ABSTRACT
OBJECTIVES: to summarize evidence on the quantitative parameters of skin-to-skin contact during hospitalization in newborns ≤32 weeks of gestational age that are associated with infant interactive skills.
METHODS: a systematic review was conducted, consulting databases in August 2024: BVS, Pubmed, CINAHL, Scopus, APA PsycNET, and Web of Science. Eligible studies were those focusing on mother-preterm infant interaction, evaluated by behavioral observation, that performed skin-to-skin contact during hospitalization, and analyzed infant interactive skills. Studies with indirect evaluation or those including children born above 32 weeks of gestational age were excluded. Data extraction and evaluation of methodological quality were performed independently by three reviewers using the QUIPS Tool and Quality Assessment Tool scales.
RESULTS: eight studies were included. The minimum time for the initiation of skin-to-skin contact was found to be 15 minutes of life for stable preterm infants. The duration varied from 1 to 2 hours/day, for approximately 15 days. Skin-to-skin contact was associated with improving contact initiative, responsiveness, reciprocity, gaze, vocalization, positive affect, and the infant's negative mood.
CONCLUSION: skin-to-skin contact needs to be included in the routines of neonatal units, as a tool to promote initial interaction between mother and infant.
Keywords:
Mother-infant relations, Mother-child interaction, Skin-to-skin contact, Kangaroo care, Preterm infant, Systematic review
IntroductionFor assistance to preterm newborns (PTNBs), Skin-to-skin contact (SSC) has advantages over the traditional method of care.
1-3 However, the literature could be more precise about the timing of SSC
4 and its benefits for the interaction within the mother-infant dyad.
5,6 Additionally, studies on SSC and mother-child relationships have different methodologies, which hinders evidence-based conclusions. Most studies focus only on maternal behavior,
7,8 such as the meta-analysis conducted by Karimi
et al.
9 These authors found a statistically significant association between the SSC and the mother-infant relationship. However, the studies included in the review considered only maternal reports and maternal interactive behavior.
The SSC, also known as Kangaroo Position or Kangaroo Mother Care, is defined as the maintenance of the PTNB, dressed only in a diaper, under the breast of one of the parents, in direct contact, and covered by a blanket.
10 Due to the inaccuracy of timing, the current consensus is for both to remain in this position for as long as they feel comfortable.
11 Thus, during clinical practice, the time of permanence in this position is often random or non-standardized.
SSC was proposed in Colombia in 1978 by the doctor and Professor Edgar Rey to solve the issue of overcrowding of neonatal units, a lack of incubators for PTNBs, and neonatal cross-infection, since many incubators were shared by more than one newborn.
12 Faced with the public health problem and the finding that the practice of SSC resulted in improved breastfeeding rates, a decrease in infant mortality rates, and reduced maternal abandonment, many studies were initiated after these findings.
13 In 1983, the United Nations Children's Fund (UNICEF) recognized SSC as one of the best practices in neonatal care, emphasizing the survival of newborns weighing less than 1500 grams.
12 In 2000, Brazil proposed SSC as a National Policy with broad coverage as a care method for low birth weight newborns.
11Studies have advanced and increasingly proved how SSC is an excellent strategy for promoting and maintaining breastfeeding,
14 weight gain and shorter hospital stay,
15 stabilization of maternal mental health,
16 extended child survival,
17 and favoring maternal approximation to the PTNB.
7,18 However, studies that analyze the infant's results concerning the mother-child interaction lack a robust methodological design. It is known so far that there are benefits to the mother-child dyad relationship. Nevertheless, little has been investigated about the characteristics of an infant interactive behavior, and there still needs to be a consensus on the time to perform SSC.
11 Due to the lack of methodological robustness, clinical practice sometimes becomes abstract and is not consistently integrated into the routine when the objective is to promote the relationship between the dyad.
Thus, this review aimed to summarize evidence on the quantitative parameters of skin-to-skin contact during hospitalization in newborns ≤32 weeks of gestational age that are associated with infant interactive skills.
MethodsThis paper is a systematic review conducted and presented following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA).
19 The protocol of this systematic review was registered in PROSPERO with registration number: CRD42020222006.
The research question was structured according to the PICO acronym: Population (P) was defined as all preterm infants born at ≤32 weeks of gestational age and evaluated the mother-child interaction between birth and 18 months of corrected age. The Intervention (I) was the quantitative parameter of SSC, either the onset time, duration, or frequency of SSC during hospitalization. The Control (C) was usual neonatal care. The outcome (O) was the infant's interactive skill with their mother.
Thus, we aimed to identify which SSC quantitative parameters (onset, duration, and frequency of SSC, among others) are measured in the literature in order to compare the results between experimental and observational studies. We also categorized the outcomes of SSC quantitative parameters and infant interactive developmental milestones up to eighteen months corrected age.
Furthermore, this review aims to support health practice, prevent harmful practices (such as unnecessary handling of a PTNB, as well as maternal fatigue in prolonged static positions), provide health professionals with updates, and promote alignment among hospitals that adopt this policy; to improve the understanding of the development of interactive skills in infants born preterm, thus favoring careful follow-up of infants born preterm at risk for child development disorders.
