ABSTRACT
OBJECTIVES: mapping evidences on risk and protective factors associated with early childhood development in Brazilian children.
METHODS: a scoping review was conducted. The databases used were: PubMed, Embase, BVS, Cochrane, APA PsycNet, ProQuest Library, and gray literature, searched on 04/23/2024, covering publications from 2015 to 2024. Searched descriptors: "Child preschool" OR Infant OR pediatric OR pediatric) AND ("child development" OR "mental health" OR "child guidance") AND ("Protective Factors" OR "Risk Factors"). Extracted information included the main author, year of publication, study design, study location, participants (number and age), and identified risk and protective factors. Out of a total of 6,812 documents, 24 were included.
RESULTS: a total of 43 risk factors and 15 protective factors in early childhood development were identified. The most frequently cited risk factors were socioeconomic vulnerability (n=10), low parental schooling (n=3), males (n=5) and teenage pregnancy (n=2). In contrast, the most cited protective factors included a supportive environment (n=3), higher family income (n=2), and higher maternal schooling (n=2).
CONCLUSION: early childhood development in Brazilian children is positively influenced by factors such as a supportive family environment, higher income and maternal schooling. On the other hand, low parental schooling, teenage pregnancy and males, negatively impact in this development.
Keywords:
Child development, Risk factors, Protective factors, Child behavior, Child health
RESUMO
OBJETIVOS: mapear as evidências sobre os fatores de risco e proteção associados ao desenvolvimento na primeira infância de crianças brasileiras.
MÉTODOS: realizou-se revisão de escopo. Bases utilizadas: PubMed, Embase, BVS, Cochrane, APA Psyc Net, ProQuest Library e literatura cinzenta em 23/04/2024, com publicações de 2015 a 2024. Descritores pesquisados: "Child preschool" OR Infant* OR pediatric OR paediatric) AND ("child development" OR "mental health" OR "child guidance") AND ("Protective Factors" OR "Risk Factors"). Foram extraídas informações sobre: autor principal, ano de publicação, delineamento, local do estudo, participantes (número e idade), fatores de risco e de proteção. Do total de 6812 documentos, 24 foram incluídos.
RESULTADOS: foram identificados 43 fatores de risco e 15 de proteção ao DPI. Vulnerabilidade socioeconômica (n=10), baixa escolaridade parental (n=3), sexo masculino (n=5) e gravidez na adolescência (n=2) foram os fatores de risco mais citados. Enquanto, ambiente adequado (n=3), maior renda familiar (n=2) e alta escolaridade materna (n=2) foram os de proteção.
CONCLUSÃO: o desenvolvimento na primeira infância de crianças brasileiras é influenciado favoravelmente por fatores como ambiente familiar adequado, maior renda e alta escolaridade materna, enquanto a baixa escolaridade parental, gravidez na adolescência e sexo masculino prejudicam este desenvolvimento.
Palavras-chave:
Desenvolvimento infantil, Fatores de risco, Fatores de proteção, Comportamento infantil, Saúde da criança
IntroductionEarly childhood comprises the period of life from birth to 72 months of age.
1 This phase is marked by the development of various skills that are essential for the development of more complex potentialities and abilities in adult life, such as autonomy.
2 This stage of life offers a window of opportunities for the future, since the brain has a high degree of plasticity, which contributes to a greater capacity for transformations due to the stimuli and experiences lived.
2Early childhood development (ECD) can be negatively impacted by various factors, including the economic vulnerability of families, depression, maternal stress and exposure to violence.
3 On the other hand, other factors can help full development: breastfeeding, the introduction to reading and storytelling in the first months, among others, generating benefits and favor adequate development in early childhood.
4The number of children at risk of not achieving their full development in low- and middle-income countries is approximately 43%, almost 250 million children under the age of five.
5 Recently, a project entitled "
Primeira Infância Para Adultos Saudáveis (PIPAS)" (Early Childhood for Healthy Adults), which covered 13 Brazilian State capitals, with a sample of 13,425 children aged zero to 59 months, found that 10.1% of the children aged zero to 35 months and 12.8% of the children aged 36 months and over were more likely not to reach their full potential development.
6 Concern with the ECD data has led several nations, including Brazil, to develop public policies and programs to promote child development.
To this end, Brazil has implemented programs such as the "
Marco Legal da Primeira Infância" (Lei nº 13.257/2016) (Legal Framework for Early Childhood -Law No. 13.257/2016), has brought advances in protecting Brazilian children's rights up to the age of six, establishing principles and guidelines for the formulation and implementation of public policies aimed at early childhood.
1 Likewise, the "
Primeira Infância Melhor (PIM) (Improved Early Childhood), an intersectoral public policy program of the State of Rio Grande do Sul, which aims to support the full development of children's physical, psychological, intellectual and social capacities from pregnancy to the age of five.
7Considering that delays and problems related to ECD affect children all over the world, it is essential to know which factors are related to it. Understanding and identifying the factors related to early childhood allows for the implementation of specific interventions and treatment plans for this age group.
8 In addition, there are economic reasons for investing in ECD: according to studies by economist James Heckman, for every dollar invested in programs for vulnerable children aged zero to five, there is a 13% return on investment per year.
9When searching the main databases on the subject, no up-to-date systematic or scope reviews were found on the subject of risk and protective factors for ECD in Brazilian children. Therefore, this study aims to map the evidence on the risk and protective factors associated with ECD in Brazilian children in their first six years of life.
MethodsThis scoping review was developed based on the methodology proposed by Arksey and O'Malley (2005) and Joanna Briggs, following the PRISMA-ScR guide guidelines.
