ABSTRACT
OBJECTIVE: to assess post-traumatic stress disorder (PTSD) symptoms in pregnant women diagnosed with congenital anomaly.
METHODS: his is a quantitative and cross-correlational study. The sample consisted of 111 pregnant women diagnosed with congenital anomaly between 2013 and 2014. We used a semi-structured questionnaire and the Impact of Events Scale - Revised (IES-R). For statistical analysis, the chi-square test, Student's t test or Mann-Whitney test, Cronbach Alpha coefficients, Pearson's correlation and simple linear regression models.
RESULTS: viable congenital anomalies corresponded to 66.6%, and non-viable, to 33.3%. The average of all areas of IES-R, as well as the sum of matters concerning IES-R, were high in all pregnant women diagnosed with congenital anomaly. Using a cut of 5.6 units in the IES-Rtotal score, we found that 46.8% of pregnant women diagnosed with a congenital anomaly showed PTSD symptoms; however, symptoms were more frequent among pregnant women diagnosed with non-viable congenital anomaly (64.9%). The IES-R intrusion and hyperstimulation dimensions were more correlated. We observed a decreasing connection with PTSD symptoms in relation to the time of the notification of congenital anomaly diagnosis.
Keywords:
PTSD symptoms were more frequent in pregnant women diagnosed with non-viable congenital anomaly.
RESUMO
OBJETIVOS: avaliar os sintomas do Transtorno de Estresse Pós-Traumático (TEPT) em gestantes com diagnóstico fetal de anomalia congênita.
MÉTODOS: estudo quantitativo e transversal-correlacional. A amostra foi composta por 111 gestantes com diagnóstico de anomalia, entre 2013 a 2014. Foi utilizado um questionário semiestruturado e a Escala do Impacto do Evento - Revisada (IES-R). Para a análise estatística o teste Qui quadrado, t de Student ou Mann-Whitney, coeficientes alfa de Cronbach, correlação de Pearson e modelos de regressão linear simples.
RESULTADOS: as anomalias congênitas viáveis corresponderam a 66,6% e as inviáveis, a 33,3%. A média de todos os domínios da IES-R como a soma das questões dos domínios da IES-R foram altas nas gestantes com diagnóstico de anomalia congênita. Ao se utilizar um corte de 5,6 unidades no escore total da IES-R, 46,8% de todas as gestantes com diagnóstico de anomalia congênita apresentaram sintomas de TEPT, sendo mais frequente entre as gestantes com diagnóstico de anomalia congênita inviável (64,9%). As questões de intrusão e hiperestimulação da escala IES-R estiveram mais correlacionadas entre si. Pareceu existir uma relação decrescente dos sintomas de TEPT, em relação ao tempo da notícia do diagnóstico de anomalia congênita.
CONCLUSÃO: os sintomas do TEPT estiveram mais presentes em gestantes com diagnóstico de anomalia congênita inviável.
Palavras-chave:
Anormalidades congênitas, Gestantes, Diagnóstico pré-natal, Transtornos de estresse pós-traumáticos
IntroductionCongenital anomalies are structural and/or functional alterations present at birth. There are several clinical manifestations that are expressed as mild dysmorphias with high prevalence in pregnancy and even complex alterations of organs or body segments, which are rare.
1According to the World Health Organization (WHO), approximately 50% of congenital anomalies are of indeterminate cause, but may have genetic, environmental, infectious and nutritional etiologies, and may be isolated or combined. It is estimated that worldwide neonatal deaths related to congenital anomalies correspond to 295,000 each year.
2Congenital anomalies affect the incidence and prevalence of fetal and neonatal morbidity and mortality. In the long term, they can have significant impacts on affected individuals and families, the health system and society.
2In the case of genetic diseases, the family may have more than one affected child.
3The technological advance of fetal medicine allows the early detection of congenital anomalies. The impact of this fetal diagnosis at any time during pregnancy is devastating to those involved.
4It is noted that the psychic suffering generated by the pregnancy of a fetus with a congenital anomaly can generate a condition of post-traumatic stress, whose symptoms can last a lifetime.
5Post-traumatic stress disorder (PTSD) is characterized by an immediate or delayed response to one or more traumatic events.
6,7 PTSD symptoms vary depending on the nature of an individual’s traumatic event, number of exposures, and vulnerability. This is associated with high levels of social and work incapacities with economic and health system burdens.
