ABSTRACT
Hypertensive disorders of pregnancy remain among the leading causes of morbidity and mortality worldwide, with a disproportionate impact on low- and middle-income countries. In recent decades, calcium supplementation has been widely promoted as a simple and potentially effective intervention to prevent preeclampsia, supported by small clinical trials, Cochrane systematic reviews, and World Health Organization recommendations, which facilitated its incorporation into clinical guidelines and public policies. However, the 2025 update of the Cochrane review published in 2025 redefined this understanding. By restricting the analysis to trustworthy trials, requiring prospective registration, and exploring the impact of small-study effects, the novel review concludes that, in the global analysis, calcium supplementation may result in little or no difference in preeclampsia incidence (low certainty). Furthermore, when the analysis is restricted to large-scale trials with greater methodological robustness, there is high-certainty evidence of little or no difference in the incidence of preeclampsia or preterm birth. Consistent reductions were also not demonstrated in maternal mortality, severe maternal morbidity, or major adverse perinatal outcomes. This article critically reviews the trajectory of calcium as a preventive strategy, discusses the implications of the 2025 Cochrane review guidelines and clinical practice, and contrasts its role with low-dose aspirin, which is supported by more robust evidence.
Keywords:
Preeclampsia, Gestational hypertension, Calcium, Aspirin, Evidence-based medicine
RESUMO
Os distúrbios hipertensivos da gestação permanecem entre as principais causas de morbidade e mortalidade materna no mundo, com impacto desproporcional em países de baixa e média renda. Nas últimas décadas, a suplementação de cálcio foi amplamente promovida como intervenção simples e potencialmente eficaz para prevenir a pré-eclâmpsia, sustentada por ensaios clínicos pequenos, revisões sistemáticas da Cochrane e recomendações da Organização Mundial da Saúde, o que favoreceu sua incorporação em diretrizes clínicas e políticas públicas. Entretanto, a atualização da revisão Cochrane publicada em 2025 redefiniu esse entendimento. Ao restringir a análise a ensaios considerados confiáveis, exigir registro prospectivo e explorar o impacto de estudos pequenos, a nova revisão conclui que, na análise global, a suplementação de cálcio pode resultar em pouca ou nenhuma diferença na incidência de pré-eclâmpsia (certeza baixa), e que, quando a análise é restrita a ensaios de grande porte e maior robustez metodológica, há evidência de alta certeza de pouca ou nenhuma diferença na incidência de pré-eclâmpsia e de parto pré-termo. Também não se demonstraram reduções consistentes na mortalidade materna, na morbidade materna grave ou nos principais desfechos perinatais adversos. Este artigo revisa criticamente a trajetória do cálcio como estratégia preventiva, discute as implicações da revisão Cochrane de 2025 para diretrizes e práticas clínicas e contrasta seu papel com o da aspirina em baixa dose, sustentada por evidência mais robusta.
Palavras-chave:
Pré-eclâmpsia, Hipertensão gestacional, Cálcio, Aspirina, Medicina baseada em evidências
IntroductionPreeclampsia and other hypertensive disorders of pregnancy remain responsible for a substantial proportion of maternal deaths and intensive care unit (ICU) admissions, in addition to contributing significantly for prematurity, fetal growth restriction, and perinatal mortality.
1 In settings marked by inequities in access to prenatal care, social inequality, and a high burden of comorbidities, any low-cost intervention, with apparent safety and biological plausibility tends to be rapidly incorporated by clinicians, policymakers, and researchers.
Calcium supplementation aligns perfectly with this context. Epidemiological observations associating low dairy intake with an increase in gestational hypertension, experimental studies suggesting the effects of calcium on parathyroid hormone, the renin-angiotensin system, and vascular tone, as well as early clinical trials pointing to significant reductions in the incidence of preeclampsia, fueled for years the idea that it was a simple intervention capable of substantially modifying the risk of severe disease.
2,3Since 2002, successive Cochrane systematic reviews have synthetized these findings and reinforced confidence in calcium as a preventive strategy.
2,3 The 2018 update included dozens of trials, many of them small-scale, and concluded that calcium supplementation, particularly in doses equal to or greater than 1,000mg/day, reduced the risk of preeclampsia, with more pronounced effects in women with low dietary intake and in high-risk groups.
