ABSTRACT
OBJECTIVES: evaluate the relationship between family’s food and nutrition insecurity (FNI) and the social network of malnourished children.
METHODS: cross-sectional study with 92 children, included in the economic class D-E. For the analysis of the children’s social network, the mothers answered four simple questions. To investigate the FNI, the Brazilian Scale of Food Insecurity was used. The association between variables was analyzed by Poisson regression with robust analysis of variances.
RESULTS: 56.5% of the children had a weak social network (<10 individuals), and the prevalence of FNI was 72.8%. An inverse association was observed between children of the daily social network and FNI family (OR=0.94; CI95%=0.89-0.99], p=0.03). The number of individuals in the children’s daily social network was negatively associated with the likelihood of FNI. The mother’s educational level was also related to FNI (OR=2.20 [CI95%=1.11-4.34]; p=0.02), being the child up to 2.2 times more likely to be in FNI when the mother has less than four years of study.
CONCLUSION: these results suggest that social network is associated with the FNI of malnourished children. Interventions designed to strengthen instrumental and other forms of support among small social networks can improve the health/nutrition of malnourished children with FNI.
Keywords:
Malnutrition, Child, Food insecurity, Vulnerability, Stunting
RESUMO
OBJETIVOS: avaliar a relação entre a insegurança alimentar e nutricional (IAN) da família e a rede social de crianças desnutridas.
MÉTODOS: estudo transversal com 92 crianças, inseridas na classe econômica D-E. Para a análise da rede social das crianças, as mães responderam quatro perguntas simples. Para investigar a IAN foi utilizada a Escala Brasileira de Insegurança Alimentar. A associação entre as variáveis foi analisada por regressão de Poisson com análise robusta das variâncias.
RESULTADOS: 56,5% das crianças apresentaram rede social fraca (<10 indivíduos), e a prevalência de IAN foi de 72,8%. Foi observada uma associação inversa entre rede social diária das crianças e IAN da família (RP=0,94, [IC95%=0,89-0,99]; p=0,03). O número de indivíduos na rede social diária das crianças se associou negativamente com a probabilidade de IAN. O nível de escolaridade materno também estava relacionado com a IAN (RP=2,20 [IC95%=1,11-4,34]; p=0,02), tendo a criança até 2,2 vezes mais probabilidade de estar em IAN quando a mãe apresenta menos de quatro anos de estudo.
CONCLUSÃO: esses resultados sugerem que a rede social está associada à IAN de crianças desnutridas. Intervenções destinadas a fortalecer maneiras instrumentais e outras formas de apoio entre pequenas redes sociais podem melhorar a saúde/nutrição de crianças desnutridas com IAN.
Palavras-chave:
Desnutrição, Criança, Insegurança alimentar, Vulnerabilidade, Baixa estatura
IntroductionSocial networks account for maintaining the social identity of each individual; these interpersonal contact networks can be a determining factor for children’s health and health-related behaviors.
1 Children’s social network is initially formed by their mother’s social network; however, overtime, it establishes and weaves social connections with similar individuals, other children, as well as with geographically close and recurrent contacts.
2Individual factors, such as parental divorce, sexual/physical abuse of children/adolescents, poverty and impoverishment, wars and other sources of trauma, as well as low support from one’s family or groups can contribute to improper development of children/adolescents’ social skills.
3 Moreover, food insecurity is another factor significantly influencing the development of children and adolescents’ social skills, affecting their health, leading them to become withdrawn and decreasing their connections.
4Food insecurity is defined as limited or uncertain physical and economic access to sufficient amounts of nutritionally proper and safe food, in socially acceptable ways, to enable family members to maintain an active and healthy life.
5 Prevalence of moderate (4.3%) and severe (3.3%) food insecurity was observed in Brazil; it was higher in the North and Northeast regions (14.7%).
6 Study conducted with the population living in Alagoas State has evidenced 8.2% prevalence of severe food insecurity in households with individuals under the age of 18.
