ABSTRACT
OBJECTIVES: to assess the oral health profile and knowledge related to dental treatment during pregnancy, as well as variables associated with dental caries in pregnant women in the countryside of Sergipe (Lagarto).
METHODS: a cross-sectional study was conducted in the Primary Health Care with 128 women undergoing prenatal care. Participants answered a questionnaire and underwent clinical evaluation to record the decayed, missing, and filled teeth index (DMFT). Descriptive statistics were applied, and a multiple linear regression model was constructed.
RESULTS: the participants' mean age was 25.1 years (± 6.82), and the mean DMFT index was 6.5 (± 5.4). Increasing age (p < 0.01) and low educational level predicted higher DMFT, with increases of 3.84 points for women with incomplete elementary schooling (p = 0.012) and 6.01 points for those with completed elementary schooling (p<0.01), compared with participants with higher education. Lack of knowledge about the possibility of pregnant women visiting the dentist was associated with a 12.26-point increase in DMFT (p<0.01), while each additional daily toothbrushing was associated with a 1.59-point reduction in DMFT (p=0.007).
CONCLUSIONS: older age, lower educational schooling, and lack of knowledge about dental care during pregnancy were predictors of higher DMFT, whereas more frequent daily toothbrushing acted as a protective factor.
Keywords:
Pregnancy, Oral health, Prenatal care, Dental caries, DMF index
RESUMO
OBJETIVOS: avaliar o perfil de saúde bucal e de conhecimentos relacionados ao tratamento odontológico na gestação, além de variáveis relacionadas à ocorrência de cárie em gestantes no interior de Sergipe (Lagarto).
MÉTODOS: estudo transversal, realizado na Atenção Básica com 128 mulheres em acompanhamento pré-natal. As participantes responderam a um questionário e foram submetidas à avaliação clínica para registro do índice de dentes cariados, perdidos e obturados (CPO-D). Foi realizada estatística descritiva e construído um modelo de regressão linear múltipla.
RESULTADOS: a idade média das participantes foi de 25,1 anos (± 6,82) e o CPO-D médio foi de 6,5 (±5,4). Aumento da idade (p<0,01) e baixa escolaridade foram preditores de maior CPO-D, com acréscimo de 3,84 pontos para mulheres com ensino fundamental incompleto (p=0,012) e de 6,01 pontos para aquelas com ensino fundamental completo (p<0,01), em comparação às participantes com ensino superior. O desconhecimento sobre a possibilidade de gestantes irem ao dentista associou-se a um aumento de 12,26 pontos no CPO-D (p<0,01) e cada escovação adicional diária esteve associada a redução de 1,59 pontos no CPO-D (p= 0,007).
CONCLUSÕES: idade avançada, baixa escolaridade e desconhecer a possibilidade de gestantes frequentarem o dentista foram preditores de maior CPO-D, enquanto maior frequência de escovação diária foi um fator protetor.
Palavras-chave:
Gravidez, Saúde bucal, Cuidado pré-natal, Cárie dentária, Índice CPO
IntroductionPregnancy is a period in a woman's life that inspires care for general and oral health.
1 During this period, a series of physiological changes occur in the female body that impact the oral cavity, causing greater vulnerability to oral diseases, especially caries and periodontal disease.
2Due to gastrointestinal and hormonal changes, it is relatively common for pregnant women to report episodes of nausea, heartburn, and vomiting.
3 In addition, behavioral and taste changes are expected, with a greater preference for sweet flavors.
4 These factors contribute to an increase in the frequency of cariogenic snacks, which, combined with poor oral hygiene, increasing the risk of developing dental caries.
5 In fact, the prevalence of dental caries in pregnant women has been reported in being high.
6However, these habits can also influence the child's oral health. The literature reports that mothers are the main transmitters of good habits to their children,
7 habits that tend to be established for life and are extremely important to ensure good oral and general health development.
8 Furthermore, the level of pregnant women's knowledge on oral health appears to be related to their own oral health status and of their babies.