2 In parallel, another Cochrane review suggested potential additional benefits for preterm delivery and some perinatal outcomes, albeit with higher uncertainty.
4These syntheses supported international recommendations. In 2013, the World Health Organization (WHO) recommended, for populations with low calcium intake, the daily supplementation of 1.5 to 2.0 g of elemental calcium, preferentially initiated from the 20th week of pregnancy, with the explicit objective of reducing the occurrence of preeclampsia.
5 Subsequent recommendations reinforced this guidance and expanded its scope, including supplementation prior to pregnancy in women with a previous history of the disease.
6,7Against this backdrop, in early 2025, we published a narrative review advocating that the use of calcium during pregnancy went beyond preeclampsia prevention, highlighting potential additional benefits.
1 A few months later, however, the new 2025 Cochrane update delivered a substantially different message by critically reassessing the trustworthiness of the available trials, introduced more stringent methodological criteria, and redefined the balance between benefit and uncertainty.
8From biological plausibility to clinical enthusiasmFrom a biological standpoint, the hypothesis that calcium could reduce the risk of preeclampsia has always appeared seductive. Calcium plays a role in vascular smooth muscle contraction, neurotransmitter and hormone release, and the regulation of parathyroid hormone and the renin-angiotensin-aldosterone system. Observational studies suggested that higher calcium intake was associated with lower blood pressure levels and a lower incidence of hypertension. It was plausible to assume that, in pregnant women with low dietary intake, calcium supplementation would attenuate the vasoconstrictor response, stabilize endothelial function, and modulate vascular reactivity amid the hemodynamic challenges of pregnancy.
Randomized clinical trials conducted since the 1980s and 1990s seemed to confirm this expectation. Many were small, single-center studies, conducted in low-income populations with insufficient baseline calcium intake. Nevertheless, the results were compelling, with reductions in preeclampsia risk on the order of 50% or more in some studies, alongside a decrease in gestational hypertension and, in certain analyses, favorable trends regarding preterm birth and composite outcomes of severe maternal morbidity.
2,4Early Cochrane reviews captured this narrative. The 2002 version concluded that calcium supplementation appeared beneficial, particularly for high-risk women and in low-intake settings.
3 With each update, new small trials were added, and the pooled effect estimate remained favorable. In 2018, despite acknowledging heterogeneity and potential biases, the authors still summarized the evidence as consistent with a clinically relevant reduction in preeclampsia and, possibly, preterm birth.
2,4This combination of biological plausibility, striking early results, and optimistic systematic syntheses provided the basis for emphatic guidelines. The WHO began recommending high doses of calcium for pregnant women in low-intake populations, and several national guidelines incorporated this recommendation as a public health best practice.
5,6,9,10The 2025 Cochrane review: what does it really conclude?The Cochrane review published in December 2025 represents an inflection point in the history of calcium in pregnancy.
8 Although it maintains the same objective as previous versions—to evaluate whether calcium supplementation reduces hypertensive disorders of pregnancy and improves maternal and perinatal outcomes—the methodological approach adopted was substantially different.
Ten randomized clinical trials were included, totaling 37,504 pregnant women. Eight studies compared calcium with placebo or standard care, and two compared low doses (500 mg/day) with high doses (1,500 mg/day).
8 Compared to previous reviews, 20 trials were excluded: 11 for failing to meet updated eligibility criteria, including the requirement for prospective registration for studies conducted after 2010, and nine for being considered untrustworthy in light of explicit data integrity and reliability criteria.
8In an unprecedented move within the Cochrane Pregnancy and Childbirth group, the authors applied the Trustworthiness in RAndomised Controlled Trials (TRACT) checklist to assess trial reliability, adding a layer of methodological scrutiny that was absent from previous reviews. The systematic application of TRACT, combined with the requirement for prospective registration, largely explains the refinement of the study set and the removal of trials that sustained the seemingly more exuberant effects of calcium supplementation.
As a result, the analytical focus shifted from numerous small trials to a more restricted set of robust studies, including two contemporary megatrials conducted in India and Tanzania, which compared doses of 500 mg and 1,500 mg of calcium in more than 22,000 pregnant women.
