ABSTRACT
Eclampsia remains a time-dependent obstetric emergency, with a high risk of death and sequelae when there are delays, omissions, or hasty decisions. This article operationalizes the ABCDEFG mnemonic [airway and oxygenation; ventilation; circulation and fluid management; prevention of neurological damage with magnesium sulfate (MgSO₄); immediate recognition and treatment of severe hypertension and targeted tests; fetal assessment; and obstetric decision] as an integrated protocol, aligned with the grammar of emergency care and the specificities of the pregnant woman. The structure prioritizes A-E, only then advancing to F and G. Objective criteria for advanced airway management, operational targets for peripheral oxygen saturation (SpO₂), conduct and therapeutic targets for blood pressure levels, preparation/monitoring of MgSO₄, minimum laboratory panel, and neuroimaging indications are described. The obstetric decision regarding the preferred route of delivery is vaginal, with cesarean section reserved for specific indications. The manuscript also proposes elements for institutional implementation: closed-loop communication, brief simulation, critical time auditing, and indicators (magnesium port, blood pressure control port, and cesarean section for transient tracing). By translating evidence into feasible routines, ABCDEFG seeks to reduce variability in care, shorten decision times, and favor obstetric choices proportional to risk.
Keywords:
Eclampsia, Preeclampsia, Magnesium sulfate, Emergencies, Clinical protocols
RESUMO
A eclâmpsia permanece como emergência obstétrica tempo‑dependente, com risco elevado de morte e sequelas quando há atrasos, omissões ou decisões precipitadas. Este artigo operacionaliza o mnemônico ABCDEFG [vias aéreas e oxigenação; ventilação; circulação e parcimônia hídrica; prevenção de dano neurológico com sulfato de magnésio (MgSO₄); reconhecimento e tratamento imediato da hipertensão grave e exames dirigidos; avaliação fetal; e decisão obstétrica] como protocolo integrado, alinhado à gramática do atendimento de urgência e às especificidades da gestante. A estrutura prioriza A–E, para só então avançar a F e G. São descritos critérios objetivos para manejo avançado da via aérea, metas operacionais da saturação periférica de oxigênio (SpO₂), conduta e meta terapêutica dos níveis pressóricos, preparo/monitorização do MgSO₄, painel laboratorial mínimo e indicações de neuroimagem. A decisão obstétrica da via de parto como preferencial é a vaginal, sendo a cesariana reservada a indicações específicas. O manuscrito propõe ainda elementos para implementação institucional: comunicação em alça fechada, simulação breve, auditoria de tempos críticos e indicadores (porta‑magnésio, porta‑controle pressórico e cesariana por traçado transitório). Ao traduzir evidências em rotinas exequíveis, o ABCDEFG busca reduzir variabilidade assistencial, encurtar tempos decisivos e favorecer escolhas obstétricas proporcionais ao risco.
Palavras-chave:
Eclâmpsia, Préeclâmpsia, Sulfato de magnésio, Emergências, Protocolos clínicos
IntroductionThe elevation of blood pressure (BP) during pregnancy is one of the main determinants of maternal and perinatal morbidity and mortality. Among hypertensive syndromes, eclampsia —generalized tonic-clonic seizures in a patient with preeclampsia, in the absence of another neurological etiology — is considered by the
Rede Brasileira de Estudos em Hipertensão na Gestação (Brazilian Network for Studies on Hypertension in Pregnancy) to be the most severe complication within the hypertensive spectrum, requiring an immediate and organized response.
1The global burden of the disease shows striking contrasts: in high-income countries, the incidence ranges from 1.5 to 10 cases per 100,000 births, whereas in low- and middle-income countries it may reach 19.6 to 142 per 100,000.
2 In these regions, the risk of progression to eclampsia and maternal death is up to ten times higher, reflecting inequities in access, readiness, and quality of care.
3,4Complications include intracerebral hemorrhage, acute pulmonary edema, HELLP syndrome, acute kidney injury, cortical blindness, and cardiorespiratory arrest, affecting up to 70% of untreated or late-treated cases.
5,6 Maternal mortality ranges from zero to 14% but decreases substantially with structured protocols.
In the maternal–fetal dyad, seizures immediately compromise uteroplacental oxygenation and perfusion, posing a risk of acute fetal distress. Typical changes in fetal heart rate (FHR) after a seizure are usually transient and resolve with maternal stabilization. Thus, stabilizing the mother is the most effective way to protect the fetus.
7 This logic supports the prioritization of interventions, preventing delays in necessary actions and avoiding cesarean sections motivated by transient alterations.
Inspired by the trauma emergency model consolidated by the ABCDE mnemonic of the Advanced Trauma Life Support (ATLS) program—and later updated to XABCDE—professors Melania Amorim and Leila Katz proposed in 2011 the ABCDEFG mnemonic applied to eclampsia, adapting the classical ATLS sequence (ABCDE) and integrating two obstetric components: F (Fetus) and G (Gestation). Only in 2018 was the A-to-G mnemonic mentioned by the
Federação Brasileira das Associações de Ginecologia e Obstetrícia (FEBRASGO) (Brazilian Federation of Gynecology and Obstetrics Associations), although without detailed execution as a protocol.
8 Therefore, this article expands, updates, and operationalizes this mnemonic as an integrated protocol, emphasizing patient safety, effective communication, and applicability across different levels of care complexity.
9MethodsA narrative literature review was conducted using the MEDLINE/PubMed and
Biblioteca Virtual em Saúde (BVS) (Virtual Health Library
) databases, which include BIREME, SciELO, and LILACS, with the aim of developing the mnemonic as an integrated protocol. Included studies comprised clinical trials and systematic reviews on anticonvulsants and maternal outcomes,
10,11 investigations on fetal repercussions after seizures and tracing dynamics,
12 recent narrative reviews on maternal complications,
6,7 and multicenter series and studies on morbidity and mortality in different contexts.
2,3,9The research was guided by questions developed according to the PICO mnemonic (patient, intervention, comparison, and outcomes): "In women with eclampsia, does intravenous (IV) magnesium sulfate (MgSO₄), compared with benzodiazepines or phenytoin, reduce seizure recurrence, need for ventilation, and death?"; "In severe hypertension, which first-line agents ensure rapid and safe control without iatrogenic hypotension?"; and "After the seizure, are changes in fetal heart rate (FHR) transient and reversible with maternal stabilization?"
