ABSTRACT
OBJECTIVES: to analyze the spatial distribution and temporal trend of the maternal mortality ratio in Pernambuco, before and during the COVID-19 pandemic.
METHODS: mixed ecological study, based on the maternal mortality ratio. The spatial units were the resident municipalities and health regions in the pre-pandemic (2017-2019) and pandemic (2020-2022) periods. The risk ratio was calculated using the pre-pandemic period as a reference. The temporal units were semesters, analyzed using the Joinpoint regression model.
RESULTS: the maternal mortality ratio increased by 14.5%, from 55.9 to 64.0 per 100,000 live births; an increase was observed in five health regions and in 63 (50.8%) of the 124 municipalities with registered deaths. In the time series, a decreasing trend in the ratio was observed between the first half of 2021 and the second half of 2022.
CONCLUSION: maternal mortality increased in some health regions and in most municipalities, highlighting the need to prioritize pregnant and postpartum women during health crises. The temporal analysis shows a decreasing trend, suggesting effective actions by health services. The implementation of policies that ensure the continuity of care is crucial to reduce preventable maternal deaths.
Keywords:
COVID-19, Maternal mortality, Time series studies, Spatial analysis, Ecological studies
RESUMO
OBJETIVOS: analisar a distribuição espacial e a tendência temporal da razão de mortalidade materna em Pernambuco, antes e durante a pandemia pela COVID-19.
MÉTODOS: estudo ecológico misto, composto pela razão da mortalidade materna. As unidades espaciais foram os municípios e regiões de saúde de residência nos períodos pré-pandêmico (2017-2019) e pandêmico (2020-2022). Calculou-se a razão de risco tendo como referência o período pré-pandêmico. As unidades temporais foram os semestres de ocorrência, analisados por meio do modelo de regressão Joinpoint.
RESULTADOS: a razão de mortalidade materna aumentou 14,5%, saindo de 55,9 para 64,0 por 100.000 nascidos vivos; observou-se elevação em cinco regiões de saúde e em 63 (50,8%) dos 124 municípios com óbitos maternos registrados. Na série temporal, observou-se tendência decrescente da razão entre o primeiro semestre de 2021 até o segundo semestre de 2022.
CONCLUSÃO: a mortalidade materna aumentou em algumas regiões de saúde e na maior parte dos municípios, destacando a necessidade de priorizar gestantes e puérperas em crises sanitárias. A análise temporal mostra uma tendência de decréscimo, sugerindo ações eficazes dos serviços de saúde. A implementação de políticas que garantam a continuidade do cuidado de serviços de saúde é crucial para reduzir óbitos maternos evitáveis.
Palavras-chave:
COVID-19, Mortalidade materna, Estudos de séries temporais, Análise espacial, Estudos ecológicos
IntroductionMaternal death, defined as the death of women during the pregnancy-puerperal cycle, is an undesirable event that is mostly preventable and requires mandatory notification to international health authorities.
1 According estimates from the World Health Organization (WHO), in 2020, about 800 women died every day from preventable maternal causes, and nearly 95% of these deaths occurred in developing countries.
2The distribution of maternal mortality reflects social vulnerabilities in geographic spaces, producing patterns that show a concentration of risk in the poorest areas.
3 Events that cause crises in health services, such as the COVID-19 pandemic, reinforce existing vulnerabilities, exacerbating flaws in access and care, which in turn leads to an increase in maternal mortality.
4In the period from December 2019 to June 2020, six countries reported 160 maternal deaths due to COVID-19 worldwide; of these, 124 occurred in Brazil.
5 For the year 2021, according to
Observatório COVID-19 Fiocruz (COVID-19 Fiocruz Observatory), the number of maternal deaths due to COVID-19 was 1,519, which represented 3.3 times the number of deaths recorded in 2020.
6 Similarly to national data, the state of Pernambuco had a number of deaths due to COVID-19 in 2021 that was 1.9 times higher than the previous year.