7,8 Psychological suffering, anxiety, depression and suicide
6 are also highlighted and can negatively affect an individual’s quality of life.
The study aims to assess PTSD symptoms in pregnant women diagnosed with congenital anomalies treated at a reference service for congenital anomalies in Brazil.
MethodsThis is a quantitative study with a cross-correlational design. The sample consisted of 111 pregnant women diagnosed with viable and non-viable congenital anomaly, assisted at the Fetal Medicine Ambulatory of the Federal University of São Paulo (UNIFESP – Portuguese acronym), from November 2013 to November 2014. The pregnant women recruited for the study were referred by Unified Health System (SUS – Portuguese acronym), by health insurance hospitals and by the teaching hospital of the aforementioned research.
We included pregnant women diagnoses with congenital anomaly, who knew their diagnosis for at least 7 days, as described in the Impact of Events Scale - Revised (IES-R) applicability criterion.
9 We excluded pregnant women with congenital anomaly who reported a psychiatric disorder and with previous psychological care. It is noteworthy that there was no exclusion by age, but classification by age group, with young women (maternal age 21 to 34 years), followed by adolescents (maternal age ≤20 years) and, later, with advanced maternal age (AMA) (maternal age ≥35 years).
The instruments used for data collection were a semi-structured questionnaire, composed of socioeconomic and demographic, obstetric and fetal variables. Moreover, to screen for PTSD symptoms, we use the IES-R, which can be used both in clinical practice and in scientific research.
10,11 The IES-R includes the PTSD assessment criteria published in the Diagnostic and Statistical Manual of Mental Disorders – Fifth Edition (DSM-V)
7, and was validated in Brazil in 2012 by Caiuby
et al.
12The IES-R aims to screen for PTSD symptoms at any stage of symptom development (acute, chronic, and late), but is not indicated as a diagnostic tool for this disorder.
10,12 It is worth mentioning that individuals answer the questions regarding the memories of the stressful event that occurred in the last 7 days before applying the scale.
9The IES-R is composed of 22 questions that were arranged in three subscales (intrusion, avoidance and hyperstimulation).
12 The score for each question varies from zero to 4 points, and the calculation of each subscale’s score is obtained by the mean of the items that make up the intrusion, avoidance and hyperstimulation subscales, disregarding the unanswered questions.
9The analysis of the sum of the IES-R questions with results above 33 points are considered the best cut-off points for the probable presence of PTSD symptoms associated with clinical assessment.
13However, according to the authors of the IES-R, calculating the mean of the items is more indicated.
9 The cross-cultural adaptation of the Brazilian version uses a cut-off of 5.6 units in the IES-R total score, defined as the sum of the means of the questions that make up the three subscales (ranging from zero to 12 points), to screen for PTSD symptoms.
12For statistical analysis, we used the following tests: chi-square for categorical variables; Student’s t test or Mann-Whitney test for continuous variable comparisons; Cronbach’s alpha coefficients
14 and Pearson’s correlation in the domains that make up the IES-R scale; simple linear regression models
15 to jointly assess the effect of the time of the notification of viable and non-viable congenital anomaly diagnosis, with the IES-R total score and domains.
The results were presented comparing the characteristics of pregnant women diagnosed with viable and non-viable congenital anomalies. The analyzes were performed using the software R 3.2.2.16. The graphs were built with the ggplot2 package.
17The tests were interpreted considering a significance level of 5%. This research was approved by UNIFESP’s Research Ethics Committee (REC 449.061/13 and CAAE (
Certificado de Apresentação para Apreciação Ética - Certificate of Presentation for Ethical Consideration) 19776613000005505).
ResultsIn the study, we included 111 pregnant women diagnosed with congenital anomaly, 67.7% from SUS and the rest from health insurance plans, who were referred to the teaching hospital of the aforementioned research. The mean maternal age was 27.2±7.8 years.Young pregnant women (maternal age 21 to 34 years) predominated, equivalent to 57.7% of the sample, followed by adolescents (maternal age ≤20 years), with 24.3% and, later, pregnant women with AMA (maternal age ≥35 years), with 18%. It is also noteworthy that these pregnant women mostly self-declared as brown (43.2%) and reported having completed high school and incomplete higher education (73.9%), in addition to being Catholic (49.5%) and single (67.6%).
