ABSTRACT
OBJECTIVES: to analyze a decade of spatio-temporal behavior of pertussis in Brazil and its epidemiological characteristics.
METHODS: ecological time series study of pertussis cases and deaths from the Notifiable Diseases Information System in Brazil (2010-2019). The method of generalized linear analysis of Prais-Winsten and the Kernel analysis were used.
RESULTS: 32,849 cases were reported, of which 466 (1.42%) evolved to death, with a prevalence of 1.63/100,000 inhabitants and a mortality rate of 0.023/100,000 inhabitants. In the temporal analysis, the cyclical behavior of pertussis was evidenced, with trend variations in the period in 2014. Most cases occurred in children under 1 year of age (60.16%, p<0.01), sex female (55.28%, p=0.066) and white (48.42%, p=0.14). The largest share of deaths was in children aged <1 year (98.07, p<0.01), females (56.01%, p=0.066) and whites (43.78%, p=0.14). In the Kernel of prevalence, the South, Southeast and Northeast regions stood out with high density; while for mortality, the Southeast and Northeast stood out.
CONCLUSIONS: the cyclical behavior of pertussis was observed, with a decreasing trend in recent years and the concentration of cases in children. This reinforces the importance of strengthening the population's immunization process.
Keywords:
Whooping cough, Vaccine-preventable diseases, Spatial analysis
RESUMO
OBJETIVOS: analisar uma década do comportamento espaço-temporal da coqueluche no Brasil e as suas características epidemiológicas.
MÉTODOS: estudo ecológico de série temporal dos casos e óbitos por coqueluche do Sistema de Informação de Agravos de Notificação no Brasil (2010-2019). Utilizou-se o método de análise linear generalizada de Prais-Winsten e a análise de Kernel.
RESULTADOS: notificaram-se 32.849 casos, desses 466 (1,42%) evoluíram para óbito, com prevalência de 1,63/100.000 habitantes e coeficiente de mortalidade de 0,023/100.000 habitantes. Na análise temporal, evidenciou-se o comportamento cíclico da coqueluche com variações de tendência no período em 2014. A maioria dos casos ocorreu em menores de 1 ano (60,16%, p<0,01), sexo feminino (55,28%, p=0,066) e brancos (48,42%, p=0,14). A maior parcela dos óbitos foi em crianças <1 ano (98,07, p<0,01), sexo feminino (56,01%, p=0,066) e brancos (43,78%, p=0,14). No Kernel da prevalência, destacaram-se as regiões Sul, Sudeste e Nordeste com alta densidade; enquanto para mortalidade, sobressaíram-se Sudeste e Nordeste.
CONCLUSÃO: observou-se o comportamento cíclico da coqueluche, com tendência de decréscimo nos últimos anos e a concentração de casos no público infantil. O que reforça a importância de fortalecer o processo de imunização da população.
Palavras-chave:
Coqueluche, Doenças preveníveis por vacina, Análise espacial
IntroductionPertussis is an acute infectious disease, of compulsory notification and reemerging, of global distribution, which is caused by the bacterium
Bordetella pertussis. It mainly affects the respiratory tract of human beings, who are the only natural reservoir.
1,2 Despite being a vaccine-preventable disease by the pentavalent vaccine (DTP + Hib + Hep.B), it is still considered a public health problem because it is responsible for significant infant morbidity and mortality.
1,3,4According to the World Health Organization (WHO), it is estimated that around 30-50 million cases and 300,000 deaths are reported worldwide per year, the majority of which involving children under six months of age and infants; it may manifest in its severe form and culminate in the negative outcome of death.
5Furthermore, for Trevizan e Coutinho
6 e Bricks,
7 the increase in cases of pertussis is particularly important, once it is possible to identify that its prevalence is concentrated in children under one year of age (about 70% of cases), and it also occurs more frequently in three-month-old children, as they have not yet received all three doses of the vaccine. From a clinical perspective, the main symptom presented is a persistent cough which lasts from 10 to 14 days, in addition to paroxysmal cough, vomiting, cyanosis and the presence of leukocytosis above 20,000 cells/mm, presented by the laboratory test.
2,4Historically, the coverage expansion of the triple bacterial and tetravalent vaccines from the 1990s onwards contributed significantly to the reduction in the prevalence of pertussis in the country, from 10.6 cases per 100 thousand inhabitants (inhab) at the beginning of the decade to 0.32/100 thousand inhab, once the vaccination coverage increased from 70% to over 95%. However, in 2011 there was an unexpected and sudden increase in pertussis cases, which remained through 2013 and 2014. Studies indicate that this increase was probably due to better laboratory diagnosis with the introduction of biomolecular techniques, the improvement of health surveillance, the decrease in immunity conferred by the vaccine and the increase in asymptomatic carriers.
3,8Thus, the reemergence of this disease is considered a public health problem in Brazil, because it was once a controlled disease with the vaccine available for free in the Unified Health System (SUS), but it remains an important cause of morbidity and mortality, especially in children under one year of age.
2,8Given the above, this article is justified due to the need for updates on the scope of scientific productions on pertussis and its geographical distribution in Brazil. In addition, it seeks to support the decision-making process of public health managers in the formulation and implementation of strategies to control its cases in the country’s priority areas. Thus, this study aims to analyze a decade of the spatiotemporal behavior of pertussis in Brazil and its epidemiological characteristics.
