ABSTRACT
OBJECTIVES: to evaluate the association between intimate partner physical violence (IPPV) and inadequate gestational weight gain (GWG).
METHODS: cross-sectional study composed of 554 women who attended four Basic Health Units in the city of Rio de Janeiro between 2005 and 2009. The GWG was calculated through the difference between the final weight of pregnancy and pre-gestational weight. For the measurement of IPPV, the Portuguese version of the Conflict Tactics Scales (CTS-1) was used. Data analysis was based on multinomial logistic regression models, estimating odds ratios and respective 95% confidence intervals for associations between the variables of interest.
RESULTS: the prevalence of minor and severe IPPV was 31.6% and 16.3%, respectively. Almost two-thirds of the women had insufficient or excessive GWG. After adjusting the model, it was observed that the presence of IPPV increased by 1.66 (CI95%=1.05-2.64) times the chances of insufficient GWG, compared to couples who did not experience this type of violence. Concerning the excessive GWG, the associations with IPPV were not statistically significant.
CONCLUSION: women who experience IPPV in their relationships are more likely to have insufficient GWG during pregnancy. From this perspective, prenatal care becomes an essential service for screening domestic violence and its possible repercussions.
Keywords:
Weight gain, Pregnancy, Intimate partner violence
RESUMO
OBJETIVOS: avaliar a associação entre violência física entre parceiros íntimos (VFPI) e o ganho de peso gestacional (GPG) inadequado.
MÉTODOS: estudo seccional composto por 554 mulheres que compareceram a quatro Unidades Básicas de Saúde do município do Rio de Janeiro, entre 2005 e 2009. O GPG foi calculado através da diferença entre o peso final da gestação e o peso pré-gestacional. Para a mensuração da VFPI foi utilizada a versão em português da Conflict Tactics Scales (CTS-1). A análise dos dados se baseou em modelos de regressão logística multinomial, estimando-se razões de chance e respectivos intervalos de 95% de confiança para as associações entre as variáveis de interesse.
RESULTADOS: a prevalência de VFPI menor e grave foi 31,6% e 16,3%, respectivamente. Quase dois terços das mulheres apresentaram GPG insuficiente ou excessivo. Após o ajuste do modelo, observou-se que a presença de VFPI aumentou em 1,66 (IC95%=1,05-2,64) vezes as chances de GPG insuficiente, em comparação aos casais que não vivenciaram este tipo de violência. Em relação ao GPG excessivo as associações com VFPI não foram estatisticamente significantes.
CONCLUSÕES: mulheres que vivenciam a VFPI têm maiores chances de apresentarem GPG insuficiente. Nessa perspectiva, o pré-natal passa a ser um serviço fundamental para o rastreamento de violência doméstica e suas possíveis repercussões.
Palavras-chave:
Ganho de peso, Gestação, Violência entre parceiros íntimos
IntroductionThe assessment of gestational weight gain (GWG) is a widely used indicator in health services, as well as in epidemiological studies, for monitoring pregnant women's health status.
1 Inadequate GWG is an important public health problem worldwide, and its consequences may lead to health impairments for both mother and baby.
2The literature mentions some factors that may interfere with adequate GWG, such as age and schooling of women at the moment of pregnancy, ethnicity, marital status, food consumption, pre-gestational nutritional status, intervals between pregnancies and births, socioeconomic, psychosocial factors and those related to a couple's intimate relationship.
2,3 In the latter, intimate partner violence (IPV) stands out.
4,5 Athar
et al. 6 conducted a scoping review assessing nine articles published between 2015 and 2020 and demonstrated that IPV affects gestational weight gain. Another review conducted by Zhou
et al. 7 about determinants of excessive gestational weight gain-including 70 studies published between 2009 and 2020, originated in countries from America, Asia, Europe, Oceania and Africa-demonstrated IPPV as an important risk factor for excessive gestational weight gain.
7It is worth mentioning that IPPV is also an important national and international public health problem, is defined as "any behavior that inflicts or has the possibility of inflicting physical, psychological or sexual harm to those that are in an intimate relationship".
8 Distinct manifestations of violence (psychological, physical or sexual) may coexist within a relationship, in various moments of a couple's life, including pregnancy. A systematic review, published in 2019 and conducted by the Pan American Health Organization (PAHO), aiming to synthetize studies about IPPV prevalence in the Americas, demonstrated that 16.9% of Brazilian women between 15 and 49 years of age experienced physical and/or sexual IPV at any moment of their lives.