7The COVID-19 pandemic, associated with the precarization of health services, led Brazil to revert to the maternal mortality rates of the 1990s, when over 100 maternal deaths per 100,000 live births occurred.
8 Accordingly, collaborative efforts are necessary across all government, public and private sectors to mitigate deaths during pregnancy, childbirth and the puerperium.
Spatiotemporal ecological studies allow for the identification of inequalities in the distribution of maternal mortality risk, in addition to assessing the provision, access, and quality of health services, thus informing rapid-response actions and the enhancement of obstetric care in priority areas.
11-13 In this context, epidemiological analyses that encompass spatial and temporal dimensions are essential to identify vulnerable territories and guide public policies. The present study aims to analyze the spatial distribution and temporal trend of the maternal mortality ratio in Pernambuco, before and during the COVID-19 pandemic.
MethodsThis is a mixed ecological study with a temporal and spatial approach, comprising all maternal deaths of residents in Pernambuco, as recorded in the Mortality Information System (SIM – Portuguese acronym), from 2017 to 2022. This period corresponds to both the pre-pandemic triennium (2017-2019) and the pandemic triennium (2020-2022).
The state of Pernambuco comprises 184 municipalities and the administrative district of Fernando de Noronha, organized into 12 regional health authorities. The state is home to approximately 3,034,239 women between ten to 49 years.
The units for spatial analysis were the municipalities of the state of Pernambuco. Fernando de Noronha was excluded due to its lack of contiguity with the mainland, which prevents any spatial correlation analysis. The 12 semesters from 2017 to 2022 constituted the temporal analysis units.
Deaths of women aged ten to 49 years were analyzed, specifically those in the pregnancy-puerperal cycle up to 42 days after the end of pregnancy. The underlying cause of death was any code of the Chapter XV of the International Statistical Classification of Diseases and Related Health Problems (ICD-10), as well as the other maternal causes classified in other chapters: Obstetric Tetanus (A34); Mental and behavioral disorders associated with the puerperium, not-elsewhere classified (F53); Puerperal Osteomalacia (M83.0); Neoplasm of uncertain or unknown behavior of placenta (D39.2); Hypopituitarism (E23.0); and HIV/AIDS (B20-B24).
Deaths from external causes were excluded (O93), in addition to deaths from any obstetric cause that occurred more than 42 days but less than one year after childbirth (O96), and deaths from sequelae of direct obstetric causes occurring more than one year after childbirth (O97).
Data were obtained from the Mortality Information System and the Live Birth Information System using the Tabnet platform, available on DataSUS. The data were accessed on April 10, 2025. In the spatial analysis, we used cartographic meshes obtained from the Brazilian Institute of Geography and Statistics, accessed on April 10, 2025.
The indicator used was the Maternal Mortality Ratio (MMR), which is calculated by dividing the number of maternal deaths by the number of livebirths given geographic area and time period, multiplied by 100,000.
Variables related to the date of death were analyzed and used for the temporal analysis of the MMR, by year and by semester. In this study, the MMR was calculated dividing the number of maternal deaths by the number of live births by semester. In the distribution of the MMR and spatial analysis, municipalities of residence were used. The MMRs were classified into: low (MMR<20 by 100,000 Live Births – LB); medium (MMR 20-50 by 100,000 LB); high (MMR 50-150 by 100,000 LB) or very high (>150 by 100,000 LB). We also calculated the risk ratio of municipalities and health regions within the periods, according to the expression bellow:
Where: CV is the current value and RV is the reference value. We used the pre-pandemic datum as the reference value.
The risk ratio compares the probability of an outcome between the exposed and unexposed groups to a specific factor. Values greater than one indicate an increase in risk; values less than one, a decrease.
14In order to assess the temporal impact of COVID-19, we analyzed the MMR trend in Pernambuco from 2017 to 2022, with a semester-based disaggregation (12 observations). We applied the Joinpoint regression model, which identifies significant changes in trends and estimates the Semestral percent change (SPC), with 95% confidence intervals and 5% significance level.