7Food insecurity is also among multiple and interrelated factors determining malnutrition,
5 which weakens individuals’ nutritional status and makes them more susceptible to develop different diseases and to premature death. Thus, food insecurity is a devastating issue, mainly for the poorest individuals.
8 Therefore, interventions aimed at providing social support to food acquisition play significant role in improving individuals’ nutritional status, mainly that of children.
9Short stature is the most prevalent malnutrition type in Brazil and abroad; it often results from undernourishment and recurrent infections that are strongly associated with unhealthy living conditions.
8 Short stature is a sensitive indicator used to measure children’s well-being, the progress of a given country, human capital accumulation and poverty. Children with delayed growth often live in food-insecure households; they are more likely to die during their first five years of life, get sick more often and perform poorly in school.
10,11Thus, the context children live in affects their health, regardless of their features, or of their mother and family’s features. Accordingly, communities share physical, social and economic attributes capable of determining the health condition of all individuals. These attributes, which form social networks, can influence individuals’ health by spreading information, as well as by supporting and guiding them to adopt certain health and social well-being behaviors.
10Thus, it is clear that social networks in early childhood lead to a wide variety of outcomes, later in life, such as health, nutrition, cognition and future performance.
12 There is evident need of providing better quality childcare at this life stage, when stimuli influence children’s development and have long-term repercussions on school success, on relationships’ formation, on self-protection required for economic independence, as well as on individuals’ preparation for life, and for family and community coexistence.
2Based on this scenario, it is possible questioning whether social support networks can help improving food security promotion at family level, since individuals need these relationships to face and solve different issues in their lives.
1 The aim of the current study was to assess the association between food and nutrition insecurity (FNI) in malnourished children’s family and their social network.
MethodsCross-sectional study conducted from January to October 2019, with children enrolled at the Center for Nutritional Recovery and Education of Alagoas State (CREN-AL – Portuguese acronym), which is located in one of the areas recording the lowest Human Development Index (HDI) in Maceió City, adjacent to Federal University of Alagoas, as one of its extension projects. CREN-AL offers assistance in health, food, education and human resources’ qualification for care provided to children under six years old. The aforementioned Center admits children at risk of stature deficit (Z-score -1.5 for height/age (H/A)) and those with stature deficit (Z-score -2 for H/A), based on the standard proposed by the World Health Organization.
13 The Center provides daily care for 100 children (on average) who attend it throughout the week, from 08:00 am to 05:00 pm, and who receive daily pediatric, nutritional, dental, psychological and pedagogical care. It also provides social and psychological care for families. The institution’s mission is to recover the nutritional status of children diagnosed with malnutrition, in an interdisciplinary way, in order to contribute to the empowerment and fully development of both these children and their families.
All children whose guardians were their mothers (biological/adoptive), and who were economically classified as D-E classes, based on the Brazilian Economic Classification Criteria (CCEB – Portuguese acronym), were included in the current study.
14 They were identified based on the analysis of CREN children’s medical records. Home interview, based on the application of previously tested questionnaires, was carried out.
Food and nutrition security was used as dependent variable. Food insecurity was assessed based on the Brazilian Food Insecurity Scale (EBIA-
Escala Brasileira de Insegurança Alimentar).
15 This tool comprises 14 closed core questions (with yes/no answer options) about participants’ experience with food insufficiency at different intensity levels, in the last three months. It ranges from concern about running out of food to spending a whole day without eating anything. Each positive answer in the questionnaire represents 1 point; scale classification is based on the sum of points, which ranges from 0 to 15. The aforementioned classification was carried out as follows: 0: security; 1-5: mild insecurity; 6-10: moderate insecurity; and 11-14: severe insecurity. Prevalence estimates were calculated based on using this variable at its four levels. On the other hand, dichotomized variable was used for both the bi- and the multivariate models; households under “Food security + mild insecurity” conditions were classified as not at risk, whereas households under “Moderate insecurity + severe insecurity” conditions were classified as at risk; the combination of the last two conditions was used to feature individuals living under food deprivation condition.