Algorithm development and supporting toolsBased on the anchors (A–E for stabilization and F–G for fetal assessment and obstetric decision-making), supporting tools were developed: MgSO₄ preparation and monitoring charts, blood pressure targets, antihypertensive regimens, laboratorial panel, and delivery interruption algorithms, using the recommended definitions (Table 1).
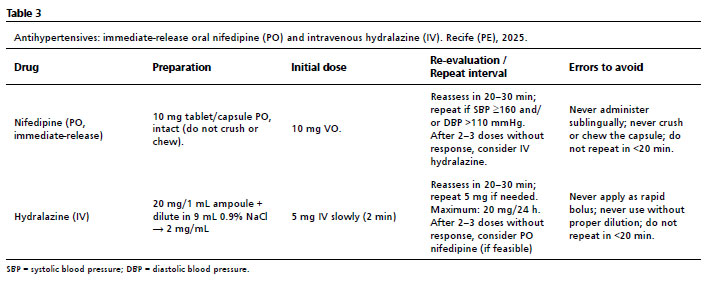
All recommendations were tailored to resources available in Brazil, but adaptable to other settings: oral nifedipine (O) and intravenous hydralazine as the cornerstones of severe hypertension treatment; standardized MgSO₄ preparation with immediate antidote availability; and structured clinical monitoring.
Clinical validation and updatingThe protocol was confronted with the emergency department practices and reviewed by specialists in maternal–fetal medicine, obstetric anesthesia, and intensive care. Divergences were resolved by consensus, prioritizing safety and feasibility. The document is dynamic, updated according to new reviews, trials, and implementation data (time portal to magnesium and blood pressure control portal, cesarean rate due to non-reassuring FHR, and adverse events). Courses and training sessions conducted by Amorim and Katz continue to serve as platforms for dissemination and audit.
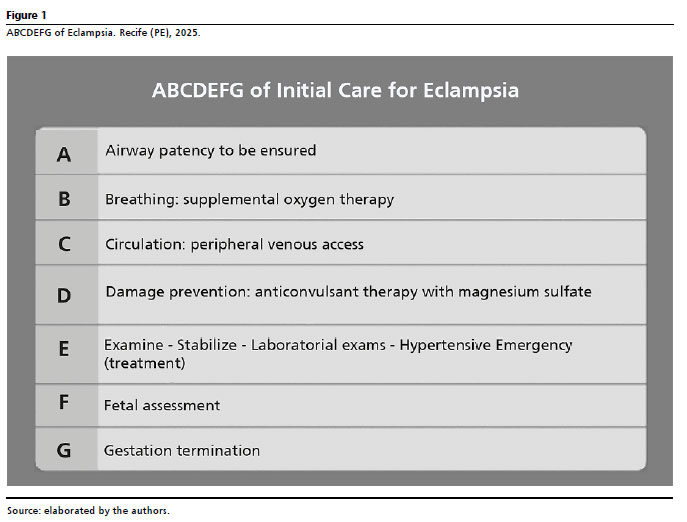
8,13The ABCDEFG mnemonicPurpose and rationaleThe ABCDEFG mnemonic organizes, in operational language, the initial management of eclampsia in a time-dependent manner centered on maternal–fetal safety. Its principle is straightforward: stabilize the mother through rapid primary assessment and successive reassessments (A–E), and only then evaluate the fetus and determine the timing and mode of delivery (F–G). Its construction follows the alphabet—ABCDEFG (Figure 1):
A – Aid/Airway: airway protection and team mobilization with defined roles.
B – Breathing: assessment of respiratory pattern and titrated oxygenation.
C – Circulation: venous access, cautious hydration, and perfusion monitoring.
D – Disability (Damage Prevention): focused neurological assessment and administration of the anticonvulsant of choice (MgSO₄).
E – Examination/Emergency hypertension/Exams: targeted physical examination, immediate treatment of severe hypertension, and laboratorial panel.
F – Fetus: assessment of fetal well-being after maternal stabilization, recognizing transient post-seizure alterations.
G – Gestation: decision on delivery and interruption timing is based on obstetric criteria, avoiding premature interventions.
Principles of use: Parallel execution by trained (briefed) staff, short reassessment cycles, loud communication, and recording of critical times. Requires readiness of materials, antidotes, and simple goals, integrating with checklists and flowcharts to reduce omissions and variability. |
Adaptation to different settings
In resource-limited settings, the priority should be on essentials: lateral positioning, suction of, oxygen administration, two venous accesses, bedside MgSO₄ with antidote available, immediate treatment for hypertension, and fetal assessment after stabilization. In higher-complexity centers, advanced monitoring, imaging studies (as indicated), and support from anesthesia and obstetric intensive care units (ICU) should be incorporated.
Practical application of XABCDE in eclampsia
The ABCDEFG mnemonic was created before the ATLS modification to XABCDE. Since eclampsia is not primarily a hemorrhagic condition, the omission of X was maintained; however, a rapid inspection for trauma or postpartum hemorrhage (PPH) is recommended. After this quick scan, proceed as follows: A and B: airway patency, protection against aspiration, and adequate ventilation/oxygenation; C: two calibrous access, conservative hydration, and hemodynamic monitoring; D: neurological assessment and early administration of MgSO₄ IV; E: focused physical examination, immediate treatment of severe hypertension, and priority laboratorial testing. Steps F and G (secondary assessment) should only be initiated after maternal stabilization to avoid cesarean sections prompted by transient fetal changes.12
Room preparation and role distribution
Before starting the sequence, confirm the availability of materials (suction, oxygen, mask, cannulas, venous access, infusion pump, MgSO₄, antidote, and calibrated sphygmomanometer), define roles (monitoring, medication, suction, documentation, communication with neonatology and imaging), and review the A–B–C plan in case advanced airway management becomes necessary.
Parallel execution and continuous reassessment
The ABCDE sequence should be performed in parallel, with clearly defined roles and aloud, structured communication. Airway, breathing, and circulation must be reassessed in short cycles, while MgSO₄, antihypertensives, and exams are implemented without interrupting clinical monitoring. This design shortens critical times and prepares a orderly transition to steps F and G.