15,16 The best model was selected with Schwarz's Bayesian Information Criterion (BIC). The analyses were performed using Joinpoint software, version 4.9.0.1.
The study was developed in accordance with Resolutions 466/2012 and 674/2022 of the
Conselho Nacional de Saúde (National Health Council). Since it uses public data with aggregated information that prevents the identification of participants, it was exempted from review by the Research Ethics Committee on Human Beings.
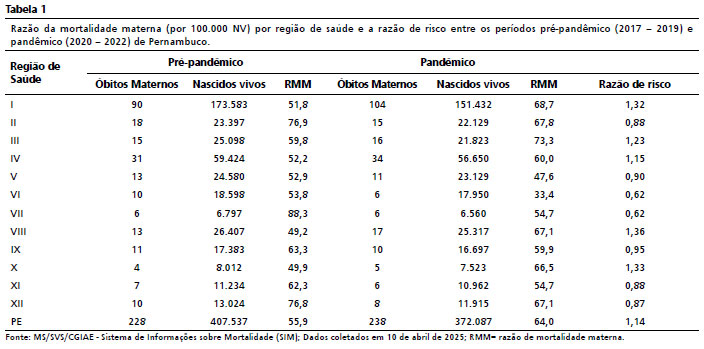
ResultsIn the study period, 466 maternal deaths were recorded in Pernambuco. In the triennium preceding the pandemic, the MMR was 55.9. During the pandemic triennium, it was 64.0 per 100,000 LB, which represents a 14.5% increase (Table 1).
The distribution of the MMR by health region showed that, of the 12 health regions, five (I, III, IV, VIII, X) experienced an increase in the MMR during the three pandemic years. We highlight health region III, which experienced the highest MMR in the pandemic period (73.3 per 100,000 LB) and health region VIII, which experienced the greatest risk ratio, 1.36 (Table 1).
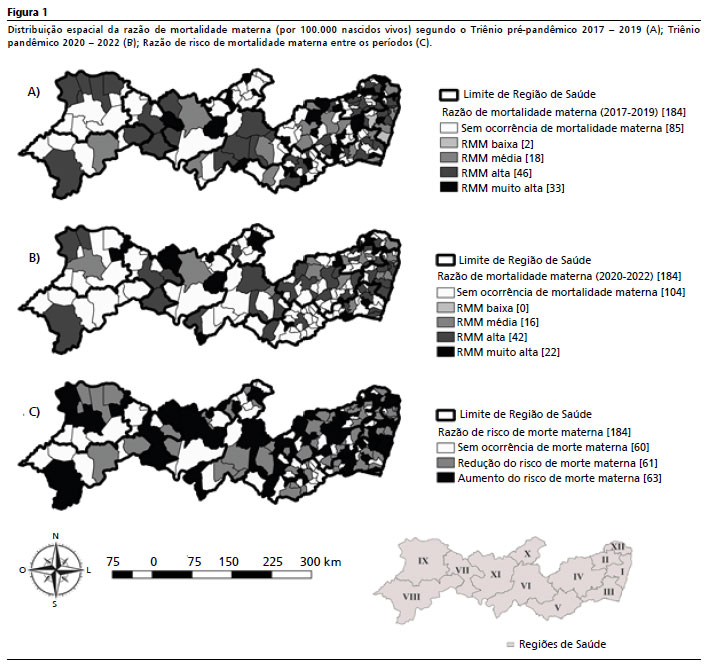
In the spatial distribution of MMR by municipalities, 99 municipalities recorded maternal deaths during the pre-pandemic period. Of these, 46 (46.46%) had a high MMR and 33 (33.33%), had a very high MMR. Two (2.02%) municipalities showed a low MMR (Figure 1A). During the pandemic period, 80 municipalities recorded maternal deaths. Of these, 42 (52.50%) had a high MMR and 22 (27.50%) had a very high MMR (Figure 1B). In the comparative analysis between the periods, we observed that 124 municipalities recorded maternal deaths in at least one of the periods. Of these, 63 (50.81%) had an increased risk of maternal death during the pandemic period (Figure 1C).