Children’s social network was used as independent variable. Mothers answered four simple questions, which were adapted from the questionnaire proposed by Mitchinson
et al.,
16 to enable assessing social network size and the amount of contact with children’s network:
1. How many people or relatives does your child have contact with, including his/her father and siblings?
2. How many close people or family members does your child see at least once a month? To assess children’s social support, mothers were asked:
3. Does your child go to church, synagogue, temple, mosque or other worship places at least once a week? (Yes or No)
4. Does your child participate in social institutions (health center or other places) other than CREN, at least once a week? (Yes or No). Social networks comprising up to ten individuals in children’s daily life were considered small.
Socioeconomic and housing data, as well as children’s nutritional status, were used as adjustment variables. Socioeconomic variables comprised household features, basic sanitation, maternal schooling in years of study (0 to < 4 years; 4 to 8 years and > 8 years), mothers’ marital status (married, divorced or widow), benefited by
Bolsa Família [Family Allowance – social welfare program] (no/yes) and family income
per capita, including
Bolsa Família value. The following cut-off points were adopted for evaluation purposes: ≤ R$ 124.75; > R$ 124.75 to ≤ R$ 249.51; > R$ 249.51).
Anthropometric data were collected based on the analysis of CREN nutritional care records to enable assessing children’s nutritional status. Standard infantometer (105-cm long and 0.1-cm accuracy) and vertical stadiometer (measurement ranging from 0 to 200 cm; 1-mm precision; Wiso, Paraná State, Brazil) were used to measure the length of children under 24 months and > 24 months old, respectively. Participants’ weight was measured with the aid of Filizola, BP Baby and Filizola Personal scales, Campo Grande, Brazil.
Nutritional status classification took into consideration BMI/Age and Length/Age (height/age) ratios, which were analyzed in Anthro and Anthro Plus software, version 3.2.2, based on using the following cut-off points for H/A index: Proper H/A (z score > -1), risk of low H/A (z score ≤ -1 and > -2), and low H/A (z score ≤ -2).
13 With respect to statistical analyses, continuous variables were expressed as mean and standard deviation, whereas categorical variables were expressed as relative and absolute frequencies. Linear regression was carried out to check whether there was association between the daily social network variables and children’s H/A ratio. Welch test was used to compare daily mean values recorded for social network between the two EBIA categories. Poisson regression based on robust estimate of variances, as well as on adjustments to likely confusion variables (children’s age, sex, family income
per capita, mother’s age,
Bolsa Família, mother’s schooling), was performed to investigate association between daily social network and food insecurity. Alpha value of 5% was adopted for analysis purposes. All statistical analyses were conducted in R statistical software (R Foundation for Statistical Computing, Vienna, Austria), based on using the “Rcmdr” package.
The present study was submitted to, and approved by the Research Ethics Committee of Federal University of Alagoas, under protocol number: 09801818.3.0000.5013.
ResultsEight (8) of the 100 children eligible for the study were excluded from it (five of them have changed address, one was in economy class C, and two had their father as guardians); thus, the final sample comprised 92 children. Anthropometric, socioeconomic and social network features of children, and of their families, are shown in Table 1. Mean age of three years and short stature for age with mean value of -2.17 (± 95 H/A) were more prevalent in boys (98.3%) than in girls (90.6%). Daily social network with less than ten individuals was observed for 52 children (56.5%); 33 (63.5%) were boys. In total, 62 children (67.4%) presented monthly social network only comprising four individuals; 47 (75.8%) of them were male (data not tabulated). Moreover, more than 50% of the assessed children did not have contact with any religion (51.1%) and only 18.5% of them attended another institution besides CREN.
