ABSTRACT
INTRODUCTION: the COVID-19 pandemic has had a strong impact on maternal health, amplifying biological and social vulnerabilities and highlighting regional inequalities. In Brazil, pregnant and postpartum women showed a high risk of complications and death, particularly in regions with limited health system response capacity. This study aimed to describe the clinical and care profile of maternal deaths due to COVID-19 in Recife, Brazil, between 2020 and 2021.
DESCRIPTION: eighteen cases of maternal deaths due to COVID-19 were analyzed, based on records from the Mortality Information System of the Brazilian Unified Health System (SIM/SUS) and the Municipal Committee on Maternal Mortality (CMMM) of the city of Recife. Most women were 20-35 years old, of mixed race, and had comorbidities, mainly hypertensive syndromes (60.9%) and obesity (33.3%). Dyspnea and dry cough were the most common symptoms. Cesarean section was the predominant delivery route (61.1%), and 83.3% required intensive care, with mechanical ventilation used in 94.4% of cases. The CMMM classified 72.2% of the deaths as preventable, and the most frequent underlying causes were acute respiratory distress syndrome and septic shock.
DISCUSSION: the findings reveal high clinical severity and persistent weaknesses in obstetric care, reflected in delayed transfers and a high proportion of preventable deaths. Maternal deaths from COVID-19 expose structural inequalities and reinforce the need to strengthen epidemiological surveillance, improve data recording, and expand access to timely and qualified obstetric intensive care.
Keywords:
Maternal mortality, COVID-19, Coronavirus infections, Maternal health, Pregnancy
RESUMO
INTRODUÇÃO: a pandemia de COVID-19 produziu forte impacto na saúde materna, ampliando vulnerabilidades biológicas e sociais e evidenciando desigualdades regionais. No Brasil, gestantes e puérperas apresentaram risco elevado de complicações e morte, especialmente nas regiões com menor capacidade de resposta assistencial. O objetivo deste estudo foi descrever o perfil clínico e assistencial das mortes maternas por COVID-19 em Recife-PE, entre 2020 e 2021.
DESCRIÇÃO: foram analisados 18 casos de mortes maternas por COVID-19, com base em registros do Sistema de Informações sobre Mortalidade do Sistema Único de Saúde (SIM/SUS) e do Comitê Municipal de Mortalidade Materna (CMMM) da cidade do Recife. A maioria das mulheres tinha entre 20 e 35 anos, era parda e apresentava comorbidades, sobretudo síndromes hipertensivas (60,9%) e obesidade (33,3%). Dispneia e tosse seca foram os sintomas mais frequentes. A cesariana predominou como via de parto (61,1%), e 83,3% necessitaram de unidade de terapia intensiva, com ventilação mecânica em 94,4% dos casos. O CMMM considerou 72,2% dos óbitos evitáveis, sendo as causas básicas mais comuns a síndrome respiratória aguda grave e o choque séptico.
DISCUSSÃO: os achados revelam gravidade clínica elevada e fragilidades persistentes na rede obstétrica, expressas em transferências tardias e óbitos evitáveis. As mortes maternas por COVID-19 refletem desigualdades estruturais e reforçam a urgência de fortalecer a vigilância epidemiológica, qualificar os registros e ampliar o acesso a cuidados obstétricos intensivos e oportunos.
Palavras-chave:
Mortalidade materna, COVID-19, Infecções por coronavírus, Saúde materna, Gravidez
IntroductionThe disease caused by SARS-CoV-2, referred to as COVID-19, had a substantial impact on maternal health worldwide. In Brazil, pregnant and puerperal women constituted a risk group, exhibiting increased maternal mortality.
1-3 The presence of comorbidities, such as hypertensive disorders and obesity, potentiates the severity of the infection.
4-5 The late inclusion of pregnant and puerperal women in the National COVID-19 Immunization Program contributed to the observed severity.