9In Brazil, we have the
Sistema Único de Saúde (SUS) (Public Health System), which provides universal and comprehensive access to health services, a right of all Brazilians, from pregnancy and throughout life, aiming at prevention, recovery, and health promotion.
10 Within SUS, there is prenatal dental care, which aims to guide pregnant women on the care necessary to maintain good oral health, both during pregnancy and in early childhood for their babies.
11However, there are still many doubts about oral health care during pregnancy,
12 and pregnant women's lack of knowledge about the increased likelihood of developing oral diseases during pregnancy and the consequences of these for maternal and child health represents a major barrier in using dental services during pregnancy. In addition, fear and anxiety associated with some popular beliefs about oral problems and dental treatment during pregnancy have hindered the access for decades.
13Conducting a study on the factors that impact the number of caries experiences in pregnant women in a city in the countryside of Sergipe, the smallest State in Brazil, is essential due to the unique challenges faced by regions with fewer economic resources and limited access to health services.
This study aimed to assess the oral health profile and knowledge related to dental treatment during pregnancy, in addition to variables related to the occurrence of caries in pregnant women in the city of Lagarto/SE.
MethodsThis is a cross-sectional observational study with a quantitative and analytical approach. The city of Lagarto is located in the South-Central region of the State, considering part of the
Agreste Sergipano (Rugged area in Sergipe). It has 101,579 inhabitants, with approximately 52% of this population being women, according to the
Censo Demográfico do Instituto Brasileiro de Geografia e Estatística (IBGE) (Demographic Census of the Brazilian Institute of Geography and Statistics) released in 2022. The
Atenção Primária à Saúde (APS) (Primary Health Care) of the
Sistema Único de Saúde (SUS) (Public Health System) in the city of Lagarto has 15 Basic Health Units (UBS) and 12 health centers to provide care to the urban and rural population.
For this study, three UBS in the urban area were selected, which provide care to a large number of registered users and serve as an internship field for health students at the
Universidade Federal de Sergipe (Federal University of Sergipe). All pregnant women who were receiving prenatal care at the UBS in the city of Lagarto participated in the study, with no restrictions on the stage of pregnancy, and puerperals (up to one month after childbirth) were also included. Those who did not respond or withdrew from participating during the interview were excluded.
Data collection took place from October 2019 to May 2021 and was carried out by previously trained researchers. A questionnaire was used to collect information from the research participants, administered by two different professionals in the form of interviews in the waiting rooms for regular prenatal consultations at the aforementioned UBS. This was developed by the authors for this research, based on previous studies.
14,15 The instrument contained questions about sociodemographic data and the current pregnancy, presence of complaints and self-perception of oral health during pregnancy, oral hygiene and dietary habits, last visit to the dentist, and knowledge about changes in the oral cavity and dental care during pregnancy. After applying the questionnaires, at the end the pregnant women were offered guidance and clarification of doubts about the topics covered in the interview.
Following the questionnaire, the pregnant women's caries experience was assessed individually through clinical dental examination and recording of the decayed, missing, and filled teeth (DMFT) index. The examinations were performed in a private area in the UBS waiting room with the aid of natural light and wooden spatulas. All universal biosafety standards and criteria recommended by the World Health Organization in 1997 for epidemiological surveys of oral health were followed. Finally, oral hygiene instructions were given to the pregnant women, and oral hygiene kits containing toothbrushes and fluoride toothpaste were provided.
All data collected were analyzed using the statistical program Jamovi version 2.3.28. Descriptive data analysis was performed for the sociodemographic and clinical characterization of the study population, as well as to compare the caries experience of pregnant women with their knowledge of maternal and child oral health. This analysis included measures of central tendency (frequencies, mean, median, minimum, and maximum) and measures of dispersion (standard deviation, interquartile range). To analyze the factors (independent variables) that predict or protect the DMFT index, a multiple linear regression was conducted using the Forward technique. All assumptions for performing a linear regression were respected. Initially, a univariate analysis was performed, and variables with a
p-value of up to 0.20 were selected for multivariate analysis. A significance level of 5% was considered.