Step-by-Step (Guide)
A – AIRWAY / AID
The first action is to protect and maintain airway patency and prevent aspiration from the onset of the seizure through the postictal period, while the team is mobilized and roles are defined aloud. The clinical leader should activate the obstetric, anesthesia experienced in obstetric airway management, bedside nursing, and, when indicated, neonatology teams—clearly assigning who monitors, does the suctions, records time, and communicates with the delivery room or ICU—to minimize omissions and shorten critical response times.14,15
Bed safety must be immediate: left lateral decubitus, head turned to the side, padded rails, and removal of rigid objects. Vigorous restraint should be avoided during the seizure. Lateral positioning reduces aspiration risk and facilitates secretion drainage while the team organizes the care sequence.14
Once the convulsive phase ends, airway patency should be systematically confirmed: check phonation, air movement, and respiratory effort; perform basic opening maneuvers (chin-lift and jaw-thrust); and suction secretions as needed. In cases of decreased consciousness, insert an appropriately sized oropharyngeal airway to maintain patency and prevent tongue biting. No improvised objects should be placed in the mouth, and the mouth should not be forced open with fingers or a Guedel airway inserted in an awake, conscious patient.15
The decision for advanced airway management should not be delayed when criteria are met: inability to protect the airway, persistent hypoxemia, apnea, significantly reduced consciousness (Glasgow Coma Scale ≤8), or recurrent/refractory seizures. In pregnant women, the likelihood of a difficult airway is higher—due to mucosal edema, reduced oxygen reserve, and a full stomach—so the first attempt must be the best attempt. Prior planning by a trained professional is essential, with a backup strategy, supraglottic device availability, and rescue cricothyrotomy equipment ready when needed.15,16
Safe performance depends on a brief obstetric airway checklist, including equipment (suction, mask and bag-valve, cannulas of various sizes, videolaryngoscope, supraglottic device, and cricothyrotomy kit), defined team roles, and clear first-pass and rescue plans. Continuous monitoring of oxygen saturation (SpO₂), heart rate, and BP should begin upon admission and continue throughout stabilization.14
The "Never" of A:
• Never insert improvised objects into the patient's mouth during a seizure.
• Never force the mouth open with fingers or insert a Guedel airway in a conscious patient.
• Never delay airway protection when objective criteria for intubation are present.
• Never perform multiple uncoordinated intubation attempts without a defined rescue plan.
• Never remove lateral positioning or neglect bed safety.
• Never stop MgSO₄ infusion to free the line for other medications.
B – BREATHINGThis step aims to ensure adequate ventilation and oxygenation in the immediate postictal period, when respiratory fluctuations are common and the risk of hypoxemia is highest. Clinical assessment should be repeated in short cycles, observing respiratory rate (RR), ventilatory pattern (depth, accessory muscle use, and pauses), chest expansion, and pulmonary auscultation. Repeated monitoring allows early identification of deterioration due to aspiration, central depression, or fatigue, guiding timely escalation.
5,6Oxygen therapy should be titrated, not automatic: begin with a non-rebreather mask, adjusting flow to maintain SpO₂ ≥95%, and reduce it as the patient stabilizes. The goal is to correct hypoxemia without inducing sustained hyperoxia, which may cause hemodynamic instability. The team should document time, targets, and responses, prioritizing trends over isolated values.
6Triggers for advanced support are explicit: persistent desaturation despite titrated oxygen, increased respiratory effort, clearly inadequate ventilation, or clinical signs of aspiration (ineffective cough after vomiting, stridor or persistent wet sounds, new crackles at lung bases, and progressive hypoxemia not explained by other factors). Based on these findings, activate the responsible team promptly, following institutional protocols for noninvasive support or intubation. In parallel, reassess step A, since ventilatory failure may indicate airway loss, significant aspiration, or the need for controlled sedation due to recurrent seizures.
Mandatory principles include: avoid hyperventilation without indication; avoid maintaining high oxygen flow without periodic reassessment and gradual weaning once SpO₂ targets are achieved; and do not delay escalation when objective criteria are met. During the first hour, serial SpO₂ and RR intervals should be recorded, integrating these data into subsequent hemodynamic and neurological decisions.
6,16The "Never" of B:
• Never maintain oxygen on high-flow without serial reassessment and adjustment as needed.
• Never hyperventilate the patient without clinical indication.
• Never ignore signs of respiratory fatigue or evident ventilatory effort.
• Never delay escalation when SpO₂ <90% despite supplemental oxygen.
• Never persist with only a face mask if criteria for advanced airway management are present.
C – CIRCULATIONAt this stage, maternal perfusion is sustained, vascular access is prepared for critical therapies, and hemodynamic monitoring is organized for the first hours, always with fluid restraint and disciplined documentation. BP should be measured with an appropriately sized cuff and standardized to the same arm for sequential readings to reduce variability. Postictally, BP should be reassessed at short intervals, alongside clinical evaluation (peripheral perfusion, capillary refill, and level of consciousness), as isolated readings may be misleading.
5,6Venous access should be obtained early: two peripherals calibers (16–18G) on the upper-limb, secured and tested, with infusion pumps and standardized labeling. Whenever possible, reserve one line exclusively for MgSO₄ to avoid interruptions and switches that compromise therapy, leaving the other for medications and fluids. In difficult access situations, humeral intraosseous access is a safe and rapid alternative.
5Fluid management should be conservative. The goal is to maintain perfusion with a low basal rate of isotonic crystalloid, adjusted by clinical response. Persistent hypotension requires a search cause investigation, such as antihypertensive use, vasovagal reflex, or bleeding, without automatic expansion. In pregnant women with preeclampsia/eclampsia, altered vascular compliance and fluid overload risk, make excessive volume administration dangerous; prudence prevents congestion and hypoxemia.
5,6,17Urine output should be monitored via indwelling catheter, interpreted in the hemodynamic and renal context. The operational goal is ≥0.5 mL/kg/h (or 25–30 mL/h), serving as an alert sign. Persistent oliguria should prompt reassessment of volume status, perfusion, and renal function, and adjustment of MgSO₄ infusion.
5,17Proper organization of infusions is key to safety: every solution must be labeled with the drug, concentration, rate (mL/h and g/h), start time, and double verification. Avoid Y co-infusion with incompatible solutions and plan replacements without interrupting critical therapies. Each relevant administration should have documented time and effect (BP, HR, SpO₂, urine output) to guide decisions and generate quality indicators.
6This step is directly linked to steps B and E: adequate ventilation preserves hemodynamics, and blood pressure control is only safe when circulation is stable and monitored. In any deterioration, rapid reassessment of A–B–C should be performed.
The "Never" of C:
• Never correct hypotension empirically with large volumes without investigating the cause.
