ABSTRACT
OBJECTIVES: to identify variables associated with the presence of a companion in the delivery room and its association with breastfeeding (BF) in the first hour of life.
METHODS: cross-sectional analysis of data from a cohort study (n=344). To investigate the factors associated with the presence of a companion during childbirth and breastfeeding in the first hour; we performed Poisson regression analyses, considering p<0.05 as the level of statistical significance.
RESULTS: 93.9% of the pregnant women had a companion in the delivery room, and no association was found between socioeconomic, obstetric and neonatal characteristics of the mother-child binomial and the presence of a companion. In a univariate analysis, the absence of a companion reduced the frequency of breastfeeding in the first hour (PR=0.64; CI95%=0.42-0.96), a result that was not confirmed in the adjusted analyses (PR=0.79; CI95%=0.54-1.15). Secondly, it was identified that the five minutes Apgar score was associated with first hour breastfeeding (PR=1.27; CI95%=1.14-1.40) regardless of the other factors.
CONCLUSIONS: most women in the cohort had a companion in the delivery room, with no differences according to socioeconomic, obstetric and neonatal variables. The frequency of first hour breastfeeding was high; however, it was lower in the absence of a companion but this association was not independent of other factors.
Keywords:
Breastfeeding, Pregnant women, Infant
RESUMO
OBJETIVOS: identificar variáveis associadas à presença de acompanhante na sala de parto e sua associação com o aleitamento materno (AM) na primeira hora de vida.
MÉTODOS: análise transversal de dados provenientes de um estudo de coorte (n=344). Para investigação dos fatores associados entre a presença de companhia durante o parto e o AM na primeira hora foram realizadas análises de regressão de Poisson, considerando p<0,05 como nível de significância estatística.
RESULTADOS: 93,9% das parturientes tiveram acompanhante na sala de parto, não sendo encontrada associação entre características socioeconômicas, obstétricas e neonatais do binômio mãe-filho e esta presença. Em análise univariada, a ausência de acompanhante reduziu a frequência de AM na primeira hora (RP=0,64; IC95%=0,42-0,96), resultado que não se confirmou nas análises ajustadas (RP=0,79; IC95%=0,54-1,15). Secundariamente, identificou-se que o Apgar no quinto minuto associou-se com AM na primeira hora (RP=1,27; IC95%=1,14-1,40) independentemente dos demais fatores.
CONCLUSÕES: a maioria das mulheres da coorte contou com acompanhante na sala de parto, sem diferenças segundo variáveis socioeconômicas, obstétricas e neonatais. A frequência de AM na primeira hora também foi alta e menor na ausência de acompanhante, contudo, essa associação não se mostrou independente de outros fatores.
Palavras-chave:
Aleitamento materno, Parturiente, Recém-nascido
IntroductionLabor and delivery are human experiences that involve physical, psychological and social changes
1; therefore, they should be regarded as crucial for early breastfeeding. In this connection, the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) recommend that breastfeeding (BF) be started in the first hour of life; exclusive breastfeeding be practiced until the infant's sixth month of life; and, after this period, the child should continue to be breastfed, with complementary foods, until two years of age or more.
2The indicator of breastfeeding in the first hour of life is classified by WHO as poor (0 - 29%), fair (30 - 49%), good (50 - 89%), and very good (90 - 100%). According to data released by the
Estudo Nacional de Alimentação e Nutrição Infantil (ENANI, National Child Food and Nutrition Study),
4 the prevalence of breastfeeding in the first hour of life in children under two years of age was 62.4% in Brazil from 2019 to 2020; the highest prevalence was observed in the Northern region (73.5%), followed by the Midwest (64.0%) and Northeast (63.2%). The southern (61.8%) and southeastern (58.5%) regions had the lowest prevalence.
The practice of breastfeeding in the first hour of life is a protective factor against neonatal deaths,
5 besides increasing the probability of exclusive breastfeeding up to six months, as well as lasting up to two years of life or more.
6 However, care that the woman receives during childbirth, as well as the quality of her own experience, may influence breastfeeding in early life.
1A birth companion is recommended by the WHO guidelines dated 2012, 2014, 2015 and 2018 that provide "Recommendations for intrapartum care for a positive childbirth experience".