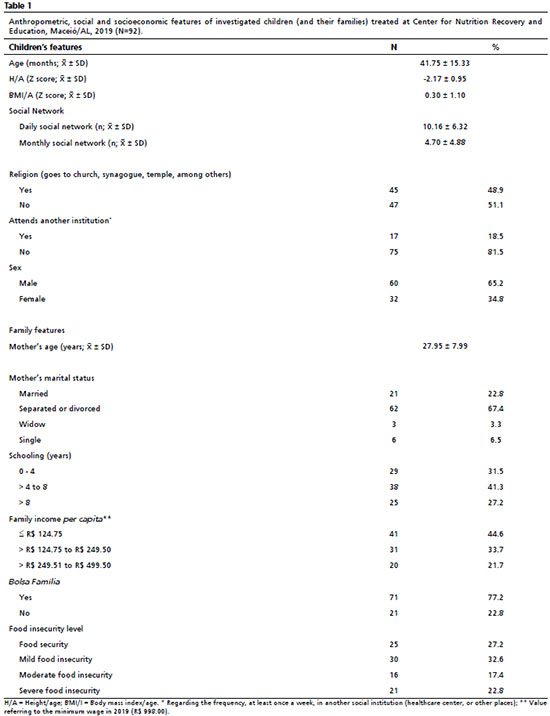
With respect to mothers’ marital status, 77.2% were separated or divorced from the father of the child selected for the study, single or widows. As for maternal schooling, 72.8% of mothers did not complete Elementary School (less than eight years of study). Income
per capita of 41 families (44.6%) was lower than R$125.00 and mostly (77.2%) derived from
Bolsa Família (Table 1). Food insecurity (mild, moderate and severe) was prevalent in 72.8% of families. If one takes into consideration moderate and severe food insecurity, it is possible saying that 37 households (40.2%) were living under food deprivation condition (Table 1).
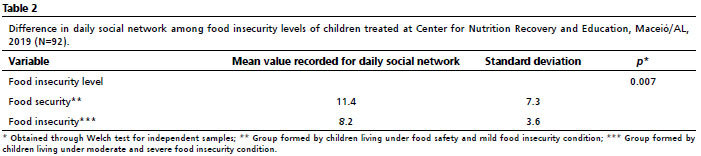
No association between variable H/A and daily social network was observed (β=-0.007; [CI95%=-0.03-0.02];
p=0.66) (data not tabulated). However, there was difference in means recorded for children’s daily social network between the two EBIA categories, i.e., children living under moderate and severe food insecurity condition presented smaller daily social network (Table 2).
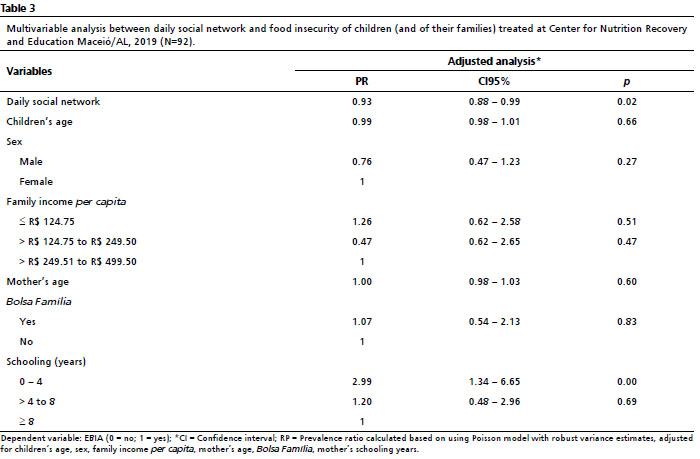
The process to associate the size of children’s daily social network with food insecurity has shown reduction by 7% in the likelihood of food insecurity for each increase by one unit in children’s daily social network (PR=0.93; [CI95%=0.88-0.99]:
p=0.02), even after adjustments made based on children’s age and sex, family income
per capita, mother’s age and years of schooling, and
Bolsa Família. Children of mothers with less than four years of schooling were 2.99 times more likely to live under food insecurity condition than those whose mother had more than four years of schooling (Table 3).