9 This review included 25 studies which contemplated estimates of this kind of violence in 24 countries. It is worth mentioning that there is no study at the national level about IPPV prevalence during pregnancy. However, recent surveys about IPPV during pregnancy conducted in the municipalities of Caxias/MA
10 and Rio de Janeiro/RJ
11 registered a prevalence of intimate partner physical violence (IPPV) of 4.3% and 20.4%, respectively. These data evidence the importance of this problem in the country.
The mechanisms that lead to IPV interference in GWG are still not elucidated. Studies about this subject are still scarce, and their results differ.
4,12-17 A longitudinal study conducted with 734 women in the Province of Ilam (Iran) did not observe a significant difference between physical, psychological and sexual violence and gestational weight gain.
16 Other studies point to an association of IPV with excessive GWG,
4,12,13,15 some with insufficient GWG
13-15,17 and a more recent study on the theme, assessing this relation using path analysis, observed the indirect effect of IPV in GWG through depressive symptoms, stress and anxiety experienced by women.
16 The heterogeneity of these factors may be explained by using distinct screening tools for measuring IPV and gestational weight gain, different designs, sample sizes and study populations.
Given the above, expanding knowledge about the subject is necessary, which can help with the generation of new strategies and actions to improve mother and child health. In this sense, this study aimed to assess the association of IPPV during pregnancy with inadequate GWG.
MethodsThis study is part of a broader research project titled "The impact of violence, child maternal care and social support on infant growth", a cohort study. The primary objective of this project consisted in analyzing social determinants of infant growth at newborns' first year of life assisted in Basic Health Units (BHU) in the municipality of Rio de Janeiro.
The present study is sectional, with a sample of 544 women that attended four Basic Health Units in the municipality of Rio de Janeiro between 2005 and 2009. Data collection was performed through interviews, using a pre-tested questionnaire and applied by previously qualified researchers.
The theoretical-conceptual framework (Figure 1) aims to screen potential confounding factors (adjustment variables). The framework was built based on a literature review about the central subject of this study-the relation of IPV during gestation to GWG.
The main interest exposition is the IPPV from the last 12 months to the interview date. For measuring the exposure, the Portuguese version of CTS-1 tool (Conflict Tactics Scales-Form R) was adapted for usage in Brazil.
18 The collection of these data occurred in the second month of life of the newborn. The present study only used the subscale of physical violence, which is divided into minor and severe physical violence. It was considered positive for this kind of violence when women affirmatively answered at least one question in each of the subscales of interest. It was considered as IPPV the acts performed by partners against women (pregnant women/mother) and the reciprocal.
The outcome consisted of GWG, calculated using the difference between the last weight record of the pregnancy (concerning the last prenatal consultation) and the self-declared pre-gestational weight. Women's weight at the last prenatal consultation was extracted from the pregnant women's booklets. For the classification of GWG, we used recommendations from the Institute of Medicine (IOM) (2009),
19 classifying it as adequate, insufficient and excessive. It is worth mentioning that Brazilian guidelines for the assessment of GWG combine two assessment methods: Atalah's curve and IOM guidelines.
20 However, since most national and international studies used IOM guidelines forthe estimation and classification of GWG, we opted for this method since it enables a higher comparability of the findings of this study.
From the distal dimension to the outcome of interest, there are socioeconomic, demographic and reproductive history characteristics (Figure 1), which were assessed through the variables "environmental dwelling conditions","age and maternal schooling" and "number of children". Environmental dwelling conditions were measured utilizing a system of scores containing the following variables related to residence: agglomeration (number of people per room living in residence), house building material, type of internal sanitation, water supply and type of garbage collector. Residences were classified as presenting inadequate environmental conditions (score: 0-6 points) or adequate (score: ≥7 points) categorization adapted from Reichenheim and Harpham.
21 Maternal age was calculated by difference between the date of questionnaire application and birth date divided by 365.25, being posteriorly categorized in age under 20 years, 20-34 year and 35 years or older. Maternal schooling was measured by the grade in which women attended at the moment of the interview and was categorized into incomplete elementary (<for years of schooling) and complete elementary (≥4 years of schooling. The number of children alive was assessed by each woman's total number of live births until the interview date. This variable was used categorically: primiparous (one child), multiparous (two to four children) and great multiparous (over five children).