MethodsThis is an ecological time series epidemiological study, based on secondary data obtained from the Notifiable Diseases Information System (SINAN – Portuguese acronym) of the SUS Department of Informatics (DataSUS – Portuguese acronym), referring to pertussis cases and deaths in Brazil from 2010 to 2019; such information is available in the “Epidemiological and Morbidity” tab.
9Data referring to the population are based on population estimates made by the Brazilian Institute of Geography and Statistics (IBGE – Portuguese acronym), available in DataSUS under the tab “Demographics and Socioeconomics of the resident population”.
9 For the tabulation of cases, the variable “Federative Unit (FU) of residence” was selected for the row section and, in the column section, the other variables were selected. Regarding the information on deaths, the same methods were applied, adding the filter of “deaths” in the variable of “evolution of the case” in the section “available selections” on the website.
9Geographically, Brazil is located in South America and has a territorial area of 8,510,345,538 km
2. It is currently administratively divided into 5,570 municipalities, 26 states and the Federal District, distributed in five geographic regions (North, Northeast, Southeast, South and Midwest), with an estimated population of 211,755,692 inhab for the year 2020.
10The variables selected for the study were: year, sex, age group, race/color, pregnant woman, confirmation criteria, case evolution, geographic region and FU, according to the place of residence and deaths. This selection aimed to analyze the behavior of the disease in the studied localities in a sociodemographic manner. Subsequently, data were organized in Microsoft Office Excel 2016
® spreadsheets and analyzed in TerraView 4.2.2, QGIS 3.12.2 and R 3.6.3 software with the prais package.
The absolute and relative frequencies of each variable were calculated, as well as the prevalence rate and the mortality coefficient by sex (male and female) and by the total number of cases, both per 100,000 inhab. In addition, the Chi-Square test was used to verify statistical associations between the different categories of variables, with a statistical significance level of 5% (
p<0.05) being adopted to characterize the epidemiological scenario of pertussis in Brazil (Table 1).
During the first stage of the process, the statistical analysis sought to carry out a study of the temporal trend of the prevalence rate and the mortality rate per 100,000 inhabitants in order to analyze the temporal evolution of these indicators over the period studied. In order to achieve the goal numbers, the Prais-Winsten generalized linear regression analysis model was used, in which years of study were considered as independent variables (X) while prevalence and mortality rates were considered as dependent variables (Y). A logarithmic transformation was performed to smooth the Y values so that the model could accurately detect the variations and estimate the values of b1. After finding the values of b1, in order to obtain the rates of change, the values were applied to the following formula
11,12:
From the analysis of the change rate, it is possible to infer that a trend is increasing when the rate of change is positive (+), decreasing when the rate is negative (-) or stationary when there is no significant difference between the value obtained and zero.
11,12 Then, confidence intervals (CI) were calculated, applying the following formula:
Minimum b and maximum b values were obtained through the CI generated by the R software during the statistical analysis and then applied to the formula. The values of minimum b and maximum b correspond, respectively, to the minimum and maximum points of the CI.
During the second stage of the study, the spatial analysis sought to provide a visualization of the geographic distribution of the disease in the country, measuring its properties and relationships, enabling the visualization of existing patterns.
13 The use of Geographic Information Systems (GIS) has proved to be an important tool for the monitoring and control of diseases, as it contributes to the prevention of diseases and injuries, allows for the evaluation of the control measures used and guarantees updated information on the epidemiological situation and the distribution in the geographic space.
14In this study, the Kernel density tool was used as a strategy to enable the visualization and analysis of the behavior of density patterns and spatialization of cases and deaths from pertussis in Brazil. This is a method of statistical analysis that allows the estimate of density curves and their convertion into continuous surface data through the interpolation of point data per unit area.
The Kernel density estimator is calculated according to the Silverman equation,
15 in which is χ is the coordinate vector that represents the location of the analyzed point;
n is the total number of analyzed points;
h is the bandwidth;
K is the Kernel function; and
Xi is the vector of the i-th coordinate which represents each analyzed point in relation to the estimated one.
By concept, a surface that is smoothly curved can be fitted over each point, the value of the surface being highest at its location and decreasing with increasing distance from the point until it reaches zero at the end of the search radius. The density in each output raster cell is calculated by adding the values of all Kernel surfaces where they overlap the center of the raster cell.
The free license QGIS software was used to calculate the Kernel maps by applying the heatmap tool and the quartic function of Silverman.
15 The stratification of the classes for the distribution maps and Kernel occurred by quantile.
ResultsWithin the period from 2010 to 2019, 32,849 cases and 466 deaths from pertussis were identified in Brazil, with an average prevalence of 1.63 cases per 100,000 inhab and an average mortality rate of 0.023 deaths/100,000 inhab.
