ABSTRACT
OBJECTIVES: to analyze the factors associated with late prenatal care attendance by pregnant women at the Lugela health center in the first quarter of 2023.
METHODS: cross-sectional survey conducted with 205 pregnant women. Data were collected using a structured questionnaire, supplemented with information from the pregnant woman's prenatal records. R software version 4.2.0 was used to perform inferential statistical analyses, calculating odds ratios (ORs) and constructing a logistic regression model. Categorical variables were analyzed descriptively and tested for associations with late prenatal care attendance. Multivariate logistic regression considered a significance level of 5%, with early prenatal care attendance as the dependent variable.
RESULTS: 69.3% (n=142) of the pregnant women interviewed considered prenatal care initiation late. Late prenatal care seeking was significantly associated with education (p=0.034, OR=0.228, 95%CI= -2.915 to -0.046), age (p=0.040, OR=0.506, 95%CI= -1.369 to 0.006), and pregnancy planning (p=0.009, OR=0.451, 95%CI= -1.485 to -0.106).
CONCLUSION: the factors associated with late prenatal care seeking were essentially obstetric, socioeconomic, and sociodemographic, highlighting the need for strategies targeted at more vulnerable groups.
Keywords:
Prenatal care, Associated factors, Mozambique
RESUMO
OBJETIVOS: analisar os fatores associados à procura tardia por atendimento pré-natal por gestantes no centro de saúde de Lugela, no primeiro trimestre de 2023.
MÉTODOS: pesquisa transversal realizada com 205 gestantes. Os dados foram coletados por meio de questionário estruturado, complementado com informações da ficha pré-natal da gestante. Utilizou-se o software R versão 4.2.0 para realização de análises de estatísticas inferenciais, com cálculo do odds ratio (OR) e construção de modelo de regressão logística. Variáveis categóricas foram analisadas descritivamente e testadas quanto à associação com a procura tardia do pré-natal. A regressão logística multivariada considerou nível de significância de 5%, tendo como variável dependente a adesão precoce à consulta pré-natal.
RESULTADOS: o início do pré-natal foi considerado tardio para 69,3% (n=142) das gestantes entrevistadas. A procura tardia esteve significativamente associada à escolaridade (p=0,034, OR=0,228, IC95%=-2.915 a -0.046), à idade (p=0,040, OR=0,506, IC95%= -1.369 a 0.006) e ao planejamento da gravidez (p=0,009, OR=0,451, IC95%= -1.485 a -0.106).
CONCLUSÃO: os fatores associados a procura tardia da assistência pré-natal foram essencialmente de âmbito obstétrico, socioeconómico e sociodemográfico, evidenciando a necessidade de estratégias direcionadas para grupos mais vulneráveis.
Palavras-chave:
Assistência pré-natal, Fatores associados, Moçambique
IntroductionThe World Health Organization (WHO) envisions a world where all women and newborns receive high-quality care throughout pregnancy, childbirth, and the post-natal period. Antenatal care (ANC), also known as prenatal care, serves as a platform for important healthcare functions, including health promotion, screening, diagnosis, and disease prevention.
1,2Studies have demonstrated that the combination of prenatal care and risk prevention during pregnancy provides pregnant women with a healthy life. The success of prenatal care depends on the timing and number of consultations.
3,4Accordingly, early initiation is one of the factors associated with adequate prenatal care, which aims to decrease maternal and neonatal mortality, ensuring the birth of a healthy infant at the end of the pregnancy and maternal satisfaction.
5,6In Africa, over two thirds of pregnant women attend at least one prenatal care consultation. To achieve this life-saving potential of ANC for women and neonates, four or more medical consultations are required, a package often referred to Focused Prenatal Care.
7,8A study concerning opportunities for newborns in Africa demonstrated 71% ANC coverage, while in developed countries, this figure was over 95%. In Sub-Saharan Africa, 69% of pregnant women have at least one prenatal consultation. However, the main challenge is the coverage of early initiation, which is less than 44% in Africa.
9According to Mozambique's 2021 health sector report, 95% of pregnant women had at least one prenatal consultation, and of these, 11% attended the healthcare facility at 12 weeks of pregnancy or less. On the other hand, the 2021 health statistical yearbook for Zambezia province, revealed 100% coverage of pregnant women who benefited from ANC consultations, but only 11% had their first consultation with a gestational age of 12 weeks or less.