This model also shows potential intervening variables of this relation, such as women's mental health, food consumption and physical activity-which due to the selected analytical model for data analysis, were not estimated in this study.
Pre-gestational nutritional status and prenatal follow-up were used for the evaluation of the profiles of interviewees. The first was assessed utilizing the pre-gestational Body Mass Index (BMI), categorized according to cutoff points for adult individuals as proposed by the World Health Organization (WHO).
22 Pre-gestational BMI was calculated by dividing self-referred pre-gestational weight by height squared. Qualified anthropometrists assessed height and in a standardized manner while performing the neonatal health prick or at the first vaccine of the neonate. In order to obtain information related to prenatal follow-up, the interviewee answered the question: "Did you have any follow-up by a physician or nurse during this pregnancy?", with option of answers: "yes" or "no".
Initially, absolute and relative frequencies were determined for all study variables and their respective 95% confidence intervals (CI). In sequence, multinomial simple and multivariate logistic regressions were conducted to analyze the relation of IPPV to inadequate GWG, the analysis guided by the theoretical-conceptual framework (Figure 1). Multivariate models were adjusted by the aforementioned variables ("environmental dwelling conditions", "age and maternal schooling" and "number of alive children"). All analyses were performed with Stata 15.0 software.
The present study was approved by the Research Ethics Committee of the Social Medicine Institute of the Federal University of Rio de Janeiro (UERJ-Portuguese acronym). All participants signed the Free and Informed Consent Form and received information on the institutions that support families that are victims of violence.
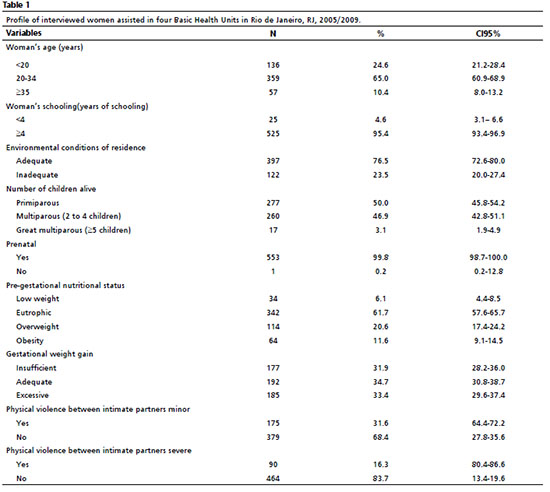
ResultsTable 1 shows the study population's profile. Most interviewees had an age between 20 and 34 years (65%), complete elementary school or more (95.4%) and lived in adequate housing conditions (76.5%). In relation to the assessment of pre-gestational nutritional status, 6.0% presented low weight, 20.6% overweight, and 11.6% were obesity. Half of the women interviewed were primiparous, and almost all of them performed prenatal follow-up. In relation to GWG, around 65% of women presented weight gain incompatible with IOM (2009) guidelines, and 31.9% had insufficient weight gain and 33.4% excessive weight gain. Concerning IPV, 32.7% of intimate partners performed physical violence to solve conflicts, 31.6% reported having experienced minor physical violence events, and 16.3% severe physical violence events.
After adjusting for the multinomial multivariate logistic regression model (Table 2), we observed that minor IPPV increased 1.62 (CI95%=1.02-2.38) times the chance of insufficient GWG, compared to couples that did not experience this kind of violence. Severe IPPV did not show a significant relationship with insufficient weight gain or excessive weight gain.
Discussion The results of this survey show that the experience of IPPV increased the chance of insufficient GWG compared to those women that did not experience this kind of violence in their relationships. We highlight that this association was also identified in studies conducted with women from other nationalities. Both national studies, conceived by Moraes
et al.
14 and Nunes
et al.,
15 and those conducted by Kott
13, in the United States and by Garg
et al.
17 in India. Such studies found the association of IPPV with GWG, demonstrating that IPPV effect on fetus development seems to be independent of factors related to the culture or socioeconomic levels of a given country.
Moraes
et al.
14 highlighted some possible aspects that may be related to lower weight gain in women that were victims of IPPV during pregnancy: lack of interest in buying and preparing food, irregular consumption, lack of appetite due to increase of stress initiated by the abuses suffered or the abuse itself. These biological and behavioral conditions, among others, are mentioned in the literature as related to associations of IPPV with inadequate GWG, and it might be a theoretical path for understanding this relationship. Studies in other life stages suggest that stress motivated by the conflicting environment may lead to hormonal, physiological and behavioral alterations, affecting appetite and/or nutritional standards and promoting inadequate weight gain.