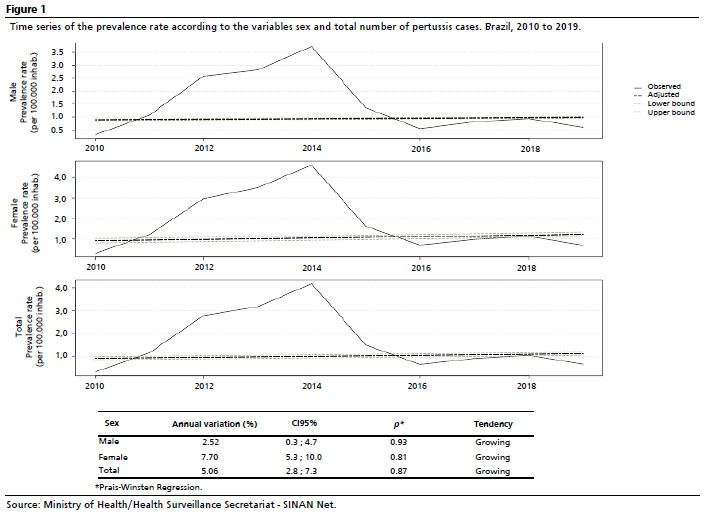
In the generalized linear regression analysis of Prais-Winsten, it was observed that the percentage of annual increase in the pertussis prevalence rate in Brazil, within the analyzed period, was estimated at 2.52% (CI95%=0.3-4.7) in male individuals (showing an increase tendency). Regarding females, the tendency was similar, with a percentage increase in 7.7% (CI95%=5.3-10), as well as for both male and female individuals, showing a percentage increase in 5.06% (CI95%=2.8 - 7.3) (Figure 1).
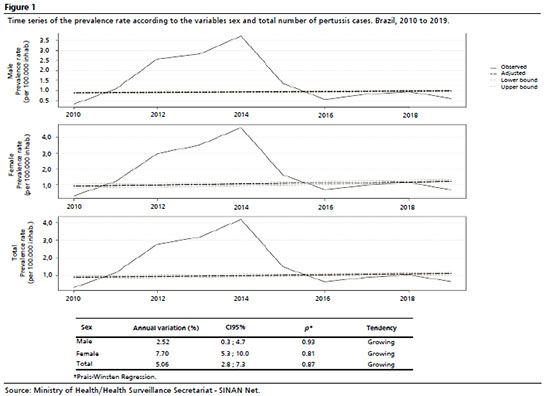
Still in Figure 1, one can see that the temporal trend of the prevalence rate by sex and the total number of cases show a varied behavior over the years. The chart demonstrates the cyclical behavior of pertussis, once it is possible to notice that there is a trend of increasing prevalence between the years 2010 to 2014, then the scenario changes in the following couple of years until 2016, when there is an increase in this rate again, which soon decreases again in the following years (from 2018 to 2019).
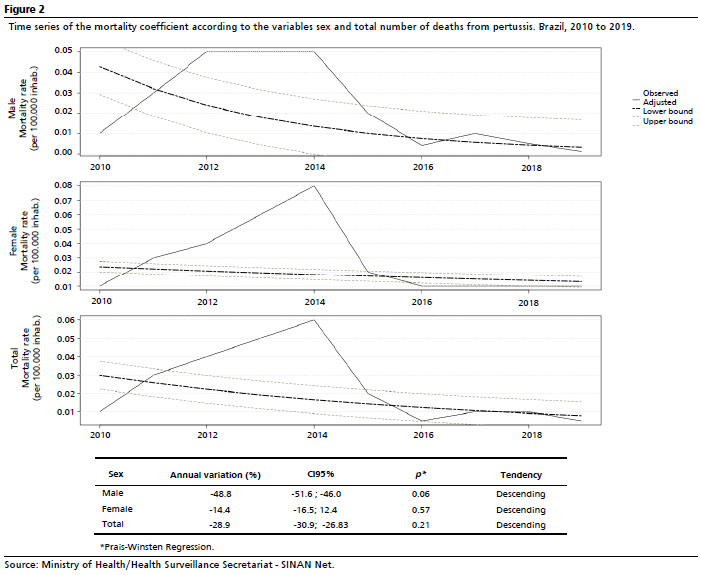
Regarding the percentage of anual decrease in the mortality rate, it was estimated at -48.8% (CI95%=-51.6 to -46.0) in male individuals with a tendency to further decrease. The analysis for females also showed a decreasing trend of -14.4% (CI95%=-16.5 to -12.4), and the total number of deaths decreased in -28.9% (CI95%=-30.9 to -26.83). The cyclical behavior of pertussis in terms of deaths can also be noticed; even though there was a general decrease trend in the period, it is observed that there were years marked by an increase, followed by a decrease in the aforementioned rate. The peak for the pertussis mortality rate occurred in 2014 (Figure 2).
