ABSTRACT
OBJECTIVES: to assess the COVID-19 pandemic impact on breastfeeding rates during birth hospitalization in a Baby-Friendly certified perinatal hospital in Portugal.
METHODS: observational retrospective study comparing pre-pandemic (2019) and pandemic (April-December 2020) periods. A total of 900 healthy term mother-newborn dyads in rooming-in were included. Maternal and neonatal variables associated with breastfeeding at discharge were analyzed using chi-square, Student's t-test, and multivariable logistic regression (p<0.05).
RESULTS: breastfeeding rates were higher in the pandemic period (99.3%) than in the pre-pandemic period (97.6%; p=0.031). Exclusive breastfeeding (80.2% vs. 81.6%; p=0.611) and skin-to-skin contact (56.2% vs. 58.0%; p=0.590) did not differ significantly. Exclusive breastfeeding was associated with vaginal delivery (pre-pandemic OR=3.07; 95%CI=1.83-5.13; p<0.001; pandemic OR=2.29; 95%CI=1.39-3.77; p=0.001), weight loss <10% (p<0.001), and absence of phototherapy in the pre-pandemic period (OR=3.38; 95%CI=1.96-7.12; p<0.001). No associations were found with maternal age, parity, sex, or gestational age.
CONCLUSIONS: exclusive breastfeeding rates were not negatively affected by pandemic restrictions. Maintaining Baby-Friendly practices preserved essential breastfeeding support.
Keywords:
Breastfeeding, COVID-19 pandemic, Newborn
IntroductionThe COVID-19 pandemic, declared by the World Health Organization (WHO) on March 11, 2020,
1 profoundly affected healthcare systems and practices worldwide. The rapid need to implement infection control measures – such as social distancing, isolation, and the reorganization of hospital workflow – had potential implications for maternal and neonatal care. Among these, restrictions on companionship during labor, reduced postnatal support, and limitations on mother–newborn contact raised concerns about the establishment and maintenance of breastfeeding.
2Pregnant and postpartum women and their newborns are particularly vulnerable to disruptions in care. In the early months of the pandemic, uncertainty regarding SARS-CoV-2 transmission routes led to inconsistent recommendations on breastfeeding and rooming-in practices.
3,4 Initial concerns about possible vertical transmission prompted some hospitals, including in Portugal, in restricting skin-to-skin contact and temporarily separating mothers and infants.
5-8 As scientific evidence accumulated, it became clear that breastfeeding was safe and that COVID-19 transmission occurred mainly via respiratory droplets.
9-11 Consequently, international guidelines – led by WHO – were revised in favor of maintaining breastfeeding and early contact, provided that infection control measures were observed.
11Despite these clarifications, the pandemic context introduced emotional stress, reduced in-person support, and modified care routines that could negatively affect breastfeeding initiation and continuation.
12,13 Several studies worldwide reported heterogeneous effects, reflecting variability in hospital policies, resources, and adherence to Baby-Friendly practices.
5,6,14The Baby-Friendly Hospital Initiative (BFHI), launched by WHO and UNICEF in 1991, aims to protect, promote, and support breastfeeding through the implementation of ten evidence-based steps.
15 Hospitals adhering to these standards are recognized as Baby-Friendly. Our institution, certified since 2007, is committed to maintaining these practices through staff training and consistent breastfeeding support during hospitalization.
16Understanding how COVID-19 pandemic influenced breastfeeding within a Baby-Friendly environment is crucial, particularly in contexts where protective measures may have conflicted with breastfeeding promotion principles. Therefore, this study aimed to evaluate the impact of COVID-19 pandemic on breastfeeding rates during birth hospitalization in a Baby-Friendly certified perinatal hospital in Portugal.
MethodsThis was an observational, analytical, retrospective study based on clinical data from mother–newborn dyads whose births occurred during the pandemic period (April 1 to December 31, 2020) and the homologous pre-pandemic period in 2019. These months correspond to the phase of stricter restrictions and greater uncertainty regarding the impact of SARS-CoV-2 on maternal and neonatal health.
The hospital, located in central Portugal, recorded 2366 births in 2019 and 2354 in 2020. During the pandemic, rooming-in was maintained whenever possible, under strict infection control measures. Hospital discharge was generally at 48 hours of life for all healthy term newborns when clinical and social conditions were met; prior to the pandemic, discharge after cesarean section occurred at 72 hours.