Source of informationThe following electronic databases were consulted: BVS (254 retrieved articles), Pubmed (397), CINAHL (282), Scopus (247), APA PsycNET (3), and Web of Science (103). The final search date for all databases was August 2024. The keywords and search terms combined in the investigation are described in the Supplementary Table 1.
Eligibility CriteriaOriginal scientific articles published on mother-preterm infant interaction between birth and 18 months corrected age were included, using a quantitative methodology with no restriction on language or publication period. For studies that used SSC as a synonym for skin-to-skin contact, studies that included performing SSC during hospitalization were considered eligible. For studies that analyzed infant interactive skills, the criterion was direct analysis through observation of infant behavior (e.g., videos or on-site evaluation), due to the possibility of detailing the collected data.
Studies based on interviews or questionnaires (indirect analysis), case report studies, expert opinions, animal experiments, reviews, theoretical essays, and research protocols were excluded. In addition, we excluded theses and dissertations, as well as those in which SSC was performed exclusively at home or in children born above 33 weeks of gestational age.
When multiple publications originated from the same cohort,
20-27 we opted for that publication that focused its results on the interaction.
21,25 In the case of clinical trials, unpublished results were sought. When necessary, the authors were contacted to clarify any doubts about the study.
Selection processAfter manually excluding duplicate publications, the initial screening was performed by reading titles, abstracts, and keywords. Three independent researchers completed the screening of the selected papers according to the eligibility criteria. A 98% inter-researcher agreement was reached. Disagreements were resolved in a consensus meeting with a fourth author.
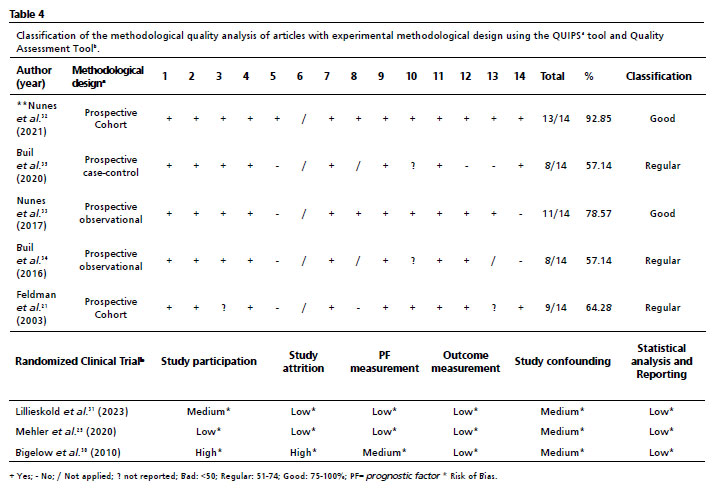
Assessment of methodological qualityThe quality of the articles was analyzed using instruments validated in the scientific literature. The methodological quality of the included experimental studies was assessed using the QUIPS Tool scale.
28 This tool comprises six domains (study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, statistical analysis, and reporting). Each domain is classified as having a high, moderate, or low risk of bias. No experimental studies were excluded, as all had a predominantly low or medium risk of bias.
The methodological quality of the included observational studies was assessed using the Quality Assessment Tool for Observation Cohort and Cross-Sectional Studies.
29 This tool provides for items to determine potential flaws in study or implementation methods, including sources of bias (e.g., patient selection, performance, attrition, and detection), confounding, study power, and the causal strength in the association between interventions and outcomes. Quality reviewers can select "Yes", "No" or "cannot be determined / not reported / not applicable" in response to each item. Two independent reviewers performed these analyses. In cases of disagreement, a third reviewer was consulted to assist in decision-making. No observational studies were excluded, as they presented a final score greater than 50%.
Data extraction processFor the data screening stage, a pre-defined form was used. This form collected the following information: author, year of publication, country, study objective, study type, mean birth weight and gestational age at birth, corrected age at which the interaction was evaluated, duration of the interaction video, interaction assessment instrument, sample size (sampling power), comparison group, SSC quantitative parameters (onset, duration, frequency), other measures of SSC, the inclusion of the Kangaroo Method, interaction constructs appreciated, primary results, study funding, conflicting interest, blinded observers, and limitations stated by authors.
The data extraction process was carried out by two authors and validated by the research team. Finally, the results were presented in table format. When data of interest were unavailable, the corresponding author of the selected study was contacted by email for further clarification.
ResultsAmong the 1,218 articles retrieved using search terms, 798 abstracts were reviewed after duplicate records were removed. Of these, eight studies met the eligibility criteria and demonstrated adequate methodological quality (Figure 1).
Of the articles that remained in this review, three utilized an experimental study design,
25,30,31 and five utilized an observational design.
21,32-35 All included articles evaluated the mother-child relationship. Only the Lilliesköld
et al.
31 study included the father in skin-to-skin contact, in addition to the mother. Mehler
et al.,
25 Bigelow
et al.,
30 Feldman
et al.,
21 Buil
et al.,
35 Lilliesköld
et al.
31 studies declared receiving financial support, unlike the other three.
32-34 Only six of these studies presented a clear and precise statement of the absence of author conflict of interest.