7 Along this line, in Brazil, the Companion Act determines that the health services of the
Sistema Único de Saúde (SUS, Government Health System) or of the SUS affiliated network, should allow pregnant women to be accompanied during the entire period of labor, delivery and postpartum. The law determines that the companion will be indicated by the pregnant woman and may be the baby's father, the current partner, the mother, a friend, or another person of her choice.
8Women are less likely to suffer mistreatment and abuse when supported by a companion of their choice during labor.
9 A systematic review has shown that companionship helps women to have a positive birth experience, unlike unaccompanied women who referred to the lack of support as a form of suffering, stress and fear, making childbirth a difficult experience.
10 A national population-based study found that 77% of women who breastfed in the first hour of their baby's life received social support, defined as the presence of a companion, against 23% without social support.
11Another study from the national survey
Nascer no Brasil revealed that the delivery companion can be considered a provider of safety, quality of care and respect for the rights of women in care, helping the parturient to have a positive childbirth experience and also allowing favorable repercussions concerning the initiation and duration of breastfeeding.
12 Depriving women of their right to be accompanied in labor, delivery and post-partum is one of the ways of committing obstetric violence. Women must be clearly informed in advance about this right, enabling the selection and participation of her companion.
13As a result of the COVID-19 pandemic outbreak in March 2020, several restrictions were imposed; the limitation of the companion presence in the delivery room occurred in different hospitals with unfavorable outcomes. In a descriptive, cross-sectional, multicenter study, the presence of a companion was prohibited in the delivery room in 83.3% of the health centers. This measure was challenged since such restriction increases maternal anxiety, which may be harmful to labor and birth.
14In a retrospective study carried out in a public hospital in Hong Kong, it was observed that babies born to women without the continuous support of a companion during the COVID-19 period had a reduced first hour breastfeeding rate when compared to newborns of women followed up during an equal period of the previous year.
15Therefore, the objective of the present study was to identify the variables associated with the presence of a companion in the delivery room and to study the association of this presence and breastfeeding in the first hour of life in a cohort of pregnant women and infants.
MethodsThis is a cross-sectional analysis of data from a cohort study of pregnant women assisted in the 20 health units of the primary health care network in Botucatu, a medium-sized city in the interior of the state of São Paulo. These pregnant women were monitored from mid-pregnancy until delivery and the first childcare visit of the newborn, from May 2018 to June 2019.
The matrix project formed a cohort of 466 pregnant women. Inclusion criteria were: be literate, residing in the urban area of the municipality and presenting physical and cognitive conditions to participate in face-to-face and telephone interviews, that is, to understand and answer the questions clearly asked. In the present study, pregnant women/mothers of twin infants and women or their children who had conditions that hinder or prevent breastfeeding, such as positive serology for HIV, cleft lip and palate, heart malformations, among others, were excluded. In addition the number of postpartum women was limited due to the lack of entries in the medical records used. Thus, the data provided by companions in the delivery room formed the sample of the present study, totaling 344 mothers.
In addition to the interview at the basic health units, part of the data on pregnancy, delivery and birth were collected at the maternity hospital at the
Hospital das Clínicas de Botucatu, the only public hospital in the municipality and, therefore, where all births charged to SUS occurred. Such data were complemented by an interview carried out at the public neonatal care unit called
Clínica do Bebê, where the first childcare visit and neonatal screening tests for newborns in the municipality are held. The population coverage of
Clinica do Bebê is high, involving about 85% of all births in the city.
16Recruitment of pregnant women for the cohort study took place from May to September 2018 and data collection took place in four stages: 1) Recruitment of pregnant women and their inclusion in the cohort by the Health Unit team itself; 2) Telephone interview within 15 days after recruitment, to collect data on socioeconomic and demographic conditions, social support and pregnancy planning or desire, among others; 3) Obtaining data on the mother's obstetric history, on the evolution of the pregnancy and on the newborns from the health records of the health units where those pregnant women received prenatal care and, from the electronic records, at the maternity hospital where the deliveries took place; 4) Data collection related to breastfeeding practices from the
Clinica doBebê medical records.