3,23 According to Yount
et al.,
21 an important manner to comprehend the relationship between violence, food consumption and nutritional status would be via the biological system of response to stress. The recurrent exposure to familiar violence may alter the functioning of this system, mainly due to the hyperactivation of hypothalamic-pituitary-adrenal axis, which increases the levels of energy-saving hormones, mainly cortisol. The increase in cortisol is associated with increased visceral fat tissue and, consequently, weight excess.
In other cases, aggressive partners may use food as an instrument of manipulation and control of their companions, thus impairing their access to balanced nutrition.
4,24 Chilton and Booth,
24 in a quanti-qualitative study with 44 families headed by women living in the United States, observed that the perpetrator of violence used food in exchange for maintaining women in the abusive relationship. Another possible explanation for the relation between IPPV and inadequate GWG is that, generally, families in violence have higher difficulty managing their financial resources and are less capable of organizing the purchase of food at home.
25 Nunes
et al.
15 demonstrated that women who suffered IPV during pregnancy had lower income and were financially dependent on their partners, being more vulnerable to violence and the purchase or not of food by their abusive partners.
The literature also evidences that women exposed to IPV are more prone to show depressive behavior, suicidal ideation, anxiety and high levels of stress.
26,27 In some moments, this situation may provoke problems such as the abusive use of alcohol, tobacco and other illicit drugs
8,14 and, subsequently, the exaggerated use of these substances may lead to lower food ingestion and non-healthy lifestyles. According to Ribeiro-Silva
et al. ,
25 mental health problems and alcohol and drug abuse may impair the maintenance and obtaining of a job, affecting family income and, consequently, food consumption outgoings.
In this study, severe IPPV did not show association with insufficient GWG, nor with excessive GWG. This can be related to the small proportion of women victims of this type of violence who had excessive GWG. Further studies with larger samples and, consequently, higher statistical significance are needed for a better understanding of this relationship since there are few national and international studies on this subject.
The present study should be analyzed according to its limitations and strong points. Among the limitations of the studies is the assessment of women that search for the health service since the literature mentions that women who are victims of IPPV, mainly severe violence, have a lower chance of attending adequate prenatal care for its late onset ora low number of consultations, or even both.
5 At the same time, the study used information on pre-gestational weight as declared by participants, which can be listed as another limitation of the study due to the risk of underestimation of the actual measure and, consequently, of categorization of women's nutritional status in an inadequate manner. Nonetheless, studies about the subject show that the weight reported by women is close to the assessed values.
28As a strong point of this study, we highlight the use of a tool transculturally adapted and validated for the assessment of exposition. The CTS-1 was translated and used by other authors in epidemiological surveys in Brazil with a low refusal rate; good reliability, mainly for the physical violence scales.
18 Another point that deserves emphasis is the subject investigated in this study, the relationship between IPV and GWG, since only seven national and international surveys focused on this subject.
The results of this survey indicate the need for care and practical approach to assist pregnant women during prenatal consultations, a proper moment for identifying nutritional disturbances and screening for domestic violence. It is important to mention that the literature shows that the occurrence of IPV may onset or increase its frequency during the gestational period.
29 Women who experience IPV during the gestational period demand special care from health services since pregnancy is a moment of high physical and emotional fragility.
30 IPV during pregnancy and postpartum period lead to severe consequences on the health of both woman and child, such as postpartum depression, urinary tract infection, insufficient gestational weight gain, surgical delivery, vaginal bleeding, inadequate prenatal care, gestational diabetes, fetal and maternal mortality, preterm birth, low birth weight, intrauterine growth restriction, early weaning, infant malnutrition, immunization failures and impairments in children follow-up in health services.
14,15 In this sense, it is essential that health professionals assisting these women are aware and sensitive to identifying potential IPV cases during prenatal consultations, by virtue of its magnitude and deleterious effect on mother and child health.
The present study's findings may help the elaboration and implementation of more effective actions for the promotion and prevention of IPV and inadequate GWG, decreasing, thus, health risks for both mother and baby. We also reinforce the role of managers and decision-makers in the health area for the inclusion of violence between intimate partners in policies that involve assistance and follow-up of pregnant women so that women themselves can be aware of this problem, enabling the identification, notification and/or denounces in the existing mechanisms. In front of the scarcity of studies about violence between intimate partners during pregnancy and gestational weight gain, we also highlight the need for more studies regarding this relationship in different socioeconomic and cultural contexts of longitudinal design and that include analyses that are more robust in order to better comprehend this relationship.