According to the prenatal diagnoses of congenital anomalies, this study showed that 66.6% were pregnancies with fetuses with a prognosis of viability, while 33.3% were non-viable. These fetal diagnoses were established mainly in the second trimester of pregnancy in 77.5% of cases.
Among all cases of congenital anomalies, those related to the nervous, circulatory and urinary systems stood out. The non-viable congenital anomalies were anencephaly (35.1%), in addition to those related to the urinary (27%) and respiratory (24.3%) systems. The most frequent viable congenital anomalies were of the nervous system (31.1%) and the circulatory system (27%). When comparing fetal diagnoses of viable and non-viable congenital anomalies, it was found that those related to the respiratory system were associated with a greater chance of fetal non-viability.
It is noted that pregnant women with non-viable congenital anomaly thought more about carrying out the therapeutic interruption of pregnancy than those with viable congenital anomaly, corresponding to 37.8% and 5.4%, respectively (
p<0.001). Only a third of these pregnant women planned pregnancy, but in general, pregnancy was desired (97.3%).
When comparing PTSD symptoms in pregnant women with viable and non-viable congenital anomaly, they identified that the mean of all IES-R domains (avoidance, intrusion and hyperstimulation), as well as the sum of questions from the IES-R domains were high in all pregnant women diagnosed with congenital anomaly. However, higher in pregnant women diagnosed with non-viable congenital anomaly (Table 1).
The mean IES-R total score among pregnant women diagnosed with non-viable congenital anomaly was 1.9 points, i.e., higher than that of women with viable congenital anomaly (
p<0.001). This difference occurred in all IES-R domains (Table 1).Table 1 shows the statistics for the score, adding the questions that made up the IES-R. The sum of questions in the subscale domains was 48.1 for pregnant women diagnosed with a non-viable fetus and 33.9 for pregnant women with viable fetus diagnosis, indicating the probable presence of PTSD symptoms in both groups.
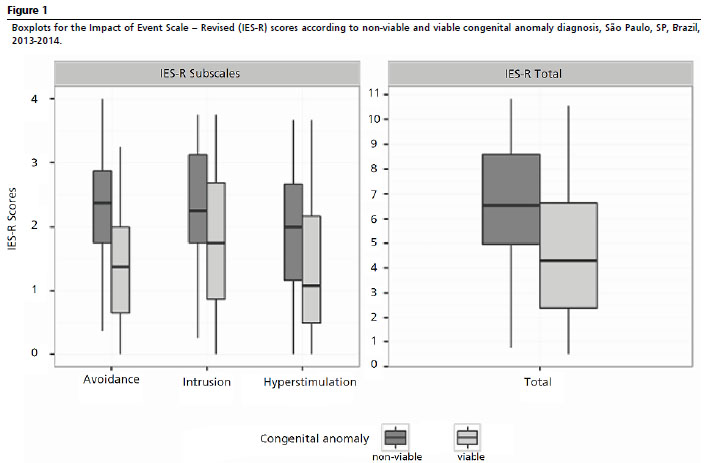
Figure 1 separates the boxplots for the IES-R domains, according to viable and non-viable congenital anomaly prenatal diagnosis. The score value in all IES-R domains was higher among pregnant women diagnosed with non-viable congenital anomaly.
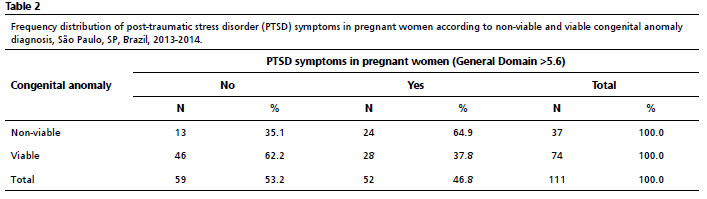
Table 2 demonstrates that when using the 5.6-unit cut-off in the IES-R total score to screen for PTSD symptoms, it was found that such symptoms were present in 46.8% of pregnant women diagnosed with viable and non-viable congenital anomalies. However, it was higher with 64.9% in those with non-viability diagnosis (
p<0.001; chi-square test).
When assessing Pearson’s correlation coefficient between the IES-R domains, it was noticed that intrusion and hyperstimulation were more correlated with each other than with avoidance.The Cronbach’s alpha of the domains was high in all IES-R subscales: 0.842 (avoidance); 0.908 (intrusion); and 0.868 (hyperstimulation). Cronbach’s alpha for the total score of this scale was 0.943. This demonstrated that the IES-R had high internal consistency values for the total score, also for its subscales.