The main exposure variable was the presence of a companion in the delivery room and the investigated outcome was breastfeeding in the first hour of life. In addition, variables associated with the presence/absence of a companion in the delivery room were investigated; such variables may also influence the outcome of the interest (breastfeeding in the first hour of life) and thus exert some confounding effect on the association under investigation. These were: socioeconomic factors (mother's age and education, skin color, living with a partner, working outside the home, receiving a family allowance); obstetrics (parity, being part of a group of pregnant women, smoking during pregnancy, drinking alcohol during pregnancy, number of prenatal visits, social support during pregnancy - measured by the Medical Outcome Scale-Social Support (MOS-SSS), which consists of 19 items answered on a five-point Likert-type scale and aims to assess the extent to which the person has the support of others to face different situations in their life,
17 type of delivery, labor of preterm delivery, five minutes Apgar score, gestational age and infants birth weight; mother-child neonatal ratios (skin-to-skin contact and skin-to-skin time).
The presence of a companion in the delivery room was categorized in a dichotomous way (yes or no). When there was a companion, his/her description was also considered. In this case, the categories were: husband/partner; mother/mother-in-law/grandmother; another relative; friend/neighbor or other unrelated person.
Descriptive analyses on the presence of a companion in the delivery room, who this companion was, as well as the socioeconomic, obstetric and neonatal variables of the mother-child binomial to characterize the sample were carried out.
The investigation of the association between socioeconomic, obstetric and neonatal variables of the mother-child binomial and the presence of a companion in the delivery room was performed using Poisson regression. Those associations that presented
p<0.20 in the univariate analysis were included in a multivariate model to investigate their effect independently of the others, considering
p<0.05 as the level of statistical significance.
The investigation of the association between a companion in the delivery room and breastfeeding in the first hour of the infant's life was also performed using Poisson regression models. In the multivariate analyses, true confounders were included, that is, those that were associated (
p<0.05) or presented (
p<0.20) with the exposure variable of interest (companion in the delivery room) and also with the outcome in question, as they may eventually act as confounding factors for the association of interest. Final results were presented as prevalence ratios (PR) with 95% confidence intervals (CI95%) and
p values, considering
p<0.05 as the level of statistical significance. The Statistical Package of Social Science for Windows (SPSS) software, version 20.0, was used to perform the statistical analyses.
The study was approved by the Ethics Committee of the
Faculdade de Medicina de Botucatu (CAAE: 88314318.3.0000.5411).
ResultsTable 1 presents the results of the descriptive analyses of the presence of a companion in the delivery room, as well as the socioeconomic, obstetric and neonatal variables of the mother-child binomial to characterize the sample.
Out of the total 344 postpartum women evaluated, 93.9% were accompanied in the delivery room. Husband or partner was the most frequent companion (63.5%), followed by mother or mother-in-law (21.3%). About 13% of the women had another relative as companion during childbirth and 2.2% had a friend or neighbor (data not presented in tables).
Out of the total number of postpartum women in the cohort, 4.2% were younger than 18 years, 85.9% were between 18 and 35 years old, and 9.9% were 35 years old or older. The majority (82.7%) had less than eight years of study, 51.4% reported white skin color, 16.4% participated in an income transfer program (
Bolsa Família) and 81.9% lived with a partner. The rate of women working outside home was 46.5%. Most were in their first pregnancy (45.9%). The rate of women who reported not having smoked or consumed alcohol during pregnancy was 81.8% and 94%, respectively (Table 1).
Out of the total number of postpartum women assessed, 58.4% had had vaginal delivery and for 94.6% of the women delivery occurred at 37 weeks or more of gestational age. The percentage of infants' weight in the range of 2500 to 4000 grams at birth was 86.9%. About 98.5% of the babies had five minutes Apgar scores >7 points, 79.9% were breastfed in the first hour and 57.9% were placed in skin-to-skin contact with the mother soon after birth (Table 1).