25,31-35The gestational age at birth of the newborns included in the studies ranged from 29 to 32 weeks. The mean birth weight ranged from 1,245.8±2.7 to 1,807.9±250.5. Most studies presented non-probabilistic samples, with the exception of three: Mehler
et al.,
25 which presented a sample calculation based on maternal sensitivity. However, the final sample collected was below the number of participants required for 80% power. Lilliesköld
et al.
31 which presented a sample calculation based on the main outcome variable of infant cardiorespiratory stability.
36 However, the initial sample with 90% power would require 100 participants, while the final sample was 71 mother-child dyads. Finally, Nunes
et al.,
32 presented a sampling power of 98% for a sample with 72 participants.
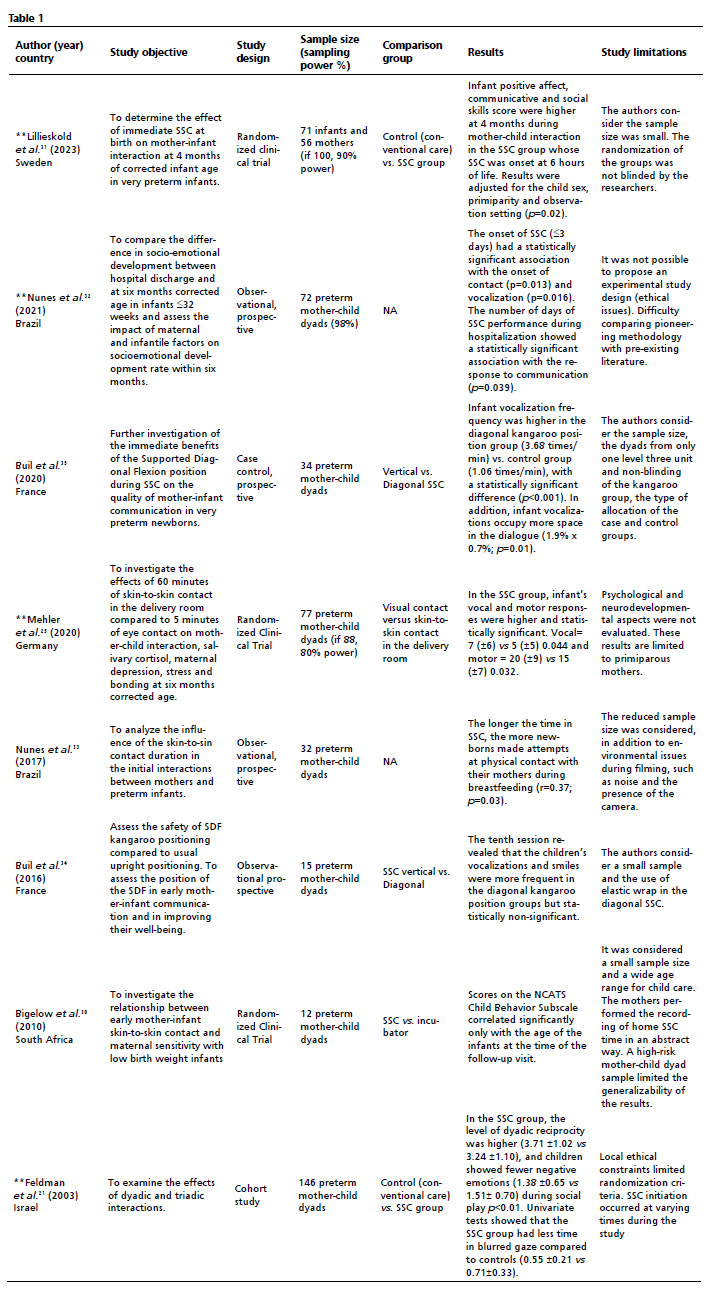
The age at which the mother-child interaction was assessed ranged from hospital admission to 12 months of corrected age. Additionally, SSC was compared to standard care (incubator), maternal eye contact at birth, and diagonal SSC. More details, such as objectives, populations, main results, and limitations, can be seen in Table 1.
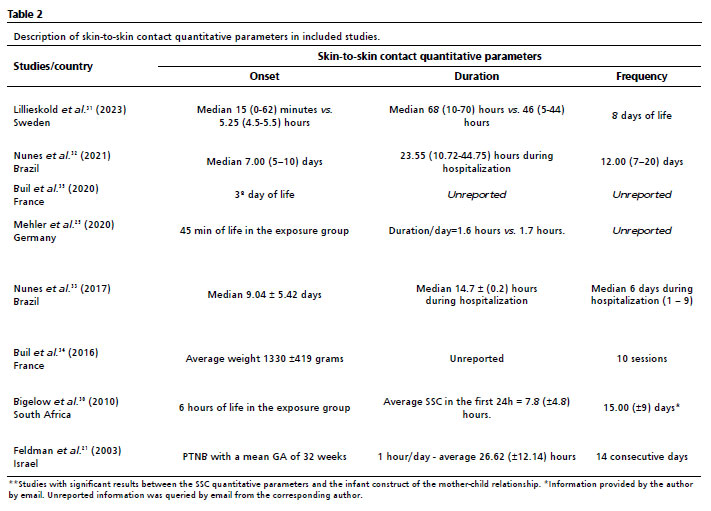
The studies varied in terms of the criteria for SSC onset. Lilliesköld
et al.,
31 Mehler
et al.
25 e Bigelow
et al.