DiscussionThe present study has evidenced that most malnourished children who live in social vulnerability (56.5%) presented small social network comprising less than ten individuals. It has also shown that this population recorded high prevalence of food insecurity (77.2%). Based on multivariate analysis, it was possible seeing the positive impact of the size of children’s daily social network, which presented reduction by 7% in food insecurity for each increase by one individual in children’s social network.
The current study has shown that children’s daily social network and mothers’ years of schooling were associated with food insecurity, since the likelihood of living under food insecurity condition decreased as children’s daily social network increased. Although Brazil recorded reduced food insecurity prevalence in recent years, such a reduction was smaller in Northeast region and in the poorest states, such as Alagoas.
6,17 Varying and interrelated factors were the ones determining food insecurity; social network was one of the main factors at household level.
5This fact can be observed in a study conducted with 111 female heads of households who lived in a community in Kenya, where lower social support was significantly associated with increased food insecurity.
18 Another example of it can also be seen in a study conducted with a sample comprising 1,056 households in Burkina, Western Africa, where the head of household’s social network played positive role in food security.
19 These data have shown that the population investigated in the current study is similar to that of African countries, which present low income and high food insecurity levels.
Food insecurity recorded prevalence of 72.8% among families investigated in the current study; this value was much higher than the national estimate (36.7%) for 2017-2018.
17 However, it is worth emphasizing that the prevalence level recorded for moderate and severe food insecurity (40.2%) was higher than the ones observed for households with children under five years old (14.7%) in 2017-2018
17 and than the one observed in rural area occupied by a
Quilombola community in Bahia State (27%).
20 These findings are alarming, since they evidence a large number of individuals who still live under food insecurity condition and who experience inequalities associated with color/race, income range, and urban vs. rural location; these inequalities pose relevant challenges to the implementation of public policies focused on ruling out hunger and poverty.
Maternal schooling is one of the main significant predictors of children’s healthy eating habits.
21 In addition, adequate education levels can provide better opportunities for mothers to enter the labor market to help increasing both family income
22 and access to food. Study conducted in central Ethiopia with 635 lactating mothers in the age group 15-49 years has shown that mothers lacking formal education were 1.82 times more likely to live under food insecurity condition.
23 These data corroborate the present study, which observed association between low maternal schooling (less than four years of schooling) and moderate and severe food insecurity. This finding is also similar to the one reported in study carried out with 365 children under the age of five, who had diarrhea, in Bangladesh, where there is high poverty and malnutrition rates. The aforementioned study has evidenced that children of illiterate mothers were 2.14 times more likely to experience food insecurity.
24 This finding has evidenced the contextual complexity marking the association of inequalities and inequities with food insecurity.
Social network belongs to contextual factors associated with causes of malnutrition, since the involvement of other individuals in mothers’ social network has influence on children’s complementary feeding.
25 However, the current study did not find straight association between children’s daily social network and stature deficit. Nevertheless, it is well known that moderate and severe food insecurity can lead to malnutrition, which, in its turn, can result in death, mainly when it is associated with recurrent infections.
5,11,15 Social indicators, such as low income and schooling, as well as lack of employment and basic sanitation, are also the main conditions associated with linear growth issues faced by Brazilian children under the age of five, in a context wherein, although these two events are different from each other, they are associated with social determination.
26 Study conducted with 2,222 children in the Gicumbi district of Rwanda, Africa, where most homes do not have toilets, has shown 2.47 times higher likelihood of 6-59-month-old children living under moderate food insecurity conditions to have low stature than children from food-secure families.
27 Based on the current study, the likelihood of having children living under food insecurity condition was inversely related to the size of their daily social network. Thus, the fact that social network is associated with food insecurity enables inferring that interventions in these networks can positively influence nutritional levels among these vulnerable populations. However, social networks are not the only ones associated with multiple factors capable of influencing food insecurity; education also has significant influence among individual factors,
5 as also observed in the present study.
Accordingly, data collected in a study carried out with beneficiary families of
Bolsa Família Program in 2011, who lived in substandard settlements in Maceió City (AL), have evidenced that 92% of families lived under food insecurity condition.