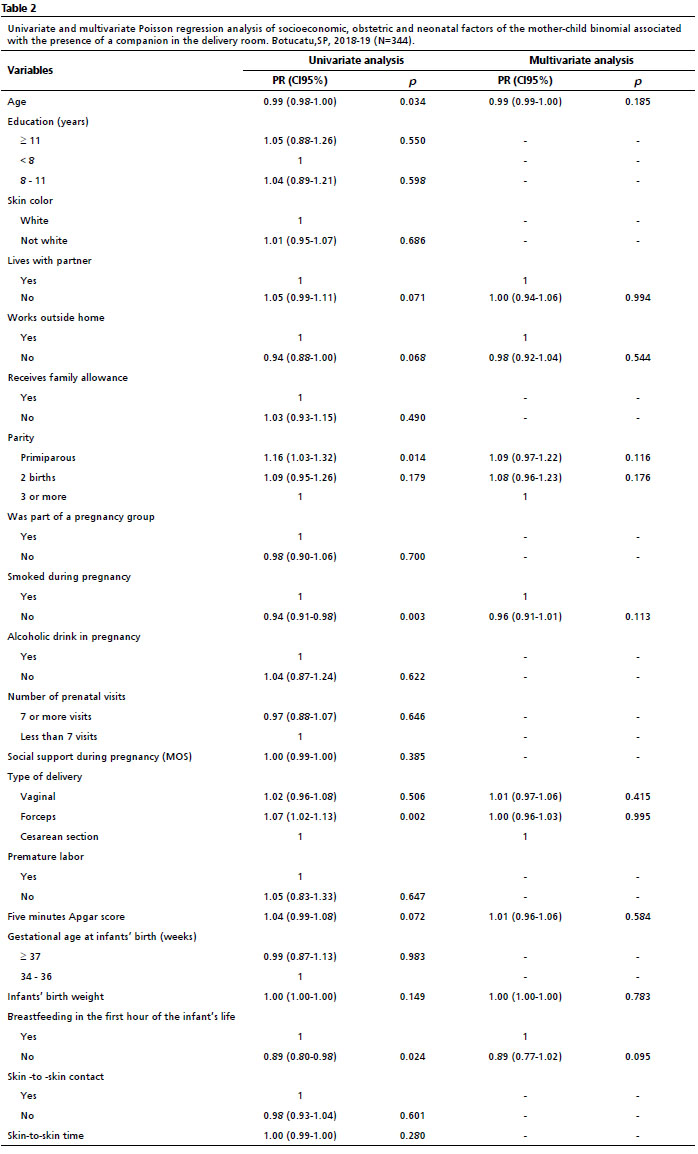
Table 2 presents the results of the association analyses of the socioeconomic, obstetric and neonatal variables of the mother-child binomial with a companion in the delivery room. Regarding socioeconomic/demographic variables, only maternal age was statistically associated with the presence of a companion in the delivery room in the univariate analysis. Living with a partner and working outside home were selected as adjustment variables for the multivariate analysis (
p<0.20). Regarding the obstetric and neonatal variables of the mother-child binomial, parity, smoking during pregnancy, type of delivery and breastfeeding in the first hour of the baby's life were statistically associated with the outcome of interest, with the infant's birth weight (BW) also included in the multivariate analysis, as it had presented
p<0.20 in the univariate analysis. In the multivariate analysis, no variable was independently associated with the situation of a companion in the delivery room.
Table 3 presents the results of the univariate and multivariate analyses that investigated the association between a companion in the delivery room and BF in the first hour of infants' life. Considering the univariate analyses, those parturients without a companion in the delivery room had a lower prevalence of BF in the first hour of infants life when compared to those who had a companion (PR=0.64; CI95%=0.42-0.96;
p<0,0.34). Working outside the home, social support during pregnancy, type of delivery, five minutes Apgar score and skin-to-skin contact were associated (
p<0.05) with BF in the first hour of infants' life, while gestational age (GA) and infants' BW, reached the statistical criterion defined for a variable potentially capable of exerting a confounding effect (
p<0.20) on the association of interest. In the multivariate analysis, a companion in the delivery room no longer had a statistically significant association with first hour infant's breastfeeding (PR=0.79; CI95%=0.54-1.15). Among the variables included as adjustment factors, five minutes Apgar scores were independently associated with BF in the first hour of the baby's life (PR=1.27; CI95%=1.14-1.40;
p<0.01); that is, each additional point on the five minutes Apgar score increased the prevalence of this outcome by 27%.