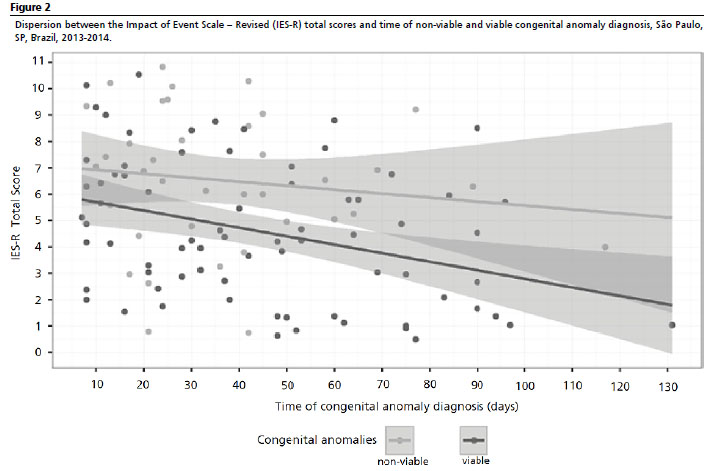
Figure 2 demonstrates the relationship between the time of the news of congenital anomaly diagnosis and PTSD symptoms in pregnant women with viable and non-viable fetuses. The mean IES-R score was higher among non-viable cases and there was a decreasing relationship of the total score in relation to the time of the news of congenital anomaly diagnosis.
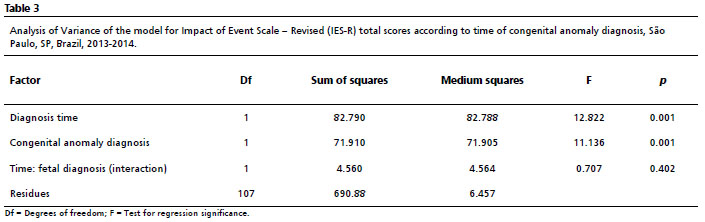
To test the strength and interaction of the time of the notification of congenital anomaly diagnosis with PTSD symptoms in pregnant women, a model was initially built for the IES-R total score. In the analysis of variance (ANOVA), there was no interaction effect between time of congenital anomaly diagnosis and IES-R score according to congenital anomaly diagnosis (Table 3).
Therefore, another statistical model was adjusted (multiple linear regression) with only fixed effects. We conclude that, at the 5% significance level, the score decreased by 0.028 unit on average for each day after congenital anomaly diagnosis, regardless of fetal viability.The fit quality, however, was not very high, with a coefficient of determination (R²) of only 18.2%, and much of this variability was explained by the type of congenital anomaly diagnosis. Anyway, there was a relationship with time, although weak.
Among pregnant women diagnosed with viable and non-viable congenital anomaly, there seemed to be a weak relationship in the IES-R avoidance domain. The other two domains (intrusion and hyperstimulation) showed stronger relationships with time. The relationship with the type of congenital anomaly diagnosis was important in all IES-R domains.
DiscussionIn this study, young pregnant women predominated, followed by adolescents and those with AMA.Viable congenital anomalies were more frequent in adolescent and young pregnant women, while non-viable anomalies were more frequent in pregnant women with AMA. In this context, age extremes are considered important risk factors for congenital anomalies.
2,18The most frequent congenital anomalies were related to the nervous system (excluding anencephaly), circulatory and urinary systems. These findings corroborate those found by other researchers, who describe the main diagnoses of congenital anomalies in prenatal care: central nervous system, nephrological and cardiovascular anomalies, especially among pregnant adolescents.
19,20When assessing the main prenatal diagnoses of non-viable congenital anomalies, anencephaly stood out, followed by urinary and respiratory system. According to Benute
et al.,
21 among the diagnoses of non-viable congenital anomalies, anencephaly is the main one. On the other hand, when analyzing viable congenital anomaly diagnosis, anomalies of the nervous system and of the circulatory system were the most common.
Congenital anomalies characterized as viable are compatible with life, because, regardless of the degree of limitation suffered by the developing being, individuals will be able to adapt and live with these limitations. However, severe congenital anomalies make the fetus non-viable/incompatible with extrauterine life.