10,11According to data from Mozambique's latest Demographic and Health Survey (DHS 2022-2023), 87% of women who attended a maternity service in the two years preceding the inquiry, received prenatal care from a qualified health professional. However, concerning the provinces, Zambezia shows the lowest coverage (66%). The survey revealed that coverage of four or more prenatal consultations for women who had a live birth within two years prior to the survey varied across provinces, with Maputo showing the highest percentage (83%) and Zambezia the lowest (26%).
11Regarding the study location, 90.2% of pregnant women received ANC. Of these, 4% had their first consultation before 12 weeks, ranking second in achieving the provincial goal for Zambezia Province. The Namarrói district ranked first with 3% of reaching this goal during the analysis period.
12,13According to WHO (2016), late prenatal care is defined as the initiation of prenatal care after the 12th week of pregnancy.
9 This late initiation compromises the adequate follow-up of the pregnancy, hindering the timely completion of supplementary tests and leading to negative maternal and fetal outcomes.
13Therefore, the present study aimed to analyze factors associated with the delayed initiation of prenatal care at the Lugela health center.
MethodsThe research was conducted in Lugela district, situated in the central region of Zambezia province, 210 km from the capital city of Quelimane. It has an area of 6,178 km
2 and is located between parallels 15º 18' South and 15º 20' South, and meridians 36º 08' and 36º 14'. This represents about 5.9% of the province's total area (105,008 km
2). The district is bordered to the south by the Mocuba district, along the Lugela River; to the north by the Namarrói district, via the Lú River; to the east by the Ile and Mocuba districts, along the Licungo River; and to the west by the Milange district. The data collection process was carried out at the health center in the district's main village. The Lugela health center was selected because it is one of the district's two level I health facilities that have low ANC coverage up to 12 weeks of pregnancy.
Healthcare facilities in rural areas are classified as Type I and Type II. Type II facilities are the smaller ones that provide primary healthcare services and do not offer inpatient care in rural areas. Type I facilities are larger, more specialized, and offer inpatient services.
14 The average life expectancy of the district's population is 46 years, and the illiteracy rate is 70.9% (49.5% for men and 87.4% for women). The fertility rate is 7.9%.
15 This was a cross-sectional study with a quantitative approach.
The research was conducted from January to March, comprising the first quarter of 2023. This period was when data was collected at the study site.
The study population included individuals aged 18 years or older. The sample size was 205 pregnant women who attended the health center during normal working hours seeking prenatal care. A non-probabilistic convenience sampling technique was used.
For the calculation of sample size, a projection of the monthly mean values of prenatal care service usage at the study location was considered. Based on these means, the sample size was calculated using a 95% confidence interval and a 5% margin of error.
16Inclusion criteria were pregnant women who attended prenatal consultations at the health center during the study period, were 18 years of age or older, and who agreed to participate in the study. The exclusion criteria comprised any acute or chronic condition that limited pregnant women's ability to participate in the study, pregnant women with impaired mental health, and those aged under 18 years. The non-inclusion of adolescent pregnant women was due to the difficulty in obtaining assent and informed consent.
The dependent variable was benefiting from or adhering to prenatal consultations. The independent variables related to sociodemographic characteristics were: age group in years (18–24 years and >25 years); educational attainment (no schooling, primary, secondary, university); place of residence (around the village Yes/No); marital status (with partner or without partner); distance from home to the hospital (<10 km or >10 km); pregnancy planning (Yes or No); time in months from seeking prenatal services (1–3 months, 4 or more); number of children; occupation (farmer, self-employed, non-governmental organization - NGO, public sector); economic variable: average monthly income in minimum wage, corresponding to R$ 676.97 (1–3, 4–5, don't know).
For the study, the data collection technique used was face-to-face interviews. Trained interviewers used a structured interview guide for women eligible for the study. Data collection was also completed using the pregnant woman's prenatal form "Mod-SIS-B01-B," which is intended for use at her first and subsequent contacts with the health facility to record demographic and obstetric variables for the purpose of monitoring the pregnancy. The selection of participants was performed by the trained data collection team, who identified potential participants as soon as they left their prenatal care appointments. Participants were then led to a specific room to ensure greater privacy, where they were informed about the study's purpose and the informed consent process. If the pregnant women consented to participate in the study, the interviewers proceeded with data collection, guided by the structured questionnaire.