9 The review utilized the Cochrane Risk-of-Bias tool for randomized trials (RoB 2) to assess bias, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system to classify the certainty of evidence, and performed sensitivity analyses excluding studies with fewer than 500 participants, which are particularly susceptible to effect overestimation and publication bias.
8 This combination—RoB 2, TRACT, and GRADE—lends the 2025 review the character of a qualitative reinterpretation of the body of evidence, rather than a mere quantitative update.
The results are consistent. Considering all studies included in the primary analysis, calcium supplementation may result in little or no difference in the occurrence of preeclampsia (RR=0.83; 95%CI=0.67–1.04; low certainty), as well as in perinatal loss, with very uncertain evidence regarding preterm birth before 37 weeks and maternal death.
8 When the analysis is restricted to trials with more than 500 participants, the effect disappears: in four large studies involving 14,730 women, the risk of preeclampsia is virtually identical between the calcium and placebo groups (RR=0.92; 95%CI=0.79–1.05), with the certainty of evidence classified as high.
8 This distinction between the global analysis and the analysis restricted to larger trials is fundamental for the correct interpretation of the certainty level according to the GRADE system, as the classification reflects not only the direction of the effect but also the methodological robustness and trustworthiness of the studies supporting the estimate. Similar findings are observed for gestational hypertension and major perinatal outcomes, with estimates consistently close to the null and higher certainty of evidence in large-scale trials.
8The same logic applies to preterm birth. Although the global analysis is marked by uncertainty, the sensitivity analysis restricted to large trials indicates little or no difference in the proportion of births before 37 weeks.
8 For the composite outcome of maternal death or severe maternal morbidity, the evidence is of moderate certainty and points to little or no benefit, while isolated events of maternal death are too rare to allow for robust conclusions.
8 Regarding HELLP syndrome, the scarcity of events results in low or very low-certainty evidence, with wide confidence intervals that encompass both potential benefit and harm.
These findings were summarized in a table presenting the main maternal and perinatal outcomes—including preeclampsia, gestational hypertension, maternal death, death and severe maternal morbidity, HELLP syndrome, stillbirth, neonatal death, and perinatal loss—with their respective relative risks, 95% confidence intervals, and GRADE classifications, accompanied by comments explaining the factors determining the certainty of evidence (Table 1).
8 No modification of effect was observed according to baseline calcium intake or risk status for preeclampsia. Women with low dietary intake did not benefit more than those with adequate intake, and high-risk women did not present superior benefits to those observed in low-risk pregnant women.
8 This homogeneity of effect across subgroups, associated with the stability of estimates in large and trustworthy trials, reinforces the absence of "niches" in which calcium exerts a relevant preventive impact on hypertensive disorders of pregnancy.
The two large trials conducted by Dwarkanath et al.
9 corroborate this scenario. In both, the 500 mg/day dose proved non-inferior to the 1,500 mg/day dose for preeclampsia and preterm birth, suggesting that if any effect of calcium exists, it is independent of high doses and, at best, modest.
9 These megatrials also provide the foundation for the main forest plots of the review, in which the statistical weight is concentrated on estimates close to the null.
In summary, the authors' interpretation is unequivocal: when restricted to trials with more than 500 participants and higher methodological reliability, there is high-certainty evidence that calcium supplementation initiated between five and 26 weeks of pregnancy results in little or no difference in the incidence of preeclampsia and preterm birth, as well as little or no effect on maternal death, severe maternal morbidity, perinatal loss, and stillbirth.
8Guidelines in transition and the gap between evidence and policyIf the new Cochrane review so forcefully weakens the hypothesis of calcium's benefits in preventing preeclampsia, why do guidelines still recommend its supplementation? The answer lies, in part, in the inherent inertia of the processes for developing and updating health recommendations.
World Health Organization (WHO) guidelines on calcium during pregnancy, published in 2013 and reaffirmed in subsequent documents, were based primarily on earlier versions of the Cochrane review, in which results from small trials were combined with those from larger studies.
2,5,6,10 In those analyses, the apparent effect of supplementation was substantial, with preeclampsia risk reductions on the order of 50% in populations with low calcium intake, alongside potential additional benefits for preterm birth and certain neonatal outcomes.