22The diagnoses of congenital anomalies were performed in the second gestational trimester (14
th to 27
th weeks) in 77.5% of cases.This is because most pregnant women with such diagnoses are lately referred to the reference service in fetal medicine, after 24 weeks of gestation. This fact makes it difficult to screen for congenital anomalies, including chromosomal ones, through invasive procedures such as chorionic villus sampling and amniocentesis. We add to this is the importance of multidisciplinary care for pregnant women and their families with the aim of alleviating emotional distress and maternal-fetal risks, in addition to contributing to a better neonatal prognosis, in cases of viable congenital anomalies.
Congenital anomalies have different approaches to prenatal care depending on fetal viability. Thus, the differentiation between viable and non-viable congenital anomalies is important in care plan and in biolaw, since it delimits the therapeutic interruption of pregnancy. This is performed only in pregnant women with fetuses with non-viable congenital anomalies, without any potential for life, which does not characterize abortion.
22Faced with anencephaly diagnosis, pregnant women have the right to maintain their pregnancy or interrupt it.
23 In addition to anencephaly, an anomaly case in which therapeutic interruption is legalized in Brazil, there are other types of congenital anomalies that are also considered non-viable, especially if associated with severe pulmonary hypoplasia. In these cases, in Brazil, the therapeutic interruption of pregnancy is possible only by means of a judicial request and with a favorable opinion. Additionally, pregnant women must attend prenatal care with a multidisciplinary team, preferably in fetal medicine.
These fetal diagnoses of congenital anomalies can generate PTSD symptoms in pregnant women, as they can be considered stressful and life-threatening events.Thus, given the stress of such fetal diagnoses, pregnant women may present: invasive memories (flashbacks), dreams or nightmares, insomnia, anger, fear, aggressiveness and hypervigilance.
6,7 Such symptoms can be associated with anxiety, depression and even suicide.
6In this context, PTSD symptoms can be verified using the IES-R. According to the authors,
9,12,13 symptoms can be assessed as follows: sums of questions from the IES-R
13 subscales; calculation of the mean of the IES-R
9 subscale items; and cross-cultural adaptation of the IES-R, Brazilian version, which can use a cut of 5.6 units in the total score, defined as the sum of the means of the questions that make up the three subscales.
12 In this study, all these analyzes were performed with pregnant women with congenital anomalies.
When analyzing the sum of questions from the IES-R subscales, pregnant women diagnosed with non-viable congenital anomaly scored 48.1 points and those diagnosed with a viable congenital anomaly scored 33.9 points. The sum of the IES-R questions in the two groups studied was equivalent to 38.7. These results demonstrate the probable presence of PTSD in the studied pregnant women, being higher in those with non-viability diagnosis.
According to Reed,
13 in the IES-R, results exceeding 24 points can be significant as individuals who experience at least one PTSD symptom become a clinical concern. A result above 33 points is considered the best cut-off point for the probable presence of PTSD associated with clinical assessment. A score above 37 points is high enough to compromise the immune system,
13 which has an impact on quality of life.
A study carried out in a reference service for fetal medicine in Norway analyzed the sums of the IES-R questions, verifying that pregnant women diagnosed with congenital anomaly had a score in all IES-R subscales (intrusion, avoidance and hyperstimulation) ≥20 points, mainly in the intrusion and hyperstimulation domains. These authors consider this score as the probable presence of PTSD. When comparing pregnant women with congenital anomaly diagnosis with pregnant women without such a diagnosis, we have found that the former had significantly higher levels of psychosocial distress in all tests, including IES-R assessment.
24Other authors, when assessing PTSD symptoms in postpartum women through the IES-R, identified that more than half of the sample had a score ≥24 points in the total score, and the other participants, equivalent to 37 points. PTSD symptoms were more present in the group of puerperal women diagnosed with non-viable congenital anomaly.
25 Such findings are equivalent to those found in the group of pregnant women diagnosed with fetal non-viability. This demonstrates that PTSD symptoms are present in women since congenital anomaly diagnosis and after childbirth, for an indefinite period, and varies according to individual coping and support network.
However, according to the authors
9 of the IES-R, it is more appropriate to calculate the mean of the items than just the sum of the IES-R subscale questions.In this study, the mean total score of the IES-R among pregnant women diagnosed with non-viable congenital anomaly was higher than that of pregnant women diagnosed with a viable congenital anomaly (
p<0.001).This difference was observed in all IES-R domains, which confirms the presence of PTSD symptoms.