28 These data have show that nothing, or almost nothing, was done after eight years; this finding was corroborated by food insecurity values recorded in the present study. Food security is directly affected by economic factors, such as low income.
11 However, the current study did not find association between family income
per capita and food insecurity; this finding can be explained by the fact that all investigated families belonged to the same social class (D-E) and that most of them were
Bolsa Família beneficiaries. It is noteworthy that although
Bolsa Família Program helps improving the living conditions of these families, it is not enough to guarantee food security by itself, as evidenced by other studies.
7,29The present study has some limitations. First, its cross-sectional nature does not enable any causal inferences; second, its sample size may explain the lack of significance observed in some investigated variables. However, it is worth highlighting the use of children’s social network as strong point in the current study, since it can differ from their mother’s social network. For example, children of divorced parents can incorporate the social network of their new families.
The herein presented results suggested inverse association among children’s daily social network, maternal schooling and food insecurity levels. Given the food insecurity pervasiveness observed in this population, it is essential understanding its etiology and identifying ways to make interventions focused on improving its nutrition and health and, consequently, its malnutrition condition. Interventions aimed at strengthening instrumental, among other forms of support between small social networks can help improving the health and nutritional status of malnourished children living under food insecurity condition.
AcknowledgementThe authors are grateful to all children and mothers who participated in the current study, as well as to the institution - Center for Nutritional Recovery and Education of Alagoas State - for accepting to participate in it.
References1. França MSD, Lopes MVDO, Frazão CMFDQ, Guedes TG, Linhares FMP, Pontes CM. Características de la red social de apoyo ineficaz: revisión integrativa. Rev Gaúcha Enferm. 2018; 39: e20170303.
2. Kennedy-Hendricks A, Schwartz HL, Griffin BA, Burkhauser S, Green HD, Kennedy DP,
et al. Health implications of social networks for children living in public housing. Health Place. 2015 Nov; 36: 145-51.
3. Morais NA, Koller S, Raffaelli M. Rede de apoio, eventos estressores e mau ajustamento na vida de crianças e adolescentes em situação de vulnerabilidade social. Univ Psychol. 2012; 11 (3): 779-91.
4. Higashi RT, Lee SC, Pezzia C, Quirk L, Leonard T, Pruitt SL. Family and social context contributes to the interplay of economic insecurity, food insecurity, and health. Ann Anthropol Pract. 2017 Nov; 41 (2): 67-77.
5. Kepple AW, Segall-Corrêa AM. Conceptualizing and measuring food and nutrition security. Ciênc Saúde Colet. 2011 Jan; 16 (1): 187-99.
6. Santos TG, Silveira JAC, Longo-Silva G, Ramires EKNM, Menezes RCE. Tendência e fatores associados à insegurança alimentar no Brasil: Pesquisa Nacional por Amostra de Domicílios 2004, 2009 e 2013. Cad Saúde Pública. 2018; 34 (4): e00066917.
7. Costa NS, Santos MO, Carvalho CPO, Assunção ML, Ferreira HS. Prevalence and Factors Associated with Food Insecurity in the Context of the Economic Crisis in Brazil. Curr Dev Nutr. 2017; 1 (10): e000869.
8. Wells JC, Sawaya AL, Wibaek R, Mwangome M, Poullas MS, Yajnik CS,
et al. The double burden of malnutrition: aetiological pathways and consequences for health. Lancet. 2020 Jan; 395 (10217): 75-88.
9. Tsai AC, Bangsberg DR, Emenyonu N, Senkungu JK, Martin JN, Weiser SD. The social context of food insecurity among persons living with HIV/AIDS in rural Uganda. Social Sci Med. 2011 Dec; 73 (12): 1717-24.
10. Perkins JM, Subramanian SV, Christakis NA. Social networks and health: a systematic review of sociocentric network studies in low- and middle-income countries. Soc Sci Med. 2015 Jan; 125: 60-78.