In our study, we could verify that the absence of a companion reduced the prevalence of BF in the first hour of the infant's life, but this result was significant in the univariate analysis, that is, its effect was not independent of the other variables inserted in the multiple models as potential confounders . Thus, the predicted hypothesis was not confirmed in the study population. Further, it was observed that a five minutes higher Apgar score increased the prevalence of BF in the first hour of the infant's life. It is worth noting that no association was found between socioeconomic, obstetric and neonatal characteristics of the mother-child binomial associated with the presence of a companion in the delivery room. It is possible that the effects of the absence of a companion are due to factors that have not been reviewed.
A cross-sectional study carried out in hospitals in the state of Santa Catarina showed that unaccompanied puerperal women had 2.13 times higher prevalence of being tied up during childbirth. Among women who underwent vaginal delivery, the prevalence of being submitted to non-pharmacological maneuvers, receiving analgesia and being able to choose the position for delivery were, respectively, 96%, 189% and 63% higher among mothers who were with a companion.
18Allowing women to have a companion of their choice to offer physical and/or emotional support during labor, delivery and the immediate postpartum period is among the practices of the global Woman-Friendly Care criterion, which is part of the set of goals established by the Baby-Friendly Hospital Initiative.
19 The prevalence of a companion in the delivery room found in the current study (93.9%) was higher than that revealed by the
Nascer no Brasil study conducted in 2011 (46.4%) and by the Cegonha Network Assessment. held in 2017 (84.7%).
20Hence, the good performance of the health staff of the municipality where the present study was carried out ensuring the parturient's right to have the presence of a companion of her choice during childbirth should be pointed out. The woman's husband or partner was identified as the most frequent companion, similar to other studies.
21,22 Satisfaction with the childbirth experience is significantly higher in women who could count on the presence of one or more supporting people.
23 Wilson
et al.
24 highlighted the improvement in the labor process of women who were accompanied.
Skin-to-skin contact and breastfeeding in the first hour of life are practices that impact the neonatal adaptation process, strengthening the bond between mother and baby and preventing early neonatal complications, such as neonatal hypothermia and hypoglycemia.
25 In our study the prevalence of breastfeeding in the first hour of infant's life was higher when compared to the findings of ENANI-2019 referring to Brazil (62.4%) and to the Southeast region (58.5%).
4Among the possible explanations to understand why the absence of a companion does not have an independent adverse effect on the occurrence of breastfeeding in the first hour after the infant's birth, the sample size can be pointed out as it is small enough to assess a condition with low prevalence; hence, the study in question may not have had the statistical power to find such an association. The same result and explanatory hypothesis were presented in the research by Martins
et al.
26In the present study, the five minutes Apgar score was the only variable significantly associated with BF in the first hour of the infant's life. Results from other studies also found an association between the five minutes Apgar score and factors related to the initiation of breastfeeding; however, they also observed the influence of other factors.
Bryanton
et al.
27 found maternal weight at hospital admission, gestational age at delivery and the five minutes Apgar score as factors significantly associated with the effective initiation of breastfeeding up to approximately 36 hours after birth. Boakye-Yiadom
et al.
28 found that advancing maternal age, first-born neonates, rooming-in of the newborn with the mother, administration of infant formulas and higher five minutes Apgar scores were determinants of the time of breastfeeding initiation.
Still in connection with BF in the first hour of infant's life in other locations, different factors have been identified, but none was found that investigated the influence of the presence of a companion. A cross-sectional study, comprising 727 pregnant women, who delivered at a Baby-Friendly Hospital, found an association between BF in the first hour after the infant's birth and full-term birth, birth weight ≥ 2500g, Apgar score > 7 in the first minute, vaginal delivery, six or more prenatal visits, beginning prenatal care in the first trimester, skin-to-skin contact, and multiparity.
25On the other hand, a study carried out in Bangladesh found that early initiation of breastfeeding was higher among lower family income and schooling groups.
29 A study that reviewed health surveys in 58 low- and middle-income countries revealed vaginal delivery in a health facility associated with an increased risk of delayed initiation of breastfeeding in 26 countries, with women who delivered at home being less likely to delay breastfeeding initiation. However, cesarean delivery showed a higher risk of late breastfeeding initiation in all countries studied.