Microsoft Excel version 2016 and the R statistical package version 4.2.0 were used for data analysis. Excel was used to create the database, perform descriptive statistics, and format tables. The R package was used for inferential analysis, including tests of association between variables, univariate logistic regression, and Fisher's exact test for values less than five. For the multiple logistic regression analysis, a 5% significance level was considered statistically significant.
The final logistic regression analysis identified a significant association between prenatal care outside the recommended period and the variables of maternal age, education, and pregnancy planning. Based on this finding, a reduced model was developed. Subsequently, a comparison between the two models was performed using the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) to assess the quality of the fit.
17,18The AIC and BIC criteria served as auxiliary tools for final model selection, providing an objective metric for model comparison. The approach of choosing the model with the lowest AIC aligns with the goal of finding a balance between model complexity and fit.
18The AIC and BIC were chosen for model selection because they allow for the comparison of different models, helping to select the one with the best fit. Both criteria penalize complex models, which helps to avoid overfitting (excessive fit to the training data) and ensures the chosen model is capable of explaining the data's patterns.
17The Wald test was applied to the research to evaluate the logistic model as a whole. This test is used to determine the significance of the estimated model coefficients, checking if each coefficient is significantly different from zero.
17,18The study was approved by the research ethics committee of the Higher Institute of Health Sciences of Maputo under code TFCMEPS15/22. Furthermore, data collection was authorized by the administrative entities that oversee the Lugela health center.
ResultsRegarding the initiation of prenatal care, the criterion for prenatal care was considered non-recommended for 69.3% (n=142) of pregnant women and recommended for 30.7% (n=63), according to WHO guidelines. For the age group variable, 49.2% (n=101) of those who attended prenatal consultations were over 25 years old, and of these, 75.2% had a late initiation of prenatal care. Concerning marital status, 66.7% of those who affirmed not having a partner had late initiation. With regard to educational attainment, 63.3% of those who reported having no education or only the primary level had late initiation of prenatal care. Regarding residence, 65.5% of the pregnant women who reported to live outside the village initiated prenatal care in an inadequate period.
Regarding the descriptive analysis of gestational variables, 60% of respondents who initiated prenatal care late were multiparous. As for pregnancy planning, 77.9% of those who reported not having planned their pregnancy had a late initiation of prenatal care. Finally, regarding partner support during pregnancy, it was found that 72.3% of those who reported not receiving support initiated prenatal care late. (Table 1)
For the socioeconomic variable, 70.6% of the women surveyed who reported an income between one and three minimum wages initiated prenatal care during a non-recommended period.
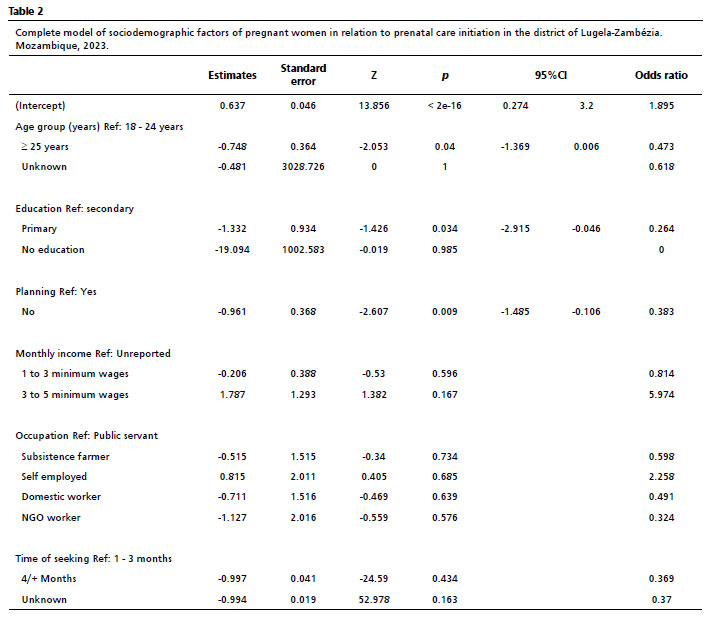
The analysis of variables in the final logistic regression model (Table 2), after variable selection, showed a significant
p-value for prenatal care outside the recommended period in the variables of maternal age, education, and pregnancy planning.