Healthy term newborns in rooming-in from birth to discharge were included. Exclusion criteria were maternal conditions or medications contraindicating breastfeeding, confirmed SARS-CoV-2 infection, and declared intention not to breastfeed. Infection was ruled out through polymerase chain reaction testing on nasopharyngeal samples.
A structured convenience sample was used, including the first 50 eligible dyads per month between April and December in each period, totaling 450 dyads for both the pre-pandemic and pandemic groups. This sampling approach ensured representation across the study period and exposure to different healthcare teams.
The main outcome was the rate of breastfeeding and exclusive breastfeeding at hospital discharge. Exclusive breastfeeding was defined as feeding only with breast milk at discharge; breastfeeding included both exclusive and mixed feeding. The secondary outcome was the identification of maternal and neonatal factors associated with exclusive breastfeeding in each period.
Collected maternal and newborn variables included: maternal age, parity, gestational age, mode of delivery (vaginal or cesarean), skin-to-skin contact (≥30 minutes), newborn sex, birth weight (<2,500 g, 2,500–3,999 g, ≥4,000 g), weight loss during hospitalization (%), and complications such as hyperbilirubinemia requiring phototherapy.
Data were extracted from electronic medical records (SClínico
®) between September 2022 and March 2023 by trained neonatologists and pediatricians, and stored in a secure database.
Statistical analysis was performed using IBM SPSS Statistics (version 26). Categorical variables were expressed as absolute and relative frequencies; continuous variables as means and standard deviations or medians and interquartile ranges, according to distribution. Group comparisons (pandemic vs. pre-pandemic) were made using the chi-square test for categorical variables and Student’s t-test for continuous variables with normal distribution. A
p-value <0.05 was considered statistically significant.
To explore factors associated with exclusive breastfeeding, univariable and multivariable logistic regression analyses were performed, reporting adjusted odds ratios (OR) and 95% confidence intervals (CI). The final model included variables with statistical significance in univariable analysis and those previously reported in the literature to influence exclusive breastfeeding positively (skin-to-skin contact, multiparity) or negatively (significant weight loss, cesarean delivery). The adequacy of the model was verified using the Hosmer–Lemeshow and Omnibus tests.
The study was approved by the Ethics Committee of the
Unidade Local de Saúde de Coimbra, Portugal (PI OBS. SF.143-2022), in accordance with national ethical standards and the Declaration of Helsinki. Given the retrospective design and the use of anonymized medical record data, informed consent was waived. Confidentiality and anonymity of the participants were guaranteed.
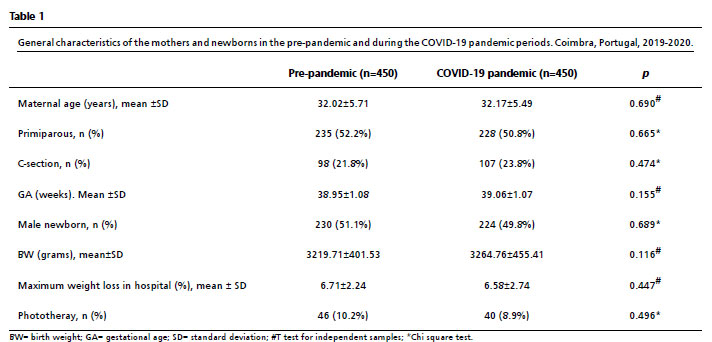
ResultsA total of 900 mother–newborn dyads were included, 450 in each period (pre-pandemic and pandemic). The number of full-term deliveries per month was similar over the periods.
There were no significant differences in baseline maternal or neonatal characteristics between groups (Table 1). The maximum weight loss during hospitalization was comparable in both periods.
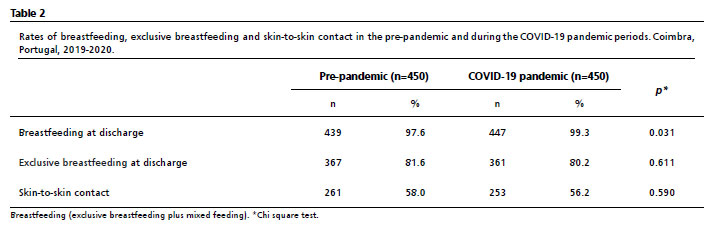
As shown in Table 2, the overall rate of breastfeeding at hospital discharge was significantly higher during the pandemic period compared with the pre-pandemic period (
p=0.031). However, exclusive breastfeeding and skin-to-skin contact rates did not differ between periods.