Studies corroborate these results, as they showed that the mean of all IES-R domains was high among pregnant women diagnosed with congenital anomalies, being higher among those with non-viable fetuses.
9 Kaasen
et al.
24 observed that pregnant women with severe congenital anomalies, without treatment and with indeterminate fetal prognosis (such as acrania, skeletal dysplasia and bilateral renal agenesis), had higher means in all IES-R domains.On the other hand, pregnant women diagnosed with a less severe congenital anomaly, with treatment and better prognosis (such as gastroschisis and unilateral renal cyst) had lower means in the IES-R.Thus, the severity and ambiguity in congenital anomaly diagnosis was a strong predictor of psychological distress verified in all IES-R domains.
24Finally, when performing a 5.6-unit cut in the IES-R total score for PTSD symptom screening,
12 we found that such symptoms were present in 46.8% of pregnant women with viable and non-viable congenital anomalies. PTSD symptoms were more frequent in pregnant women with non-viable congenital anomaly, equivalent to 64.9%, than among pregnant women with viable fetuses.
When assessing the correlation between the IES-R domains, it is noted that intrusion and hyperstimulation are more correlated with each other than with avoidance. The Cronbach’s alpha of the domains was high in all IES-R subscales: 0.842 (avoidance), 0.908 (intrusion) and 0.868 (hyperstimulation). The Cronbach’s alpha for the total score of this scale was 0.943. Such results are similar to other studies, demonstrating that the IES-R has high internal consistency values for its total score (Cronbach’s alpha between 0.85 to 0.96) and subscales (avoidance from 0.77 to 0.87; intrusion from 0.72 to 0.94; hyperstimulation from 0.81 to 0.91).
11,12The greatest correlation between the IES-R intrusion and hyperstimulation domains may be related to some PTSD symptoms in pregnant women diagnosed with congenital anomaly, both with a prognosis of viability and non-viability. According to the DSM-V,
7 these symptoms can be involuntary intrusive memories and distressing, recurring dreams of a traumatic event; psychological distress and intense physiological reactions to signs that symbolize some aspect of the traumatic event, in this case, congenital anomaly diagnosis.
Furthermore, there is increased excitability, as pregnant women with a congenital anomaly may experience irritability and outbursts of anger, usually expressed in the form of verbal or physical aggression towards people and objects; reckless or self-destructive behavior; hypervigilance; exaggerated startle response; and difficulty concentrating and initiating and maintaining sleep.
7Although the IES-R avoidance domain presents a lower correlation with intrusion and hyperstimulation, it is important to highlight PTSD symptoms related to avoidance. Pregnant women with congenital anomalies may also have periods of avoidance or efforts to avoid distressing memories, thoughts, or feelings about the traumatic event, in addition to avoiding places, people, actions, activities, objects, and anything else that recalls the traumatic event.
7However, a lower percentage of avoidant symptoms compared to intrusive and hyperstimulating symptoms may be related to congenital anomaly diagnosis at follow-up. This is because pregnant women cannot avoid certain places and people, such as prenatal care service.
It was observed that among pregnant women with congenital anomaly, there was a decreasing, albeit weak, relationship between PTSD symptoms in relation to the time of the notification of congenital anomaly diagnosis. In the IES-R avoidance domain, this relationship is weaker and, in intrusion and hyperstimulation, there are more prominent relationships with time.
The IES-R total score decreases by 0.028 units, on average, for each day after congenital anomaly diagnosis, regardless of fetal viability. This means that only after 35 days elapsed from the diagnosis of congenital anomaly, pregnant women decreased, on average, by 1 point in the IES-R. Thus, PTSD symptoms prevail throughout pregnancy or even at childbirth or postpartum.
These analyzes demonstrate that PTSD symptoms are more significant among pregnant women diagnosed with nonviable fetuses. PTSD diagnosis includes investigation of its symptoms, the individual’s past history, and the differential diagnosis with other psychopathological disorders.
26 PTSD symptoms manifest within the first 3 months after the trauma, but there may be a delay of months or even years before the diagnostic criteria are met – a fact known as “late onset”.
7PTSD treatment includes drug therapy, cognitive-behavioral and psychodynamic approach.
27 Cognitive-behavioral therapy is pointed out as the most efficient for the treatment of PTSD.
28 On the other hand, drug treatment is controversial for individuals with PTSD.
29In this regard, pregnant women diagnosed with a congenital anomaly have coping strategies, such as religiosity, in the unconditional hope for a miracle. On the other hand, feelings of anxiety, frustration and guilt remain, in addition to fear regarding maternal-fetal risks.