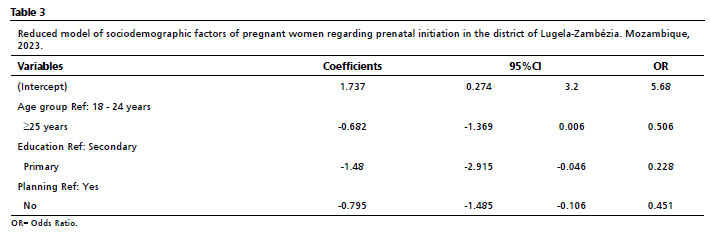
For the education variable, women who reported having a primary or no education had a 22.8% reduced chance of seeking prenatal care in the first months after conception compared to those with a secondary education (OR=0.228, 95%CI= -2.915 to -0.046). Regarding maternal age, women aged 25 or older had a 50.6% reduced chance of seeking prenatal care in the first twelve weeks of gestation compared to those who were younger (OR=0.506, 95%CI= -1.369 to 0.006). As for pregnancy planning, women who reported not having planned their pregnancy had a 45.1% reduced chance of complying with the recommended period for prenatal care compared to those who had planned their pregnancy (OR=0.451, 95%CI= -1.485 to -0.106) (Table 3).
DiscussionConcerning factors associated with late seeking of initiation of prenatal care, the present study identified diverse socioeconomic, sociodemographic and obstetric factors.
The educational attainment variable showed a positive association between having no education and late initiation of prenatal care, which suggests that women who reported having only the primary education were less likely to complete the recommended period of prenatal care compared to those who had completed high school. Analyzing the context of the study area, with an illiteracy rate of 70%, we can conclude that educational attainment negatively influences the access to health services. This also explains the refusal of some women to participate in the study, who claimed lack of time. These results were similar to those found in studies conducted in Ghana in 2018,
19 which observed that women with secondary and higher education were less likely to postpone their first prenatal appointment than women without formal education. This may be due to differences in comprehension levels and awareness of the negative effects of delaying prenatal appointments among women with varying levels of education. In other words, educated women are likely to be more appreciative or knowledgeable of the problems associated with delaying their first prenatal consultation than those who have not received formal education.
20 Therefore, education allows women to develop the necessary confidence to make decisions about their health and more easily understand the importance of prenatal services. Moreover, a higher level of education is generally linked to greater autonomy in the decision to seek prenatal care.
This finding is corroborated by Goudard's study,
20 which also identified that pregnant women with a lower level of education are more likely to initiate prenatal care late. These results were also observed in other studies,
21,22 which indicated that women with higher levels of education are better able to identify signs of complications during pregnancy and tend to practice healthy eating habits to avoid risks to themselves and their babies. Therefore, education influences both the utilization of health services and the completion of prenatal care at the Lugela health center.
Regarding family planning, the study showed that women who reported their pregnancy was unplanned were about 55.9% less likely to receive the recommended number of prenatal care visits compared to those who had planned their pregnancy. This scenario is likely because women discovered their pregnancy late, combined with a lack of a joint family planning culture or even a fear of telling their partners about the birth of a child. This aligns with what some oral sources at the study site reported: the number of children a couple should have is planned by the man, and the woman simply obeys. These findings are consistent with several studies, such as the research on 870 pregnant women conducted by Cruz-Bendezú
21 in the USA. This author and their collaborators found that women with unplanned pregnancies were more likely to detect their pregnancy later, which may also be due to the fact that the pregnant woman dedicates less attention and affection to this pregnancy. Furthermore, a woman with an unwanted pregnancy may not seek appropriate care and may be unwilling to obtain any prenatal information from health professionals.
23,24,25Intimate partner violence during pregnancy is an important factor that can influence maternal and child health, including delayed access to prenatal care, as highlighted in a recent systematic review. This relationship underscores the need to address gender-based violence as an integral part of maternal and child health care.
26 For the study site, policies and programs are in place to protect women and children, including a law against domestic violence, a program for the prevention of and response to violence against women and children, and economic empowerment initiatives designed to strengthen women financially.
Our analysis of the marital status variable revealed that 66.7% of the respondents who reported not having a partner at the time of the survey initiated prenatal care late. This is likely because single pregnant women take longer to come to terms with their pregnancy due to a lack of partner support. They may also feel apprehensive about attending their first prenatal care visit without a partner, unlike married women or those with partners who are often accompanied by their partners on their first visit to the healthcare facility. These findings are consistent with a study by Rurangirwa,
23 which reports that pregnant women who did not live with a partner had a higher frequency of inadequate prenatal care utilization.