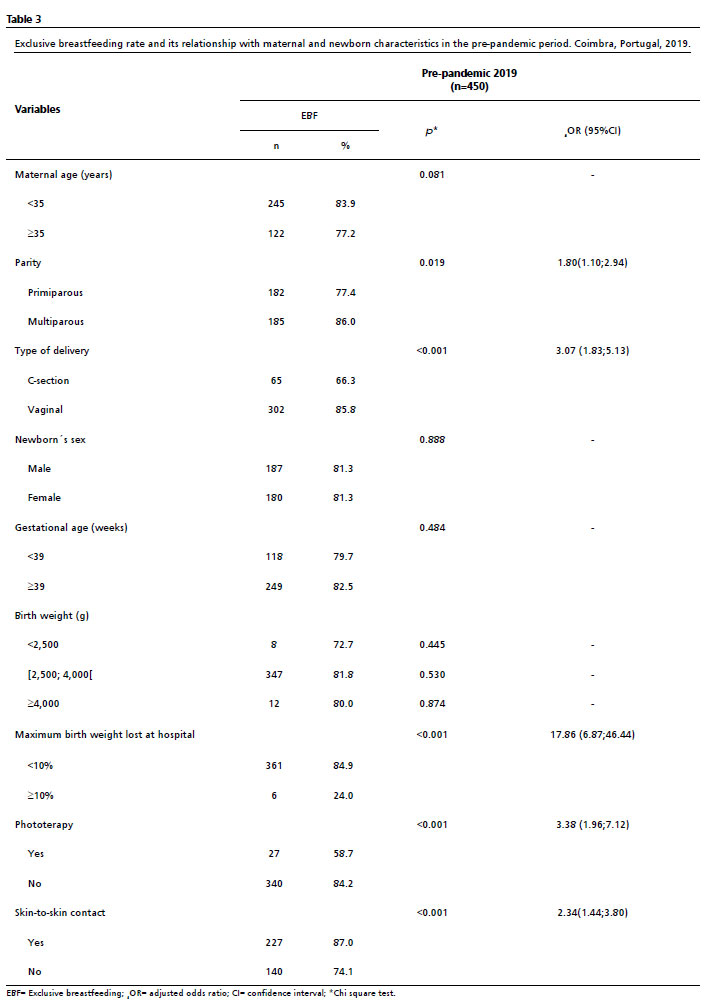
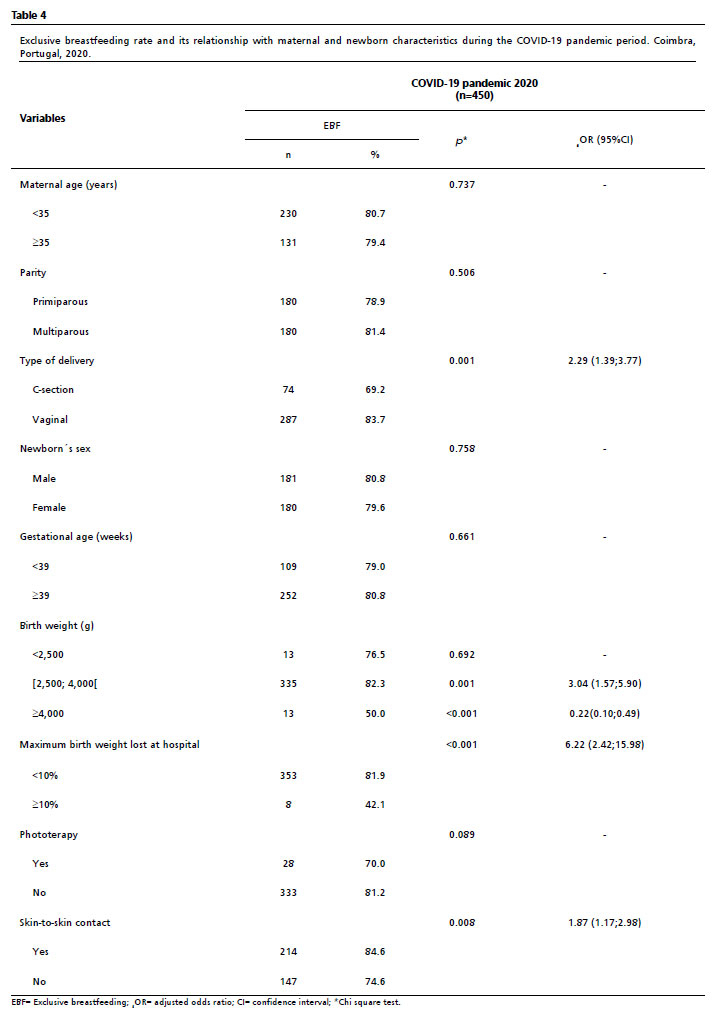
Analysis of factors associated with exclusive breastfeeding in the pre-pandemic (Table 3) and in the COVID-19 pandemic period (Table 4) revealed no relation with maternal age, gestational age, or newborn sex in either period. In both periods, vaginal delivery (pre-pandemic OR=3.07, 95%CI= 1.83;5.13;
p<0.001; pandemic OR=2.29, 95%CI= 1.39;3.77;
p=0.001) and skin-to-skin contact (pre-pandemic OR 2.34; 95%CI= 1.44;3.80;
p<0.001; pandemic OR=1.87; 95%CI= 1.17;2.98;
p=0.008) were positively associated with exclusive breastfeeding. In the pre-pandemic period, multiparity (OR=1.80, 95%CI= 1,10;2.94;
p=0.019) and absence of phototherapy (OR= 3.38; 95%CI= 1.96;7.12;
p<0.001) were also significantly associated with higher exclusive breastfeeding rates.
During the pandemic, normal birth weight (OR=3.04, 95%CI= 1.57;5.90;
p=0.001) was positively associated with exclusive breastfeeding, whereas macrosomia showed a negative association (OR=0.22, 95%CI= 0.10;0.49;