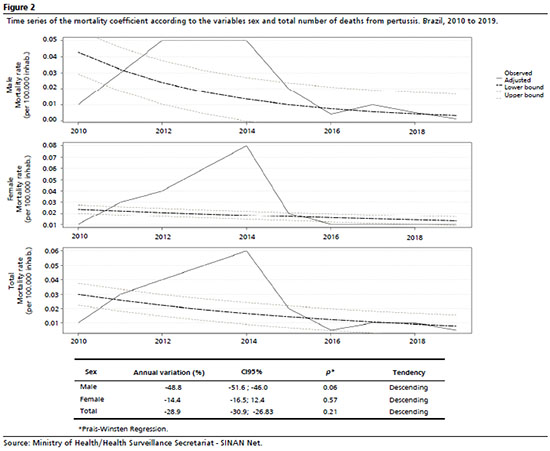
Table 1 presents an assessment of the epidemiological characterization of pertussis cases and deaths in the country: the majority occurred in female individuals (55.28%), under one year of age (60.16%) and of white race/color (48.42%). The most used confirmation criterion was the clinical one (50.74%); the criterion of being pregnant did not apply in most cases (92.23%); most cases evolved to cure (90.96%), while 466 (1.42%) individuals had death as a result of the reported disease.
Regarding the epidemiological characterization of deaths from pertussis in Brazil, it was found that the majority were female (56.01%), under one year of age (98.07%), of white race/color (43.78%), the confirmation criterion were lab tests (49.14%) and the pregnant criterion did not apply to any cases (Table 1).
It is worth noting that the Chi-square association test showed significance between the characterization variables and the situation of the individuals for the age group (
p<0.01) and for the confirmation criterion (
p<0.01). Concerning the age group, there was a high number of cases and deaths in children under one year of age. For the other variables, there was no statistically significant association, and concerning the case evolution and pregnant women, there was no application of the test, because for these variables there are no data on deaths in any categories.
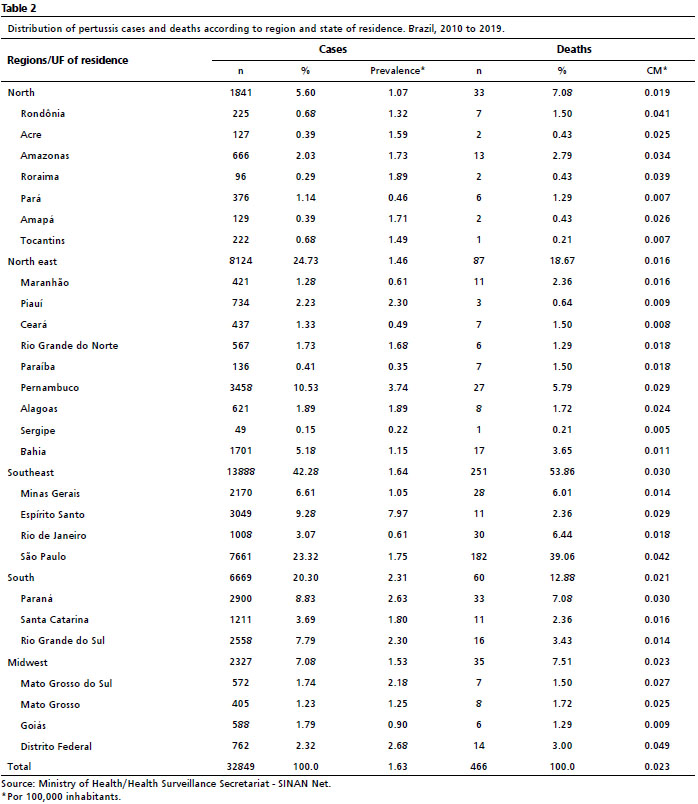
As shown in Table 2, it was observed that the Brazilian geographic region of residence that registered the most cases and deaths from pertussis in the studied period was the Southeast region (42.28% and 53.86%, respectively), followed by Northeast (24.73 % and 18.67%, respectively), South (20.30% and 12.88%, respectively), Midwest (7.08% and 7.51%, respectively) and North (5.60% and 7.08%, respectively).
Regarding the prevalence of the disease according to the geographic regions in Brazil, the South region stood out with 2.31 cases per 100 thousand inhab, followed by the Southeast (1.64/100 thousand inhab), Mid-West (1.53/100 thousand inhab), Northeast (1.46/100 thousand inhab) and North (1.07/100 thousand inhab). Regarding the mortality rate, the Southeast region had a mortality of 0.03 deaths per 100,000 inhab, while the other regions had an MR of 0.02 deaths per 100,000 inhab (Table 2).
Regarding the analysis by FU, Espírito Santo stood out with the highest prevalence in the studied period (7.97/100 thousand inhab), followed by Pernambuco (3.74/100 thousand inhab), Federal District (2.68/100 thousand inhab), Paraná (2.63/100 thousand inhabitants) and Rio Grande do Sul (2.30/100 thousand inhabitants). In contrast, the five FUs with the lowest prevalence were Sergipe (0.22/100,000 inhab), Paraíba (0.35/100,000 inhab), Pará (0.46/100,000 inhab), Ceará (0.49/100 thousand inhab) and Rio de Janeiro (0.61/100 thousand inhab) (Table 2).
Concerning mortality rates, it was found that the FUs with the highest ones were Distrito Federal (0.059/100,000 inhab), São Paulo (0.042/100,000 inhab), Rondônia (0.041/100,000 inhab), Roraima (0.039/100,000 inhab.) and Amazonas (0.034/100 thousand inhab); the lowest ones were found in Sergipe (0.005/100,000 inhab), Tocantins (0.007/100,000 inhab), Pará (0.007/100,000 inhab), Ceará (0.008/100,000 inhab) and Goiás (0.009/100,000 inhab) (Table 2).