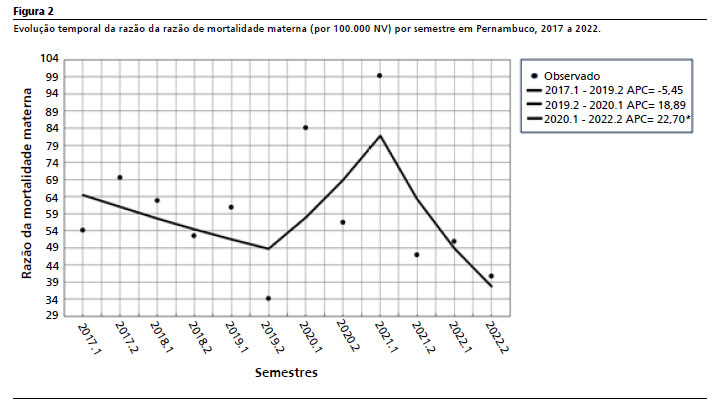
The analysis of the time series using the Joinpoint regression model revealed three trends. The first two, (2017 to 2019) and (2020 to 2021) were stationary. The third trend was decreasing during the period of the second semester of 2021 and 2022, (SPC = -22.7;
p=0.049) (Table 2 and Figure 2).
DiscussionThis study observed an increased risk of maternal death during the pandemic triennium in some of the municipalities and health regions of the state of Pernambuco that had recorded maternal deaths. The analysis of the time Semestral time series by semester demonstrated a decreasing trend in the maternal mortality ratio starting in the second semester of 2021 and continuing until the end of the study period.
The first years of the public health crisis were the period in which the majority of maternal deaths occurred, and consequently, an increase in the MMR. This finding aligns with a study conducted in Brazil on the temporal trend, which reported excess maternal mortality in the majority of months.
17 Initially, the scarcity of diagnostic resources and the lack of knowledge on the adequate management of pregnant and puerperal women with COVID-19 were factors that heightened the risk of maternal death.
18,19 Moreover, the unavailability of vaccines further weakened the healthcare network, especially in local communities where the availability of services is insufficient, and resources are limited.
18 This led to several flaws that include not only a decrease in prenatal consultations, but also impaired access to high-complexity services, such as intensive care units.
19Although the services provided to pregnant and puerperal women were not discontinued, the COVID-19 pandemic strained health services, which occasionally hindered access.
4,10,20 Besides the direct consequences of having COVID-19, the restrictions in displacement, combined to the insecurity in relation to contamination promoted a decrease in prenatal consultations.
21 Accordingly, diseases that should be diagnosed and treated during prenatal care evolved to unfavorable outcomes.
22,23 Thus, there was an increase in MMR,
24 which is consistent with the present study.
An ecological study conducted in Brazil from 2010 to 2020, aiming to assess the impact of COVID-19 on maternal mortality, evidenced a significant difference in the increase in the number of maternal deaths between women with low-risk pregnancies, that is, those who did not have an elevated risk of sepsis and hemorrhages.
25 Thus, in the year 2020, the straining of obstetric services during the pandemic may have had a greater impact on deaths from direct obstetric causes than either COVID-19 or preexisting comorbidities.
25It is widely known that the risk of maternal death is geographically uneven. Areas with lower economic development and impaired availability of access to actions and basic health services demonstrate higher risk.
18,19,26 Poverty, suboptimal referral conditions and delayed access to care may lead to unfavorable maternal outcomes.