30 considered the first hours of life. Buil
et al.
35 started on the third day of life, and Nunes
et al.
32,33 started SSC when the newborns were clinically stable. Buil
et al.
34 adopted the weight criteria, and Feldman
et al.
21 gestational age (Table 2). Among the studies that reported the duration and frequency of SSC, this relationship varied between approximately 1 and 7 hours/day of SSC.
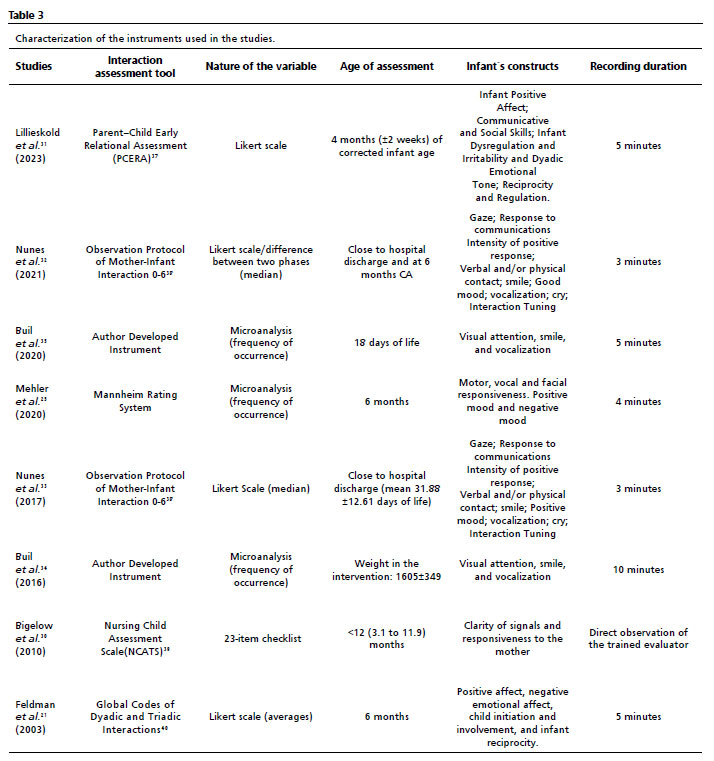
Regarding the constructs analyzed during the interaction, it is possible to categorize them as macro-analytic (infant state, positive and negative mood, dyadic conflict, and infant behavior such as responsiveness and the initiation of physical/verbal contact, reciprocity, mutuality and attunement between the dyad) And micro-analytic (which observes the gaze, smile, cry, and vocalization) (Table 3).
Among the constructs evaluated in this review, those that were repeated throughout the articles include responsiveness,
25,30,33 positive mood,
21,25,31,33 negative mood,
21,25,31 reciprocity,
21,31,33 initiation of physical/eye contact,
21,30,33 smile, gaze and vocalization.
32-35 The constructs that showed a statistically significant association with SSC were the onset of physical contact at hospital discharge,
33 infant positive affect at four months of corrected age,
31 infant vocalization,
25,32 responsiveness,
21,25,32 reciprocity, negative mood, and gaze at six months corrected age
21,25(Table 3). Table 4
compares the methodological quality of experimental and observational studies.
In this review, it was impossible to conduct a meta-analysis and heterogeneity analysis due to the variability of criteria for measuring SSC, the operationalization of mother-child interaction instruments, and the diversification of the ages addressed in the studies.
DiscussionThis study selected articles that associated SSC quantitative parameters and child interaction. We observed the early onset of SSC was possible from the first minutes of life to the first week, provided that the PTNBs were stable from a respiratory and hemodynamic point of view.
Regarding the quantitative parameters of SSC, the study by Nunes
et al.,
32 found high collinearity between the duration and frequency of SSC. However, these variables were not always reported or controlled in the other studies. Another issue was the randomization of the groups, as a control group not exposed to SSC would be ethically limited, given that SSC is a consolidated practice in many countries.
In summary, SSC was generally performed between 1 and 2 hours per day. We verified favorable associations with children's interactive behavior was possible as long as it was performed frequently for at least two weeks. However, there are facilitators and obstacles to realizing the SSC.
41 Among the facilitators, the most effective approach would be for the neonatal team to be trained and proactive in proposing and ensuring conditions for performing SSC with the mother and newborn.
42 On the other hand, some authors of the included studies cited the maternal absence during the hospital stay as a hindrance to controlling SSC performance after its initiation. Furthermore, Smith
et al.
43 also pointed out, in a systematic review, the difficulty of maternal permanence after her clinical discharge to ensure continuity of care for the PTNB in the neonatal unit. Thus, it is essential to emphasize the importance of infrastructure that facilitates skin-to-skin contact and socio-emotional support for the PTNB's family.
11However, PTNBs are at risk for neurodevelopmental challenges, particularly interactive,
44 linguistic,
45 and socioemotional development.
46 This is risk is due to social reasons, such as parents' removal during prolonged hospitalization in neonatal units,
47 biological factors , such as preterm birth itself, and environmental factors, such as exposure to excessive noise and light that can impair the PTNB's circadian cycle and, consequently, brain development.