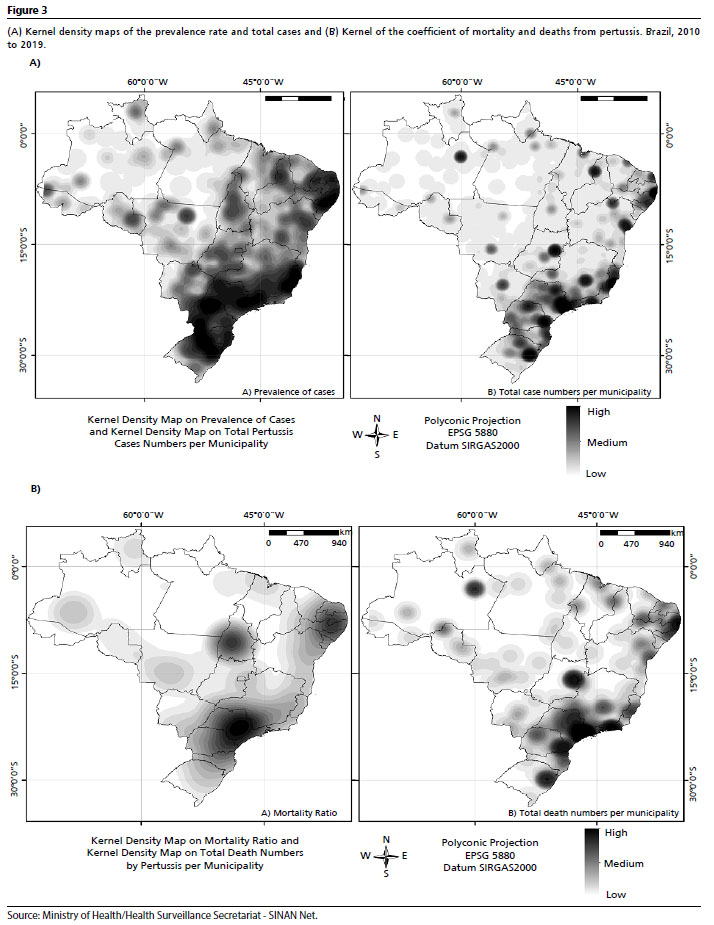
As for the Kernel density maps of pertussis prevalence rates (Figure 3 A-A) and total cases (Figure 3 A-B), the concentration of areas with a higher density is observed in states in the South, Southeast and Northeast regions. It is also worth mentioning the presence of a cluster of high concentration of cases in the coastal area of Pernambuco and on the borders with the states of Paraíba and Alagoas, as well as in Espírito Santo, São Paulo, Paraná, Santa Catarina and part of Rio Grande do Sul. In the Kernel map with the total number of cases (Figure 3 A-B), there was a similarity when compared with the prevalence rate map, having the Federal District and the border between Piauí and Maranhão in addition to the FUs mentioned above (Figure 3 A-A).
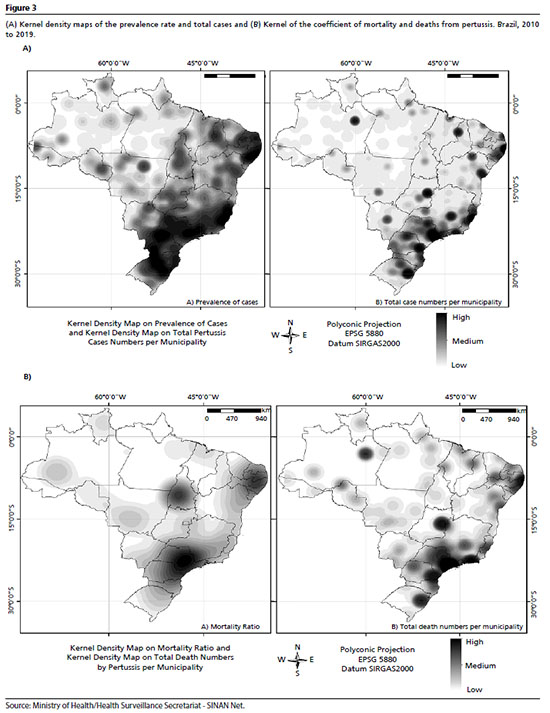
In the spatial analysis of mortality, high-density pertussis mortality clusters were observed in São Paulo (Southeast) and Pernambuco (Northeast), and a medium-density cluster was found in Tocantins (North). In the spatialization of the absolute frequency of deaths, a concentration of high-density clusters was observed in Pernambuco (Northeast), Federal District (Midwest), São Paulo (Southeast) and Rio de Janeiro (Southeast), while Rio Grande Sul (South), Paraná (South) and Amazonas (North) showed medium and low density clusters (Figure 3 B).
Comparing the prevalence rate (Figure 3 A-A) and the mortality rate maps (Figure 3 B-A) for pertussis, it was observed that the states of Pernambuco and São Paulo are present in both maps with high-density clusters for both indicators. When assessing the maps of total cases (Figure 3 A-B) and total deaths (Figure 3 B-B), it was observed that the areas in common were São Paulo, Espírito Santo, Distrito Federal, Pernambuco, Paraná and Rio Grande do Sul. In both maps, the North region presented clusters of medium and low density.