p<0.001). Of the 26 macrosomic newborns in the pandemic period sample, only 50% were discharged with exclusive breastfeeding, but all were discharged with any breastfeeding (exclusive breastfeeding or mixed feeding), reflecting a greater use of formula milk. In the group of low-birth-weight newborns, there were no differences in exclusive breastfeeding rates in relation to the other weight groups in both periods. In both periods, newborns with a weight loss below 10% during hospitalization had greater odds of exclusive breastfeeding (
p<0.001).
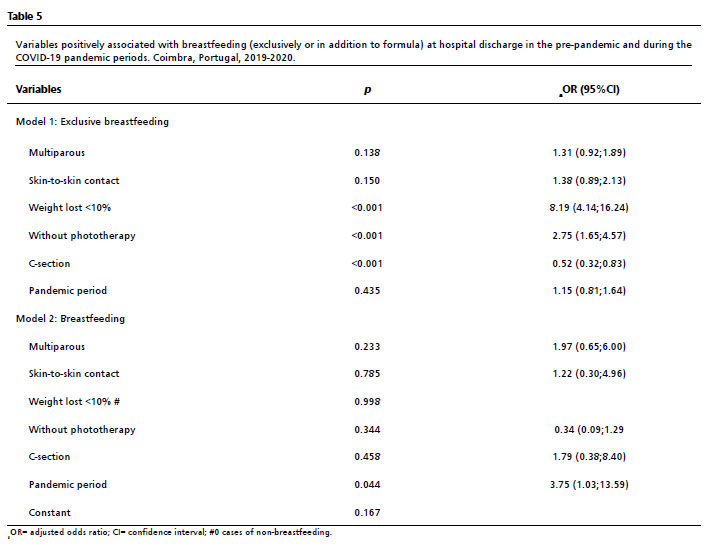
In the multivariable logistic regression model (Table 5), independent factors associated with exclusive breastfeeding at hospital discharge were vaginal delivery (
p<0.001), multiparity (
p=0.019), weight loss under 10% (
p<0.001), and absence of phototherapy (
p<0.001).
DiscussionDuring the COVID-19 pandemic, hospitals faced the dual challenge of protecting mothers and newborns from infection while preserving the quality of perinatal care and the support of breastfeeding. The first hours and days after birth represent a crucial period for the establishment of breastfeeding, and practices such as skin-to-skin contact and early initiation of breastfeeding — strongly recommended by WHO — are known to promote breastfeeding success and maternal–infant bonding.