30 The relevance of qualified and attentive multidisciplinary care in prenatal and puerperium to the symptoms and effects of stress and trauma caused in women with congenital anomalies stands out.
AcknowledgmentsWe would like to thank CAPES, for promoting this research, and the multidisciplinary team, the pregnant women from
Casa da Saúde da Mulher Prof. Dr. Domingos Deláscio, and statistician Lucas Petri, for their contributions.
References1. São Paulo (cidade). Secretaria Municipal da Saúde. Coordenação de Epidemiologia e Informação – CEInfo. Declaração de Nascido Vivo. Manual de preenchimento da Declaração de Nascido Vivo. São Paulo: Secretaria Municipal da Saúde; 2011.
2. World Health Organization (WHO). Congenital anomalies. Geneva: WHO; 2022 [access in 2022 Jun 1]. Available from:
https://www.who.int/health-topics/congenital-anomalies#tab=tab_33. Abrahão AR, Sala DC, Moron AF. Aconselhamento genético. In: Moron AF, Camano L, Júnior LK. Obstetrícia. São Paulo: Manole; 2011. p. 1413-9.
4. Fisher J. Interrupção da gravidez por anomalia fetal: a perspectiva de uma organização de apoio aos pais. Reprod Health Matters. 2008; 16 (31): 57-65.
5. Federação Brasileira das Associações de Ginecologia e Obstetrícia (FEBRASGO). FEBRASGO se posiciona sobre fetos anencéfalos. São Paulo: FEBRASGO; 2011 [access in 2020 Jun 6]. Available from:
https://portaldeboaspraticas.iff.fiocruz.br/biblioteca/posicao-da-febrasgo-sobre-gravidez-com-fetos-anencefalos/6. Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde: Manual de Instruções. Capitulo V - Transtornos mentais e comportamentais. 10th ed. rev. São Paulo: Edusp; 2007. p. 40.
7. American Psychiatric Association (APA). Manual diagnóstico e estatístico de transtornos mentais (DSM-5). 5th ed. Porto Alegre: Artmed; 2014.
8. Kapczinski F, Margis R. Transtorno de estresse pós-traumático: critérios diagnósticos. Rev Bras Psiquiatr. 2003; 25 (Supl. 1): 3-7.
9. Weiss DS, Marmar CR. The impact of Event Scale-Revised (IER-R). In: Wilson J, Keane MT, editors. The impact of Event Scale-Revised: assessing psychological trauma and PTSD. New York: Guilford Press; 1997. p. 399-411.
10. Joseph S. Psychometric evaluation of Horowit’s Impact of Event Scale: a review. J Trauma Stress. 2000; 13 (1): 101-13.
11. Silva AC, Nardi AE, Horowitz M. Versão brasileira da Impact of Event Scale (IES): tradução e adaptação transcultural. Rev Psiquiatr Rio Gd Sul. 2010; 32 (3): 86-93.
12. Caiuby AV, Lacerda SS, Quintana MI, Torii TS, Andreoli SB. [Cross-cultural adaptation of the Brazilian version of the Impact o f Events Scale-Revised (IES-R)]. Cad Saúde Pública. 2012 Mar; 28 (3): 597-603.
13. Reed SB. Measuring the Emotional Impact of an Event. 2007 [access in 2016 May 9]. Available from:
http://psychotherapy-center.com/counseling-issues/trauma-and-stressors/ptsd-post-traumatic-stress-disorder-therapy/measuring-the-emotional-impact-of-an-event14. Cronbach LJ. Coefficient alpha and the internal strucuture of tests. Psychometrika. 1951 Sep; 16 (1): 297-334.
15. Neter J, Kutner MH, Nachtsheim CJ, Wasserman W. Applied linear statistical models. 4th ed. USA: Times Mirror Higher Education Group; 1996.
16. R Core Team. The R Project for Statistical Computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing; 2015 [access in 2016 May 9]. Available from:
http://www.R-project.org/17. Wickham H. Elegant graphics for data analysis. 3th ed. Spain: Springer; 2009.
18. Loane M, Dolk H, Morris JK; EUROCAT Working Group. Maternal age-specific risk of non-chromosomal anomalies. BJOG. 2009; 116 (8): 1111-9.