DiscussionThe present study presents data on an increase in pertussis cases in Brazil from 2010 to 2014, which was followed by a downward trend in the following years. This may be related to the improvement of diagnosis confirmation mechanisms in laboratories, through the introduction of biomolecular techniques in the routine of such institutions, which brought quick and accurate confirmation; also, the heterogeneous vaccination coverage and the temporal behavior of the disease itself.
16-18 The decrease, in turn, may be related to the introduction of the dT vaccine for pregnant women and healthcare professionals, as well as the strengthening of chemoprophylaxis measures for suspected cases and the epidemic cycle of the disease.
18In addition, pertussis has a cyclic behavior: it presents itself in epidemic peaks every three to five years among the population, which may explain its temporal variation,
1 as identified in this study. Another factor that strengthens the occurrence of pertussis cases is the incompleteness of the vaccination schedules of pregnant women, compromising the natural passive immunization of babies through the placenta and the need to comply with the recommended number of doses for children.
17The prevalence of pertussis in children and adolescents may be related to the non-compliance with the immunization schedules among this group, causing a deficiency in immunity and favoring the spread of the bacillus responsible for the disease.
19 According to the epidemiological bulletin,
1 from 2010 to 2014, there was a significant increase in the number of pertussis cases in children aged one to nine years, who should be completely immunized according to the aforementioned vaccination schedule; such data denote an important public health problem which requires special attention.
19Another concern for health authorities is that pertussis is still a cause of infant morbidity and mortality, as children under one year of age are the most susceptible group to the disease. This is because children under one year of age have not yet completed the recommended doses of the vaccine, in addition to having their immune system still under development
19 and, as shown in this and other studies, most cases and deaths from pertussis occur in this age group. Considering that the only reservoir of the disease is the human being, it is understood that transmission to babies occurs through people who are close, which highlights the need for immunization as a way to protect the whole population.
20Furthermore, despite advances in filling out notification forms and health information systems, there is a problem with the high percentage of ignored participants in some variables, as seen in this study regarding race/color. Such situation may occur due to the lack of knowledge or unpreparedness of health professionals on the relevance of such information for health management and research.
21It was noticed that, although pertussis has a heterogeneous geographic distribution in Brazil, there is a greater concentration of the disease in the Southeast, Northeast and South regions, which corroborates the results from another study,
18 and it may be associated with the population and climatic characteristics of these regions.
22,23 A survey carried out between 2006 and 2013,
24 reported the Southeast and Northeast regions to be areas with the highest lethality for pertussis, where most deaths happened with children under one year of age, while the South had a lower lethality; such findings corroborate the results of the current research.
Regarding the Southeast region, such data can be explained by its tropical weather and how much it varies throughout the year; however, during spring and summer periods, the region reaches peaks above 30°C, which favors the development of the bacteria, in addition to its population density.
16,25 One the other hand, the Northeast region presents a humid coastal climate, with high temperatures which enables the development of bacteria, in addition to being a very touristic region, a fact that can contribute to the proliferation of
Bordetella pertussis16,26Regarding the South region, it may be related to its subtropical climate and the occurrence of cases in adolescents and adults who might have reduced their vaccine protection over time, which favors the circulation of bacteria among the population, mainly affecting children who have not yet completed their vaccination schedule.
6,26 The North region presents probably the lowest record in the study, which is probably associated with its lower population density, since although it is the largest region in the country, a major part of its territory is occupied by the Amazon Forest,
16,26 in addition to the underreporting of cases and deaths.
In a study on Hospitalizations for Conditions Sensitive to Primary Care (ICSAP -Portuguese acronym) of children under one year of age in São Paulo, between 2008 and 2014,
27 significant numbers of hospitalizations for pertussis were evidenced, and the need for greater attention to this disease was emphasized. Hence, although it has a different object of study, the work emphasizes the importance of expanding care with the immunization of adults and children, as the disease can present a worse scenario, with the need for hospitalization and, in the worst of the outcomes, evolve to death.
One of the limitations of this research is the possibility of reproducing biases present in the notifications of cases and deaths recorded in SINAN, which may not reliably express the country’s reality on the increase, decrease and stability of cases and deaths from pertussis. Thus, studies that also dealt with pertussis in Brazil were searched in the literature to support the interpretation and discussion of these results.
The study shows the need for expansion of healthcare actions as well as surveillance for the identification, diagnosis and treatment of the disease in a timely manner, in order to avoid death outcome. Furthermore, it is necessary to enhance the performance of the National Immunization Program to expand vaccination within the target population and/or ensure that the vaccination schedule is complete,
3,5,8,28 given the current scenario of expansion of the anti-vaccination movement in the world.
29Finally, from the time-space analyzes carried out, it was possible to observe the behavior of pertussis in the country, marked by fluctuations in the increases and decreases in prevalence and mortality rates over time, usually every three or five years, which displays the cyclical presentation of the disease. In addition, despite a downward trend in these rates in recent years, it is important to strengthen the attention of health authorities and the population to pertussis, in order to avoid a new increase in cases and deaths in the country from a vaccine-preventable disease.