10 Unlike the systematic review, the scoping review aims to map and explore literature in a broader way, providing an overview of the current perspective on a topic.
11 The scoping review protocol was registered on the Open Science Framework platform on August 30, 2021 (Risk and protection factors in early childhood development: a scoping review, public domain document). The guiding question for this study was: What are the risk and protective factors for ECD in the Brazilian context?
We included observational studies (cross-sectional, case-control and cohort) and intervention studies (clinical trials). We selected studies conducted with a Brazilian population aged zero to 72 months with typical development and published between 2015 and 2024, with no language restrictions. Bearing in mind that several domains make up human development, we included studies that assessed at least one of the following domains: cognitive, motor, language, neuropsychomotor and socio-emotional development.
12 We excluded articles in the format of preprints, abstracts without full papers, guidelines, case reports, books and systematic reviews (as they do not only include studies with the Brazilian population). We also excluded studies with clinical population groups, i.e. children diagnosed with atypical development (disorders, syndromes, diseases, etc.). Studies included with these children could hinder data analysis, overshadowing the results related to typical development, since they often have specific needs and characteristics.
To identify the studies, we searched the following electronic databases on April 23, 2024: PubMed, Embase, Cochrane Library, VHL, American Psychological Association (APA Psyc Net), ProQuest Library and Grey Literature. The search strategy included MeSH terms, synonyms, related terms and free terms related to ECD (Table 1). This search strategy was adapted for each electronic database. Duplicate studies were excluded.
The references identified in the electronic databases were exported to Rayyan software. Duplicate documents were removed, the titles and abstracts of the documents were evaluated and the evaluators' decision to include or exclude them was registered in this software.
The documents were selected independently in two stages by two previously trained researchers. In the first stage, the titles and abstracts of the documents were evaluated according to the eligibility criteria. Subsequently, the full texts of the documents considered potentially eligible in the screening stage were read and evaluated. Disagreements were resolved by consensus between the researchers.
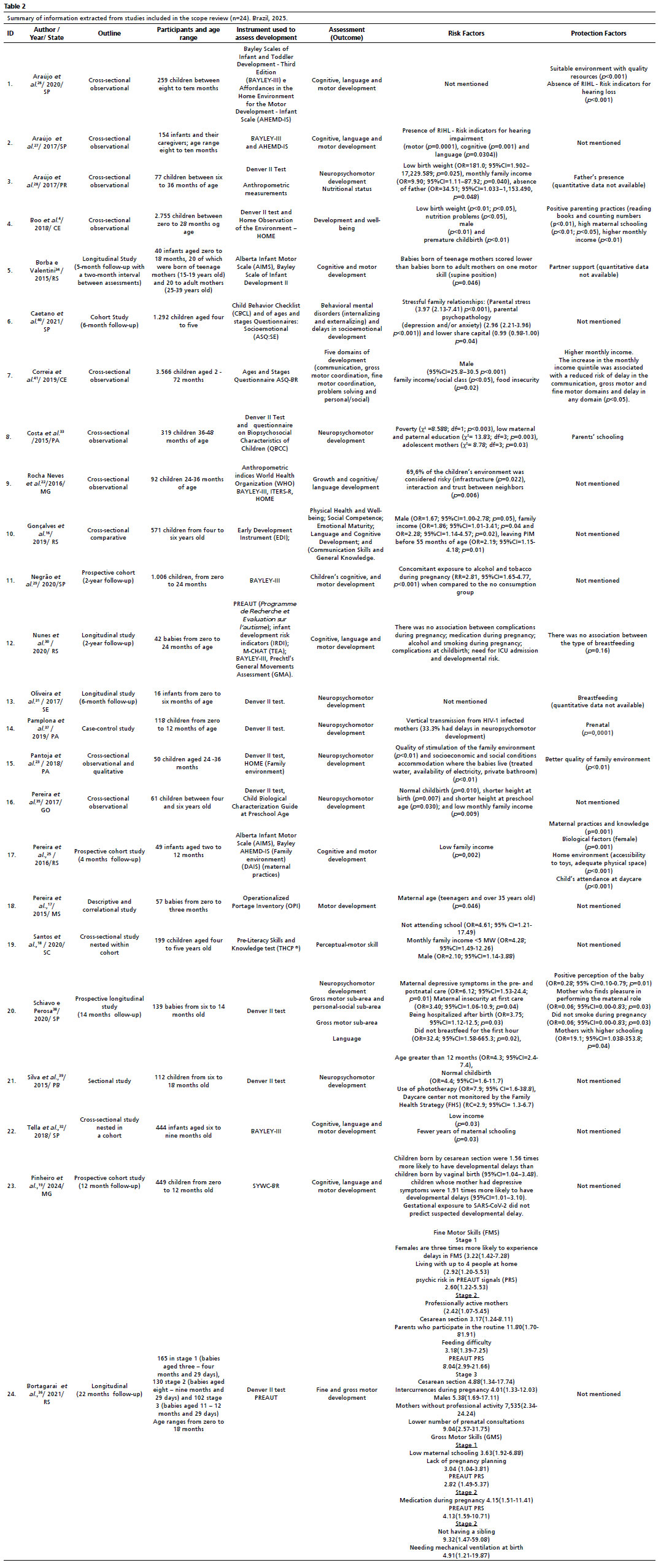
Data extraction from the included articles was carried out using a data collection form designed for this scoping review. The data was mapped independently by the reviewers. Data was extracted on the main author, the year and State in which the study was conducted. Study design, number of participants and age range, instruments used to assess child development, study outcome and finally risk and protective factors (Table 2).