19,24 Some studies also report that single women have a three times higher risk of not receiving prenatal care when compared to married women. A hypothesis for this finding could be related to partner support during pregnancy.
27In the analysis of socioeconomic variables, it was observed that 33.2% of the respondents earned less than three minimum wages, and of these, 70.6% initiated prenatal care outside the recommended period. The context of the study site is critical to these findings. The population must travel a minimum of 11 km to reach a healthcare facility, and these long distances, combined with a lack of public transportation and difficult access roads, are significant barriers. Consequently, pregnant women often do not have enough money for the main mode of transport in the area - motorcycle taxis - which contributes to their delayed seeking of prenatal care. These findings are consistent with studies by other authors who have shown that the quality of prenatal care is affected by income, as low-income pregnant women initiate care late and, consequently, have fewer consultations.
28,29 Therefore, the likelihood of receiving prenatal care within the recommended period was greater among women with higher incomes than among those with low incomes.
While there are numerous policies and initiatives aimed at reducing gender inequality, it is important to note that most of them focus on empowering women. Although there are also broader efforts to promote gender equality, men and boys also benefit from specific policies, especially in patriarchal contexts. The action plan for gender equality, education programs, and civil society initiatives are key policies that seek to address the cultural and social norms that perpetuate patriarchy.
30The research had several limitations, including communication difficulties with the eligible group due to a lack of fluency in the local language; the refusal of some women to participate, citing lack of time; and the poor condition of prenatal records, which hindered the proper visualization of variables.
The findings of this study led to the conclusion that factors associated with the late seeking of prenatal care are sociodemographic, obstetric and socioeconomic in nature. The study found that having only a primary-level education or no formal education, being 25 years of age or older, and having an unplanned pregnancy were all associated with the late seeking of prenatal care. Therefore, paying special attention to this group may reduce delays in the prenatal visit. Having completed high school or higher education, the presence of a partner in prenatal consultations, and a planned pregnancy all increase the likelihood of receiving the first prenatal consultation within the recommended period.
The identified factors for the irregular use of prenatal care services imply that the engagement of other government sectors, beyond the Ministry of Health, is pertinent and indispensable for improving health indicators.
References1. Organização Mundial da Saúde (OMS). Recomendações da OMS sobre cuidados pré-natais para uma experiência positiva na gravidez. Geneva: OMS; 2016. [access in 2024 Abr 6]. Available from:
https://iris.who.int/bitstream/handle/10665/250800/WHO-RHR-16.12-por.pdf2. Lira ES, Almeida JS. A importância da consulta de enfermagem no pré-natal nas unidades básicas de saúde. Rev JRG Estud Acad. 2024; 7 (15): e151716.
3. Reis-Muleva B, Duarte LS, Silva CM, Gouveia LMR, Borges ALV. Assistência ao pré-natal em Moçambique: número de consultas e idade gestacional no início do pré-natal. Rev Latino-Am Enf. 2021; 29: e3481.
4. Luz LAD, Aquino R, Medina MG. Avaliação da qualidade da atenção pré-natal no Brasil. Saúde Debate. 2018; 42: 111-26.
5. Livramento DVP, Backes MTS, Damiani PR, Castillo LDR, Backes DS, Simão MAS. Percepções de gestantes a cerca do cuidado pré-natal na atenção primária à saúde. Rev Gaúcha Enferm. 2019; 40: e20180211.
6. Gadelha CAG. Programa Nacional de Imunizações: o desafio do acesso universal no Século XXI. Ciênc Saúde Colet. 2020; 25: 4234-34.
7. World Health Organization (WHO). Committing to implementation of the Global Strategy for Women's, Children's and Adolescents' Health (2016–2030). [
Internet]. Geneva: WHO; 2023. [access in 2023 Abr 6]. Available from:
https://www.who.int/publications/i/item/WHO-UHL-MCA-GS-23.018. Trevisanuto D, Marchetto L, Arnilda G, Chien TD, Lincetto O, et al. Neonatal resuscitation in Vietnam: a national survey of a middle‐income country. Acta Paediatr. 2015; 104 (6): 255-62.