• Never liberalize fluids in preeclampsia/eclampsia without clinical criteria due to pulmonary edema risk.
• Never use the same line for MgSO₄ and other medications, interrupting therapy.
• Never omit recording time, doses, rates, and hemodynamic responses (lack of traceability compromises safety).
• Never neglect urine output monitoring.
• Never ignore early signs of fluid overload (dyspnea, crackles) or hemodynamic instability.
D – DISABILITY / PREVENTION OF NEUROLOGICAL DAMAGE / MgSO4₄The focus of this step is clear: stop the seizure, prevent recurrences, and protect maternal brain function while systemic stabilization continues. MgSO₄ is the treatment of choice, proven superior to diazepam and phenytoin in reducing recurrent seizures and maternal mortality. Administration should be immediate, right after the seizure, without waiting for test results, with clinical monitoring of RR, deep tendon reflexes, and urine output.
4,8,18The Collaborative Eclampsia Trial (1995) established the superiority of MgSO₄. Subsequent systematic reviews published in the Cochrane Library confirmed its effectiveness and safety compared with diazepam, phenytoin, and the lytic cocktail.
4,8,17 This evidence supports simple, reproducible protocols: loading and maintenance doses, toxicity prevention, antidote preparation, and recurrence management.
The main classical therapeutic regimens are:
• Zuspan: loading dose 4g IV over 20–30 min; maintenance 1g/h IV.18
• Pritchard: loading dose 4g IV + 10 g intramuscular (IM) (5g per buttock); maintenance 5g IM every 4h, provided deep tendon reflexes are present, RR adequate, and urine output >25–30 mL/h.19
• Sibai: loading dose 6g IV over 20–30 min; maintenance 2 g/h IV.20
The
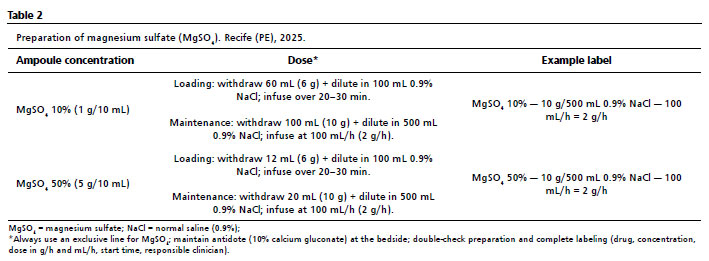
Instituto de Medicina Integral Prof. Fernando Figueira (IMIP) uses the Sibai regimen, with a 6g IV loading dose over 20–30 min and maintenance varying from 1g/h for preeclampsia to 2g/h for eclampsia (Table 2), after observing seizure recurrence rates above the literature average (10%) with the 1g/h infusion. Duration should be 24 hours after delivery or the last seizure.
5,6 We suggest the IV regimen, as the systematic review published in the Cochrane Library in 2023 did not demonstrate unequivocal superiority among the different MgSO₄ regimens, but highlighted methodological limitations of the studies.
21 Nevertheless, the continuous IV regimen is preferred for several reasons:
• Predictable onset of action and the possibility of dose control (immediate interruption or reduction in case of toxicity, which is not feasible with large IM depots).
• Safer monitoring, facilitating adjustments according to clinical status.
• Lower risk of local complications (severe pain, abscess, and gluteal hematoma), particularly relevant in thrombocytopenia or anticoagulant use.
• IM administration contraindicated in HELLP syndrome with thrombocytopenia.
• Lower chance of preparation/dose errors (standardized infusion pump, full labeling, and exclusive line).
• Feasibility within the service context, which provides pumps, trained staff, and logistics for continuous monitoring.
It is recognized that the literature has not yet demonstrated unequivocal superiority of one regimen over another for critical outcomes. New clinical trials would be necessary to define the role of the IM regimen, which may be appropriate in transport situations without an infusion pump or when fluid restriction is required, provided contraindications are respected.
Variations in therapy duration (single dose, 6h, 12h, 24h, or adjusted according to diuresis) have also been tested,
17,22 but the largest and most robust study, the Eclampsia Trial, used MgSO₄ for 24 hours. Therefore, there is no clinical justification to shorten a regimen that remains the most studied.
17,23During MgSO₄ infusion, the patient should be monitored with simple and continuous parameters suggestive of intoxication; there is no need for serum magnesium measurement for monitoring:
24• Respiratory: serial respiratory rate (RR); and continuous SpO₂.
• Neurological: presence of deep tendon reflexes (patellar/bicipital).
• Renal: urine output ≥ 25–30 mL/h (or ≥ 0.5 mL/kg/h).
• Signs of toxicity: loss of reflexes at elevated levels; respiratory depression at higher levels; cardiac arrest at extreme levels.5,6
• It is important to know that when signs of toxicity appear, you should:
• Suspend MgSO₄.
• Provide oxygen/ventilatory support as needed (if respiratory depression or arrest).
• Administer antidote (10% calcium gluconate, 10 mL [1 g] IV slowly over 2–3 min, with cardiopulmonary monitoring).
Management of recurrent seizures under MgSO4₄Most recurrences of purely convulsive episodes (without intracranial hemorrhage) respond to an additional MgSO₄ dose. Sedation and advanced airway management should be considered early in refractory cases or when aspiration/hypoxemia risk is high due to an increased chance of secondary hemorrhage (time should not be wasted on hydantoin). Management should include:
• Confirm that the loading dose was complete and maintenance infusion is active and correct.
• Immediate re-dose: 3g IV over 5–10 min.
• Recurrence or persistence: hydantoin (10mg/kg) IV and anesthesia evaluation for sedation, intubation, and ventilation if indicated. If the initial hydantoin dose is effective, continue IV maintenance.
• In status epilepticus or respiratory/hemodynamic deterioration: rapid-sequence sedation per institutional protocol, prioritizing airway protection and hemodynamic control, maintaining MgSO₄ after stabilization.5,6
Adjustments in renal dysfunction/oliguriaMgSO₄ is renally excreted, and eclampsia often associates with renal function deterioration. The loading dose should always be maintained, but maintenance adjustments may be necessary (Table 2):
• Oliguria or oligo/anuria (<25–30 mL/h): maintenance suspend.
• Presence of diuresis but elevated creatinine:
* <1.5 mg/dL: maintain standard maintenance (eclampsia = 2 g/h).
* 1.5–2.4 mg/dL: halve the maintenance dose (eclampsia = 1 g/h).