References1. Chagas DCd. Ganho de peso gestacional e sua influência retenção de peso pós-parto e índice de massa corporal infantil: contribuição das coortes de nascimento Brisa e Geração XXI [Tese]. São Luís, MA: Universidade Federal do Maranhão; 2016.
2. Silva LOd, Alexandre MR, Cavalcante ACM, Arruda SPM, Sampaio RMM. Adequate versus inadequate weight gain and socioeconomic factors of pregnant women followed up in primary care. Rev Bras Saúde Matern Infant. 2019; 19 (1): 99-106.
3. Leite T, Port ACR. Fatores associados ao ganho ponderal de gestantes atendidas na Unidade básica de saúde da mulher "Maria de Lourdes Campos Silva" em Monte Azul Paulista-SP. Rev Ciênc Nutr Online. 2018; 2 (2): 26-31.
4. Alhusen JL, Geller R, Dreisbach C, Constantoulakis L, Siega-Riz AM. Intimate Partner Violence and Gestational Weight Gain in a Population-Based Sample of Perinatal Women. JOGNN. 2017; 46 (3): 390-402.
5. Alhusen JL, Ray E, Sharps P, Bullock L. Intimate partner violence during pregnancy: maternal and neonatal outcomes. J Women's Health. (2002). 2015 Jan; 24 (1): 100-6.
6. Athar U, Daud NUA, Khan WA, Khalid A, Gill SI. Caught Between External Pressures and Internal Battles: Psychosocial Factors Affecting Gestational Weight Gain-A Scoping Review. Cureus. 2021; 13 (2): e13487-e.
7. Zhou M, Peng X, Yi H, Tang S, You H. Determinants of excessive gestational weight gain: a systematic review and meta-analysis. Arch Public Health. 2022 Mai; 80 (1): 129.
8. Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R. World report on violence and health. Geneva: WHO; 2002. [access in 2020 out 10]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/42495/9241545615_eng.pdf9. Bott S, Guedes A, Ruiz-Celis AP, Mendoza JA. Intimate partner violence in the Americas: a systematic review and reanalysis of national prevalence estimates. Rev Panam Salud Publica. 2019 Mar; 43: e26.
10. Conceição HN, Coelho SF, Madeiro AP. Prevalência e fatores associados à violência por parceiro íntimo na gestação em Caxias, Maranhão, 2019-2020. Epidemiol Serv Saúde. 2021; 30 (2): e2020848.
11. Vaz JDS, Souza M, Valério ID, Silva MTD, Freitas-Vilela AA, Bierhals IO,
et al. Physical intimate partner violence and dietary patterns in pregnancy: a Brazilian cohort. Cien Saúde Colet. 2022; 27 (4): 1317-26.
12. Khodakarami N, Naji H, Dashti MG, Yazdjerdi M. Woman abuse and pregnancy outcome among women in Khoram Abad, Islamic Republic of Iran. East Mediterr Health J. 2009; 15 (3): 622-8.
13. Kott A. Intimate Partner Violence And Pregnancy Weight Gain Weakly Associated. Perspect Sex Reprod Health. 2011; 43 (3): 209-10.
14. Moraes CL, Amorim AR, Reichenheim ME. Gestational weight gain differentials in the presence of intimate partner violence. Int J Gynaecol Obstet. 2006 Dec; 95 (3): 254-60.
15. Nunes MA, Camey S, Ferri CP, Manzolli P, Manenti CN, Schmidt MI. Violence during pregnancy and newborn outcomes: a cohort study in a disadvantaged population in Brazil. Eur J Public Health. 2011 Feb; 21 (1): 92-7.
16. Dolatian M, Sharifi N, Mahmoodi Z, Fathnezhad-kazemi A, Bahrami-vazir E, Rashidian T. Weight gain during pregnancy and its associated factors: a path analysis. Nurs Open. 2020;7 (5): 1568-77.
17. Garg S, Rustagi R, Singh MM, Engtipi K. Effect of Intimate Partner Violence on Maternal and Birth Outcomes of Pregnancy among Antenatal Clinic Attendees in Delhi: A Prospective Observational Study. Indian J Community Med. 2020;45 (4): 501-5.