This study was submitted for evaluation by the Ethics Committee on Research Involving Human Subjects of the
Universidade Federal de Sergipe (CEP) and (CAAE: 90518218.2.0000.5546; opinions Nº. 3,226,292 (03/27/2019) and 3,759,212, 12/11/2019) were approved.
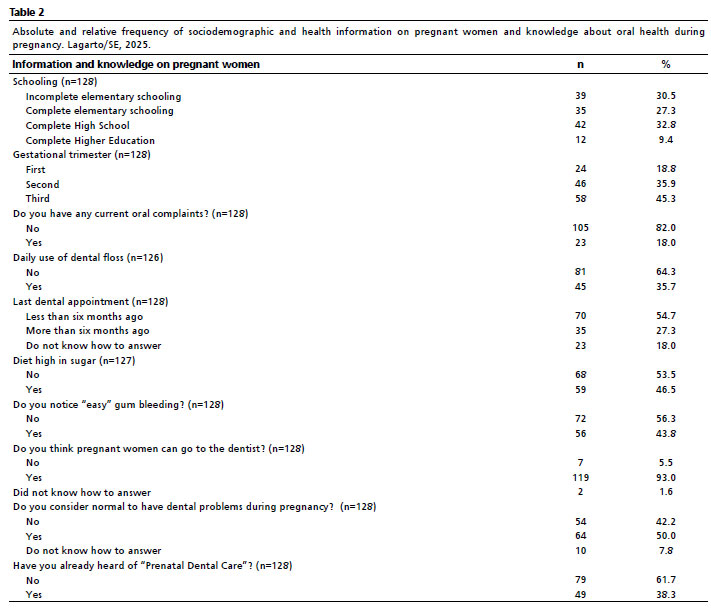
ResultsA total of 128 women with a mean age of 25.1 ± 6.82 years participated in the study. The mean DMFT index was 6.5 (±5.4). Table 1 details the DMFT according to the participants' age group and presents the absolute and relative number of women free of caries. Only nine women (7.03%) were free of caries. Most participants had completed high school and were in their third trimester of pregnancy. Regarding oral health information, most had no oral health complaints at the time of the interview, reported not flossing daily, had no gum bleeding, had their last dental appointment in the last six months, reported not consuming diets rich in sugary food, and were unaware of the term "prenatal dental care". The average daily toothbrushing was 2.83 ± 0.66. Table 2 shows the complete distribution of these variables.
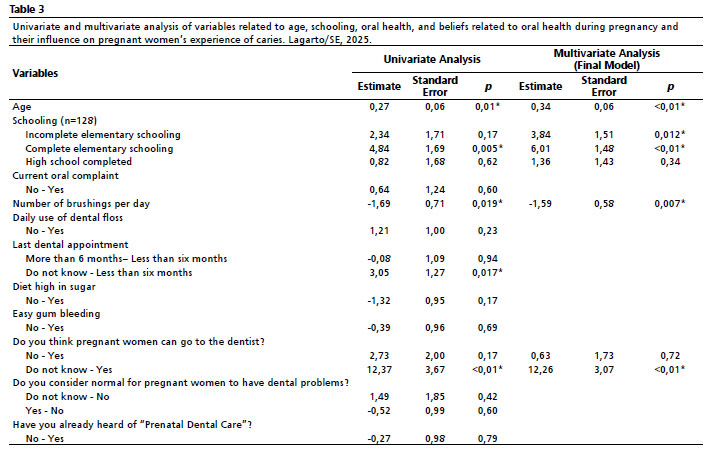
The final multiple linear regression model had an R
2 of 0.406 (
p<0.001). The results showed no multicollinearity and presented normality of the residuals. The Durbin Watson statistic was 1.60 (
p=0.022); the VIF (Variance Inflation Factor) ranged from 1.02 to 1.05; there was normality of the residuals according to the Shapiro-Wilk test of 0.988 (
p=0.326). The estimates of the final model, standard error, and
p-value are presented in Table 3.