30It is important to consider that this study was carried out with a sample of mothers and babies assisted in the same SUS maternity, in which the practices and management offered were possibly, the same, reflecting a specific reality. Thus, studies in other locations, and considering larger samples, should still investigate the role of the absence of a companion on the occurrence of BF in the first hour of the infant's life. This understanding is necessary so that the positive effect on the chances of adequate breastfeeding initiation can be included (or discarded) in the list of benefits concerning the presence of a companion freely appointed by the mother during her labor and delivery. In addition, as previously indicated, there was a limitation in the sample size due to the lack of entries in the medical records used.
In summary, most women in the cohort had a companion of their choice in the delivery room, with no differences in relation to socioeconomic, obstetric and neonatal variables. The frequency of the first hour breastfeeding after the infant's birth was also high yet lower in the absence of a companion. Nevertheless, this association was not independent of other factors, losing statistical significance when other factors associated with breastfeeding in the first hour of the infant's life were considered.
References1. Diniz CSG, D'Orsi E, Domingues RMSM, Torres JA, Dias MAB, Schneck CA, Lansky S, Teixeira NZF, Rance S, Sandall J. Implementation of the presence of companions during hospital admission for childbirth: data from the Birth in Brazil national survey. Cad Saúde Pública. 2014; 30: 140-53.
2. World Health Organization (WHO). Department of Nutrition for Health and Development. Guideline: protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services. Geneva: WHO; 2017. [access in 2022 mar 3]. Available from:
https://www.who.int/publications/i/item/97892415500863. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: Aleitamento Materno e Alimentação Complementar. 2
nd ed. Brasília (DF): Ministério da Saúde; 2015. [access in 2022 jan 31]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/saude_crianca_aleitamento_materno_cab23.pdf4. Universidade Federal do Rio de Janeiro (UFRJ). Aleitamento materno: Prevalência e práticas de aleitamento materno em crianças brasileiras menores de 2 anos 4: ENANI 2019. [access in 2022 jan 31]. Available from:
https://enani.nutricao.ufrj.br/index.php/relatorios/5. Boccolini CS, Carvalho ML, Oliveira MIC, Pérez-Escamilla R. A amamentação na primeira hora de vida e mortalidade neonatal. J Pediatr (Rio J. ). 2013; 89: 131-6.
6. UNICEF, WHO. Capture the Moment - Early initiation of breastfeeding: The best start for every newborn. New York: UNICEF; 2018.
7. World Health Organization (WHO). WHO recommendations: intrapartum care for a positive childbirth experience. Geneva: WHO; 2018. [access in 2022 jan 31]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/260178/9789241550215-eng.pdf8. Brasil. Lei nº 11.108, de 7 de abril de 2005. Altera a Lei nº 8.080, de 19 de setembro de 1990. Brasília (DF): DOU de 7 abr. 2005. [access in 31 jan 2022]. Available from:
http://www.planalto.gov.br/ccivil_03/_ato2004-2006/2005/lei/l11108.htm. 9. Diamond-Smith N, Sudhinaraset M, Melo J, Murthy N. The relationship between women's experiences of mistreatment at facilities during childbirth, types of support received and person providing the support in Lucknow, India. Midwifery. 2016; 40: 114-23.
10. Bohren MA, Berger BO, Munthe-kaas H, Tunçalp O. Perceptions and experiences of labour companionship: a qualitative evidence synthesis. Cochrane Database Syst Rev. 2019 Mar; 3 (3): CD012449.
11. Seehausen MP, Pérez-Escamilla R, Oliveira MIC, Leal MC, Boccolini CS. Social support modifies the association between pre-pregnancy body mass index and breastfeeding initiation in Brazil. Plos One. 2020 May; 15 (5): e0233452.
12. Diniz CSG, D'orsi E, Domingues RMSM, Torres JA, Dias MAB, Schneck CA, Lansky S, Teixeira NZF, Rance S, Sandall J. Implementação da presença de acompanhantes durante a internação para o parto: dados da pesquisa nacional Nascer no Brasil. Cad Saúde Pública. 2014; 30: 140-53.
13. Almeida NMO, Ramos, EMB. O direito da parturiente ao acompanhante como instrumento de prevenção à violência obstétrica. Cad Ibero-amer. 2020; 9: 12-27.