11. FAO, FIDA, UNICEF, PMA, OMS. El estado de la seguridad alimentaria y la nutrición en el mundo 2018. Fomentando la resiliencia en aras de la paz y la seguridad alimentaria. Rome: FAO; 2018. [access in 2021 out 1]. Available from:
https://www.fao.org/3/I9553ES/i9553es.pdf12. Betebo B, Ejajo T, Alemseged F, Massa D. Household food insecurity and its association with nutritional status of children 6–59 months of age in east Badawacho District, south Ethiopia. J Environm Public Health. 2017; 2017: 6373595
13. World Health Organization (WHO). WHO Child Growth Standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva: WHO; 2006. [access in 2021 out 1]. Available from:
https://www.who.int/publications/i/item/924154693X14. Associação Brasileira de Empresas de Pesquisa (ABEP). Critério Brasil 2018. [access in 2021 out 1]. Available from:
https://www.abep.org/criterio-brasil15. Segall-Corrêa AM, Marin-León L, Melgar-Quiñonez H, Pérez-Escamilla R. Refinement of the Brazilian Household Food Insecurity Measurement Scale: Recommendation for a 14-item EBIA. Rev Nutr. 2014; 27 (2): 241-51.
16. Mitchinson AR, Kim HM, Geisser M, Rosenberg JM, Hinshaw DB. Social connectedness and patient recovery after major operations. J Am Coll Surg. 2008 Feb; 206 (2): 292-300.
17. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2017-2018: análise da segurança alimentar no Brasil. Rio de Janeiro: IBGE; 2020. [access in 2021 out 1]. Available from:
https://biblioteca.ibge.gov.br/visualizacao/livros/liv101749.pdf18. Nagata JM, Fiorella KJ, Salmen CR, Hickey MD, Mattah B, Magerenge R,
et al. Around the table: food insecurity, socioeconomic status, and instrumental social support among women living in a rural Kenyan island community. Ecol Food Nutr. 2015; 54 (4): 358-69.
19. Becquey E, Delpeuch F, Konaté AM, Delsol H, Lange M, Zoungrana M,
et al. Seasonality of the dietary dimension of household food security in urban Burkina Faso. Br J Nutr. 2012; 107 (12): 1860-70.
20. Silva EKPD, Medeiros DSD, Martins PC, Sousa LDA, Lima GP, Rêgo MAS,
et al. Insegurança alimentar em comunidades rurais no Nordeste brasileiro: faz diferença ser quilombola? Cad Saúde Pública. 2017; 33: e00005716.
21. Arsenault JE, Yakes EA, Munirul I, Hossain MB, Tahmeed A, Hotz C. Very low adequacy of micronutrient intakes by young children and women in rural Bangladesh is primarily explained by low food intake and limited diversity. J. Nutr. 2013 Feb; 143 (2): 197-203.
22. Mahlmeister RS, Ferreira SG, Veloso FA, Menezes-Filho NA, Komatsu BK. Revisitando a mobilidade intergeracional de educação no Brasil. Rev Bras Econ. 2019; 73 (2): 159-80.
23. Getacher, L, Egata, G, Aynalem, YA, Molla A, Tesfaye A, Abebe H,
et al. Food insecurity and its predictors among lactating mothers in North Shoa Zone, Central Ethiopia: a community based cross-sectional study. BMJ Open. 2020; 10: e040627.
24. Chowdhury MRKC, Khan MMH, Islam MR, Perera NKP, Shumack MK, Kader M. Low maternal education and socio economic status were associated with household food insecurity in children under five with diarrhoea in Bangladesh. Acta Paediatr. 2016 May; 105 (5): 555-61.
25. Stewart CP, Iannotti L, Dewey KG, Michaelsen KF, Onyango AW. Contextualising complementary feeding in a broader framework for stunting prevention. Matern Child Nutr. 2013 Sep; 9 (Supl. 2): 27-45.