* ≥2.5 mg/dL: do not administer.
The "Never" of D:
• Never interrupt MgSO₄ infusion to make the line available for other drugs.
• Never administer successive MgSO₄ re-doses without following service protocol: single re-dose of 3g IV; if persistent, use hydantoin and evaluate for orotracheal intubation (OTI).
• Never adjust infusion rate without checking respiration, deep tendon reflexes, and urine output.
• Never keep the antidote (calcium gluconate) away from the bedside.
• Never use IM regimen in patients with thrombocytopenia or HELLP syndrome, due to hematoma/abscess risk.
E – HYPERTENSIVE EMERGENCY, STABILIZATION, AND TESTSSevere hypertension in eclampsia [systolic blood pressure (SBP) ≥160 mmHg and/or diastolic blood pressure (DBP) ≥110 mmHg] is a time-dependent emergency requiring immediate treatment, without waiting for additional "confirmation" or completion of the MgSO₄ loading dose. Antihypertensive administration and MgSO₄ infusion should be simultaneous. The goal in the first hours is to reduce BP by approximately 15–25% and maintain SBP between 130–150 mmHg and DBP between 80–100 mmHg, avoiding abrupt drops that compromise cerebral and uteroplacental perfusion.
2,5Management starts with correct measurement: appropriately sized cuff, standardized limb, and documentation of each measurement time. Severe values trigger immediate treatment, in parallel with other measures. At IMIP, immediate-release oral nifedipine and IV hydralazine are used (labetalol is unavailable in Brazil). In any regimen, the rule is one change at a time: adjust, measure, wait for response, then decide the next step (Table 3).
2,5 BP control should be accompanied by measures that reduce adrenergic surge and complications: calm environment, lateral positioning with head elevation or uterine displacement, plus antiemetics and analgesia when indicated. Fluid management follows the parsimony of step C, with fluid balance and urine output targets. Record BP, target symptoms, and response at 10, 30, and 60 min. Communication should follow closed-loop protocol (explicit order, read-back, confirmation, record of time and result).
25 Safety depends on continuous clinical monitoring and documentation, paying attention to iatrogenic hypotension and adjusting treatment according to BP response.
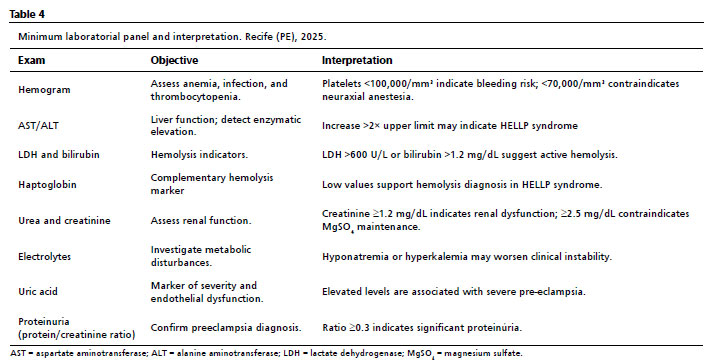
Priority exams include complete blood count with platelets, liver function exams [aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), and bilirubin], haptoglobin for hemolysis assessment, urea, creatinine, electrolytes, uric acid, and proteinuria (spot protein/creatinine ratio) (Table 4). Complementary tests: electrocardiogram (ECG) when indicated, chest X-ray for suspected aspiration or pulmonary edema. Fundoscopy is indicated for persistent amaurosis, aiding differential diagnosis of retinal detachment and cortical blindness. Neuroimaging [CT or MRI] is recommended for prolonged coma, focal deficits, thunderclap headache, persistent amaurosis, recurrent seizures despite MgSO₄, or suspected intracranial hemorrhage/cerebral venous thrombosis, to identify structural lesions and reversible posterior encephalopathy (Table 4).
5 Eclampsia requires intensive care. Proper management is inconceivable without ICU perspective at some stage. Referral may be necessary at various points: airway and breathing for intubation or ventilatory support; circulation for hemodynamic instability or renal dysfunction; neurological for recurrent seizures or status epilepticus; hypertensive control when refractory to initial therapy. Even after delivery, puerperal instability risk justifies ICU admission.
Every patient with eclampsia should be admitted or transferred to ICU, either immediately in severe cases or after initial stabilization, to ensure continuous monitoring and advanced support. The ideal location provides uninterrupted monitoring, specialized staff, and rapid response to sudden deterioration—conditions inherent to eclampsia.
With controlled BP and clinical stability, primary management concludes, and secondary assessment begins, focusing on F (fetus) and G (pregnancy). This prioritization avoids premature interventions prompted by transient fetal alterations post-seizure and maintains focus on maternal recovery and fetal protection.
2,5In this phase, ATLS
27 uses the AMPLE mnemonic (Allergies, Medications, Past Medical History, Last Meal or Oral Intake, and Events Leading to Injury) to collect essential history; for pregnant patients, we adapt to CODE (Complications of pregnancy, Obstetric history, Estimated date, and Additional events). Here, we intentionally simplify: secondary assessment is restricted to F and G, reflecting eclampsia clinical priority.
Step E should run concurrently with MgSO₄ (D) and respiratory measures (B), always with fluid parsimony (C); separation of letters is didactic—everything is executed simultaneously.
The "Never" of E:
• Never delay antihypertensive initiation in severe hypertension.
• Never use sublingual nifedipine or manipulate capsule/tablet.
• Never administer other drugs in rapid sequence without respecting dose-response time.
• Never switch multiple agents simultaneously (one change at a time).
F – FETUS (Fetal Assessment)The principle is "mother first." The best fetal intervention immediately post-seizure is complete maternal resuscitation. Uteroplacental perfusion depends on maternal hemodynamic and ventilatory stability. Hypoxemia, uncontrolled severe hypertension, tachysystole, and improper maternal positioning reduce flow, explaining typical fetal heart rate (FHR) changes post-seizure. Prioritizing airway and breathing (A–B), circulation (C), MgSO₄ (D), and BP control (E) restores the fetal physiological substrate, with most cardiotocographic (CTG) tracings normalizing within minutes to a few hours.
5,10Once maternal stability and BP are within operational range, fetal assessment gains focus. Common post-seizure patterns: initial bradycardia, compensatory tachycardia, reduced FHR variability, often with transient decelerations. These usually regress with titrated oxygen, hypertension control, tachysystole correction, and lateral maternal positioning. Document recovery with temporal milestones (minute of seizure, start/end of bradycardia, measures taken, onset of tachycardia, time to normalized variability) to avoid hasty interventions based on isolated post-seizure snapshots.