18. Hasselmann MH, Reichenheim ME. Adaptação transcultural da versão em português da Conflict Tactics Scales Form R (CTS-1), usada para aferir violência no casal: equivalências semântica e de mensuração. Cad Saúde Pública. 2003; 19 (4): 1083-93.
19. Institute of Medicine (IOM). Weight Gain During Pregnancy: Reexamining the Guidelines: Committee to Reexamine IOM Pregnancy Weight Guidelines; National Research Council; 2009.
20. Amorim AR, Lacerda EMA, Kac G. Uso e interpretação dos indicadores antropométricos na avaliação do estado nutricional de gestantes. In: Kac G, Sichieri R, Gigante DP, editors. Epidemiologia nutricional Rio de Janeiro: Editora FIOCRUZ/Atheneu; 2007. p. 30-47.
21. Reichenheim ME, Harpham T. Perfil intracomunitário da deficiência nutricional: estudo de crianças abaixo de 5 anos numa comunidade de baixa renda do Rio de Janeiro (Brasil). Rev Saúde Pública. 1990; 24 (1): 69-79.
22. World Health Organization (WHO
). Physical status: the use and interpretation of anthropometry-report of a WHO expert committee. Geneva: WHO; 1995. [access in 2020 out 10]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/37003/WHO_TRS_854.pdf?sequence=1&isAllowed=y23. Yount KM, DiGirolamo AM, Ramakrishnan U. Impacts of domestic violence on child growth and nutrition: a conceptual review of the pathways of influence. Social Sci Med. 2011 May; 72 (9): 1534-54.
24. Chilton M, Booth S. Hunger of the body and hunger of the mind: African American women's perceptions of food insecurity, health and violence. J Nutr Educ Behav. 2007; 39 (3): 116-25.
25. Ribeiro-Silva RC, Fiaccone RL, Barreto ML, Santana ML, Santos SM, Conceição-Machado ME,
et al. The association between intimate partner domestic violence and the food security status of poor families in Brazil. Public Health Nutr. 2016 May; 19 (7): 1305-11.
26. Altarac M, Strobino D. Abuse during pregnancy and stress because of abuse during pregnancy and birthweight. J Am Med Women's Assoc. 2002; 57 (4): 208-14.
27. Rachana C, Suraiya K, Hisham AS, Abdulaziz AM, Hai A. Prevalence and complications of physical violence during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2002 Jun; 103 (1): 26-9.
28. Oliveira AFd, Gadelha AMJ, Leal MC, Szwarcwald CL. Estudo da validação das informações de peso e estatura em gestantes atendidas em maternidades municipais no Rio de Janeiro, Brasil. Cad Saúde Pública. 2004; 20 (Supl. 1): S92-100.
29. Han A, Stewart DE. Maternal and fetal outcomes of intimate partner violence associated with pregnancy in the Latin American and Caribbean region. Int J Gynaecol Obstet. 2014 Jan; 124 (1): 6-11.
30. Moraes CL, Arana FDN, Reichenheim ME. Violência física entre parceiros íntimos na gestação como fator de risco para a má qualidade do pré-natal. Rev Saúde Pública. 2010; 44: 667-76.
Received on January 12, 2021
Final version presented on May 24, 2022
Approved on June 28, 2022
Associated Editor: Aurélio Costa
Authors' contribution: Hasselmann MH and Flor RB contributed with conceptualization and design of the article.
Flor RB, Marques ES and Hasselmann MH contributed with analysis and interpretation of data and writing of the manuscript.
Oliveira ASD contributed with interpretation of data and writing of the manuscript. All authors approved the final version and are responsible for all aspects of the study, including the assurance of its precision and integrity. The authors declare no conflict of interest.


 ; Emanuele Souza Marques2
; Emanuele Souza Marques2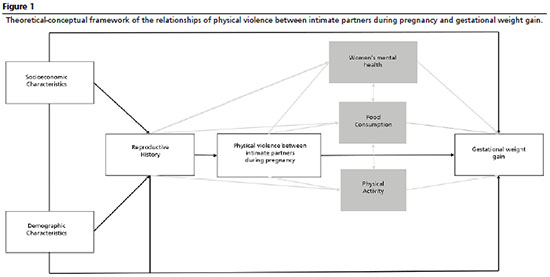







 Ler em português
Ler em português