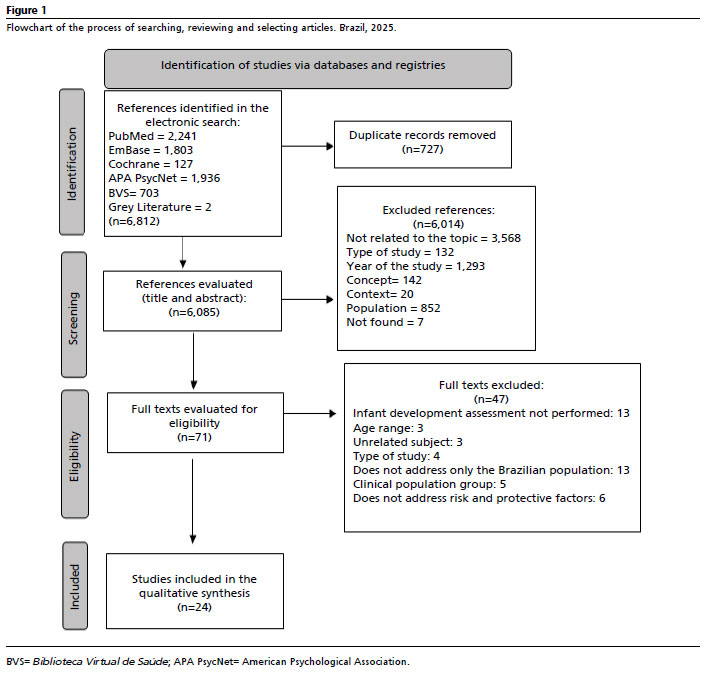
ResultsWe identified 6,812 documents in the electronic search (databases). After removing duplicates, the number declinded to 6,085. Of the articles, 6,014 were excluded based on the title and abstract, for the following reasons: not related to the topic (n=3,568), type of study (n=132), year of study (n=1,293), concept (n=142), context (n=20) and population (n=852). Seven articles were not found after searching institutional libraries, websites and trying to contact the authors. 71 studies were left and read entirety, of which 24 were included in this scoping review as they met the eligibility criteria. The reasons for excluding articles during the full-text reading stages are shown in Figure 1.
Characteristics of the articlesOf the 24 articles included, they were conducted in the States of São Paulo (n=6), Rio Grande do Sul (n=5), Pará (n=3), Ceará (n=2), Minas Gerais (n=2), Sergipe (n=1), Maranhão (n=1), Goiás (n=1), Mato Grosso do Sul (n=1), Santa Catarina (n=1), Paraíba (n=1), Paraná (n=1), one of which was conducted in two States, SP and MA. The cross-sectional design was the most frequent one (n=12), followed by longitudinal and cohort studies (n=9), case-control (n=1), descriptive correlational (n=1) and cross-sectional (n=1). The number of participants varied from 16 in a longitudinal study to 3,566 in a cross-sectional observational study. Participants' age ranged from zero to 72 months.
Assessment (outcome)A considerable number of the articles covered in this review used the term "neuropsychomotor development" as the study outcome (n=6). Of these, one study used nutritional status as an outcome in addition to neuropsychomotor development (n=1) and another study used the outcome "neuropsychomotor development" subdivided into: personal-social subarea, gross motor skills and language. Other studies had motor, cognitive and language development as outcomes (n=5) or only cognitive and language development (n=1). Some studies assessed only motor and cognitive development (n=3). Only motor development (n=1), fine and gross motor (n=1) and perceptual-motor skills (n=1). The term "development and well-being" was also used in one study (n=1). One study had mental and behavioral disorders and delayed socio-emotional development as outcomes (n=1). Communication, broad motor coordination, fine motor coordination, problem solving and personal/social development was used in one study as an outcome (n=1). Finally, one study assessed: physical health and well-being, social competence, emotional maturity, language and cognitive development and communication skills and general knowledge (n=1).
Developmental assessmentMost of the studies used the Developmental Screening Tests (Denver II) scale (n=10) and the Bayley Scales of Infant and Toddler Development - Third Edition (BAYLEY III) (n=8). The Denver II scale assesses the ability of children from zero to six years of age in four areas of child development: personal-social, fine motor-adaptive, gross motor and language. The Brazilian version of this instrument showed good psychometric properties: excellent reliability and good evidence of concurrent validity, sensitivity and specificity, making it a reliable and valid instrument.
12 The Bayley III scale is indicated for assessing five developmental domains in children between one and 42 months of age, involving: cognition, language, motor behavior, socio-emotional and adaptive, the scale was translated and cross-culturally adapted in Brazil and showed high convergent validity and good internal consistency.
13 The Alberta Infant Motor Scale (AIMS) instrument was used in two studies (n=2). The AIMS assesses the children's motor skills from ages zero to 18 months and has good consistency, content, criterion and constructed reliability. It is considered suitable for use with Brazilian children.
14 The Ages and Stages Questionnaire (ASQ-BR) was used in two studies (n=2). The ASQ-BR is a screening instrument for assessing development in the domains of communication, motor skills, problem solving and personal-social skills in children up to five years old. It has good internal consistency and psychometrically sound results.
15 The Early Development Instrument (EDI) scale (n=1) assesses various developmental domains and showed adequate psychometric properties and good test-retest reliability in all domains.