2 In light of this evidence, it is understandable that the WHO issued strong recommendations in favor of supplementation, especially in contexts of nutritional deficiency.
In 2020, the WHO also published a specific recommendation on calcium supplementation before and in early pregnancy, based on a multicenter trial that evaluated women with a prior history of preeclampsia.
7 Although it already acknowledged uncertainties regarding some outcomes, the document still positioned calcium as a promising intervention along the preconception-pregnancy continuum.
Specialized scientific societies followed similar logic. The International Society for the Study of Hypertension in Pregnancy (ISSHP) guideline, for example, recommends calcium supplementation for women with low dietary intake (<800 mg/day), although it classifies this as a weak recommendation based on low-certainty evidence.
10 In many countries, especially low-income ones, this recommendation was uncritically incorporated into prenatal care routines.
In Brazil, the recommendations of the Brazilian Network for the Study of Hypertension in Pregnancy (RBEHG) well illustrate this transitional moment. The most recent care protocol, published in 2025, maintains the indication of low-dose aspirin for pregnant women with one high-risk factor or two moderate-risk factors for preeclampsia and, simultaneously, recommends universal calcium supplementation, along with lifestyle guidance.
11 It is a technically consistent document grounded in the best evidence available at the time; however, it evidences the inevitable discrepancy between carefully crafted national guidelines and systematic reviews that, years later, reevaluate with greater critical rigor the same studies that originated them.
It is important to recognize that this entire regulatory framework was constructed before the 2025 Cochrane update, which makes the persistent enthusiasm for supplementation understandable, even in the face of the substantial shift in the balance between benefit and uncertainty brought about by the new synthesis.
8The 2025 review prompts a critical reevaluation of these guidelines in light of the new evidence synthesis.
8 Updating them, however, takes time: it requires a formal reassessment of the evidence, coordination among specialist groups, and consideration of aspects such as equity, costs, and feasibility, which are often permeated by political implications. Until this process is complete, an uncomfortable scenario remains: on one hand, current guidelines still recommending calcium; on the other, a robust systematic review pointing to an absence of clinically relevant benefit. In this context, it is fundamental to make this gap explicit and recognize that maintaining calcium prescription as a preventive strategy for preeclampsia—without informing that the best evidence currently available does not confirm this effect—represents a subtle, yet relevant, form of outdated clinical practice.
What really works in preeclampsia prevention?Questioning the role of calcium as a preventive intervention does not mean that effective strategies to prevent preeclampsia do not exist. On the contrary, over the last two decades, a much more robust body of evidence has been established, in favor of using low-dose aspirin in high-risk pregnant women.
Clinical trials and meta-analyses have demonstrated that aspirin—especially when initiated early between 12 and 16 weeks of pregnancy, in doses between 100 and 150 mg/day—significantly reduces the risk of preeclampsia, preterm birth, and composite outcomes of perinatal morbidity and mortality.
6 The absolute effect depends on baseline risk but is consistently superior to the effect observed with calcium.
In 2021, the U.S. Preventive Services Task Force (USPSTF) updated its recommendation, reinforcing the use of 81 mg/day starting at the 12th week for pregnant women at high risk of preeclampsia, based on evidence of reduced maternal and perinatal outcomes without an increase in severe hemorrhagic events.
12,13 The Journal of the American Medical Association (JAMA) also concluded that low-dose aspirin significantly reduces preeclampsia, fetal growth restriction, and perinatal loss in at-risk populations, with an excellent safety profile.
6The American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM) recommend the routine use of 81 mg/day of aspirin between 12 and 28 weeks—ideally initiated by 16 weeks—in women at high risk (prior preeclampsia, multiple gestation, chronic hypertension, or pre-gestational diabetes) or with multiple moderate risk factors.
13,14 The ISSHP also endorses this strategy.
10In summary, if we seek a pharmacological intervention capable of consistently reducing the incidence of preeclampsia and improving perinatal outcomes, aspirin offers evidence of greater magnitude and higher certainty compared to calcium supplementation for this specific outcome. Furthermore, non-pharmacological strategies—such as rigorous control of chronic hypertension, preconception management of obesity and diabetes, reproductive planning, reduction of iatrogenic multiple pregnancies, and strengthening high-quality prenatal care—remain fundamental, and are likely responsible for a significant portion of the reduction in hypertensive complications observed in high-income countries.