48 This is in addition to exposure to medications, respirators, and painful and routine stimuli.
49Thus, this review found studies that associated SSC with improved contact initiative, responsiveness, reciprocity, gaze, vocalization, positive affect and children's negative mood. These behaviors should be well-established to ensure typical child development
50 in several areas, such as linguistic, psychological, socio-emotional, and motor skills.
Thereby, the contact initiative is the child's ability to act to engage the adult through vocalizations, smiles, looks, and physical approaches. Responsiveness, in turn, is the child's ability to be responsive and provide rewarding feedback to the adult. However, reciprocity refers to the coordinated interaction with behavioral and physiological signals that reflect the bidirectional attunement of one partner with the psychophysiological, cognitive, emotional, and behavioral state of the other.
51,52 These behaviors can occur through trans-modal communicative acts such as the look, vocalizations, smiles, and physical contact.
Interactive gaze has been present since birth.
53 Newborns already prefer to focus on human faces
53 and may be favored by physical proximity (30 cm from the mother's lap during breastfeeding, SSC
34,35). During social interaction, the gaze is part of the shared attention skill.
54 The absence of interactive gaze is one of the markers for the early investigation of pervasive developmental disorders.
55Vocalization is also present since birth, with a less complex structure when the newborn is on active alert.
56 Initially, as cooing, it will move on to vocalizations until babbling in this pre-linguistic phase. Success in the linguistic phase is determined by the number of positive auditory and proprioceptive experiences the newborn has had in the pre-linguistic phase.
57Negative mood is defined as crying, whimpering, negative vocalizations, and when the child demonstrates anger, restlessness, or discontent, and is measured by the number of episodes that occur during the observation of the infant's interactive behavior. Bruce
et al.58 observed that negative mood predicts children's expressive language. Therefore, despite causing discomfort in the caregiver responsible for the child, it is a necessary behavior and mediator of child satisfaction. Negative mood, with duration and punctual frequencies, will help the younger child to demonstrate discomfort. Thus, it will be up to the caregiver's sensitivity to interpret, attribute meaning and respond appropriately to the situation.
59 In this way, the negative mood is also considered a means of communication, especially for newborns, as it can mobilize people around them, resulting in actions.
60 Furthermore, negative mood participates in the capacity for emotion regulation, which consists of modulating the occurrence, duration, and intensity of internal feeling states.
61Limitations and future directionsThe main limitation for deeper comparative analysis lies in the methodological heterogeneity of the studies, specifically the use of diverse and non-standardized assessment tools for mother-infant interaction, many of which also lack cultural validation. There is also a clear knowledge gap regarding outcomes between 12 and 18 months of corrected age. To address this, future research should enhance methodological rigor, using representative samples and probabilistic models to reduce selection bias. Standardized measurement of SSC onset, duration, and frequency is essential to explore potential dose-response relationships. Comparative analyses between SSC subgroups (e.g., early vs. late initiation, longer vs. shorter duration) are recommended, along with adequate statistical control of confounding variables.
Clinical implicationsDespite methodological variability, evidence strongly suggests that SSC parameters—especially early initiation, frequency, and duration—positively influence mother-infant interaction in preterm infants. Improvements have been observed in key interactive behaviors, including contact initiation, vocalization, responsiveness, reciprocity, affect, and gaze. These findings underscore the importance of integrating SSC into neonatal care routines as a cost-effective strategy to promote early social development and bonding.
Final considerationsThe reviewed studies indicate that SSC can begin as early as 15 minutes post-birth in stable very preterm newborns, with typical sessions lasting two hours per day for approximately 15 days. Crucially, while only a few studies evaluated timing quantitatively, SSC was consistently associated with enhanced mother-infant interactive behaviors up to 12 months of corrected age. A significant knowledge gap remains in understanding outcomes between 12 and 18 months. Overall, SSC emerges as a promising, low-cost intervention to foster social interaction in preterm infants and warrants reinforcement as standard practice in neonatal care.
References1. Aho L, Metsäranta M, Lönnberg P, Wolford E, Lano A. Newborn Neurobehavior Is Related to Later Neurodevelopment and Social Cognition Skills in Extremely Preterm-Born Children: A Prospective Longitudinal Cohort Study. Front Psychol. 2021; 12: 710430.
2. Pathak BG, Sinha B, Sharma N, Mazumder S, Bhandari N. Effects of kangaroo mother care on maternal and paternal health: systematic review and meta-analysis. Bull World Health Organ. Jun. 2023; 10 1(6): 391-402G.
3. Kristoffersen L, Bergseng H, Engesland H, Bagstevold A, Aker K, Støen R. Skin-to-skin contact in the delivery room for very preterm infants: a randomised clinical trial. BMJ Paediatr Open. Mar 2023; 7 (1): e001831.
4. Forde D, Fang ML, Miaskowski C. A Systematic Review of the Effects of Skin-to-Skin Contact on Biomarkers of Stress in Preterm Infants and Parents. Adv Neonatal Care. 2022 Jun; 22 (3): 223-30.
5. Anderson GC, Moore E, Hepworth J, Bergman N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2003; (2): CD003519.
6. Seidman G, Unnikrishnan S, Kenny E, Myslinski S, Cairns-Smith S, Mulligan B,
et al. Barriers and enablers of kangaroo mother care practice: a systematic review. PLoS One.