References1. Ministério da Saúde (BR). Secretária de Vigilância em Saúde. Coqueluche no Brasil: análise da situação epidemiológica de 2010 a 2014. Boletim epidemiológico. Brasília (DF): Ministério da Saúde; 2015 [access in 2021 fev 9]; 46 (39): 1-8. Available from:
https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/c/coqueluche/arquivos/boletim-epidemiologico-da-coqueluche-brasil-2010-a-2014.pdf2. Chadi PF. Vacina dTpa em gestantes na redução da coqueluche na criança [tese]. São Paulo: Faculdade de Medicina de Botucatu da Universidade Estadual Paulista “Júlio de Mesquita Filho”; 2018.
3. Medeiros ATN, Cavalcante CAA, Souza NL de, Ferreira MAF. Reemergência da coqueluche: perfil epidemiológico dos casos confirmados. Cad Saúde Coletiva. 2017; 25 (4): 453-9.
4. Ribeiro RMM, Mendes VA. Situação epidemiológica da coqueluche no Distrito Federal entre 2007 e 2016. Rev Bioét. 2019; 27 (4): 764-71.
5. Santos AMC, Medeiros KC. Situação epidemiológica da coqueluche em Salvador - Bahia nos anos de 2012 a 2014. Rev Enferm Contemp. 2015; 4 (2): 145-51.
6. Trevizan S, Coutinho SED. Epidemiological profile of pertussis in Rio Grande do Sul state, Brazil: a study of the correlation between incidence and vaccine coverage. Cad Saúde Pública. 2008; 24 (1): 93-102.
7. Bricks LF. Pertussis: novas estratégias de vacinação para prevenção de uma antiga doença. J Health Biol Sci. 2013; 1 (2): 73-83.
8. Verçosa RCM, Pereira TS. Impacto da vacinação contra pertussis sobre os casos de coqueluche. Rev Enf UFPE. 2017; 11 (9): 3410-8.
9. Ministério da Saúde (BR). Departamento de Informática do Sistema Único de Saúde (DataSUS). TabNet [Internet]. Brasília (DF); 2022. [access in 2021 jan 30]. Available from:
https://datasus.saude.gov.br/informacoes-de-saude-tabnet/10. Instituto Brasileiro de Geografia e Estatística (IBGE). Panorama Brasil. IBGE Cidades. 2021 [access in 2021 mar 13]. Available from:
https://cidades.ibge.gov.br/brasil/panorama11. Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saúde. 2015; 24 (3): 565-76.
12. Cunha AP, Cruz MM, Torres RMC. Tendência da mortalidade por aids segundo características sociodemográficas no Rio Grande do Sul e em Porto Alegre: 2000-2011. Epidemiol Serv Saúde. 2016; 25 (3): 477-86.
13. Druck S, Carvalho MS, Câmara G, Monteiro AVM (eds). Análise Espacial de Dados Geográficos. Brasília (DF): EMBRAPA; 2004.
14. Oliveira ECA, Silva IEP, Ferreira RJ, Guimarães RJPS, Gomes ECS, Barbosa CS. Mapping the risk for transmission of urban schistosomiasis in the Brazilian Northeast. Geospat Health. 2020 Dec; 15 (2).
15. Silverman BW. Density Estimation for Statistics and Data Analysis. 1
st ed. Londres: Chapman and Hall; 1986. p. 8-11.
16. Secretaria de Estado da Saúde de São Paulo. Situação epidemiológica atual da coqueluche - Cenário global. BEPA. Bol Epidemiol Paul. 2012; 9 (97): 26-35.
17. Castro HWV, Milagres BS. Perfil epidemiológico dos casos de coqueluche no Brasil de 2010 a 2014. Univ Ciênc Saúde. 2017; 15 (2): 81-90.
18. Oliveira DR, Alves RV, Pereira MCCQ, Gonçalves MAP, Matos ZM, Garcia KKS,
et al. Coqueluche. Bol Epidemiol [Internet]. 2019 set; 50 (esp):10-11. In: Vigilância em Saúde no Brasil 2003-2019: da criação da Secretaria de Vigilância em Saúde aos dias atuais. [acesso em 2021 jun 18]. Disponível em:
https://ameci.org.br/wp-content/uploads/2019/09/boletim-especial-21ago19-web.pdf19. Silva LMN, Graciano AR, Montalvão PSD, França CMJ. O atual e preocupante perfil epidemiológico da coqueluche no Brasil. Rev Educ Saúde. 2017; 5 (1): 21-7.
20. Willemann MCA, Goes FCS, Araújo ACM, Domingues CMAS. Adoecimento por coqueluche e número de doses administradas de vacinas Pertussis. Epidemiol Serv Saúde. 2014; 23 (2): 207-14.
21. Santos ABS, Coelho TCB, Araújo EM. Identificação racial e a produção da informação em saúde. Interface (Botucatu). 2013; 17 (45): 341-5.
22. Mançaneira JF, Benedetti JR, Zhang L. Hospitalizations and deaths due to pertussis in children from 1996 to 2013. J Pediatr (Rio J). 2016; 92 (1): 40-5.
23. Soares JS, Brito LCF, Coêlho MB, Costa RKE, Oliveira EH. Análise do perfil epidemiológico dos casos de coqueluche no estado do Piauí no período de 2013 a 2018. Res Soc Dev. 2021; 10 (2): 1-7.