19. Gallo JH. Gravidez na adolescência: a idade materna, consequências e repercussões. Rev Bioet. 2011; 19 (1): 179-95.
20. Reis LV, Araujo Junior E, Guazzelli CAF, Cernach MCSP, Torloni MR, Moron AF. Anomalias Congênitas identificadas em recém-nascidos de mulheres adolescentes. Acta Med Port. 2015; 28 (6): 708-14.
21. Benute GR, Nomura RM, Lucia MC, Zugaib M. Interrupção da gestação após o diagnóstico de malformação fetal letal: aspectos emocionais. Rev Bras Ginecol Obstet. 2006; 28 (1): 10-7.
22. Baraldi IA, Diniz NM. Reflexões sobre a interrupção da gestação de feto anencefálico. Rev Bras Bioet. 2007; 3 (2): 170-90.
23. Conselho Federal de Medicina (CFM). Resolução CFM nº 1.989, de 14 de maio de 2012. Dispõe sobre o diagnóstico de anencefalia para antecipação terapêutica do parto e dá outras providências. Brasília (DF): DOU 14 de maio 2012; Seção I. p. 308-9. [access in 2016 Mai 9]. Available from:
http://www.portalmedico.org.br/resolucoes/CFM/2012/1989_2012.pdf24. Kaasen A, Helbig A, Malt UF, Naes T, Skari H, Haugen G. Acute maternal social dysfunction, health perception and psychological distress after ultrasonographic detection of a fetal structural anomaly. BJOG. 2010; 117 (9): 1127-38.
25. Oliveira VJ, Westphal F, Abrahão RA. Impacto do desfecho neonatal em puérperas de recém-nascidos portadores de anomalia congênita. Cogitare Enferm. 2015; 20 (2): 360-7.
26. Cavalcante FG, Morita PA, Haddad SR. Sequelas invisíveis dos acidentes de trânsito: o transtorno de estresse pós- traumático como problema de saúde pública. Rev Ciênc Saúde Colet. 2009; 14 (5): 1763-72.
27. Saporta JA. Psychodinamic psychotherapy for PTSD. J Clin Psychiatry. 2000 Oct; 61 (10): 787.
28. Caporossi JA, Ribeiro HS, Morinigo T, Campos A, Stoppiglia LF. Mastectomia e incidência de transtorno de estresse pós-traumático. Rev Psicol Saúde Doenças. 2014; 15 (3): 800-15.
29. Eisenstein E, Jorge E, Lima LA. Transtorno do estresse pós-traumático e suas repercussões clínicas durante a adolescência. Rev Adolesc Saúde. 2009; 6 (3): 7-15.
30. Bomfim OL, Coser O, Moreira MEL. Unexpected diagnosis of fetal malformations: therapeutic itineraries. Physis. 2014; 24 (2): 607-22.
Received on June 20, 2020
Final version presented on February 8, 2021
Approved on March 28, 2022
Author’s contributionAguiar MAV, responsible for the research, carried out the bibliographic review, research project and methodological design construction, in addition to data collection, statistical analysis and results. Abrahão AR was the project advisor. All authors approved the final version of the article and declare no conflict of interest.


 ; Anelise Riedel Abrahão 2
; Anelise Riedel Abrahão 2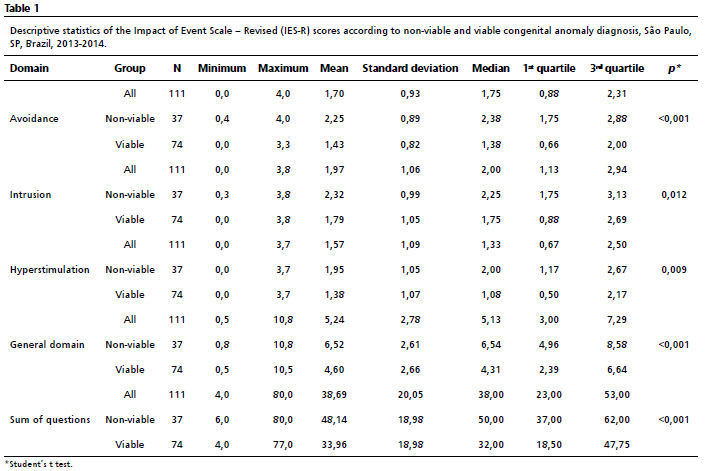






 Ler em português
Ler em português