6 Characterizing the profile of these deaths allows for the identification of care deficiencies and informs prevention strategies. The aim of this study is to report this case series of maternal deaths due to COVID-19 in Recife-PE between 2020 and 2021, highlighting clinical and care aspects.
DescriptionA total of 18 confirmed cases of maternal death due to COVID-19, occurring in Recife-PE between 2020 and 2021, were included. Data were obtained from the Brazilian Mortality Information System and the Municipal Maternal Mortality Committee, as reported in the Epidemiological Bulletin of the Recife Health Secretariat.
7 Most women were between 20 and 35 years of age, were Brown and married, had completed high school and had paid employment. Dyspnea (83.3%) and dry cough (77.7%) were the most prevalent symptoms, with hypertensive disorders being the most frequent comorbidity (60.9%). Obesity was present in one third of patients, while smoking and alcohol use were infrequent.
Most deaths occurred in the puerperium (77.8%), with a median gestational age of 33.6 weeks. Cesarean section was the predominant mode of birth (61.1%). While 83.2% of women received prenatal care, only 44.4% had more than six consultations, and only a single woman had been immunized against COVID-19 (Table 1).
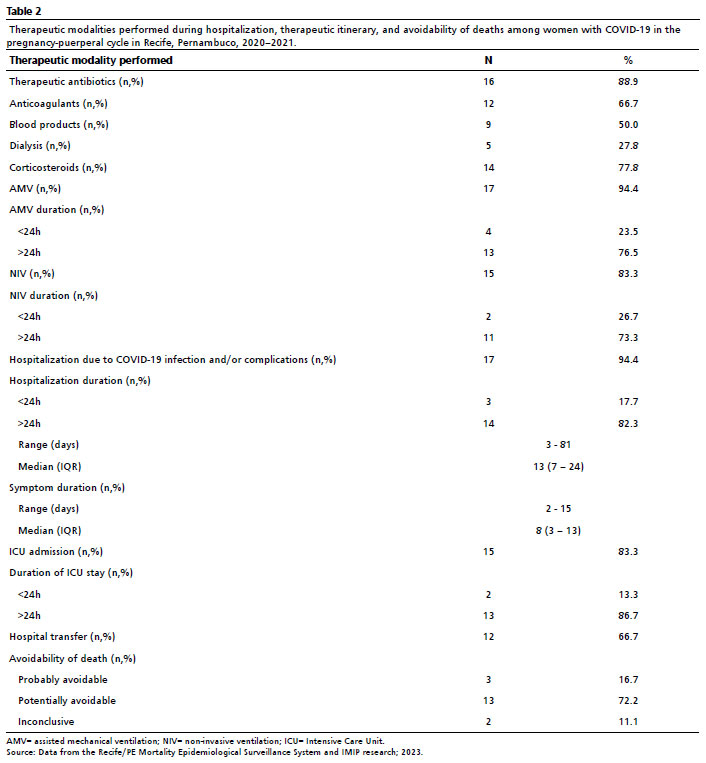
During hospitalization, 83.3% required ICU admission, and 94.4%, required mechanical ventilation, often lasting more than 24 hours. Approximately two thirds were transferred between healthcare facilities, highlighting vulnerabilities in the care network. Antibiotics were used in 88.9% of cases, corticosteroid therapy in 77.8%, and anticoagulants in 66.7%. Notably, 72.2% of cases, the deaths were classified as avoidable (Table 2). The most frequent underlying causes were severe acute respiratory syndrome (SARS) and septic shock, with information complemented by the Epidemiological Bulletins of the Recife Health Secretariat and the Brazilian Ministry of Health.
7,8 DiscussionThe findings of this series reveal a pattern of high severity, marked by a predominance of puerperal deaths and a high requirement for intensive care. The association between severe COVID-19 and preexisting comorbidities, particularly hypertensive disorders and obesity, is well-documented, reinforcing a synergy linked to worse maternal outcomes.
