Eclampsia remains one of the most feared emergencies in obstetrics. Although the use of magnesium sulfate (MgSO
2) to treat eclamptic crises has been described since the early 20th century,
1 it was the standardizations by Pritchard in the 1950s and by Zuspan in the 1960s who systematized reproducible therapeutic regimens for attack and maintenance.
2,3Clinical evidence was definitively consolidated in 1995 with publication of the Eclampsia Trial, demonstrating the superiority of MgSO
2 over diazepam and phenytoin in preventing recurrence and reducing severe outcomes.
4 Subsequently, three Cochrane reviews reinforced the effectiveness and safety of magnesium in eclampsia, establishing it as the standard of care.
5-7Even so, failures persist: delays in administration, incorrect doses lack of monitoring, and even non-recognition of indications. A recent review of maternal deaths in South Africa showed that, even among women with obvious indications, MgSO
2 was not administered in part of the cases and, in others, was used incorrectly, with attack dose or inadequate maintenance. These failures,combined with delays and lack of clinical vigilance—resulted in preventable deaths and underscore the gap between consolidated evidence and everyday practice.
8It is in this scenario that the mnemonic
ABCDEFG is proposed in 2011 by Amorim & Katz and refined in national and international courses. Inspired by Advanced Trauma Life Support (ATLS) logic,
9 it organizes the primary assessment quickly and repetitively, but adapted to the physiology and ethics of the maternal–fetal dyad: stabilize the mother first (A–E), and only then assess the fetus and pregnancy (F–G). The strength of the acronym lies not in the letters themselves, but in what they make possible at the bedside: reducing noise, ordering priorities, distributing roles, and preventing the essentials from being forgotten in high-stress contexts.
9The ABCDEFG, step by step (Table 1):
A — Assistance/Airway. Call the multidisciplinary team, assign roles, and protect the airway. Place the patient in the lateral decubitus position, suction secretions, use an oropharyngeal airway when indicated, and observe criteria for an advanced airway.
B — Breathing. Monitor respiratory rate (RR) and peripheral oxygen saturation (SpO
2) from admission. Offer titrated oxygen via non-rebreather mask with a target of ≥95%, and escalate ventilatory support if necessary.
C — Circulation. Ensure two large-bore venous accesses, careful hydration, and monitoring of perfusion. Insert a urinary catheter and aim for urine output ≥0.5 mL/kg/h, avoiding fluid overload.
D — Disability/"Damage" (neurologic). Core management: intravenous magnesium sulfate (IV) attack and maintenance, monitoring of reflexes, respiration, diuresis and antidote at the bedside. Re-dose if seizures recur; escalate to hydantoin and advanced airway if refractory.
E — Hypertensive Emergency/Examinations. Immediately treat systolic blood pressure (SBP) ≥160 mmHg and/or diastolic blood pressure (DBP) ≥110 mmHg. Target: 15–25% reduction and maintenance between SBP 130–150 and DBP 80–100 mmHg. In Brazil: immediate-release oral (PO) nifedipine and IV hydralazine. Request priority tests without delaying therapy.
10F — Fetus. Fetal assessment only after maternal stabilization. Post-seizure changes are usually transient; fetal bradycardia lasting >10–15 minutes suggests premature detachment of a normally inserted placenta (PDNIP) and requires immediate obstetric decision-making.
11G — Gestation. Interruption is mandatory, but not immediate or untimely. Whenever possible, wait at least one hour after the last seizure and avoid removing the fetus at the peak of acidosis. Vaginal delivery is preferable when feasible;
12 cesarean section for persistent fetal distress, PPHN, severe hemorrhage, or unfeasibility of induction.
A safety culture that underpins the acronymABCDEFG only works when integrated with safety practices: closed-loop communication, with explicit orders and mandatory confirmation; in situ simulation, to transform protocol into automatic behavior; and continuous audit, with indicators such as magnesium door time, pressure control door time, and the rate of cesarean sections motivated by transient tracings.