In the multivariate analysis, increased age (
p<0.01) and low schooling level were predictors of a higher DMFT index, with an increase of 3.84 points for women with incomplete elementary schooling (
p=0.012) and 6.01 points for those with complete elementary schooling (
p<0.01), compared to the participants with higher education. Lack of knowledge about the possibility of pregnant women going to the dentist was strongly associated with an increase of 12.37 points in the DMFT index (
p<0.01), and not knowing when their last dental appointment was, was associated with an increase of 3.05 points in the DMFT index (
p<0.05). In addition, each additional brushing per day was associated with a reduction of 1.69 points in the DMFT (
p<0.05).
DiscussionThis study evaluated the knowledge of pregnant women who received prenatal care in SUS in the countryside of Sergipe and factors related to caries experience. Advanced age, low schooling level, and lack of knowledge about the possibility of pregnant women visiting the dentist were predictors of higher DMFT, while higher frequency of daily toothbrushing was a protective factor. Furthermore, the average DMFT was 5 among women aged 15 to 19 and 12.62 among those aged 35 to 44, ranging from 0 to 28, with 7.03% caries-free in the total sample.
Caries experience is commonly assessed by the DMFT index. The most recent national epidemiological survey
16 revealed an average DMFT of 3.41 and 10.70 for the above-mentioned age groups, respectively. Furthermore, the percentage of caries-free individuals in these groups was 33.8% and 5.20%, respectively. However, it is known that pregnant women are more susceptible to oral diseases than non-pregnant women.
2-6,17 Geevarghese
et al.,
17 when evaluating 150 pregnant and 150 non-pregnant women in India, observed worse DMFT scores for pregnant women, ranging from zero to 13 on this index.
17 In fact, the total mean of DMFT of our sample (6.5) was very similar to that found by Mariotti
et al.
18 (6.65), who evaluated 144 puerperals of a similar age group in Minas Gerais State.
Although most participants had completed high school, more than 30% had not completed elementary school. According to the
Pesquisa Nacional por Amostra de Domicílios Contínua (PNAD)(Continuous National Household Sample Survey), although the proportion of people over 25 who have completed high school has grown in recent years, more than half have not completed it, mainly due to the need to work, lack of interest, pregnancy, and domestic chores.
19 Unfortunately, perverse issues of gender inequality involving pregnancy and domestic chores as factors related to dropping out of school are still observed in the country. In this context, we observed that low educational attainment was associated with a higher experience of caries in the studied population. In agreement, Jain
et al.
20 observed low educational attainment as a negative predictor of the prevalence of myths about oral health among pregnant women, while Barbieri
et al.
14 reported that pregnant women with eight or more years of schooling had greater adequate knowledge on oral health, thus being a protective factor for the development of caries.
The data on oral health raise intriguing questions: while most pregnant women do not report oral complaints, their oral hygiene habits reveal the need for special care at this stage of life. SUS, through the
Estratégia de Saúde da Família (ESF) (Family Health Strategy), presents guidelines that recommend guidance and care for priority groups, including pregnant women.
21 Thus, the
Equipe de Saúde Bucal (eSB) (Oral Health Team) has the role of ensuring dental care during prenatal care.
12,22 However, most participants in this study were unfamiliar with the term "
Pré-Natal Odontológico" (Prenatal Dental Care) as observed in other studies.
11Dental care during pregnancy has always been surrounded by challenges to its effective implementation. It is true that clinical guidelines for dental care for pregnant women have evolved over time. While in 2008,
Caderno de Atenção Básica nº17 (Basic Care Notebook No. 17) (an important document guiding oral health in SUS at the time) contained passages that were not very encouraging for dentists regarding the provision of dental care during pregnancy,
22 in 2018, the material was updated with greater encouragement for coordination between teams, guiding the referral of pregnant women for dental consultations at the beginning of prenatal care.
23At the end of 2019, a new model for financing APS in SUS was published.
24 Among the strategic indicators, for the first time in SUS, a specific incentive measure was observed to improve the proportion of pregnant women receiving dental care, since this number has always been historically low in the country. Furthermore, the measure sought to improve the impact on maternal and child health indices, such as the risk of preeclampsia, low birth weight, and premature birth, since the relation between oral health and these negative outcomes in pregnancy is already known.