26 Additionally, healthcare hubs tend to be concentrated in the metropolitan regions of the states. The health region I is the most populous one and concentrates 41.9% of obstetric beds and 70.9% of ICU beds in the state. This uneven distribution of health services leads to flaws in the timely access, since long-distance displacements is a reality.
12The time series analysis of MMR in Pernambuco demonstrated a stationary trend in the first pandemic years. In spite of stationarity as the result of the temporal analysis model adopted, it is important to observe that the ratio between 2020 and the first half of 2021 demonstrates higher numbers. This is a reflection of an excess in the number of maternal deaths and of the decrease of the number of live births during COVID-19 pandemic. An exploratory study aiming to assess the effects of COVID-19 pandemic on maternal mortality in Brazil in 2021, revealed that, compared to the trend of the five preceding years, 2021 had a 39% excess mortality.
27For 2022, the study observed a decreasing trend in MMR. This reduction may be related to the control of the pandemic, aligned with the normalization of prenatal consultations, the increase of bed availability, in addition to the mass testing. Another important factor was the availability of vaccines for pregnant and puerperal women.
28Despite the protective effect of vaccines, the rollout of vaccination campaign against COVID-19 for pregnant and puerperal women in Brazil was marked by delays in the procurement of immunizing agents, logistical shortcomings, and delayed issuance of specific guidelines from the Ministry of Health.
29 These barriers contributed to the increase in maternal mortality in 2021. The temporal analysis indicates that the reduction in the risk of maternal death observed at the end of the pandemic could have occurred earlier if governmental actions had been timelier.
For this study, it is important to clarify that the codes O96, pertaining to late maternal death, and O97, which describes deaths from sequelae of direct obstetric causes, are, by definition, not considered in the MMR calculation.
1 However, taking into account that late maternal deaths are avoidable and may reflect the increase in survival due to developments in health technology, studies that include these deaths in their analyses are necessary.
An important limitation of the study is that maternal death is a rare event, which impairs its analysis and interpretation in small populations. Moreover, since the analysis uses secondary data, the inadequate completion of death certificates, specifically regarding the cause and moment of death in the pregnancy-puerperal period, in addition to potential errors in coding or data entry, may cause underregistration of maternal deaths, negatively affecting MMR estimates. Nonetheless, the health information systems in Pernambuco have been showing satisfactory quality in relation to vital events, which reinforces their use as reliable tools for the analysis of the health situation.
30The study showed an increase in maternal mortality in the majority of health regions and municipalities of the state, which reinforces the need for prioritizing pregnant and puerperal women during public health crises. The decreasing trend observed in the temporal analysis reflects the effective action of health services. The implementation of strategic policies that ensure the continuity of prenatal care and other essential types of care, especially for vulnerable groups, improves access to healthcare and reduces avoidable deaths.
References1. Smith H, Ameh C, Roos N, Mathai M, Broek NVD. Implementing maternal death surveillance and response: a review of lessons from country case studies. BMC Pregnancy Childbirth. 2017; 17 (1): 1-11.
2. World Health Organization (WHO). Maternal Mortality: Key facts [
Internet]. Geneva: WHO; 2023 Feb 22 [access in 2023 May 10]. Available from:
http://www.who.int/mediacentre/factsheets/fs348/en/3. Kotsadam A, Østby G. Armed conflict and maternal mortality: a micro-level analysis of sub-Saharan Africa, 1989–2013. Soc Sci Med. 2019; 239: 112526.
4. Andreucci CB, Knobel R. Social determinants of COVID-19-related maternal deaths in Brazil. Lancet Reg Health Am. 2021; 3: 100104.
5. Nakamura‐Pereira M, Andreucci CB, Menezes MO, Knobel R, Takemoto MLS. Worldwide maternal deaths due to COVID‐19: a brief review. Int J Gynaecol Obstet. 2020; 151 (1): 148-50.