Repositioning calcium: from preventive drug to essential nutrientRecognizing that calcium does fulfill the role of an "anti-preeclampsia" agent does not mean dismissing it from clinical practice. Calcium remains an essential nutrient, with a relevant impact on maternal bone health, fetal mineralization, and possibly, to long-term metabolic programming. In populations with very low dietary intake, pregnancy may exacerbate bone mass loss, with implications that extend beyond the pregnancy-postpartum cycle.
The literature that supported WHO guidelines highlights that the original rationale for supplementation was to fill a nutritional gap, not to treat the pathophysiology of preeclampsia.
5,6,10 Clinical trials and cohort studies suggest that supplementation reduces bone resorption during pregnancy and in the immediate postpartum period, although effects on long-term fractures are difficult to demonstrate. Exploratory data also indicate benefits for outcomes such as childhood blood pressure and dental health, but these associations still require further confirmation.
What the 2025 Cochrane review clearly does is separate these issues: it is one thing to recognize calcium as an important nutrient whose deficiency should be addressed through food policies and supplementation; it is quite another to treat it as a pharmacological intervention for preventing preeclampsia and preterm birth—a question for which the best answer is now negative.
8In contexts such as Brazil's, it may be more appropriate to reposition calcium as part of an agenda for nutritional security and health equity, rather than maintaining it as a preventive medication for hypertensive disorders of pregnancy. This does not mean abandoning supplementation programs where deficiency is prevalent, but rather reorienting their justification and expectations until new evidence emerges.
Methodological lessons and the research agendaThe 2025 Cochrane review offers significant methodological lessons that extend far beyond the topic of calcium. By including trials that were not prospectively registered and studies considered untrustworthy, the authors address rising concerns about the integrity of biomedical literature – concerns widely discussed in recent analyses on non-reproducible or potentially fraudulent clinical trials.
15 By explicitly exploring the impact of small-scale studies and discussing publication bias, the review reinforces the importance of going beyond statistical significance and the mere counting of trials.
The definition of a "small-scale study" as one with fewer than 500 participants, along with sensitivity analyses excluding this group, proved particularly enlightening.
8 Many of the exuberant estimates of calcium's benefit originated precisely from these smaller studies; when they are excluded, the apparent efficacy vanishes. This finding reinforces the need for caution regarding highly positive results derived from small samples, especially in contexts of heterogeneity and risk of bias.
Another relevant aspect is the review's indirect dialogue with recent criticisms of the literature on calcium meta-analyses. Wright and colleagues had already questioned, in 2024, the robustness of conclusions favoring supplementation, pointing out methodological limitations and inconsistencies between small and large studies.
16 The new Cochrane review can be seen as the operationalization of these criticisms within a methodologically more demanding synthesis.
8,16From the perspective of the research agenda, the message is clear: it is unlikely that new clinical trials of calcium in pregnancy, with designs similar to those already conducted, will substantially modify current conclusions.
8 It seems more rational to direct resources and efforts toward other issues, such as optimizing aspirin use (dose, timing of initiation, and strategies to improve adherence), refining risk stratification models based on clinical, ultrasound, and laboratory data, and integrating pharmacological and non-pharmacological interventions into viable prenatal care models within the Brazilian Unified Health System (SUS).
There is still room for research on calcium, but likely within specific niches, such as adolescents with severe nutritional deficiencies, women exposed to heavy metals stored in bone, and contexts of extreme food insecurity. In these scenarios, the question is no longer whether calcium prevents preeclampsia, but rather what its role is in protecting maternal-infant bone and metabolic health—distinct questions that demand equally distinct study designs and outcomes.
Final considerationsWhen we advocated, in 2025, that the use of calcium during pregnancy went beyond the prevention of preeclampsia, we were aligned with the systematic reviews and international guidelines then available.
1,2,5-7,10 In light of previous Cochrane meta-analyses, WHO documents, and scientific society recommendations, it was reasonable to consider calcium a simple, safe, and potentially transformative intervention, particularly in low-intake settings. It was not naïve enthusiasm, but rather an honest appraisal of the best evidence accessible at that time.