25-27Further exploring the causal relationship between oral diseases and systemic health, it is known that there is a high load of lipopolysaccharides (LPS) in inflamed periodontium. LPS can reach the placental membranes through the bloodstream and induce the release of pro-inflammatory cytokines such as interleukin 1β, prostaglandin E
2, and tumor necrosis factor α (cytokines toxic to the fetus), resulting in low birth weight and premature birth.
25 Furthermore, the translocation of oral organisms to the uteroplacental unit caused by the progression of periodontal disease can lead to inflammation and damage to the placenta, as well as clinical manifestations of preeclampsia.
28 In addition, it is known that caries is a multifactorial disease related to determine and modify factors, which can be prevented and controlled by changing habits, especially diet and hygiene. However, as already mentioned, physiological and behavioral changes inherent to pregnancy can contribute to its onset and progression.
3-5Although it is safe, especially in the second trimester, dental care during pregnancy still faces resistance due to cultural beliefs about risks to the baby.
29 Similarly, we observed that lack of knowledge about the possibility of dental appointments during pregnancy was associated with higher rates of caries.
The difficulty in implementing effective prenatal dental care in APS may be compounded by records of single and brief consultations. Lack of memory of the last consultation, possibly a long time ago, was also associated with higher caries rates, suggesting barriers to access. Ideal prenatal dental care would include appointments every trimester, with a detailed medical history, a welcoming environment, a complete treatment plan, prophylaxis and hygiene guidance, encouragement of healthy habits, and guidance on oral health in early childhood.
30In the present research, oral health issues such as flossing and number of daily brushings could have been addressed in a prenatal dental consultation and helped protect against caries, since our regression model indicated that each additional brushing per day was significantly associated with a 1.69 reduction in DMFT. It should be noted that including oral health education in prenatal care can contribute to greater knowledge among vulnerable pregnant women and, consequently, greater empowerment, participation in care and decisions, and the adoption of healthy habits, reflecting in improved health for women and their children.
9,15 Thus, it is suggested that further studies evaluating knowledge and literacy in prenatal oral health be conducted.
Among the limitations of the study, it is noteworthy that, as it was a cross-sectional study, it was not possible to verify whether there was a long-term improvement in schooling or maternal and child oral health indices in the city studied. Furthermore, although a high incidence of caries was found among the participants, it was not possible to verify whether these women sought dental treatment afterwards. Another limitation was the difficulty in recruiting participants, since the group of pregnant women generally does not adhere well to health education initiatives and research conducted at the UBS in the city, as observed by our research group, especially during the peak of the COVID-19 pandemic, when it became even more difficult to find pregnant women in waiting rooms and include them in the research.
Finally, it is worth to reinforce the importance of access to prenatal dental care to encourage oral hygiene habits, break myths and taboos, and ensure dental appointments focused on the prevention of oral diseases, promotion of healthy habits, and dental treatment for pregnant women. The results indicate the need for urgent changes in the evaluated scenario and may help to understand the predisposing factors for this disease.
References1. Silva CC, Savian CM, Prevedello BP, Zamberlan C, Dalpian DM, Santos BZ. Acesso e utilização de serviços odontológicos por gestantes: revisão integrativa de literatura. Ciênc sSaúde Colet. 2020 Mar; 25 (3): 827-35.
2. Rocha JS, Arima LY, Werneck RI, Moysés SJ, Baldani MH. Determinants of Dental Care Attendance during Pregnancy: A Systematic Review. Caries Res. 2018; 52 (1-2): 139-52.
3. Hinkle SN, Mumford SL, Grantz KL, Silver RM, Mitchell EM, Sjaarda LA,
et al. Association of Nausea and Vomiting During Pregnancy With Pregnancy Loss: A Secondary Analysis of a Randomized Clinical Trial. JAMA Intern Med. 2016 Nov 1; 176 (11): 1621-7.
4. Jevtić M, Pantelinaci J, Jovanović Ilić T, Petrović V, Grgić O, Blazić L. The role of nutrition in caries prevention and maintenance of oral health during pregnancy. Med Pregl. 2015 Nov-Dec; 68 (11-12): 387-93.