2015; 10 (5): e0125643.
7. Kurt F, Kucukoglu S, Ozdemir A, Ozcan Z. The effect of kangaroo care on maternal attachment in preterm infants. Article. Nigerian J Clin Pract. 2020; 23 (1): 26-32.
8. Vittner D, Butler S, Smith K, Makris N, Brownell E, Samra H,
et al. Parent Engagement Correlates With Parent and Preterm Infant Oxytocin Release During Skin-to-Skin Contact. Adv Neonatal Care. Feb 2019; 19 (1): 73-9.
9. Karimi FZ, Abdollahi M, Khadivzadeh T, Yas A. Investigating the effect of kangaroo mother care on maternal-infant attachment: A systematic review and meta-analysis study. Curr Women's Health Rev. 2024; 20 (2): 50-60.
10. Organization World Health (WHO). Thermal protection of the newborn: a practical guide. Geneva: WHO; 1997. [access in 2020 Jul 20]. Available from:
https://www.who.int/publications/i/item/WHO_RHT_MSM_97.211. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Atenção Humanizada ao recém-nascido: Método Canguru. (Manual Técnico) Brasília (DF): Ministério da Saúde; 2017. [access in 2020 Jul 20]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/atencao_humanizada_metodo_canguru_manual_3ed.pdf12. Whitelaw A, Sleath K. Myth of the marsupial mother: home care of very low birth weight babies in Bogota, Colombia. Lancet. 1985 May; 1 (8439): 1206-8.
13. Sloan NL, Rojas EP, Stern C, Camacho LL, Team MIAS. Kangaroo mother method: randomised controlled trial of an alternative method of care for stabilised low-birthweight infants. Lancet. 1994; 344 (8925): 782-5.
14. Clarke-Sather AR, Compton C, Roberts K, Brearley A, Wang SG. Systematic Review of Kangaroo Care Duration's Impact in Neonatal Intensive Care Units on Infant-Maternal Health. Am J Perinatol. 2024 Jun; 41 (8): 975-87.
15. Cristóbal Cañadas D, Parrón Carreño T, Sánchez Borja C, Bonillo Perales A. Benefits of Kangaroo Mother Care on the Physiological Stress Parameters of Preterm Infants and Mothers in Neonatal Intensive Care. Int J Environ Res Public Health. 2022 Jun; 19 (12): 7183.
16. Boju SL, Gopi Krishna M, Uppala R, Chodavarapu P, Chodavarapu R. Short spell kangaroo mother care and its differential physiological influence in subgroups of preterm babies. J Trop Pediatr. 2012 Jun; 58 (3): 189-93.
17. Conde-Agudelo A, Díaz-Rossello JL. Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database Syst Rev. Aug 2016; (8): CD002771.
18. Mehrpisheh S, Doorandish Z, Farhadi R, Ahmadi M, Moafi M, Elyasi F. The Effectiveness of Kangaroo Mother Care (KMC) on attachment of mothers with premature infants. Eur J Obstet Gynecol Reprod Biol X. 2022 Aug; 15: 100149.
19. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffman TC, Milrow CD,
et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar; 372: n71.
20. Feldman R, Eidelman AI, Sirota L, Weller A. Comparison of skin-to-skin (kangaroo) and traditional care: parenting outcomes and preterm infant development. Pediatrics. 2002 Jul; 110 (1 Pt 1): 16-26.
21. Feldman R, Weller A, Sirota L, Eidelman AI. Testing a family intervention hypothesis: the contribution of mother-infant skin-to-skin contact (kangaroo care) to family interaction, proximity, and touch. J Fam Psychol. 2003 Mar; 17 (1): 94-107.
22. Ulmer Yaniv A, Salomon R, Waidergoren S, Shimon-Raz O, Djalovski A, Feldman R. Synchronous caregiving from birth to adulthood tunes humans' social brain. Proc Natl Acad Sci USA. 2021 Apr; 118 (14): e2012900118.
23. Feldman R, Rosenthal Z, Eidelman AI. Maternal-preterm skin-to-skin contact enhances child physiologic organization and cognitive control across the first 10 years of life. Biol Psychiatry. 2014 Jan; 75 (1): 56-64.
24. Hucklenbruch-Rother E, Vohlen C, Mehdiani N, Keller T, Roth B, Kribs A,
et al. Delivery room skin-to-skin contact in preterm infants affects long-term expression of stress response genes. Psychoneuroendocrinology. 2020 Dec; 122: 104883.
25. Mehler K, Hucklenbruch-Rother E, Trautmann-Villalba P, Becker I, Roth B, Kribs A. Delivery room skin-to-skin contact for preterm infants - a randomized clinical trial. Acta Paediatr. 2020 Mar; 109 (3): 518-26.
26. Heine E, Trautmann-Villalba P, Schoemig C, Hucklenbruch-Rother E, Kribs A, Mehler K. Delivery room skin-to-skin contact brings mother-child-interaction of preterm infants close to normal. Acta Paediatr. 2023 Nov; 112 (11): 2381-3.
27. Mehler K, Kribs A, Klein R, Heine E, Trautmann-Villalba P. Delivery room skin-to-skin contact for very preterm infants promotes mother-child interaction and bonding. Acta Paediatr. 2024 Jun; 113 (6): 1273-5.
28. Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013; 158 (4): 280-6.
29. National Heart Lung, and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. U.S. Department of Healthe Human Services. [
Internet]. [access in 2020 Jul 20]. Available from:
https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools30. Bigelow AE, Littlejohn M, Bergman N, McDonald C. The relation between early mother-infant skin-to-skin contact and later maternal sensitivity in South African mothers of low birth weight infants. Infant Ment Health J. 2010 May; 31 (3): 358-77.
31. Lilliesköld S, Lode-Kolz K, Rettedal S, Lindstedt J, Linnér A, Pike HM,
et al. Skin-to-Skin Contact at Birth for Very Preterm Infants and Mother-Infant Interaction Quality at 4 Months: A Secondary Analysis of the IPISTOSS Randomized Clinical Trial. JAMA Netw Open. 2023 Nov; 6 (11): e2344469.
32. Nunes CRN, Azevedo VMGO, Freitas NF, Rodrigues TM, Costa PR, Alves FL,
et al. Factors associated with the socioemotional development of preterm infants. Infant Behav Dev. 2021 Jul; 64: 101602.
33. Nunes CRN, Campos LG, Lucena AM,
et al. Relação da duração da posição canguru e interação mãe-filho pré-termo na alta hospitalar. Rev Paul Pediatr. 2017; 35: 136-43.
34. Buil A, Carchon I, Apter G, Laborne FX, Granier M, Devouche E. Kangaroo supported diagonal flexion positioning: New insights into skin-to-skin contact for communication between mothers and very preterm infants. Arch Pediatr. 2016 Sep; 23 (9): 913-20.
35. Buil A, Sankey C, Caeymaex L, Apter G, Gratier M, Devouche E. Fostering mother-very preterm infant communication during skin-to-skin contact through a modified positioning. Early Hum Dev. 2020 Feb; 141: 104939.
36. Linnér A, Westrup B, Lode-Kolz K,
et al. Immediate parent-infant skin-to-skin study (IPISTOSS): study protocol of a randomised controlled trial on very preterm infants cared for in skin-to-skin contact immediately after birth and potential physiological, epigenetic, psychological and neurodevelopmental consequences. BMJ Open. 2020 Jul; 10 (7): e038938.
37. Clark R. The Parent-child early relational assessment. Educ Psychol Measurement. Instrument and manual. Madison: University of Wisconsin Medical School, Department of Psychiatry; 1985.
38. Schermann-Eizirik L, Hagekull B, Bohlin G, Persson K, Sedin G. Interaction between mothers and infants born at risk during the first six months of corrected age. Acta Paediatr. 1997 Aug; 86 (8): 864-72.
39. Sumner G. NCAST caregiver/parent-child interaction teaching manual. Seattle: NCAST Publications; 1994.
40. Viaux-Savelon S, Leclere C, Aidane E, Bodeau N, Camon-Senechal L, Vatageot S,
et al. Validation de la version française du Coding Interactive Behavior sur une population d'enfants à la naissance et à 2 mois. Neuropsychiatrie de l'Enfance et de l'Adolescence. 2014; 62 (1): 53-60.
41. Lewis TP, Andrews KG, Shenberger E, Betancourt TS, Fink G, Pereira S,
et al. Caregiving can be costly: A qualitative study of barriers and facilitators to conducting kangaroo mother care in a US tertiary hospital neonatal intensive care unit. BMC Pregnancy Childbirth. 2019 Jul; 19 (1): 227.
42. Mathias CT, Mianda S, Ginindza TG. Facilitating factors and barriers to accessibility and utilization of kangaroo mother care service among parents of low birth weight infants in Mangochi District, Malawi: a qualitative study. BMC Pediatr. 2020 Jul; 20 (1): 355.
43. Smith ER, Bergelson I, Constantian S, Valsangkar B, Chan GJ. Barriers and enablers of health system adoption of kangaroo mother care: a systematic review of caregiver perspectives. BMC Pediatr. 2017 Jan; 17 (1): 35.
44. De Schuymer L, De Groote I, Striano T, Stahl D, Roeyers H. Dyadic and triadic skills in preterm and full term infants: a longitudinal study in the first year. Infant Behav Dev. 2011 Feb; 34 (1): 179-88.
45. McGowan EC, Vohr BR. Impact of Nonmedical Factors on Neurobehavior and Language Outcomes of Preterm Infants. Neoreviews. 2019; 20 (7): e372-84.
46. Norholt H. Revisiting the roots of attachment: A review of the biological and psychological effects of maternal skin-to-skin contact and carrying of full-term infants. Infant Behav Dev. 2020 Aug; 60: 101441.
47. Petteys AR, Adoumie D. Mindfulness-Based Neurodevelopmental Care: Impact on NICU Parent Stress and Infant Length of Stay; A Randomized Controlled Pilot Study. Adv Neonatal Care. 2018 Apr; 18 (2): E12-E22.
48. Neugebauer C, Oh W, McCarty M, Mastergeorge AM. Mother-Infant Dyadic Synchrony in the NICU Context. Adv Neonatal Care. 2022 Apr; 22 (2): 170-9.