4,5The significant number of transfers and the limited availability of examinations point to deficiencies in the obstetric care network, including the access to prenatal care, timely arrival at health units, and the provision of adequate treatment – aspects described in the Thaddeus and Maine's Three Delays Model.
9 The interruption of routine prenatal care during 2020 and the late inclusion of puerperal and pregnant women in the immunization campaign may also have contributed to the observed severity.
6 Collectively, these elements support the interpretation that the pandemic potentiated pre-existing structural vulnerabilities in obstetric care. National and international reports indicate that the pandemic revealed structural inequalities in the maternal care, disproportionately affecting women in vulnerable contexts.
7,8,10The high proportion of deaths classified as avoidable underscores the need to strengthen protocols for managing respiratory insufficiency, train healthcare teams and expand the access to obstetric ICU beds. Investing in surveillance and integration between primary and specialized care is critical to mitigate avoidable deaths in future public health emergencies.
10-13Maternal mortality due to COVID-19 results from a combination of factors that extends the direct action of the virus, encompassing biological vulnerabilities, social inequalities, and structural weaknesses in the obstetric care network. The deaths recorded in Recife reflect the national scenario, characterized by regional disparities and limited response capacity in crisis situations.
The findings underscore the need to enhance epidemiological surveillance, improve the completeness and accuracy of medical records and death certificates, and invest in the continuous professional development of healthcare teams and the strengthening of Maternal Mortality Prevention Committees. We recommend expanding investigations at both the state and inter-state levels, comparing maternal deaths attributable to and non-attributable to COVID-19, aiming to inform public policies that ensure timely obstetric care, active surveillance and reproductive justice.
References1. World Health Organization (WHO). International Classification of Diseases 11
th Revision (ICD-11). Geneva: WHO; 2022. [
Internet]. [access in 2025 Set 11]. Available from:
https://www.who.int/standards/classifications/classification-of-diseases2. Ministério da Saúde (BR). Manual de recomendações para a assistência a gestante e puérpera frente à pandemia de COVID-19. Brasília (DF): Ministério da Saúde; 2021. [access in 2025 Set 11]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_assistencia_gestante_puerpera_covid-19_2ed.pdf3. Amorim MMR, Takemoto MLS, Fonseca EB. Maternal deaths with coronavirus disease 2019: a different outcome from low- to middle-resource countries? Int J Gynaecol Obstet. 2020; 151 (1): 157-8.
4. Takemoto MLS, Menezes MO, Andreucci CB, Knobel R, Sousa L, Katz L,
et al. Clinical characteristics and risk factors for mortality in obstetric patients with severe COVID-19 in Brazil. BJOG. 2020; 127 (13): 1618-26.
5. Menezes MO, Takemoto MLS, Nakamura-Pereira M, Katz L, Amorim MMR, Salgado HO,
et al. Risk factors for adverse outcomes among pregnant and postpartum women with ARDS due to COVID-19 in Brazil. Int J Gynaecol Obstet. 2020; 151 (3): 415-23.
6. Ministério da Saúde (BR). Plano Nacional de Operacionalização da Vacinação contra a COVID-19. Brasília (DF): Ministério da Saúde; 2021. [
Internet]. [access in 2025 Set 11]. Available from:
https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/c/covid-19/publicacoes-tecnicas/guias-e-planos/plano-nacional-de-operacionalizacao-da-vacinacao-contra-covid-19.pdf/view7. Recife. Secretaria de Saúde. Boletim Epidemiológico: Natalidade e mortalidade materna, fetal e infantil. Recife: Secretaria de Saúde; 2023. [access in 2025 Set 11]. Available from:
https://cievsrecife.wordpress.com/wp-content/uploads/2023/05/boletim-natalidade-e-mortalidade-materna-fetal-e-infantil_n-01_2023.pdf8. Ministério da Saúde (BR). Boletim Epidemiológico COVID-19. Brasília (DF): Ministério da Saúde; 2020. [
Internet]. [access in 2025 Set 11]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/20209. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. 1994; 38 (8): 1091-110.