16 The
Inventário Portage Operacionalizado (IPO)(Operationalized Portage Inventory) is an instrument translated into Brazilian Portuguese and adapted for Brazilian children that assesses five areas of development
17 (n=1). The
Teste deHabilidades e Conhecimento Pré-Alfabetização (THCP) (Pre-Literacy Skills and Knowledge Test), a validated instrument that assesses the children's cognitive and motor skills at ages 4 to 7 years
18 and the Brazilian version of the Survey of Well-being of Young Children (SWYC-BR), an instrument that assesses the overall development of children aged 1 to 65 months, validated in Brazil
19 were used in one study each. Two studies used the Bayley scale and AIMS together to assess infant development. Two studies used the PREAUT scale (
Programme de Recherche et Evaluation sur l'autisme) in addition to the Bayley III and Denver II tests.
Growth assessmentSome studies not only assessed development, but also infant growth (n=2). For this, the anthropometric index according to the World Health Organization (WHO) was used, encompassing data such as height, weight, and among others, thus providing information on the children's nutritional status.
20Quality of the family environment and early childhood educationThe quality of the home environment was assessed using the Toddler HOME Inventory (IT)
21 (n=3),
4,22,23 and the Affordances in the Home Environment for the Motor Development - Infant Scale (AHEMD-IS)
24 (n=3).
25,26,27 In addition, one study assessed the quality of early childhood education using the Infant/Toddler Environment Rating Scale Revised (ITERS-R).
22Place of data collectionThe studies included in this review, data were collected at home (n=2), hospitals, outpatient clinics, maternity hospitals and specialized centers (n=5), schools and early childhood education city centers (n=8), others data were collected either at home and in schools or daycare centers (n=2), in basic health units (n=1), basic health units and home (n=1), home and maternity hospital (n=2), hospitals and basic health units (n=1), through telephone calls (n=1). Only one study did not mention where the data was collected (n=1).
Training professionals to administer the questionnairesThe Bayley III, Denver II and AIMS tests should be applied properly by trained professionals. In most of the studies in which these tests were applied, the professionals were trained or trained and calibrated (n=9).
22,23,25,26,28,29,30,31,32 Seven studies did not mention whether the professionals were trained (n=7).
17,18,27,33,34,35,36 Five studies did not mention who administered the questionnaire (n=5).
4,19,37,38,39 Questionnaires that did not involve the use of specific tests, such as the ASQ, OPI, THCP and EDI, were administered by trained researchers and answered by parents or guardians (n=4).
16,33,40,41 To assess anthropometric indices, trained researchers took the measurements (n=2).
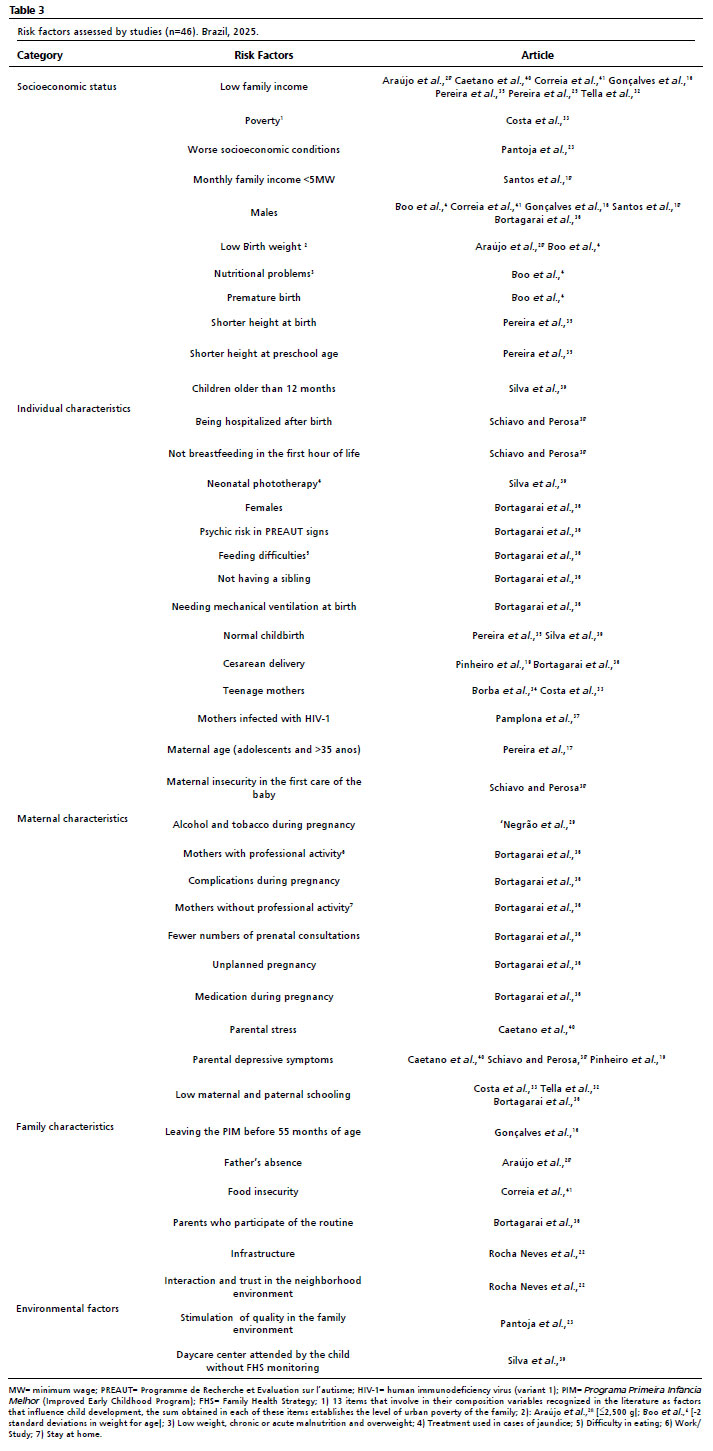
22,28Risk factorsForty-six risk factors were identified that compromise early childhood development. These factors were divided into: socioeconomic level, individual, maternal and family characteristics and environmental factors (Table 3). The most cited risk factor was vulnerable socioeconomic status (n=10), followed by individual characteristics, were males (n=5) and low birth weight (n=2). Some characteristics in relation to the child's mother were also considered a risk factor, including having had a normal/vaginal birth (n=2), having had a cesarean (n=2) and being a teenage mother (n=2). With regards to family characteristics, the most cited risk factors were depressive symptoms (n=3) and low maternal and paternal schooling (n=3). Some other risk factors mentioned in the included studies are related to individual characteristics such as: nutritional problems, lower height at birth, prematurity, not attending school, and among others. As for maternal characteristics: being a carrier of human immunodeficiency virus (variant 1) (HIV-1), consumed alcohol and tobacco during pregnancy, fewer prenatal consultations and unplanned pregnancy were also considered risk factors. Family factors were mentioned, such as the absence of the father and food insecurity, as well as environmental aspects, such as infrastructure and quality of stimulation in the family environment, which is related to the responsiveness of the caregiver, acceptance of the child, organization of the environment and materials for learning, parental involvement in the child's routine and variety of experiences, linked to the child's social contact.