6. Observatório Obstétrico Brasileiro (OOBr). Óbitos de Gestantes e Puérperas [
Internet]. São Paulo: OOBr; 2022 [access in 2023 Jun 2]. Available from:
https://observatorioobstetrico.shinyapps.io/obitos-grav-puerp7. Secretaria Estadual de Saúde de Pernambuco. Boletim epidemiológico: Morte materna em Pernambuco [
Internet]. Recife: CIEVSPE; 2023 [access in 2023 Jun 20]. Available from:
https://www.cievspe.com/_files/ugd/3293a8_c656df0449c54e4ba79236174033bbb5.pdf8. Lourenço C. Uma sociedade desigual: reflexões a respeito de racismo e indicadores sociais no Brasil. Serv Soc Soc. 2023; 146 (1): 75-96.
9. Orellana J, Jacques N, Leventhal DGP, Marrero L, Morón-Duarte LS. Excess maternal mortality in Brazil: Regional inequalities and trajectories during the COVID-19 epidemic. PLoS One. 2022; 17 (10): e0275333.
10. Long S, Loutfi D, Kaufman JS, Schuster T. Limitations of Canadian COVID-19 data reporting to the general public. J Public Health Policy. 2022; 43 (2): 203-21.
11. Guha, P. Spatiotemporal Analysis of COVID-19 Pandemic and Predictive Models based on Artificial Intelligence for different States of India. J Inst Eng India Ser B. 2021; 102 (6): 1265-74.
12. Boitrago GM, Mônica RB, Silva DM, Cerroni MDP, Cortez-Escalante JJ, Almiron M,
et al. Reestruturação dos serviços de emergência à COVID-19 no Brasil: uma análise espaço-temporal, fevereiro a agosto de 2020. Epidemiol Serv Saúde. 2021; 30 (4): e2020791.
13. Xavier DR, Silva, EL, Lara FA, Silva GR, Oliveira MF, Gurgel H,
et al. Involvement of political and socio-economic factors in the spatial and temporal dynamics of COVID-19 outcomes in Brazil: A population-based study. Lancet Reg Health Am. 2022; 10: 100221.
14. Furcada JM, Patino CM, Ferreira JC. Estimando risco em estudos clínicos: razão de chances e razão de risco. J Bras Pneumol. 2020; 46 (2): e20200137.
15. Muggeo VMR. Estimating regression models with unknown break‐points. Stat Med. 2003; 22 (19): 3055-71.
16. Souza CDFD, Paiva JPSD, Silva LFD, Leal TC, Magalhães MDAFM. Tendência da mortalidade por tuberculose no Brasil (1990-2015): análise por pontos de inflexão. J Bras Pneumol. 2019; 45 (2): e20180393.
17. Guimarães RM, Reis LGC, Gomes MASM, Magluta C, Freitas, CM, Portela MC. Tracking excess of maternal deaths associated with COVID-19 in Brazil: a nationwide analysis. BMC Pregnancy Childbirth. 2023; 23 (1): 22.
18. Siqueira TS, Souza EKG, Martins-Filho PR, Silva JRS, Gurgel RQ, Cuevas LE,
et al. Clinical characteristics and risk factors for maternal deaths due to COVID-19 in Brazil: a nationwide population-based cohort study. J Travel Med. 2022; 29 (3): taab199.
19. Ribeiro HF, Carvalho MDB, Pelloso FC, Santos LD, Silva MAP, Stevanato KP,
et al. Maternal Risk Factors Associated with Negative COVID-19 Outcomes and Their Relation to Socioeconomic Indicators in Brazil. Healthcare (Basel). 2023; 11 (14): 2072.
20. Dintrans PV, Maddaleno M, Román YG, Delpiano PV, Castro A, Vance C,
et al. ProjectInterrupção dos serviços de saúde para grávidas, recém-nascidos, crianças, adolescentes e mulheres durante a pandemia de COVID-19: projeto ISLAC 2020. Rev Panam Salud Publica. 2021;45: e140.