24. Gryninger LCF. Estudo descritivo de série histórica da coqueluche no Brasil no período de 2006 a 2013 [dissertação]. São Paulo: Faculdade de Medicina da Universidade de São Paulo; 2016.
25. Instituto Brasileiro de Geografia e Estatística (IBGE). Área Territorial Brasileira [Internet]. 2016 [access in 2021 jul 5]. Available from:
http://www.ibge.gov.br/home/geociencias/areaterritorial/principal.shtm26. Instituto Nacional de Meteorologia (INMET) [Internet]. Tempo. 2016 [access in 2021 jul 5]. Available from:
http://www.inmet.gov.br/portal/index.php?r=home2/page&page=tempo.27. Lôbo IKV, Konstantyner T, Areco KCN, Vianna RPT, Taddei JAAC. Internações por Condições Sensíveis à Atenção Primária de Menores de um ano, de 2008 a 2014, no estado de São Paulo, Brasil. Ciênc Saúde Coletiva. 2019; 24 (9): 3213-26.
28. Dias FCF, Liberato AA, Lobo PHP, Gusmão KE, Santana VMX, Oliveira VS,
et al. Perfil epidemiológico da coqueluche na região norte do Brasil entre 2012 e 2015. Rev Patol Tocantins. 2017; 4 (2): 72-6.
29. Figueiredo A, Simas C, Karafillakis E, Paterson P, Larson HJ. Mapping global rends in vaccine confidence and investigating barriers to vaccine uptake: a large-scale retrospective temporal modelling study. Lancet. 2020 Sep; 396 (10255): 898-908.
Received on July 21, 2021
Final version presented on June 8, 2022
Approved on June 10, 2022
Authors’ contributionStudy design and planning: Silva LR, Arruda LES, Freitas MVA, Santos ISF, Oliveira ECA. Data collection: Silva LR, Ferreira JF, Arruda LES, Vasconcelos AD, Freitas MVA, Santos ISF, Silva JTL, Silva MGG, Teixeira CMB, Lira G, Oliveira ECA. Data analysis and interpretation: Silva LR, Ferreira JF, Arruda LES, Vasconcelos AD, Santos ISF, Silva JTL, Silva MGG, Teixeira CMB, Lira G, Oliveira ECA. Writing of the manuscript: Silva LR, Ferreira JF, Arruda LES, Vasconcelos AD, Freitas MVA, Santos ISF, Silva JTL, Silva MGG, Teixeira CMB, Lira G, Oliveira ECA. Critical review of the manuscript: Silva LR, Ferreira JF, Freitas MVA, Oliveira ECA. All authors approved the final version of the article and declared that there was no conflict of interest.


 ; Ricardo José Ferreira 2
; Ricardo José Ferreira 2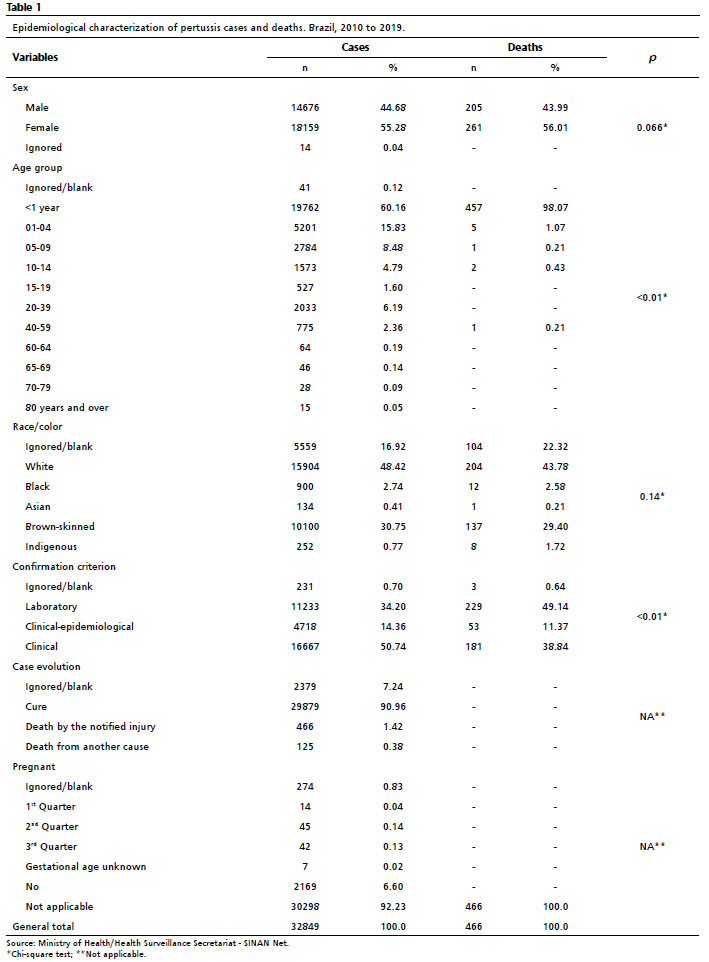







 Ler em português
Ler em português