17,18Our study showed that overall breastfeeding rates at hospital discharge were slightly higher during the pandemic than in the pre-pandemic period, while exclusive breastfeeding rates remained stable. These results indicate that, despite the restrictive measures imposed, breastfeeding practices were not negatively affected in this Baby-Friendly certified hospital. This contrasts with findings from some studies reporting a decrease in breastfeeding rates during lockdowns or under strict infection control measures,
19,20 particularly in institutions not adhering to Baby-Friendly practices. Conversely, other studies conducted in Baby-Friendly hospitals, such as those in the United Kingdom and Italy, have demonstrated the maintenance of favorable breastfeeding indicators during the pandemic, highlighting the resilience of structured institutional support.
21,22The stability of exclusive breastfeeding rates observed in our study may reflect the robustness of the Baby-Friendly Hospital Initiative framework, which emphasizes staff training, standardized protocols, and multidisciplinary involvement in promoting breastfeeding.
15,16 In our institution, the long-standing implementation of these practices and the continuous training of professionals likely contributed to mitigating the potential negative effects of service reorganization, reduced visits, and shorter hospital stays. Moreover, maintaining rooming-in and direct breastfeeding – even under strict infection-prevention measures – preserved opportunities for maternal–infant contact and lactation support during hospitalization.
Among the factors associated with exclusive breastfeeding, vaginal delivery was a consistent positive predictor in both periods, confirming previous evidence that cesarean delivery may hinder the initiation of breastfeeding by delaying maternal recovery and skin-to-skin contact.
23,24 Multiparity was also associated with higher exclusive breastfeeding rates in the pre-pandemic period, probably due to greater maternal experience and confidence; however, this effect lost significance in the adjusted model, possibly reflecting the homogeneity of support provided to all mothers.
25,26Newborns with a maximum weight loss below 10% were significantly more likely to be exclusively breastfed at discharge in both periods. Excessive weight loss is a common reason for formula supplementation, as it may signal delayed lactogenesis or inefficient milk transfer. Similarly, newborns who required phototherapy had lower exclusive breastfeeding rates, possibly due to reduced proximity during treatment and interruptions to feeding routines.
27During the pandemic, normal birth weight and skin-to-skin contact were associated with higher exclusive breastfeeding rates, whereas macrosomia was negatively associated. The latter finding may relate to early introduction of formula supplementation in macrosomic newborns, who are at greater risk of transient hypoglycaemia or delayed lactation onset. Shorter hospital stays during the pandemic could also have limited opportunities for observation and reinforcement of exclusive breastfeeding in these infants.
28Interestingly, despite the major reorganization of healthcare services during the pandemic, skin-to-skin contact rates remained unchanged in our hospital, unlike in other countries where this practice was restricted or temporarily suspended.
29,30 This likely reflects the institutional commitment to uphold WHO recommendations and the BFHI principles, balancing infection control with evidence-based perinatal care. The strong positive association between skin-to-skin contact and exclusive breastfeeding in both periods reinforces its protective role in breastfeeding initiation and maintenance.
This study has several limitations. The retrospective design and structured convenience sampling may limit external validity. Data were collected from a single hospital, and variables such as maternal schooling, socioeconomic status, and psychological factors — known to influence breastfeeding outcomes — were unavailable. Furthermore, the pandemic period analyzed spanned nine months, during which institutional measures and national guidelines evolved, possibly diluting the impact of specific restrictions. Nevertheless, the inclusion of consecutive dyads and the similarity of baseline maternal and neonatal characteristics between groups support the representativeness of our sample and the reliability of comparisons.
To our knowledge, this is the first study in Portugal to assess the COVID-19 pandemic impact of on breastfeeding rates at hospital discharge in a Baby-Friendly certified institution. The stability of exclusive breastfeeding rates observed reinforces the effectiveness of Baby-Friendly practices in safeguarding breastfeeding even under restrictive circumstances. Strengthening these institutional policies and ensuring sustained professional support are essential to maintain optimal breastfeeding outcomes in future public-health emergencies.
References1. World Health Organization (WHO). WHO Director-General’s opening remarks at the media briefing on COVID-19 – 11 March 2020. Geneva: WHO; 2020. [access in 2024 Mar 15]. Available from:
https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-20202. Lazzerini M, Covi B, Mariani I, Drglin Z, Arendt M, Nedberg IH,
et al. Quality of facility-based maternal and newborn care around the time of childbirth during the COVID-19 pandemic: online survey investigating maternal perspectives in 12 countries of the WHO European Region. Lancet Reg Health Eur. 2022; 13: 100268.