10Checkpoints: record seizure time, minute-by-minute FHR evolution, and response to interventions. Monitoring can be continuous (cardiotocographic) in early hours or intermittent every 15 min if continuous monitoring is unavailable, provided maternal resuscitation remains priority.
Sustained fetal bradycardia >10–15 min despite adequate maternal resuscitation raises suspected premature detachment of a normally inserted placenta (PDNIP), other clinical signs should be observed.
9 Significant abruption may prevent CTG recovery, showing persistent bradycardia or progressing to prolonged tachycardia with minimal variability, indicating persistent fetal compromise. PDNIP diagnosis in this context is primarily clinical, as ultrasound often fails to detect it.
In the absence of persistent findings of fetal compromise, the expectation of progressive normalization prevails, and termination of pregnancy is again guided by obstetric criteria, not by the transient reaction to the convulsive event.
5,10Communication with the team should follow a closed-loop logic: announce the expected post-seizure pattern, state the target threshold for PDNIP, and mark the next checkpoint ("reassess in 10 min"). This practice protects against two equally risky situations: postponing a necessary intervention when recovery does not occur within the expected time frame or rushing into a cesarean section in response to changes that were only a temporary expression of the mother's condition.
F Alert: mother first!
• Even if cesarean is indicated, always stabilize mother first unless urgent (PDNIP).
• Do not rush cesarean based on CTG immediately post-seizure.
• FHR changes often improve with maternal resuscitation.
• Ensure complete maternal resuscitation (A–E) before concluding sustained fetal compromise.
• Keep track of time frames in the record: time since the seizure, when the bradycardia started and when it stopped, measures taken, and response.
G – GESTATION (CHOICE OF DELIVERY AND TIMING)Eclampsia indicates pregnancy termination, not immediate fetal extraction. Sequence is deliberate: first complete maternal stabilization (A–E), then fetal reassessment (F), finally obstetric decision proportional to risk. When possible, wait ~1 hour after last seizure for maternal recovery and reversal of transient post-seizure fetal changes.
Type of delivery is not cesarean by default. Decisions should rely on objective obstetric criteria, considering maternal and fetal conditions. Vaginal delivery is preferred when clinically and obstetrically feasible, offering lower risk of anesthetic, hemorrhagic, and infectious complications, faster maternal recovery, and fewer unnecessary interventions.
6,27Cesarean should be reserved for genuine indications: persistent fetal distress unresponsive to maternal stabilization, PDNIP, significant hemorrhage, abnormal presentations, or early gestational age (<32 weeks) with unfavorable cervix and viable fetus (induction-to-delivery time may be excessively long). Decisions must be individualized. Persistent CTG alterations or Doppler with absent/reversed umbilical artery diastole also indicate cesarean, but not emergently; maternal stabilization is required.
The pregnant woman is considered stable for delivery when the decision for the moment of interruption is: regaining appropriate consciousness, airway protection ensured, adequate oxygenation under monitoring, seizures controlled with ongoing MgSO₄, BP stabilized (SBP 130–150 mmHg, DBP 80–100 mmHg), urine output measured, and clinical documentation is complete. Only then does obstetric evaluation regain centrality.
Choice of delivery Observational studies indicate that labor induction and vaginal delivery can be achieved with acceptable outcomes in cases of eclampsia, and two randomized clinical trials demonstrated that normal delivery is feasible and cesarean section does not improve maternal or perinatal outcomes
27,28 The systematic review published in the Cochrane Library on preeclampsia also supports that there is no evidence of superiority for planned cesarean delivery, reinforcing the obstetric practice of preferring vaginal delivery whenever maternal and fetal conditions allow.
28When the cervix is favorable and presentation is cephalic with a live fetus, induction or conduction of vaginal delivery is recommended, with appropriate analgesia and continuous maternal-fetal monitoring. In the case of a stillborn fetus, normal delivery remains the preferred one. If the cervix is unfavorable and there is no urgency, cervical ripening may be considered. Cesarean section is reserved for situations of disproportionate risk from waiting: persistent fetal distress unresponsive to maternal resuscitation; placental abruption (PDNIP); severe hemorrhage; abnormal presentations; and uterine scar contraindicating induction or making induction unfeasible within the available clinical timeframe.
5For labor induction, combined methods such as balloon plus misoprostol, balloon plus prostaglandin, or balloon plus oxytocin are preferred when technically available, as they distribute cervical ripening effects and reduce the risk of uterine hyperstimulation.
29During the active phase, and especially the expulsive phase, rigorous fetal monitoring should be maintained, either by structured intermittent auscultation or CTG when available, alongside adequate analgesia and continuous maternal oxygenation. The goal is to reduce the risk of sudden decompensation for both mother and fetus.
30In the context of eclampsia, intervention should be guided not only by signs of compromise but also by avoiding excessive expulsive effort that may trigger new hypertensive peaks or recurrent seizures. Therefore, delivery should be anticipated whenever the expulsive phase is prolonged, using vacuum extraction or forceps if necessary, even if fetal vitality is preserved. Maternal monitoring with SpO₂ can also indicate instrumental delivery if oxygen saturation drops (<95%).
31Regarding maternal position, the patient may assume her preferred position: if stable, she may ambulate or deliver in an upright position, provided continuous and adequate monitoring is maintained. This freedom, coupled with careful shortening of the expulsive phase when necessary, is part of the strategy to ensure maternal and fetal safety.
Labor analgesia plays a critical role in pain control and reduction of adrenergic surge, contributing to maternal hemodynamic stabilization. Neuraxial techniques are preferred when not contraindicated, such as in significant thrombocytopenia (platelets <70,000/mm³), coagulopathy, or altered consciousness. When these conditions prevent their use (severe thrombocytopenia, sedated and ventilated patient, or under general anesthesia), alternative non-neuraxial techniques are employed, always with multiprofessional monitoring.
Postpartum careIn the immediate puerperium, maintenance of MgSO₄ for 24 hours after delivery or after the last seizure remains mandatory, along with blood pressure control, conservative fluid balance, and respiratory and neurological monitoring. The patient should remain in the obstetric ICU for at least 72 hours, and transfer to step-down care and eventual discharge should only occur when objective stability criteria are met and documented.