9. Ministério de Saúde (MISAU - Moçambique). Relatório Anual de Balanço do Setor da Saúde. Maputo: MISAU; 2021.
10. Instituto Nacional de Estatística (INE) e ICF. Inquérito Demográfico e de Saúde em Moçambique 2022–2023. Maputo (MZ): INE; 2023. [access in 2023 Abr 6]. Available from:
https://www.dhsprogram.com/publications/publication-FR389-DHS-Final-Reports.cfmLink de acesso11. Direcção Provincial de Saúde da Zambézia. Relatório Anual 2021. Zambézia (MZ); 2021. [access in 2023 Abr 6]. Available from:
https://drive.google.com/drive/folders/150DKcecD5_GF8wwp4aSt3F7slSEsPVXB?usp=sharing12. Serviços Distrital de Saúde da Mulher e Ação Social de Lugela (SDSMAS). Relatório anual 2021-2020. Lugela (MZ); 2021.
13. Bonzela J, Sitoe S, Amaro F, Menete D, Pombal F, Thompson R. Determinantes de seguimento pré-natal em área rual do sul de Moçambique: resultados preliminares do sistema de vigilância demográfica de saúde Chókwè (CHDSS), 2016-2018. Rev Moçambicana Ciên Saúde. 2018; 4 (Esp.): 276 (Resumo). Disponível em:
https://ins.gov.mz/wp-content/uploads/2020/10/RMCS-V4N2.pdf14. Culuza JB, Sousa HFA. Manual Prático do Sistema de Informação de Saúde, Monitoria & Avaliação e Planificação em Saúde. Zambézia, Moçambique; 2020. [access in 2023 Abr 6]. Available from:
https://pt.scribd.com/document/600610355/Manual-SIS-M-A-indicadores15. Instituto Nacional de Estatística (INE). IV Recenseamento geral da população e habitação 2017: resultados definitivos. Maputo, Moçambique: INE; 2018. [access in 2023 Abr 6]. Available from:
http://www.ine.gov.mz/iv-rgph-2017/mocambique/censo-2017-brochura-dos-resultados-definitivos-do-iv-rgph-nacional.pdf16. Azevedo PRM. Introdução à estatística [
Internet] / Paulo Roberto Medeiros de Azevedo. 3
a ed. Natal (RN): EDUFRN; 2016. [access in 2023 Abr 6]. E-book Available from:
https://repositorio.ufrn.br/items/277937e1-5de9-4e1e-81b6-a06bcadc7d9017. Moura AR. Critérios de seleção de modelos: um estudo comparativo [dissertação]. UFPB; 2021. [access in 2023 Abr 6]. Available from:
https://repositorio.ufpb.br/jspui/handle/123456789/2300718. Gonzalez LD. Regressao Logistica e suas Aplicações. São Luís: Brasil; 2018.
19. Ziblim SD, Yidana A, Mohammed AR. Determinants of Antenatal Care Utilization among Adolescent Mothers in the Yendi Municipality of Northern Region, Ghana. Ghana J Geogr. 2018; 10 (1): 78-97.
20. Goudard MJF, Simões VMF, Batista RFL, Queiroz RCS, Brito e Alves MTSS, Coimbra LC,
et al. Inadequação do conteúdo da assistência pré-natal e fatores associados em uma coorte no nordeste brasileiro. Ciênc Saúde Colet. 2016; 21: 1227-38.
21. Cruz-Bendezú AM, Lovell GV, Roche B, Perkins M, Blake-Lamb TL, Taveras EM,
et al. Psychosocial status and prenatal care of unintended pregnancies among low-income women. BMC Pregnancy Childbirth. 2020; 20: 615.
22. Teshale AB, Tesema GA. Determinants of births protected against neonatal tetanus in Ethiopia: A multilevel analysis using EDHS 2016 data. PLoS ONE. 2020, 15 (12): e0243071.
23. Rurangirwa AA, Mogren I, Nyirazinyoye L, Ntaganira J, Krantz G. Determinants of poor utilization of antenatal care services among recently delivered women in Rwanda; a population based study. BMC Pregnancy Childbirth. 2017: 17 (142): 1-10.
24. Dantas DS, Mendes RB, Santos JMJ, Valença TS, Mahl C, Barreiro MSC. Qualidade da assistência pré-natal no Sistema Único de Saúde. Rev Enferm UFPE on line. 2018; 12 (5): 1365-71.
25. Nascimento JWA, Barbosa LMS, Lima SSHS, Lucena ML, Andrade DVS. Principais fatores associados ao tardiamento do pré-natal: uma revisão sistemática. Braz J Health Rev. 2021; 4 (6): 28273-86.