Publication and commitmentIn this issue, RBSMI publishes a special article
13 detailing the ABCDEFG mnemonic, with flows, algorithms, and operational tables. This editorial presents its architecture and clinical significance. The challenge is not to invent something new, but to turn established evidence into reliable and universal routines. What we propose is simple and demanding: adopt a common language for eclampsia, capable of reducing variability in care and shortening critical times. ABCDEFG is not an end, but a beginning—an invitation to clinical discipline, clear communication, and life-saving implementation.
References1. Sibai BM. Diagnosis, prevention, and management of eclampsia. Obstet Gynecol. 2005; 105 (2): 402–10.
2. Pritchard JA. The use of the magnesium ion in the management of eclamptogenic toxemias. Surg Gynecol Obstet. 1955; 100 (2): 131-40.
3. Zuspan FP. Treatment of severe preeclampsia and eclampsia. Clin Obstet Gynecol. 1966; 9: 954-72.
4. The Eclampsia Trial Collaborative Group. Which anticonvulsant for women with eclampsia? Evidence from the Collaborative Eclampsia Trial. Lancet. 1995; 345 (8963): 1455-63.
5. Duley L, Henderson Smart DJ. Magnesium sulphate versus diazepam for eclampsia. Cochrane Database Syst Rev. 2010; (12): CD000127.
6. Duley L, Henderson Smart DJ. Magnesium sulphate versus phenytoin for eclampsia. Cochrane Database Syst Rev. 2010; (10): CD000128.
7. Duley L, Gülmezoglu AM, Chou D. Magnesium sulphate versus lytic cocktail for eclampsia. Cochrane Database Syst Rev. 2010; (9): CD002960.
8. Khan ZL, Balie GM, Chauke L. Hypertensive Disorders of Pregnancy Deaths: A Four Year Review at a Tertiary/Quaternary Academic Hospital. Int J Environ Res Public Health. 2025; 22 (7): 978.
9. American College of Surgeons (ACS). Committee on Trauma. Advanced Trauma Life Support (ATLS
®) Student Course Manual. 11
th ed. Chicago (IL): ACS; 2025.
10. ACOG Committee Opinion No. 767. Emergent therapy for acute onset, severe hypertension during pregnancy and the postpartum period. Obstet Gynecol. 2019; 133 (2): e174–80.
11. Ambia AM, Wells CE, Yule CS, McIntire DD, Cunningham FG. Fetal heart rate tracings associated with eclamptic seizures. Am J Obstet Gynecol. 2022; 227 (4): 622.e1–622.e6.
12. Seal SL, Ghosh D, Kamilya G, Mukherji J, Hazra A, Garain P. Does route of delivery affect maternal and perinatal outcome in women with eclampsia? A randomized controlled pilot study. Am J Obstet Gynecol. 2012 Jun; 206 (6): 484.e1–484.e7.
13. Amorim MMR, Albuquerque MA, Brito JC, Carneiro ACMC, Katz L. O ABCDEFG da Eclâmpsia (Suporte Avançado de Vida na Eclâmpsia). Rev Bras Saúde Mater Infant. 2025. [artigo especial;
Epub ahead of print].
An invitation from the Editor in Chief: Lygia Vanderlei


 ; Alex Sandro Rolland Souza2,3,4
; Alex Sandro Rolland Souza2,3,4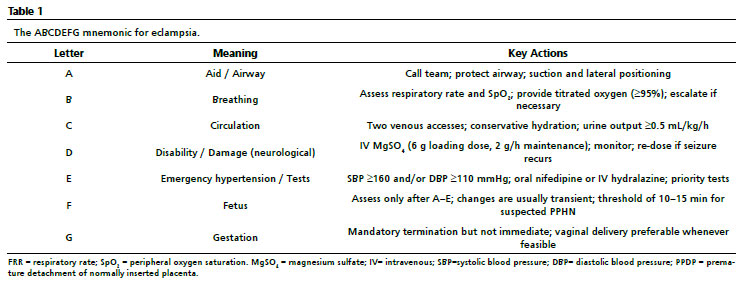






 Ler em português
Ler em português