DiscussionManagement of eclampsia requires speed, precision, and multiprofessional cooperation. In this context, tools that structure care are essential. The checklist developed by the American College of Obstetricians and Gynecologists (ACOG) is important,
29 but has limitations: it does not prioritize steps, and its integration in high-urgency situations is difficult. Implementation studies show that checklists increase the execution of critical actions, but their impact depends directly on team training and familiarity. In this scenario, adapting a consolidated model such as ATLS emerges as a more effective strategy for obstetric care.
The ABCDEFG (ALSE) mnemonic provides clarity and linearity to the assessment sequence, reducing errors associated with stress, fatigue, and cognitive overload. The proposal does not impose rigidity but provides a mental framework that prevents omissions and allows dynamic and simultaneous execution of steps, provided there is a trained team and efficient communication. Assessment must be continuous and cyclical, adjusting interventions according to clinical response.
Obstetric adaptation is fundamental: while trauma prioritizes immediate invasive interventions, in eclampsia emphasis is on airway and breathing protection, hypertension control, and prevention of further seizures. Allocating fetal assessment (F) highlights the priority that stabilizing the mother is the best way to protect the fetus. ABCDEFG thus functions as a "clinical reasoning track," without replacing team situational judgment.
Mentioning the mnemonic may suggest a rigid sequence, but practice shows that assessment should be simultaneous, dynamic, and rapid. In trauma, A–B–C–D can be inferred in seconds with brief verbal interaction with the patient.
27 In obstetrics, the analogy is valid: if the patient responds appropriately, immediate critical failure is unlikely, but primary assessment must be completed. The process is iterative, repeated in cycles to monitor response and identify new instabilities.
Standardized communication is another pillar. Closed-loop communication reduces errors, shortens critical times, and ensures traceability of decisions. It underpins management across all protocol points: role assignment in A, oxygenation targets in B, access and fluid balance in C, magnesium dose and maintenance in D, BP targets and exams in E, fetal checkpoints in F, and obstetric decision in G. Hot debriefing immediately after stabilization allows immediate synthesis and improvement commitments, while cold debriefing at 24–72 hours, indicators review, identifies root causes, and guides protocol adjustments.
ABCDEFG consolidates only when incorporated as institutional routine. The bundle is organized around four axes: readiness (available resources and algorithm posters), recognition (explicit screening triggers), response (parallel execution A–E and then F–G, always with structured communication), and learning (simulation, audit, and regular debriefings).
Although conceived for eclampsia, the model is applicable to other scenarios of maternal instability, including when diagnosis is not yet established at admission. The sequence helps quickly identify critical determinants and guide immediate actions. In obstetric trauma, ATLS remains the reference,
25 but ABCDEFG complements it, adapting to pregnancy particularities. In clinical emergencies such as postpartum hemorrhage, puerperal sepsis, and acute respiratory failure, the mnemonic organizes approach and standardizes language among teams, reducing omissions and communication failures.
Beyond operational benefit, there is educational potential: mnemonics enhance knowledge retention and safe execution of procedures, while structured protocols encourage multiprofessional communication and reduce errors due to fragmented care, a major factor in adverse outcomes.
Final considerationsMore than three decades after the Eclampsia Trial established MgSO₄ as the standard therapy for prevention and treatment of seizures, serious clinical practice failures persist. In many settings, women continue to die not from lack of scientific evidence, but from preventable failures in its application: failure to administer the drug when clearly indicated, dosing errors, absence of clinical monitoring after infusion, and unacceptable delays in treatment initiation.
These findings highlight that robust scientific evidence alone is insufficient: it must be translated into simple, applicable, reproducible protocols that reduce variability, guide rapid decisions, and support communication among teams under extreme pressure. In this context, we propose the ABCDEFG mnemonic—an obstetric adaptation inspired by ATLS that organizes care logic, prioritizes steps, and creates a common language for critical situations. It is not an isolated teaching exercise but a concrete strategy to save maternal and fetal lives, translating consolidated knowledge into safe, agile, and reproducible clinical practice.
References1. Rede Brasileira de Estudos sobre Hipertensão na Gravidez (RBEHG). Pré-eclâmpsia: Protocolo Assistêncial 2025. São Paulo: RBEHG; 2025. [access in 2025 Set 11]. Available from:
https://rbehg.com.br/wp-content/uploads/2025/04/Protocolo-RBEHG-2025-PDF-2.pdf2. Abalos E, Cuesta C, Grosso AL, Chou D, Say L. Global and regional estimates of preeclampsia and eclampsia: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2013; 170 (1): 1–7.
3. Say L, Chou D, Gemmill A, Tunçalp Ö, Moller AB, Daniels J,
et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014; 2 (6): e323–33.
4. World Health Organization (WHO). WHO recommendations for prevention and treatment of pre‑eclampsia and eclampsia. Geneva: WHO; 2011. [
Internet]. [access in 2025 Set 11]. Available from:
https://www.who.int/publications/i/item/97892415483355. Sibai BM. Diagnosis, prevention, and management of eclampsia. Obstet Gynecol. 2005; 105 (2): 402–10.
6. Bartal MF, Sibai BM. Eclampsia in the 21
st century. Am J Obstet Gynecol. 2022; 226 (2S): S1237-53.
7. Ramos JGL, Martins‑Costa SH, Sass N. Eclampsia in Brazil in the 21
st century. Rev Bras Ginecol Obstet. 2022; 44 (7): 637-9.
8. Katz L, Haddad S, Coutinho I, Parpinelli MA. Atendimento inicial à eclampsia. São Paulo: Federação Brasileira das Associações de Ginecologia e Obstetrícia (FEBRASGO); 2018. [
Internet]. [access in 2025 Set 11]. Available from:
https://www.febrasgo.org.br/pt/noticias/item/329-atendimento-inicial-a-eclampsia9. Flávio‑Reis VHP, Pessôa-Gonçalves YM, Barbosa AC, Desidério CS, Rodrigues WF, Oliveira CJF. Maternal deaths caused by eclampsia in Brazil between 2000 and 2021. Rev Bras Ginecol Obstet. 2024; 46: e‑rbgo65.
10. The Magpie Trial Collaborative Group. Do women with pre‑eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomised placebo‑controlled trial. Lancet. 2002; 359 (9321): 1877‑90.
11. Duley L, Gülmezoglu AM, Henderson‑Smart DJ, Chou D. Magnesium sulphate and other anticonvulsants for women with pre‑eclampsia. Cochrane Database Syst Rev. 2010; 11: CD000025.