10. Francisco RPV, Lacerda L, Rodrigues AS. Obstetric Observatory BRAZIL - COVID-19: 1031 maternal deaths because of COVID-19 and unequal access to health care. Clinics. 2021; 76: e3120.
11. Carvalho PI, Frias PG, Lemos MLC, Frutuoso LALM, Figuerôa BQ, Pereira CCB,
et al. Perfil sociodemográfico e assistencial da morte materna em Recife, 2006–2017. Rev Epidemiol Serv Saude. 2020; 29: e2020086.
12. World Health Organization (WHO). A woman dies every two minutes due to pregnancy or childbirth: UN agencies. Geneva: WHO; 2023. [
Internet]. [access in 2025 Set 11]. Available from:
https://www.who.int/news/item/23-02-2023-a-woman-dies-every-two-minutes-due-to-pregnancy-or-childbirth--un-agencies13. Observatório Obstétrico Brasileiro (OOBr). SRAG: Síndrome respiratória aguda grave em gestantes e puérperas. Brasília (DF): OOBr; 2021. [
Internet]. [access in 2025 Set 11]. Available from:
https://observatorioobstetrico.shinyapps.io/covid_gesta_puerp_brAuthors' contributionSouza KR: data curation, formal analysis, investigation, and manuscript writing. Katz L: conceptualization, methodology, supervision, and writing, review, and editing of the manuscript. Cunha ACC: methodology, formal analysis, visualization, writing, review, and editing of the manuscript. Amorim MMR: conceptualization, project administration, supervision; review and editing of the manuscript. All authors approved the final version of the article and declared no conflicts of interest.
Data AvailabilityAll datasets supporting this study are included in the article.
Receiced on October 6, 2024
Final version presented on October 15, 2025
Approved on October 16, 2025
Associated Editor: Alex Sandro Souza


 ; Leila Katz2
; Leila Katz2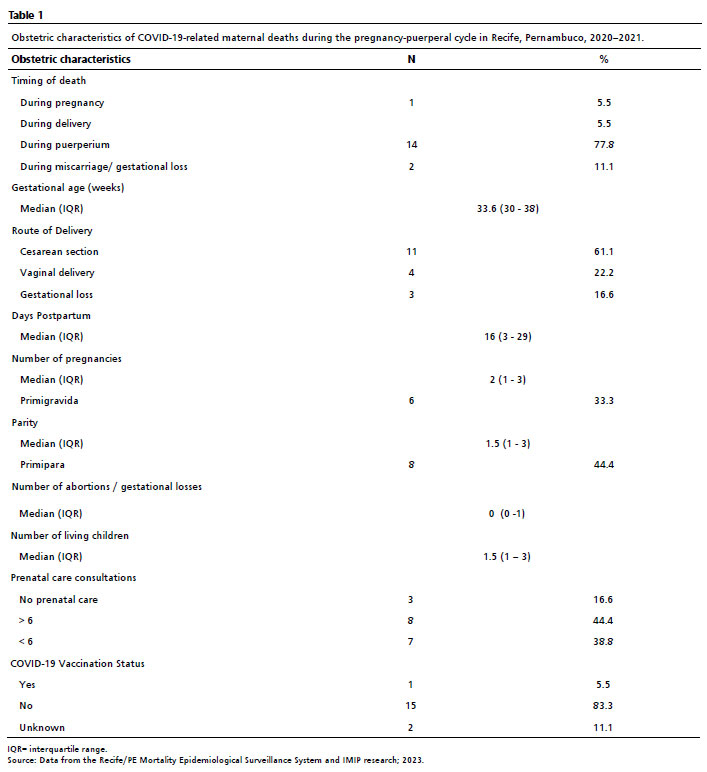






 Ler em português
Ler em português