The 2025 Cochrane update, however, compels us to recognize that the current best interpretation of the evidence is different.
8 Calcium supplementation initiated between five and 26 weeks of gestation—at the doses and in the populations studied—may result in little to no difference in the incidence of preeclampsia when considering the global analysis (low certainty) and likely results in little to no difference when restricted to larger, more reliable trials (high certainty). If any benefit exists, it is modest and insufficient to sustain the enthusiasm with which calcium was promoted as a large-scale preventive intervention. By applying more rigorous criteria for reliability and prospective registration, and giving greater weight to large-scale studies, the new review demonstrates that the "robust effect" suggested by small trials does not hold when methodological rigor is tightened.
This does not diminish the importance of calcium as an essential nutrient, nor does it deny the need to address its deficiency as part of food and nutritional security policies. What is redefined is calcium's role in the strategy for managing hypertensive disorders of pregnancy, especially when compared to interventions with more consistent evidence, such as low-dose aspirin in high-risk pregnant women.
10-14 Calcium is no longer at the center of preeclampsia prevention; instead, it is more accurately understood as a marker of food equity, a support for bone health, and a potential modulator of long-term outcomes still under investigation. In contrast, aspirin is consolidated as the preventive drug with the best benefit-risk ratio for this specific outcome.
Changing positions in light of new evidence is not a sign of incoherence, but rather a commitment to the essence of evidence-based medicine. If the 2025 Cochrane review redefines the role of calcium, it is up to us to embrace this shift, updating not only protocols and recommendations, but also the readiness to abandon comfortable narratives when the data so demand. Fidelity to the scientific method implies accepting that evidence evolves, hypotheses can be weakened, and established consensus must, at times, be rewritten.
REFERENCES1. Amorim MMR, Albuquerque MA, Neves LFM, Bernardo BC, Cunha ACC, Katz L. Use of calcium during pregnancy: far beyond preeclampsia. Rev Bras Saúde Mater Infant. 2025; 25: e20240328.
2. Hofmeyr GJ, Lawrie TA, Atallah ÁN, Torloni MR. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst Rev. 2018;10 (10): CD001059. doi:10.1002/14651858.CD001059.pub5.
3. Atallah ÁN, Hofmeyr GJ, Duley L. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst Rev. 2002;(1):CD001059. doi: 10.1002/14651858.CD001059.
4. Kongwattanakul K, Duangkum C, Ngamjarus C, Lumbiganon P, Cuthbert A, Weeks J, et al. Calcium supplementation (other than for preventing or treating hypertension) for improving pregnancy and infant outcomes. Cochrane Database Syst Rev. 2024; 11 (11): CD007079. doi:10.1002/14651858.CD007079.pub4.
5. World Health Organization (WHO). Guideline: calcium supplementation in pregnant women. Geneva: WHO; 2013. [access in 2025 Nov 1]. Available from:
https://iris.who.int/server/api/core/bitstreams/af564486-d5ce-4b3f-adaf-8ee5ca0e70ca/content6. World Health Organization (WHO). WHO recommendation: calcium supplementation during pregnancy for the prevention of pre-eclampsia and its complications. Geneva: WHO; 2018. [Internet]. [access in 2025 Nov 1]. Available from:
https://www.who.int/publications/i/item/97892415504517. World Health Organization (WHO). WHO recommendation on calcium supplementation before pregnancy for the prevention of pre-eclampsia and its complications. Geneva: WHO; 2020. [Internet]. [access in 2025 Nov 1]. Available from:
https://www.who.int/publications/i/item/97892400031188. Cluver CA, Rohwer C, Rohwer AC. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst Rev. 2025; 12 (12): CD001059. doi: 10.1002/14651858.CD001059.pub6.
9. Dwarkanath P, Muhihi A, Sudfeld CR, et al. Two randomized trials of low-dose calcium supplementation in pregnancy. N Engl J Med. 2024; 390 (2): 143-53. doi:10.1056/NEJMoa2307212.
10. Magee LA, Brown MA, Hall DR, Gupte S, Hennessy A, Karumanch SA, et al. The 2021 International Society for the Study of Hypertension in Pregnancy classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2022; 27: 148-69. doi:10.1016/j.preghy.2021.09.008.