12. Ambia AM, Wells CE, Yule CS, McIntire DD. Fetal heart rate tracings associated with eclamptic seizures. Am J Obstet Gynecol. 2022; 227 (4): 622.e1‑622.e6.
13. Barros JF, Amorim MM, Costa DG, Katz L. Factors associated with severe maternal outcomes in patients with eclampsia in an obstetric intensive care unit:a cohort study. Medicine. 2021; 100 (38): e27313.
14. Mushambi MC, Kinsella SM, Popat M, Swales H, Ramaswamy KK, Winton AL,
et al; Obstetric Anaesthetists' Association; Difficult Airway Society. Obstetric Anaesthetists' Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics. Anaesthesia. 2015; 70 (11): 1286‑306.
15. Frerk C, Mitchell VS, McNarry AF, Mendonça C, Bhagrath R, Patel A,
et al. Difficult Airway Society 2015 guidelines for unanticipated difficult intubation in adults. Br J Anaesth. 2015; 115 (6): 827‑48.
16. Silva WA, Pinheiro AM, Lima PH, Malbouisson LMS. Renal and cardiovascular repercussions in preeclampsia and impact on fluid management. Braz J Anesthesiol. 2021; 71 (4): 421‑8.
17. The Eclampsia Trial Collaborative Group. Which anticonvulsant for women with eclampsia? Evidence from the Collaborative Eclampsia Trial. Lancet. 1995; 345 (8963): 1455‑63.
18. Zuspan FP. Treatment of severe preeclampsia and eclampsia. Clin Obstet Gynecol. 1966; 9 (4): 954‑72.
19. Pritchard JA, Cunningham FG, Pritchard SA. The use of the magnesium ion in the management of eclamptogenic toxemias. Surg Gynecol Obstet. 1955; 100 (2): 131‑40.
20. Sibai BM, Graham JM, McCubbin JH. A comparison of continuous intravenous and intramuscular magnesium sulfate regimens in preeclampsia. Am J Obstet Gynecol. 1984; 150 (6): 728‑33.
21. Diaz V, Long Q, Oladapo OT. Alternative magnesium sulphate regimens for women with pre‑eclampsia and eclampsia. Cochrane Database Syst Rev. 2023; 10 (10): CD007388.
22. Beyuo TK, Lawrence ER, Kobernik EK, Oppong SA. A novel 12‑hour versus 24‑hour magnesium sulfate regimen in the management of eclampsia and preeclampsia in Ghana (MOPEP Study): a randomized controlled trial. Int J Gynaecol Obstet. 2022; 159 (2): 495‑504.
23. Shaheen RS, Ismail RA, Salama EY, Korini SM, Elsaeidy AS. Efficacy and safety of 12‑hour versus 24‑hour magnesium sulfate in the management of pre‑eclampsia and eclampsia:a systematic review and meta‑analysis. BMC Womens Health. 2024; 24: 421.
24. Shennan A, Duley L, Magee L, Hall D, Brown M, Chappell L,
et al. FIGO good practice recommendations on magnesium sulfate administration for pre‑eclampsia and eclampsia. Int J Gynaecol Obstet. 2021; 152 (1): 133‑5.
25. Wu N, Li W, Huang R, Jiang H. Effect of simulation‑based training workshop on obstetric emergency team collaboration and communication: a mixed study. Front Med (Lausanne). 2024; 11: 1282421.
26. Committee on Trauma. Advanced Trauma Life Support (ATLS). 11
th ed. Chicago: American College of Surgeons; 2025.
27. Seal SL, Ghosh D, Kamilya G, Mukherji J, Hazra A, Garain P. Does route of delivery affect maternal and perinatal outcome in women with eclampsia? A randomized controlled pilot study. Am J Obstet Gynecol. 2012; 206 (6): 484.e1‑484.e7.
28. Amorim MMR, Katz L, Ávila MB, Albuquerque RM, Souza AS, Faúndes A. Planned caesarean section versus planned vaginal birth for severe pre‑eclampsia. Cochrane Database Syst Rev. 2017; 10: CD009430.
29. Nomura RMY, Nakamura‑Pereira M, Brizot ML, Trapani A Jr, Paro HBM, Rosas CF,
et al. Misoprostol use in obstetrics: Number 6 – June 2023. Rev Bras Ginecol Obstet. 2023; 45 (6): 356‑67.
30. Amorim MMR, Katz L, Barros AS, Almeida TSF, Souza ASR, Faúndes A. Maternal outcomes according to mode of delivery in women with severe preeclampsia: a cohort study. J Matern Fetal Neonatal Med. 2015; 28 (6): 654-60.
Authors' contributionsAmorim MMR: conceptualization, methodology, project administration, supervision, manuscript writing, review, and editing. Katz L: conceptualization, validation, supervision; writing, review, and editing of the manuscript. Albuquerque MA: data curation, investigation, visualization, manuscript writing. Brito JC: investigation, validation, writing, review, and manuscript editing. Cunha ACMC, Souza ASR: visualization, writing, review, and editing. All authors approved the final version of the article and declare no conflicts of interest.
Data AvailabilityAll datasets supporting the results of this study are published within the article.
Received on October 10, 2025
Final version presented on October 15, 2025
Approved on October 16, 2025
Associated Editor: Lygia Vanderlei


 ; Anna Catharina Carneiro da Cunha1
; Anna Catharina Carneiro da Cunha1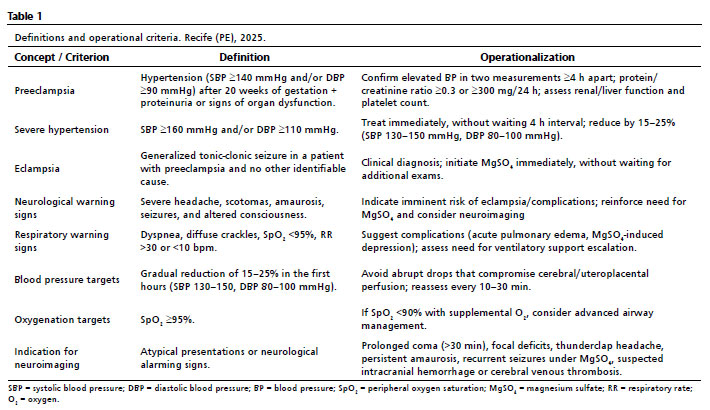






 Ler em português
Ler em português