5. Nascimento EP, Andrade FS, Costa AMDD, Terra FS. Gestantes frente ao tratamento odontológico. Rev. Bras. Odontolol. 2012; 69 (1): 125-30.
6. Yunita Sari E, Saddki N, Yusoff A. Association between Perceived Oral Symptoms and Presence of Clinically Diagnosed Oral Diseases in a Sample of Pregnant Women in Malaysia. Int J Environ Res Public Health. 2020 Oct; 17 (19): 7337.
7. Costa GM. Protocolo de Atenção à Saúde Bucal para Gestantes na Equipe da Estratégia de Saúde da Família da "Casa da Comunidade Serrinha" Em Gouveia-MG. [monografia]. Lagoa Santa (MG). Especialização em Atenção Básica em Saúde da Família, Universidade Federal de Minas Gerais, 2014.
8. Abanto J, Oliveira LB, Paiva SM, Guarnizo-Herreño C, Sampaio FC, Bönecker M. Impact of the first thousand days of life on dental caries through the life course: a transdisciplinary approach. Braz Oral Res. 2022 Oct; 36: e113.
9. Barbosa MCF, Rocha NB, Souza Gomes Rodrigues H, Oliveira DSB, Fernandes LA, Lima DC. Maternal Knowledge of Oral Health During Pregnancy and Childbirth. Matern Child Health J. 2023 Sep; 27 (9): 1607-15.
10. Ministério da Saúde (BR). Sistema Único de Saúde - SUS [
Internet]. Brasília (DF): Ministério da Saúde; 2024. [access in 2024 Mai 20]. Available from:
https://www.gov.br/saude/pt-br/sus11. Nascimento RP, Rockenbach VBM. Pré-natal odontológico: percepção das gestantes atendidas no município de Vilhena- RO. Rev Ciência Plural. 2023; 9 (3): 1-18.
12. Sousa LLA, Cagnani A, Barros AMS, Zanin L, Flório FM. Pregnant women's oral health: knowledge, practices and their relationship with periodontal disease. Rev Gaúcha Odontol. 2016 Jun; 64 (2): 154-63.
13. Jackson JT, Quinonez RB, Kerns AK, Chuang A, Eidson RS, Boggess KA,
et al. Implementing a prenatal oral health program through interprofessional collaboration. J Dent Educ. 2015 Mar; 79 (3): 241-8.
14. Barbieri W, Peres SV, Pereira CB, Peres Neto J, Sousa MLR, Cortellazzi KL. Sociodemographic factors associated with pregnant women's level of knowledge about oral health. Einstein (São Paulo). 2018 May 7; 16 (1).
15. Boggess KA, Urlaub DM, Moos MK, Polinkovsky M, El-Khorazaty J, Lorenz C. Knowledge and beliefs regarding oral health among pregnant women. The Journal of the American Dental Association. 2011 Nov; 142 (11): 1275-82.
16. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. Departamento de Estratégias e Políticas de Saúde Comunitária. SB Brasil 2023: Pesquisa Nacional de Saúde Bucal: relatório final. Brasília (DF): Ministério da Saúde; 2025. 1º ed. rev. [access in 2025 Mai 20]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/sb_brasil_2023_relatorio_final_1edrev.pdf17. Geevarghese A, Baskaradoss JK, Sarma PS. Oral Health-Related Quality of Life and Periodontal Status of Pregnant Women. Matern Child Health J. 2017 Aug; 21 (8): 1634-42.
18. Mariotti C, Santos CMML, Bulgareli JV, Paranhos LR, Herval AM. Atenção odontológica durante a gestação e a saúde do recém-nascido: um estudo transversal. Rev Odontol UNESP. 2024; 53: e20240006.
19. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa Nacional por Amostra de Domicílios Contínua (PNAD Contínua): educação: 2019 [
Internet]. Rio de Janeiro, Brasil; 2020. [access in 2024 Mai 20]. Available from:
https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=210173620. Jain L, Juneja R, Kansal R, Kumar V. Prevalence of myths regarding oral health among pregnant women in North India. Int J Dent Hyg. 2021; 19 (1): 127–34.