3. Juan J, Gil MM, Rong Z, Zhang Y, Yang H, Poon LC. Effect of coronavirus disease 2019 (COVID-19) on maternal, perinatal and neonatal outcome: systematic review. Ultrasound Obstet Gynecol. 2020; 56 (1): 15-27.
4. Rasmussen SA, Smulian JC, Lednicky JA, Wen TS, Jamieson DJ. Coronavirus Disease 2019 (COVID-19) and pregnancy: what obstetricians need to know. Am J Obstet Gynecol. 2020; 222 (5): 415-26.
5. Walker KF, O’Donoghue K, Grace N, Dorling J, Comeau JL, Li W,
et al. Maternal transmission of SARS-CoV-2 to the neonate, and possible routes for such transmission: a systematic review and critical analysis. BJOG. 2020; 127 (11): 1324-36.
6. Portugal. Direção-Geral da Saúde. COVID-19: Fase de Mitigação – Gravidez e Parto. Orientação n.º 18/2020. Lisboa: DGS; 2020. [access in 2024 Mar 15]. Available from:
https://www.stss.pt/images/_Data/Covid19/data_stss-orientacao-0182020-dgs-20200605.pdf7. Portugal. Direção-Geral da Saúde. COVID-19 – Cuidados ao Recém-Nascido na Maternidade. Orientação n.º 26/2020. Lisboa: DGS; 2020. [access in 2024 Mar 15]. Available from:
https://www.ordemenfermeiros.pt/media/22111/orienta%C3%A7%C3%A3o-026-2020-covid-19-cuidados-ao-rec%C3%A9m-nascido-na-maternidade-atualizada-a-20042021.pdf8. Royal College of Obstetricians and Gynaecologists (RCOG). Coronavirus (COVID-19) infection in pregnancy. Version 16. London: RCOG; 2022. [access in 2025 Nov 15]. Available from:
https://www.rcog.org.uk/media/0qune0d3/covid-19-infection-in-pregnancy-v161-final.pdf9. World Health Organization (WHO). Clinical management of COVID-19: interim guidance, 27 May 2020. Geneva: WHO; 2020. [access in 2024 Mar 15]. Available from:
https://iris.who.int/bitstream/handle/10665/332196/WHO-2019-nCoV-clinical-2020.5-eng.pdf10. Sirico A, Musto R, Migliorini S, Brigidi S, Sciarra FA, Carlea A,
et al. Impact of COVID-19 on breastfeeding among SARS-CoV-2 infected pregnant women: a single centre survey study. Int J Environ Res Public Health. 2022; 20 (1): 228.
11. Pace RM, Williams JE, Järvinen KM, Belfort MB, Pace CDW, Lackey KA,
et al. Characterization of SARS-CoV-2 RNA, antibodies, and neutralizing capacity in milk produced by women with COVID-19. mBio. 2021; 12 (1): e03192-20.
12. Hui PW, Ma G, Seto MTY, Cheung KW. Effect of COVID-19 on delivery plans and postnatal depression scores of pregnant women. Hong Kong Med J. 2021; 27 (2): 113-7.
13. Pacheco F, Sobral M, Guiomar R, Torre-Luque A, Caparros-Gonzalez RA, Ganho-Ávila A. Breastfeeding during COVID-19: a narrative review of the psychological impact on mothers. Behav Sci (Basel). 2021; 11 (3): 34.
14. Chertok IA, Artzi-Medvedik R, Arendt M, Sacks E, Otelea MR, Rodrigues C,
et al. Factors associated with exclusive breastfeeding at discharge during the COVID-19 pandemic in 17 WHO European Region countries. Int Breastfeed J. 2022; 17 (1): 83.
15. UNICEF Portugal. A Iniciativa Amiga dos Bebés [Internet]. Lisboa: UNICEF Portugal; [access in 2023 Mar 15]. Available from:
https://www.unicef.pt/o-que-fazemos/o-nosso-trabalho-em-portugal/iniciativa-amiga-dos-bebes/a-iniciativa-amiga-dos-bebes/16. Almeida D, Costa B, Taborda A. Twelve-month prevalence of breastfeeding among infants born in a Baby-Friendly Hospital. Port J Pediatr. 2023; 54 (3): 156-63.