11. Korkes HA, Ramos JGL, Oliveira LG, Sass N, Peraçoli JC, Cavalli RC, et al. Pré-eclâmpsia: protocolo 2025. Rede Brasileira de Estudos sobre Hipertensão na Gravidez (RBEHG). 2025. [access in 2025 Nov 1]. Available from:
https://rbehg.com.br/wp-content/uploads/2025/04/Protocolo-RBEHG-2025-PDF-2.pdf12. Henderson JT, Vesco KK, Senger CA, Thomas RG, Redmond N. Aspirin use to prevent preeclampsia and related morbidity and mortality: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021; 326 (12): 1192-206. doi:10.1001/jama.2021.8551.
13. US Preventive Services Task Force; Davidson KW, Barry MJ, Mangione CM, Cabana M, Caughey AB, et al. Aspirin use to prevent preeclampsia and related morbidity and mortality: US Preventive Services Task Force recommendation statement. JAMA. 2021; 326 (12): 1186-91. doi:10.1001/jama.2021.14781.
14. American College of Obstetricians and Gynecologists (ACOG); Society for Maternal-Fetal Medicine. ACOG Committee Opinion Nº. 743: Low-dose aspirin use during pregnancy. Obstet Gynecol. 2018; 132 (1): e44-e52. doi:10.1097/AOG.0000000000002708.
15. Van Noorden R. Medicine is plagued by untrustworthy clinical trials. How many studies are faked or flawed? Nature. 2023; 619 (7970): 454-8. doi:10.1038/d41586-023-02299.
16. Wright D, Wright A, Magee LA, von Dadelszen P, Nicolaides KH. Calcium supplementation for the prevention of pre-eclampsia: challenging the evidence from meta-analyses. BJOG. 2024; 131 (11): 1524-9. doi:10.1111/1471-0528.17769.
Autho's contributionAmorim MMR: Conceptualization, methodology, investigation, writing – original draft, writing – review and editing, supervision.
Souza ASR: Conceptualization, methodology, formal analysis, writing – review and editing.
Albuquerque MA: Conceptualization, methodology, formal analysis, writing – review and editing.
Farias JLB: Investigation, writing – original draft.
Carvalho-Filho AFP: Investigation, writing – original draft.
Neves LFM: Investigation, writing – original draft.
Cunha ACC: Conceptualization, methodology, formal analysis, writing – review and editing.
Delgado A: Formal analysis.
Katz L: Conceptualization, methodology, formal analysis, writing – review and editing, supervision.
All authors approved the final version of the article and declare no conflicts of interest.
Data availabilityAll datasets supporting the results of this study are included in the article.
Received on December 16, 2025
Final version presented on February 18, 2026
Approved on February 20, 2026
Associated Editor: Lygia Vanderlei


 ; Alex Sandro Rolland Souza2,4,5
; Alex Sandro Rolland Souza2,4,5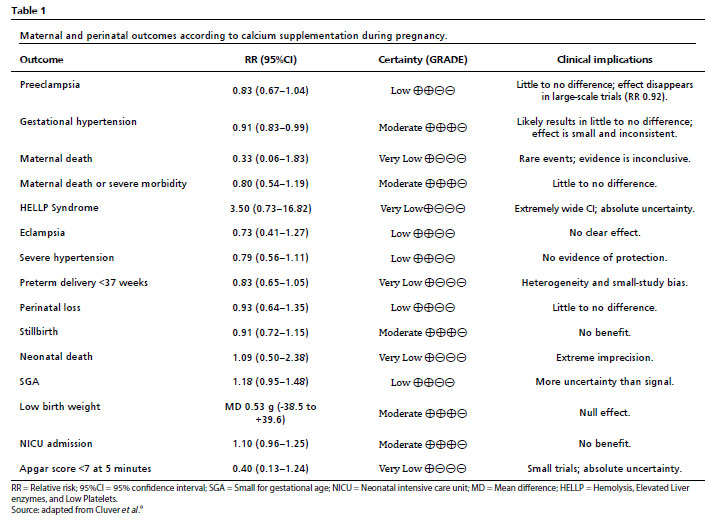






 Ler em português
Ler em português