14. Gonçalves-Ferri WA, Pereira-Cellini FM, Coca K, Aragon DC, Nader PJH, Lyra JC,
et al. The impact of coronavirus outbreak on breastfeeding guidelines among Brazilian hospitals and maternity services: a cross-sectional study. Int Breastfeed J. 2021; 16: 2-11.
15. Mok YK, Cheung KW, Wang W, Li RHW, Shek NWM, Ng EHY. The effects of not having continuous companion support during labour on pregnancy and neonatal outcomes during the COVID-19 pandemic. Midwifery. 2022 May; 108: 1-5.
16. Prefeitura Municipal de Botucatu. Secretaria Municipal de Saúde. Manual de procedimento Operacional Padrão: Clínica do Bebê. Botucatu; 2012.
17. Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991; 32: 705-14.
18. Tomasi YT, Saraiva SS, Boing AC, Delziovo CR, Wagner KJP, Boing AF. Do pré-natal ao parto: um estudo transversal sobre a influência do acompanhante nas boas práticas obstétricasno Sistema Único de Saúde em Santa Catarina, 2019. Epidemiol Serv Saúde. 2021; 30 (1): 1-12.
19. Lamounier JA, Chaves RG, Rego MAS, Bouzada MCF. Iniciativa Hospital Amigo da Criança: 25 anos de experiência no Brasil. Rev Paul Pediatr. 2019; 37: 486-93.
20. Brasil. Fiocruz. Atenção ao Parto e Nascimento em Maternidades da Rede Cegonha. Sumário Executivo. 2021. [access in 2022 jan 31]. Available from:
https://nascernobrasil.ensp.fiocruz.br/wp-content/uploads/2021/05/Avaliacaoredecegonha_Sumario.pdf21. Anjos AM, Gouveia HG. Presença do acompanhante durante o processo de parturição e nascimento: análise da prática. Rev Enferm UERJ. 2019; 27: 1-8.
22. Morhason-Bello IO, Adedokun BO, Ojengbede OA, Olayemi O, Oladokun A, Fabamwo AO. Assessment of the effect of psychosocial support during childbirth in Ibadan, south-west Nigeria: A randomised controlled trial. Aust N Z J Obstet Gynaecol. 2009; 49 (2): 145-50.
23. Preis H, Mahaffey B, Heiselman C, Lobel M. The impacts of the COVID-19 pandemic on birth satisfaction in a prospective cohort of 2.341 U.S. women. Women Birth. 2022; 35: 458-65.
24. Wilson AN, Melepia P, Suruka R, Hezeri P, Kabiu D, Babona D,
et al. Partnership-defined quality approach to companionship during labour and birth in East New Britain, Papua New Guinea: A mixed-methods study. PLOS Glob Public Health. 2022; 2:1-17.
25. Araújo KEAS, Santos CC, Caminha MFC, Silva SL, Pereira JCN, Filho MB. Skin to skin contact and the early initiation of breastfeeding: a cross-sectional study. Texto Contexto Enferm. 2021; 30: 1-14.
26. Martins ACM, Giugliani ERJ, Nunes LN, Bizon AMBL, Senna AFK, Paiz JC, et al. Factors associated with a positive childbirth experience in Brazilian women: A cross-sectional study. Women Birth. 2020. [access in 2022 jan 31]. Available from:
https://doi.org/10.1016/j.wombi.2020.06.00327. Bryanton J, Montelpare W, Drake P, Drake R, Walsh D, Larter K. Relationships Among Factors Related to Childbirth and Breastfeeding Outcomes in p primiparous Women. JOGNN. 2020; 49: 437-51.
28. Boakye-Yiadom AP, Nguah SB, Ameyam E, Enimil A, Wobil PNL, Plange-Rhule G. Timing of initiation of breastfeeding and its determinants at a tertiary hospital in Ghana: a cross-sectional study. BMC Pregnancy Childbirth. 2021; 21: 1-9.
29. Ekholuenetale M, Mistry SK, Chimoriya R, Nash S, Doyizode AM, Arora A. Socioeconomic inequalities in early initiation and exclusive breastfeeding practices in Bangladesh: findings from the 2018 demographic and health survey. Int Breastfeed J. 2021; 16: 2-18.