26. Anschau FR, Matshuo T, Segall-Corrêa AM. Insegurança alimentar entre beneficiários de programas de transferência de renda. Rev Nutr. 2012; 25 (2): 177-89.
27. Agho KE, Mukabutera C, Mukazi M, Ntambara M, Mbugua I, Dowling M,
et al. Moderate and severe household food insecurity predicts stunting and severe stunting among Rwanda children aged 6–59 months residing in Gicumbi district. Matern Child Nutr. 2019 Jul; 15 (3): e12767.
28. Cabral MJ, Vieira KA, Sawaya AL, Florêncio TMMT. Perfil socioeconômico, nutricional e de ingestão alimentar de beneficiários do Programa Bolsa Família. Estud Av. 2013; 27 (78): 71-87.
29. Cotta RMM, Machado JC. Programa Bolsa Família e segurança alimentar e nutricional no Brasil: revisão crítica da literatura. Rev Panam Salud Pública. 2013; 33: 54-60.
Received on April 21, 2021
Final version presented on May 2, 2022
Approved on June 10, 2022
Authors’ contribution: Barros LKN: data collection, statistical analysis, results’ interpretation and for coordinating the research. Clemente APG and Britto RPA: critical review of the intellectual content, approved the final version of the manuscript and co-coordinated the research. Bueno NB, Pureza IROM and Silva-Neto LGR: statistical analysis, interpreted the research results, approved the final version of the manuscript and co-coordinated the research. Santos MRC: data collection and statistical analysis. Florêncio TMMT: statistical analysis, results’ interpretation, critical review of intellectual content, and coordinated the research.
All authors approved the final version of the article and declare no conflict of interest.


 ; Ana Paula Grotti Clemente2
; Ana Paula Grotti Clemente2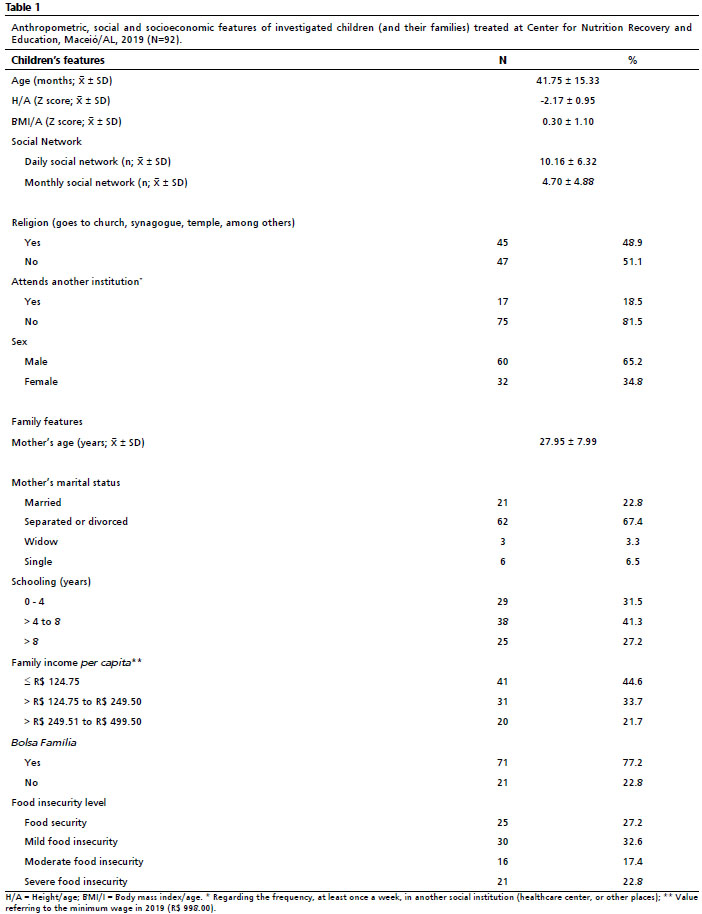






 Ler em português
Ler em português