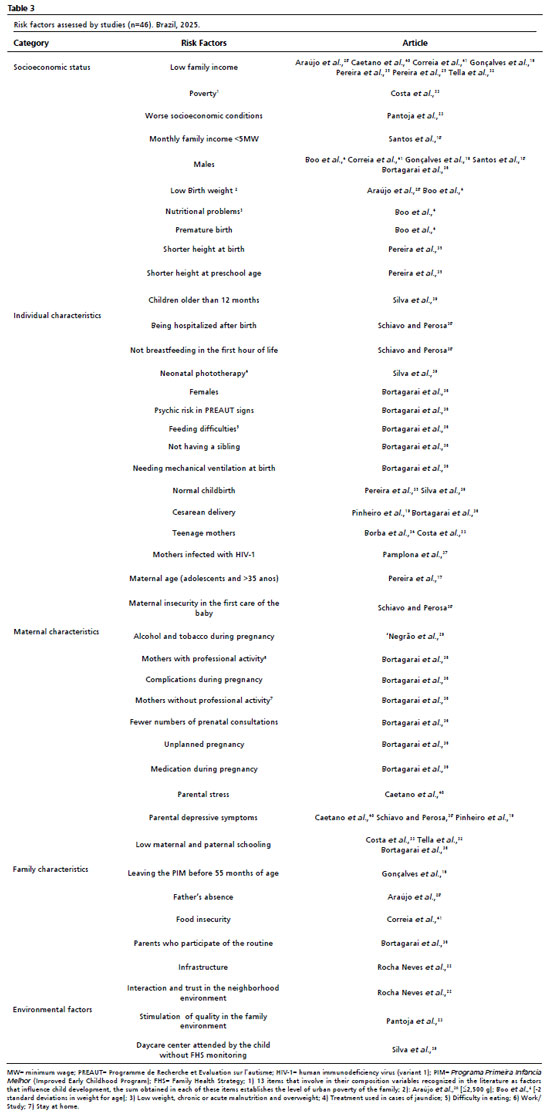
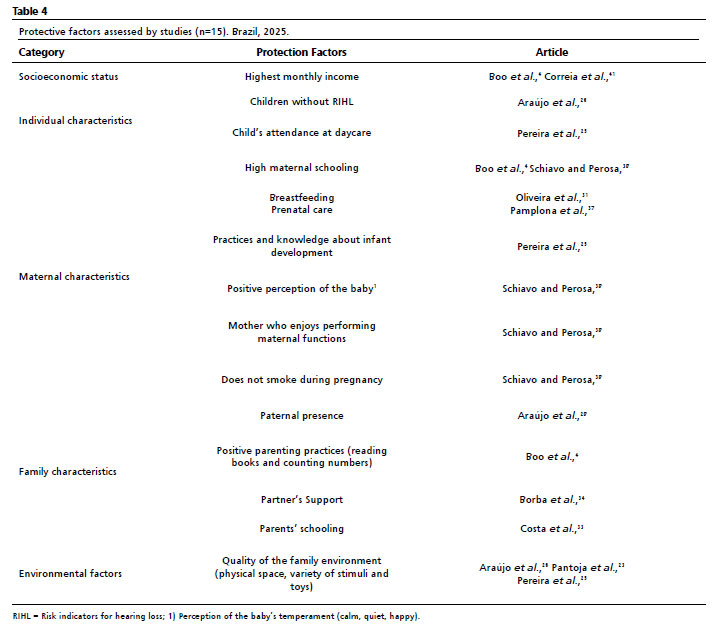
Fifteen protective factors were identified, which were also divided into: socio-economic level, individual, maternal and family characteristics and environmental factors (Table 4). Among them, the most cited was the quality of the family environment, which is related to the physical space (safe, adequate and large, involving type of floor, stairs, steps), the variety of stimuli (playing regularly, playing with the child, social contact) and the variety of toys (number of toys used, such as hanging toys, dolls, rocking chairs, balls) available to the child (n=3).
21,24 Having a higher monthly income was also considered a protective factor for early childhood development (n=2), as was high maternal schooling (n=2) and breastfeeding (n=1). Other factors such as a suitable environment, the presence of the father, positive parenting practices (reading books and counting numbers) and high maternal schooling were also cited (n=1).