30. Raihana S, Alam A, Chad N, Huda TM, Dibley MJ. Delayed Initiation of Breastfeeding and Role of Mode and Place of Childbirth: Evidence from Health Surveys in 58 Low- and Middle- Income Countries (2012-2017). Int J Environ Res Public Health. 2021; 18: 2-19.
Received on June 2, 2022
Final version presented on January 8, 2023
Approved on February 7, 2023
Associated Editor: Sheyla Costa
Authors’ contribution: Araujo LR, Carvalhaes MABL and Gomes CB contributed to the design of the article. Araujo LR carried out the data collection. Statistical analysis was performed by Araujo LR and Gomes CB. All authors approved the final version of the article and declare that there is no conflict of interest.
Acknowledgment: To the
Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, State of São Paulo Research Foundation) for granting a scientific initiation fellowship to ARAUJO LR (2020/13276-8).


 ; Maria Antonieta de Barros Leite Carvalhaes2
; Maria Antonieta de Barros Leite Carvalhaes2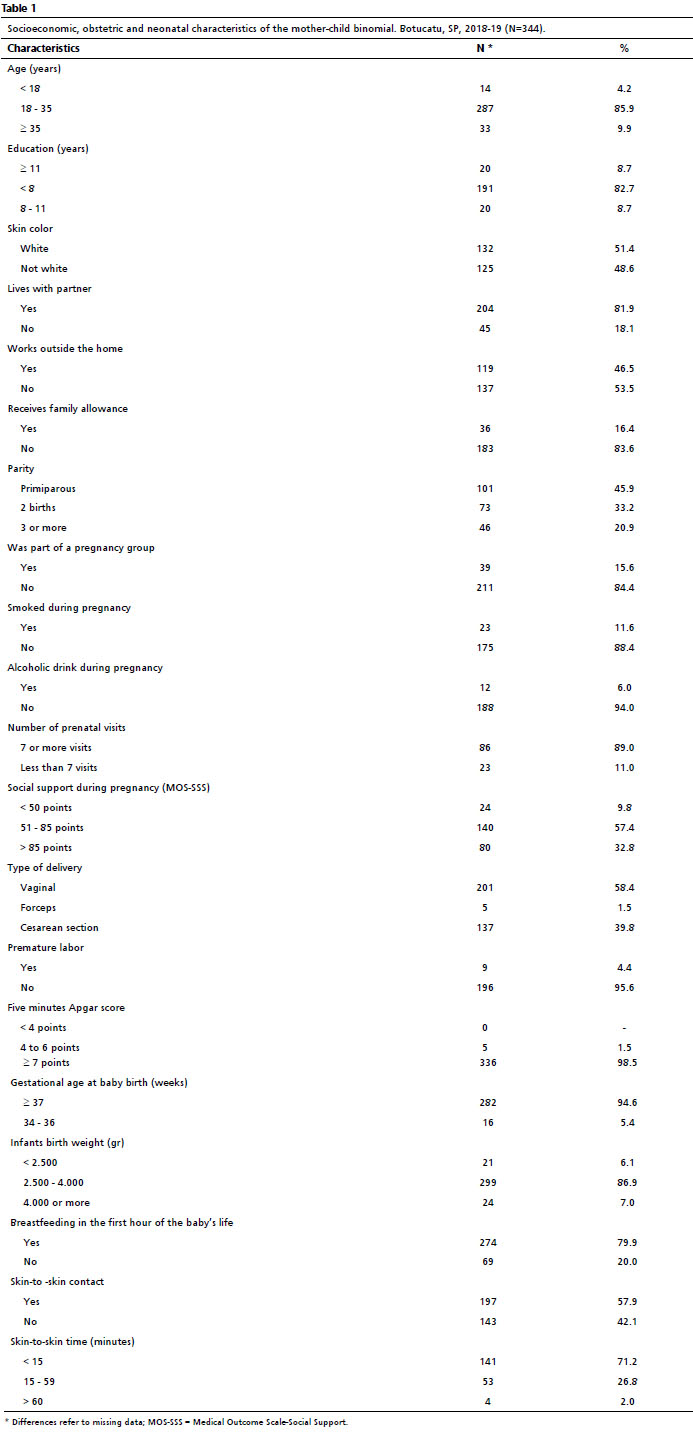







 Ler em português
Ler em português