26. Pastor-Moreno G, Ruiz-Perez I, Henares-Montiel J, Escribà-Agüir V, Higueras-Callejón C, Ricci-Cabello I. Intimate partner violence and perinatal health: a systematic review. BJOG. 2020; 127 (5): 537-47.
27. Nemer CRB, Santos ISR, Ferreira LD, Silva EV, Souza Filho ZA, Lima EQ,
et al. Fatores associados à inadequação do iníciodo pré-natal. Enferm Foco. 2021; 12 (4): 710-7.
28. Fagbamigbe AFF, Idemudia ES. Barriers to antenatal care use in Nigeria: evidences. BMC Pregnancy and Childbirth. 2015; 15: 95.
29. Adewuyi EO, Auta A, Khanal V, Bamidele OD, Akuoko CP, Adefemi K, et al. Prevalence and factors associated with underutilization of antenatal care services in Nigeria: A comparative study of rural and urban residences based on the 2013 Nigeria demographic and health survey. PloS one. 2018; 13 (5): e0197324.
30. Ministério do Trabalho (MZ). Género e Acção Social. Política de género e estratégia da sua implementação. Maputo, Moçambique; 2018. [access in 2023 Abr 6]. Available from:
https://forumulher.org.mz/wp-content/uploads/2018/09/POLITICA-DE-GENERO-e-Estrategia-Implementacao-APROVADA-CM-11.09.2018ooo.pdfAuthors' contributionMutequeta N e Germano Pires: conceptualization and study design, supervision of data collection, data analysis, manuscript writing. Cambe MI e Muamine E: study design, supervision of data collection, data analysis, manuscript writing. All authors approved the final version of the article and declared no conflicts of interest.
Data availabilityAll datasets supporting the results of this study are included in the article.
Received on November 3, 2024
Final version presented on August 19, 2025
Approved on August 21, 2025
Associated Editor: Karla Bomfim


 ; Maria Isabel Cambe2
; Maria Isabel Cambe2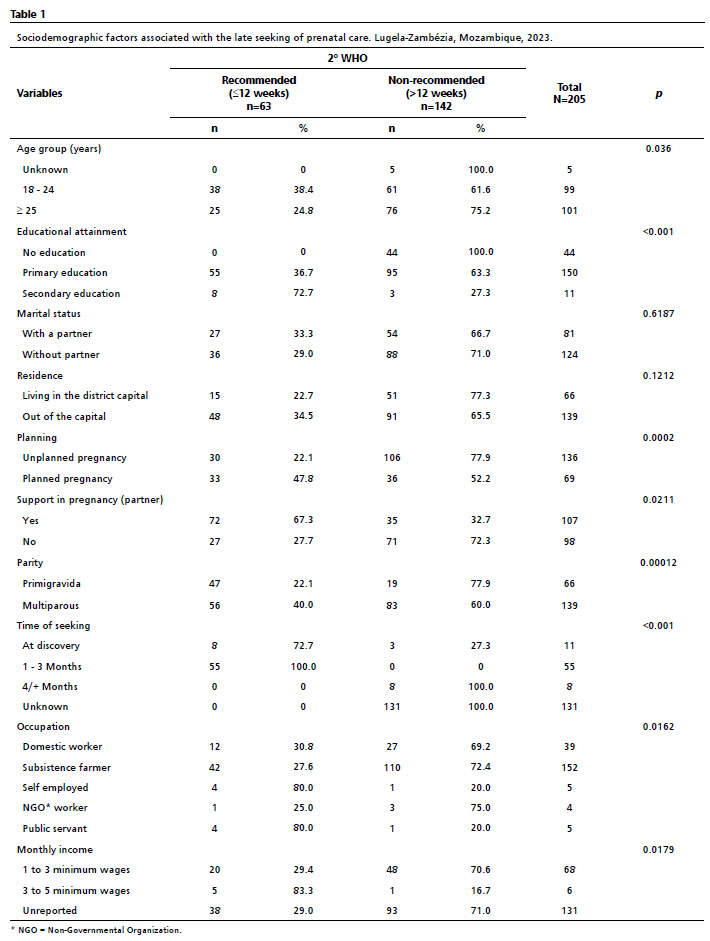






 Ler em português
Ler em português