santos: Fundação Lusíada; 1999,1: 276.
4. Carvalhaes MA de BL, Corrêa CRH. Identificação de dificuldades no início do aleitamento materno mediante aplicação de protocolo. J Pediatr (Rio J). 2003; 79 (1): 13-20.
5. Sandre-Pereira G, Colares LGT, Carmo M das GT, Soares EA. Conhecimentos maternos sobre amamentação entre puérperas inscritas em programa de pré-natal. Cad Saúde Pública. 2000; 16 (2): 457-66.
6. Faleiros FTV, Trezza EMC, Carandina L. Aleitamento materno: Fatores de influência na sua decisão e duração. Rev Nutr. 2006; 19 (5): 623-30.
7. Brasil. Presidência da República, da Casa Civil, Subchefia para assuntos jurídicos. Lei nº 8069, de 13 de julho de 1990. Dispõe sobre o Estatuto da Criança e do Adolescente e dá outras providências. Lei nº 8069, Art. 2º. Brasília (DF): DOU 13 de julho de 1990. [access in 2020 Jun 9]. Available from:
http://www.planalto.gov.br/ccivil_03/leis/l8069.htm8. Damião JDJ. Influência da escolaridade e do trabalho maternos no aleitamento materno exclusivo. Rev Bras Epidemiol. 2008; 11 (3): 442-52.
9. Bernardi JLD, Jordão RE, Filho AAB. Fatores associados à duração mediana do aleitamento materno em lactentes nascidos em município do estado de São Paulo. Rev Nutr. 2009; 22 (6): 867-78.
10. Venancio SI, Monteiro CA. Individual and contextual determinants of exclusive breastfeeding in São Paulo, Brazil: a multilevel analysis. Public Health Nutr. 2006 Feb; 9 (1): 40-6.
11. Brasil. Comissão Permanente de Protocolos de Atenção à Saúde. Portaria nº 342, de 28 de junho de 2017. Dispõe sobre a Atenção à saúde da mulher no Pré-natal, Puerpério e Cuidados ao Recém-nascido. Brasília (DF): DOU 29 de junho de 2017; Seção 8. [access in 2020 Jun 9]. Available from:
https://www.saude.df.gov.br/documents/37101/87400/Aten%C3%A7%C3%A3o+%C3%A0+Sa%C3%BAde+da+Mulher+no+Pr%C3%A9-natal%2C+Puerp%C3%A9rio+e+Cuidados+ao+Rec%C3%A9m-nascido.pdf/a8e8ffb5-1cf2-192d-fbc0-aee6820e35de?t=164864346230012. Furuta M, Sandall J, Cooper D, Bick D. Severe maternal morbidity and breastfeeding outcomes in the early post-natal period: a prospective cohort study from one English maternity unit. Matern Child Nutr. 2016 Oct; 12 (4): 808-25.
13. Weiderpass E, Barros FC, Victora CG, Tomasi E, Halpern R. Incidência e duração da amamentação conforme o tipo de parto: estudo longitudinal no Sul do Brasil. Rev Saúde Pública. 1998; 32 (3): 225-31.
14. Bandeira de Sá NN, Gubert MB, Santos W, Santos LMP. Factors related to health services determine breastfeeding within one hour of birth in the Federal District of Brazil, 2011. Rev Bras Epidemiol. 2016; 19 (3): 509-24.
15. Motta MEFA, Da Silva GAP, Araújo OC, Lira PI, Lima MDC. Does birth weight affect nutritional status at the end of first year of life? J Pediatr (Rio J). 2005; 81 (5): 377-82.
16. Dean AG, Dean JA, Burton AH, Dicker RC. Epi Info: a general-purpose microcomputer program for public health information systems. Am J Prev Med. 1991; 7 (3): 178-82.
17. Coutinho LMS, Scazufca M, Menezes PR. Métodos para estimar razão de prevalência em estudos de corte transversal. Rev Saúde Pública. 2008; 42 (6): 992-8.
18. Marra NBF, Sousa FLP, Scarpelini M, Garcia JM, Marçal VMG, Figueiredo PG,
et al. PP139. The elective prematurity birth and its perinatal effects of syndromes in hypertensive pregnancy. Pregnancy Hypertens. 2012 Jul; 2 (3): 315.
19. Vilarins GCM, Shimizu HE, Gutierrez MMU. A regulação em saúde: aspectos conceituais e operacionais. Saúde Debate. 2012; 36 (95): 640-7.
20. Sanches MTC, Buralli KO. Dificuldades iniciais na amamentação: enfoque fonoaudiológico [tese]. São Paulo: Faculdade de Saúde Pública da Universidade de São Paulo; 2000.
21. Vieira A, Costa AR, Gomes PG. Boas práticas em aleitamento materno: Aplicação do formulário de observação e avaliação da mamada. Rev Soc Bras Enferm Ped. 2015; 15 (1): 13-20.
22. Lumbiganon P, Martis R, Laopaiboon M, Festin MR, Ho JJ, Hakimi M. Antenatal breastfeeding education for increasing breastfeeding duration. Cochrane Database Syst Rev. 2012 Sep; 9: CD006425.
Received on October 5, 2020
Final version presented on February 28, 2022
Approved on June 7, 2022
Authors’ contributionBaldin PEA: data analysis, writing and editing. Pedrosa FG and Luiz MFC: Breastfeeding evaluation form application, database research, writing and editing. Domingues GR, Reis MN and Gonçalves TH: Prenatal activities, database research, writing and editing. All of the authors have approved the final version of the article, and declare no conflict of interest.


 ; Fernanda Gonzalez Pedrosa2
; Fernanda Gonzalez Pedrosa2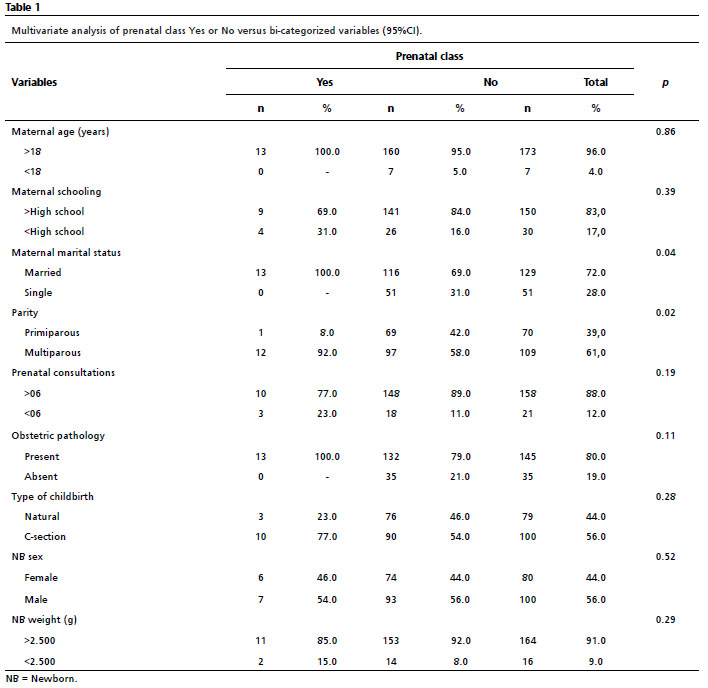






 Ler em português
Ler em português