21. Ministério da Saúde (BR). Portaria no 1.459, de 24 de junho de 2011. Institui, no âmbito do Sistema Único de Saúde - SUS - a Rede Cegonha. Brasília (DF): DOU 27 de junho 2011. [access in 2024 Mai 20]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt1459_24_06_2011.html22. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde Bucal. Brasília (DF): Ministério da Saúde; 2008. 92 p. – (Série A. Normas e Manuais Técnicos) (Cadernos de Atenção Básica; 17). [access in 2024 Mai 20]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/saude_bucal.pdf23. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. A saúde bucal no Sistema Único de Saúde. [
Internet]. Brasília (DF): Ministério da Saúde; 2018. [access in 2024 Mai 20]. Available from:
http://bvsms.saude.gov.br/bvs/publicacoes/saude_bucal_sistema_unico_saude.pdf 24. Ministério da Saúde (BR). Portaria Nº 2.979, de 12 de novembro de 2019. Institui o Programa Previne Brasil, que estabelece novo modelo de financiamento de custeio da Atenção Primária à Saúde no âmbito do Sistema Único de Saúde. Diário Oficial da República Federativa do Brasil. Brasília (DF), n. 220, p. 97. 13 nov. 2019a. Seção 1. [access in 2024 Mai 20]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2019/prt2979_13_11_2019.html25. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D, Maynor G,
et al. Periodontal infection as a possible risk factor for preterm low birth weight. J Periodontol. 1996 Oct; 67 (10 Suppl.): 1103-13.
26. Ha JE, Jun JK, Ko HJ, Paik DI, Bae KH. Association between periodontitis and preeclampsia in never-smokers: a prospective study. J Clin Periodontol. 2014 Sep; 41 (9): 869-74.
27. Manrique-Corredor EJ, Orozco-Beltran D, Lopez-Pineda A, Quesada JA, Gil-Guillen VF, Carratala-Munuera C. Maternal periodontitis and preterm birth: Systematic review and meta-analysis. Community Dent Oral Epidemiol. 2019 Jun; 47 (3): 243-51.
28. Boggess KA, Lieff S, Murtha AP, Moss K, Beck J, Offenbacher S. Maternal periodontal disease is associated with an increased risk for preeclampsia. Obstet Gynecol. 2003. 101: 227-31.
29. Cagetti MG, Salerno C, Ionescu AC, La Rocca S, Camoni N, Cirio S,
et al. Knowledge and attitudes on oral health of women during pregnancy and their children: an online survey. BMC Oral Health. 2024 Jan 16; 24 (1): 85.
30. Paula-Silva FWG. Pré-Natal Odontológico. 1º ed. São Paulo: Santos Publicações; 2023.
Authors' contributionsCarvalho DCS: conceptualization, data curation, research, manuscript writing. Souza MCS: data curation, research, writing, review, and editing of the manuscript. Dantas MFS: data curation, research, manuscript writing. Silva K: methodology, manuscript writing. Oliveira-Vanderlei KMH: conceptualization, methodology, project management, supervision, manuscript writing, review, and editing. All authors approved the final version of the article and declare no conflict of interest.
Data availabilityThe entire dataset supporting the results of this study was published in the article itself.
Received on June 20, 2024
Final version presented on August 18, 2025
Approved on Augusut 19, 2025
Associated Editor: Aurélio Costa


 ; Maria Carolina Santos Souza2
; Maria Carolina Santos Souza2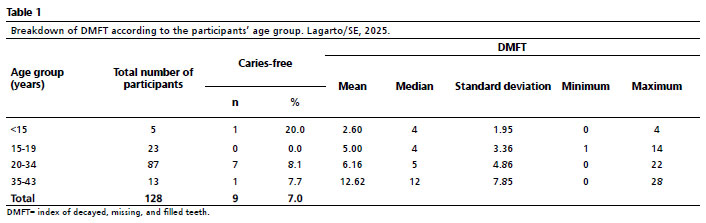






 Ler em português
Ler em português