49. Pineda R, Guth R, Herring A, Reynolds L, Oberle S, Smith J. Enhancing sensory experiences for very preterm infants in the NICU: an integrative review. J Perinatol. 2017; 37 (4): 323-32.
50. Montagna A, Nosarti C. Socio-Emotional Development Following Very Preterm Birth: Pathways to Psychopathology. Front Psychol. 2016; 7: 80.
51. Busuito A, Quigley KM, Moore GA, Voegtline KM, DiPietro JA. In sync: Physiological correlates of behavioral synchrony in infants and mothers. Dev Psychol. 2019 May; 55 (5): 1034-45.
52. Azhari A, Leck WQ, Gabrieli G,
et al. Parenting Stress Undermines Mother-Child Brain-to-Brain Synchrony: A Hyperscanning Study. Sci Rep. 2019 Aug; 9 (1): 11407.
53. Lavelli M, Stefana A, Lee SH, Beebe B. Preterm infant contingent communication in the neonatal intensive care unit with mothers versus fathers. Dev Psychol. 2022 Feb; 58 (2): 270-85.
54. Naoi N, Minagawa Y, Yamamoto JI, Kojima S. Infants' Prefrontal Hemodynamic Responses and Functional Connectivity During Joint Attention in an Interactive-Live Setting. Front Med Technol. 2022; 4: 821248.
55. Riddiford JA, Enticott PG, Lavale A, Gurvich C. Gaze and social functioning associations in autism spectrum disorder: A systematic review and meta-analysis. Autism Res. 2022 Aug; 15 (8): 1380-1446.
56. Carvalho MES, Justo JMRM, Gratier M, Tomé T, Pereira E, Rodrigues H. Vocal responsiveness of preterm infants to maternal infant-directed speaking and singing during skin-to-skin contact (Kangaroo Care) in the NICU. Infant Behav Dev. 11 2019; 57: 101332.
57. Serrat-Sellabona E, Aguilar-Mediavilla E, Sanz-Torrent M, Andreu L, Amadó A, Serra M. Sociodemographic and Pre-Linguistic Factors in Early Vocabulary Acquisition. Children (Basel). 2021 Mar; 8 (3): 206.
58. Bruce M, McFayden TC, Ollendick TH, Bell MA. Expressive language in infancy and toddlerhood: The roles of child temperament and maternal parenting behaviors. Dev Psychobiol. 2022 Sep; 64 (6): e22287.
59. Esposito G, Manian N, Truzzi A, Bornstein MH. Response to Infant Cry in Clinically Depressed and Non-Depressed Mothers. PLoS One. 2017; 12 (1): e0169066.
60. Von Dentz M. Expressões emocionais entre bebês na creche: revisão sistemática da literatura. Psicol Rev. 2019; 25 (1): 133-54.
61. Morris AS, Criss MM, Silk JS, Houltberg BJ. The impact of parenting on emotion regulation during childhood and adolescence. Child Dev Persp. 2017; 11 (4): 233-8.
AcknowledgmentWe would like to thank
J. Baeta Vianna Library - Health Campus of UFMG for their assistance with the bibliographic search.
Author's contributionNunes CRN: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, software, validation, visualization, writing – original draft, writing - review and editing.
Freitas NF: Formal analysis, data curation, validation, visualization, writing - review and editing.
Prates ABC and Silva CA: Data curation, investigation, validation, visualization, writing - review and editing.
Lemos SMA: Conceptualization, investigation, methodology, visualization, writing – review and editing.
Bouzada MCF: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, supervision, validation, visualization, writing – review & editing.
All authors approved the final version of the article and declared no conflict of interests.
Data AvailabilityAll datasets supporting the study are included in the article.
Received on September 7, 2024
Final version presented on September 13, 2025
Approved on September 16, 2025
Associated Editor: Kelly Abud


 ; Nathália Faria Freitas2
; Nathália Faria Freitas2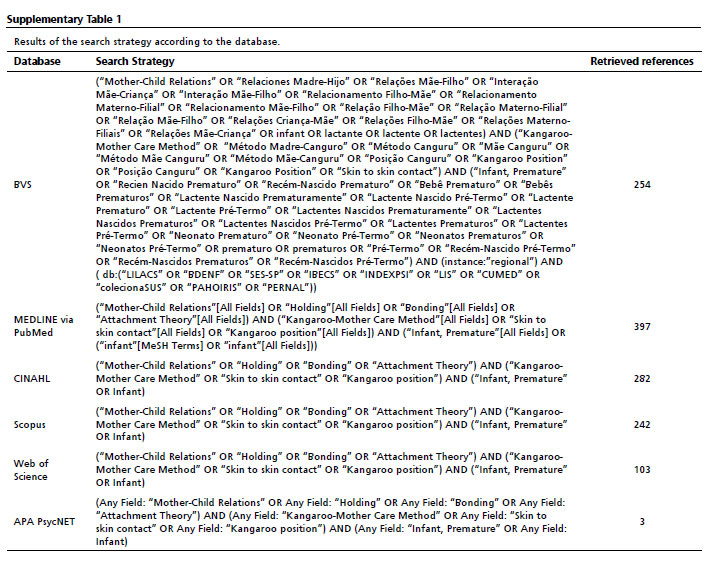






 Ler em inglês
Ler em inglês