DiscussionThis scoping review was carried out to map the evidence on risk and protective factors associated with ECD in Brazilian children in their first six years of life. Different outcomes were addressed in the included studies, ranging from neuropsychomotor development to mental, behavioral or developmental disorders. Infant development is broad and encompasses several areas and domains, such as motor, cognitive, personal-social and others.
12 Therefore, each study tends to address one or more of these dimensions according to its proposed objectives.
In order to achieve full development, it is essential that children develop skills in academic, behavioral and socio-emotional areas, and various factors, whether positive or negative, influence this process, covering aspects such as health, nutrition, safety and protection.
42 One of the risk factors for ECD that was addressed in the studies in a significant way and which involves the aspects mentioned, was in relation to socioeconomic status. Although the studies included use different methods to assess this, they all present evidence that ECD is influenced by the low socioeconomic status of families.
Poverty is closely linked to limited performance and the risk of not achieving full development in early childhood.
3,43 A study that assessed several specific brain structures linked to learning and educational functioning, including total gray matter, frontal lobe and temporal lobe, showed that the maturational delay of these structures can be influenced by the environmental circumstances of poverty.
3The interrelationship between low socioeconomic status and child development is complex because several variables act as mediators of this relationship, including limited access to resources, poor housing, nutritional deficiencies and lack of access to educational environments.
3,43 Cumulative exposure to risks can explain this relationship. Disadvantaged children are more exposed to adverse social, physical and environmental conditions.
3,43 They have less parental support, face higher levels of stress, greater family instability, greater exposure to violence and a lack of a support network when compared to advantaged children.
3,43 Reducing poverty seems to be a fundamental strategy for children to achieve their potential development, but this strategy is usually slow and gradual, so it is unlikely to bring about significant changes in a short period of time.
3,43Another risk factor pointed out in the studies was the male gender. According to a report by the
Organização das Nações Unidas para a Educação, a Ciência e a Cultura (UNESCO),
44 (Nations Educational, Scientific and Cultural Organization), girls in developing countries tend to perform better in terms of completion rates and learning outcomes. Studies have shown that boys have greater difficulty with reading, anti-social behavior, attention disorders, dyslexia and speech delays, while girls show better cognitive performance in measures of executive functioning and intelligence.
41,45 However, during the course of development, these differences between boys and girls can become insignificant.
45 Furthermore, it is important to note that of the articles included in this study, males were mentioned with other risk factors and not in isolation.
4,16,18,36,41 ECD is influenced by several factors, meaning that it is essential to avoid generalizations on this subject, thus recognizing its complexity.
According to the articles included in the study, low birth weight, vaginal and cesarean childbirth and nutritional problems are also risk factors for ECD.
4,36,28,35,39 This result corroborates the findings by Hillemeier
et al.
46 in which children with low birth weight had up to a three-fold increase in the risk of cognitive delay at 24 months of age. In addition, a meta-analysis also showed that children with very low birth weight have deficits in academic performance, attention problems and internalizing behavioral problems.
47In relation to the type of childbirth, children born by normal/vaginal childbirth were 4.4 times more likely to have altered development compared to children born by cesarean section in the study by Silva
et al.
39 However, in the study by Bortagarai
et al.
36 babies born by cesarean section were three times more likely to have delayed fine motor development compared to babies born by normal childbirth. The WHO recommends vaginal delivery as the preferred option, due to its benefits for both mother and child. According to Silva
et al.
39vaginal delivery can increase the risks for infant development, due to the conditions in which the delivery takes place and clinical misconduct, demonstrating the importance of gestational prenatal care and childbirth and puerperium care. Bortagarai
et al.
36 reported that the fact that children were born by cesarean section could be associated with other risk factors, such as perinatal anoxia, leading to microfunctional brain alterations. In Brazil, the main indications for scheduled cesarean section according to the Ministry of Health 2016 guidelines
48 include: prevention of vertical transmission of HIV; primary infection of the simple Herpes virus during the third trimester of pregnancy and women with three or more previous cesarean operations; labor and vaginal delivery is also not recommended for women with a longitudinal uterine scar from a previous cesarean operation, as there is greater impairment of the uterine musculature, increasing the risk of its rupture during labor. According to the data in this report, cesarean operations in Brazil reached 56.7%, 85% of which occurred in private services and 40% in public services. Although it is safe when carried out under medical indications, surgical delivery, when carried out without justification, can lead to unnecessary risks for the mother and baby.
48Finally, with regard to nutritional problems, delays in growth are indicative of chronic malnutrition and much of the literature associates malnutrition with developmental deficits.
49 It is known that good nutrition leads to good brain development, strengthens the immune system and improves the child's emotional and social health, adequate nutrition is considered an area of comprehensive necessary care for children to reach their full potential developmental
49 essential for early childhood development. Good prenatal care can minimize part of the effect of these risk factors.
The caregivers and adolescent mothers' mental health are also recognized as risk factors. During pregnancy and the postpartum period, women are more vulnerable, which favors the development or worsening of mental disorders such as depression and anxiety.
50 The effects of depressive symptoms on children's neurodevelopment are independent.
51 The effect of gestational depression on the child's development can be caused by hormonal changes such as an increase in cortisol levels,
52 causing damage to the fetal's brain development.
53 Exposure to prenatal stress not only affects children's physical development, but also causes poor psychomotor performance and more difficult behavior during the first ten years of life.
54 Depressed women are less likely to use recommended childcare practices and there is an impairment in the involvement with the child.
53 These results demonstrate the importance of maternal health in the overall, the child's well-being.
Maternal age was a factor that influenced children's development. Costa
et al.