17. Cohen S, Alexander DD, Krebs NF, Young BE, Cabana MD, Erdmann P,
et al. Factors associated with breastfeeding initiation and continuation: a meta-analysis. J Pediatr. 2018; 203: 190-216.e21.
18. Safari K, Saeed AA, Hasan SS, Moghaddam-Nanaem L. The effect of mother and newborn early skin-to-skin contact on initiation of breastfeeding, newborn temperature and duration of third stage of labor. Int Breastfeed J. 2018; 13: 32.
19. Latorre G, Martinelli D, Guida P, Masi E, De Benedictis R, Maggio L. Impact of COVID-19 pandemic lockdown on exclusive breastfeeding in non-infected mothers. Int Breastfeed J. 2021; 16 (1): 36.
20. Vazquez-Vazquez A, Dib S, Rougeaux E, Wells JCK, Fewtrell MS. The impact of the COVID-19 lockdown on the experiences and feeding practices of new mothers in the UK: preliminary data from the COVID-19 New Mum Study. Appetite. 2021; 156: 104985.
21. Boutsikou T, Iliodromiti Z, Pouliakis A, Soulai A, Tzounakou L, Volaki P,
et al. Breastfeeding rates in the COVID-19 era: the experience of a Greek “Baby Friendly Hospital”. J Transl Sci. 2021; 7: 1-3.
22. Vaz AS, Figueiredo S, Taborda A. Breastfeeding during the COVID-19 pandemic: experience of a Neonatology Unit. Birth Growth Med J. 2022; 31 (3): 206-11.
23. Prior E, Santhakumaran S, Gale C, Philipps LH, Modi N, Hyde MJ. Breastfeeding after cesarean delivery: a systematic review and meta-analysis of world literature. Am J Clin Nutr. 2012; 95 (5): 1113-35.
24. Rowe-Murray HJ, Fisher JRW. Baby friendly hospital practices: cesarean section is a persistent barrier to early initiation of breastfeeding. Birth. 2002; 29 (2): 124-31.
25. Lande B, Andersen LF, Baerug A, Trygg KU, Lund-Larsen K, Veierød MB,
et al. Infant feeding practices and associated factors in the first six months of life: the Norwegian infant nutrition survey. Acta Paediatr. 2003; 92 (2): 152-61.
26. Mohamed MJ, Ochola S, Owino VO. Comparison of knowledge, attitudes and practices on exclusive breastfeeding between primiparous and multiparous mothers attending Wajir District Hospital, Wajir County, Kenya: a cross-sectional analytical study. Int Breastfeed J. 2018; 13: 11.
27. Delfino E, Peano L, Wetzl RG, Giannì ML, Netto R, Consales A,
et al. Newborn Weight Loss as a Predictor of Persistence of Exclusive Breastfeeding at 6 Months. Front Pediatr. 2022; 10: 871595.
28. Li S, Wupuer T, Hou R. Factors influencing delayed onset of lactogenesis: a scoping review. Int J Gen Med. 2024; 17: 2311-26.
29. Alhaddad H, Alghamdi S. Skin-to-skin contact and breastfeeding: a scoping review. Int J Adv Appl Sci. 2022; 9 (6): 103-9.
30. Gianni ML, Bettinelli ME, Manfra P, Sorrentino G, Bezze E, Plevani L,
et al. Breastfeeding difficulties and risk for early breastfeeding cessation. Nutrients. 2019; 11 (10): 2266.
Authors’ contributionFerraz AIB: Conceived and designed the analysis, Contributed data or analysis tools, Performed the analysis, Wrote the paper. Azevedo TS: Collected the data, Wrote the paper. Costa MSRD: Collected the data, Contributed data or analysis tools. Costa CITS: Conceived and designed the analysis, Contributed data or analysis tools, Performed the analysis, Wrote the paper. Taborda A: Conceived and designed the analysis, Performed the analysis, Revision.
All authors approved the final version of the article and declare no conflict of the interest.
Data availabilityAll datasets supporting the result of this study are included in the article.
Received on November 22, 2024
Final version presented on November 11, 2025
Approved on November 14, 2025
Associated Editor: Gabriela Sette


 ; Tatiana Santos Azevedo1
; Tatiana Santos Azevedo1