21. Hallal PC, Horta BL, Barros AJ, Dellagostin OA, Hartwig FP, Pellanda LC, et al. Trends in the prevalence of COVID-19 infection in Rio Grande do Sul, Brazil: repeated serological surveys. Ciên Saúde Colet. 2020; 25 (Suppl. 1): 2395-401.
22. Villar J, Ariff S, Gunier RB, Thiruvengadam R, Rauch S, Kholin A,
et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: the INTERCOVID multinational cohort study. JAMA Pediatr. 2021; 175 (8): 817-26.
23. Alberton M, Rosa VM, Iser BPM. Prevalence and temporal trend of prematurity in Brazil before and during the COVID-19 pandemic: a historical time series analysis, 2011-2021. Epidemiol Serv Saúde. 2023; 32 (2): e2022603.
24. Leal LJ, Merckx J, Fell DB, Kuchenbecker R, Miranda AE, Oliveira WK,
et al. Characteristics and outcomes of pregnant women with SARS-CoV-2 infection and other severe acute respiratory infections (SARI) in Brazil from January to November 2020. Braz J Infect Dis. 2020; 25 (5): 101620.
25. Michels BD, Marin DFD, Iser BPM. Increment of maternal mortality among admissions for childbirth in low-risk pregnant women in Brazil: Effect of COVID-19 Pandemic? Rev Bras Ginecol Obstet. 2022; 44 (8): 740-5.
26. Ajavon DRD, Edem LAK, Yendoube K, Sibabe A, Hélène A, Christine B,
et al. Causes of maternal mortality in 2020 in the Kara Region (Togo). Open J Obstet Gynecol. 2022; 12 (1): 104-11.
27. Guimarães, Raphael Mendonça; Moreira, Marcelo Rasga. Mortes maternas como desafio para a assistência obstétrica em tempos da COVID-19 no Brasil. Rev Bras Saúde Mater Infant. 2024; 24: e20230078.
28. Paganoti CF, Costa RA, Papageorghiou AT, Costa FS, Quintana SM, Godoi LG,
et al. COVID-19 Vaccines confer protection in hospitalized pregnant and postpartum women with severe COVID-19: a retrospective cohort study. Vaccines (Basel). 2022; 10 (5): 749.
29. Maciel E, Fernandez M, Calife K, Garett D, Domingues C, Kerr L,
et al. A campanha de vacinação contra o SARS-CoV-2 no Brasil e a invisibilidade das evidências científicas. Ciênc Saúde Colet. 2022; 27 (3): 951-6.
30. Marques LJP, Oliveira CM, Bonfim CV. Assessing the completeness and agreement of variables of the Information Systems on Live Births and on Mortality in Recife-PE, Brazil, 2010-2012. Epidemiol Serv Saúde. 2016; 25 (4): 849-54.
Authors' contributionOliveira HJP: conceptualization and design of the study, analysis and interpretation of results, writing and critical review of the manuscript. Bonfim CV: conceptualization and design of the study and critical review of the manuscript. Barbosa CC: critical review of the manuscript. Maciel MMSA: writing and critical review of the manuscript. Silva APSC: conceptualization and design of the study, analysis and interpretation of results and critical review of the manuscript. All authors approved the final version of the article and declared no conflicts of interest.
AcknowledgementsWe thank the
Fundação de Amparo à Ciência e Tecnologia de Pernambuco (Foundation of Support to Science and Technology of Pernambuco) (APQ-0389-4.06/20), by means of the
Programa de Pesquisa para o SUS: Gestão Compartilhada em Saúde (SUS Research Program: Shared Management in Healthcare) (PPSUS/PE-2020).
Data availabilityAll datasets supporting the results of this study are included in the article.
Received on June 21, 2024
Final version presented on June 27, 2025
Approved on July 1, 2025
Associated Editor: Melania Amorim


 ; Cristine Vieira do Bonfim2
; Cristine Vieira do Bonfim2







 Ler em português
Ler em português