33 relate to this delay of factors such as early sexual relations and motherhood, the presence or absence of a partner, and family neglect. In addition, social factors and a lack of maternal stimulation or interaction are also influential. In the study by Borba
et al.,
34 adolescent mothers had less time breastfeeding, a lower level of schooling, a lower employment rate and a lower income. In this study, the children of teenage mothers performed worse in one motor skill (supine position). However, adolescent motherhood was not a persistent risk factor for early childhood development.
34In order to gain a broad understanding of infant development, it is necessary to understand the environment in which the child develops.
55 In this sense, the family environment has been mentioned as both a risk factor and a protective factor. The environment inhabited by the child plays an essential role in their development, and this is the first environment provided by the family.
42,56,57 It is the duty of those responsible to provide basic needs, such as affection, food, care and support.
57 An environment with the availability of learning resources such as toys and books has been positively associated with children's cognitive development.
25 In these environments, children are encouraged to develop motor skills through playing.
33 Language, imagination, creativity and intellectual skills are also favored by stimuli from the family environment.
55Regarding protective factors for ECD, having a higher monthly income was also cited by the authors, confirming the importance of this factor in the context of the infant development. An alarming figure from the United Nations Children's Fund (UNICEF) in 2018,
58 showed that six out of ten Brazilian children and adolescents live in poverty and 32 million children (61%) live in vulnerable situations in Brazil. Disadvantaged children in developing countries who fail to achieve full development are less likely to become productive adults.
59 Therefore, these results reinforce the role of public policies and interventions that minimize, in some way, the effects of poverty on the child population. According to the
Atenção e Cuidado Integral (Comprehensive Care and Attention) model for children,
58 strategies need to focus on five interrelated and indivisible components of care: good health, adequate nutrition, safety and protection, responsive care, and learning opportunities.
This scoping review had the following limitations: only Brazilian studies were included. Therefore, the results should be interpreted with caution, since it is not possible to generalize countries that do not have the same cultural, economic and social characteristics. In addition, seven potentially eligible studies were not included. The documents were not available electronically or in institutional libraries, making it impossible to extract information and critically evaluate it. Finally, since the studies included several domains of development, the interpretation of the results becomes complex and requires careful analysis of the findings. It is essential that new studies be encouraged, with designs that allow us to understand the causality of certain risk and protective factors for ECD.
The evidence provided in this study showed that several factors influence ECD in Brazilian children, acting as both risk and protective factors. Children in greater economic vulnerability face greater threats that may compromise their full development. Thus, the necessity of public interventions aimed at socioeconomic improvements that ensure a developed environment that is more favorable to early childhood is highlighted. The training and qualification of professionals who work directly with children in early childhood can minimize risk factors and encourage protective factors.
References1. Brasil. Lei nº 13.257, de 8 de março de 2016. Dispõe sobre as políticas públicas para a primeira infância e altera a Lei nº 8.069, de 13 de julho de 1990 (Estatuto da Criança e do Adolescente). Brasília (DF): DOU 8 março de 2016. [access in 2024 Jun 18]. Available from:
https://www.planalto.gov.br/ccivil_03/_ato2015-2018/2016/lei/l13257.htm2. Comitê Científico do Núcleo Ciência Pela Infância (NCPI). Funções Executivas e Desenvolvimento na primeira infância: Habilidades Necessárias para a Autonomia. São Paulo, Brasil; 2016. [access in 2024 Mai 22]. Available from:
https://ncpi.org.br/wp-content/uploads/2018/08/Funcoes_executivas.pdf3. Hair NL, Hanson JL, Wolfe BL, Pollak SD. Association of child poverty, brain development, and academic achievement. JAMA. 2016; 169 (9): 822-9.
4. Boo FL, Mateus MC, Duryea S. Analysis of socioeconomic gradients in the development of children aged 0–3 years in Fortaleza, Northeastern Brazil. Rev Saúde Pública. 2018; 52: 84.
5. Lu C, Black MM, Richter LM. Risk of poor development in young children in low-income and middle-income countries: an estimation and analysis at the global, regional, and country level. Lancet. 2016; 4 (12): e916-22.
6. Ministério da Saúde (BR). Resumo Executivo – Projeto PIPAS 2022: Indicadores de desenvolvimento infantil integral nas capitais brasileiras. Brasília (DF): Ministério da Saúde; Outubro 2023. [access in 2024 Jun 18] Available from:
https://biblioteca.fmcsv.org.br/biblioteca/pipas-indicadores-de-desenvolvimento-infantil-integral-nas-capitais-brasileiras/7. Brasil. Lei nº 12.544, de 3 de julho de 2006. Institui o Programa Primeira Infância Melhor - PIM no Estado do Rio Grande do Sul e dá outras providências. Porto Alegre (RS): DOU 3 Julho de 2006. [access in 2024 Jun 18]. Available from:
https://www.al.rs.gov.br/legiscomp/asp/compstatutogeralcompilado.asp?txtLegislacao=12544&lista=18. Vitrikas K, Savard D, Bucaj M. Developmental delay: when and how to screen. Am Fam Physician. 2017; 96 (1): 36-43.
9. Garcia JL, Heckman JJ, Leaf DE, Prados MJ. Quantifying the life-cycle benefits of an influential early-childhood program. J Polit Econ. 2020; 128 (7): 2502-41.
10. Peters MD, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L,
et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020; 18 (10): 2119-26.
11. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010; 20: 5-69.
12. Santos JAT, Ayupe KMA, Lima ALO, Albuquerque KA, Morgado FFDR, Gutierres Filho PJB. Propriedades psicométricas da versão brasileira do Denver II: teste de triagem do desenvolvimento [Psychometric properties of the Brazilian version of the Denver II: developmental screening test]. Ciên Saúde Colet. 2022; 27(3): 1097-1106.
13. Madaschi V, Mecca TP, Macedo EC, Paula CS. Escalas Bayley-III de Desenvolvimento Infantil: Adaptação transcultural e propriedades psicométricas. Paidéia (Ribeirão Preto), 2016; 26 (64): 189-97.
14. Valentini NC, Saccani R. Escala Motora Infantil de Alberta: validação para uma população gaúcha [Alberta Infant Motor Scale: validation for a population from Rio Grande do Sul]. Rev Paul Pediatr. 2011; 29 (2): 231-8.
15. Filgueiras A, Pires P, Maissonette S, Landeira-Fernandez J. Psychometric properties of the Brazilian-adapted version of the Ages and Stages Questionnaire in public child daycare centers. Early Hum Dev. 2013; 89 (8): 561-76.
16. Gonçalves TR, Duku E, Janus M. Developmental health in the context of an early childhood program in Brazil: the "Primeira Infância Melhor" experience. Cad Saúde Pública. 2019; 35 (3): e00224317.
17. Pereira VA, Alves CF, Gonçalves MBL, Vieira MEA, Pereira KF, Pereira J. Investigação de fatores considerados de risco para o desenvolvimento motor de lactentes até o terceiro mês. Pensando Fam. 2015; 19 (2): 73-85.
18. Santos EMM, Gavioli LF, Lima MC, Silva RA, Simões VMF, Barbieri MA,
et al. Predictors of low perceptual-motor skills in children at 4-5 years of age. Rev Bras Saúde Mater Infant. 2020; 20 (3): 759-67.
19. Pinheiro GSMA, Lemos SMA, Martins IA, Januário GC, Cintra ML, Farias AVSR,
et al. Effects of SARS-CoV-2 gestational exposure and risk factors on neurodevelopment until 12 months: A prospective cohort study in Brazil. Early Hum Dev. 2024; 188: 105918.
20. World Health Organization (WHO), Multicentre Growth Reference Study Group. WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva: WHO; 2006; [access in 2024 Dez 3]. Available from:
https://www.who.int/publications/i/item/924154693X.21. Gabarra Macedo L, Carvalho Wendt Schultz N, Hering de Queiroz Â, Crepaldi MA, Moraes Cruz R. Reflexões sobre os parâmetros psicométricos do Inventário HOME versão Infant Toddler. Aval Psicol. 2010; 9 (2): 233-41.
22. Rocha Neves K, Morais LS, Teixeira RA, Pinto PAF. Growth and development and their environmental and biological determinants. J Pediatr. 2016; 92 (3): 241-50.
23. Pantoja APP, Souza AC, Lima DR, Silva AP, Costa LMG, Oliveira K,
et al. Effect analysis of environmental factors on the children's Amazon community neuropsychomotor development. Rev Bras Cresc Desenvolv Hum. 2018; 28 (3): 232-9.
24. Caçola PM, Gabbard C, Montebelo MI, Santos DC. The new affordances in the home environment for motor development - infant scale (AHEMD-IS): Versions in English and Portuguese languages. Braz J Phys Ther. 2015; 19 (6): 507-25.
25. Pereira KR, Valentini NC, Saccani R. Brazilian infant motor and cognitive development: Longitudinal influence of risk factors. Pediatr Int. 2016; 58 (12): 1297-1306.
26. Araujo DM, Cabrera Santos DC, Lima MCMP. Cognitive, language and motor development of infants exposed to risk and protective factors. Int J Pediatr Otorhinolaryngol. 2020; 138: 110353.
27. Araujo DM, Rovere NC, Lima MCMP. Desenvolvimento de lactentes com indicador de risco para deficiência auditiva e classificação ambiental. Rev Bras Cresc Desenvolv Hum. 2017; 27 (1): 49-55.
28. Araujo LBD, Mélo TR, Israel VL. Baixo peso ao nascer, renda familiar e ausência do pai como fatores de risco ao desenvolvimento neuropsicomotor. Rev Bras Cresc Desenvolv Hum. 2017; 27 (3): 272-80.
29. Negrão MEA, Rocha PRH, Saraiva MCP, Barbieri MA, Simões VMF, Batista RFL,
et al. Association between tobacco and/or alcohol consumption during pregnancy and infant development: BRISA Cohort. Braz J Med Biol Res. 2021; 54 (1): e10252.
30. Nunes SF, Chiquetti SEM, Moraes AB, Souza APR. Avaliação dos Movimentos Gerais de Prechtl (GMA) na detecção precoce de risco ao desenvolvimento. Fisioter Pesq. 2020; 27 (4): 347-55.
31. Oliveira TRDS, Souza LS, Dornelas R, Domenis DR, Silva K, Guedes-Granzotti RB. Associação entre o aleitamento materno, introdução alimentar e desenvolvimento neuropsicomotor nos primeiros seis meses de vida. Distúrb Comun. 2017; 29 (2): 262-73.
32. Tella P, Almeida RM, Silva VR, Lima LR, Santos AC, Oliveira D,
et al. Socioeconomic diversities and infant development at 6 to 9 months in a poverty area of São Paulo, Brazil. Trends Psychiatry Psychother. 2018; 40 (3): 232-40.
33. Costa EF, Silva MA, Oliveira AS, Lima M, Sousa GA, Rocha J,
et al. Perfil do desenvolvimento da linguagem de crianças no município de Belém, segundo o Teste de Triagem de Denver II. Rev CEFAC. 2015; 17 (4): 1090-1102.
34. Borba LSD, Valentini NC. Motor and cognitive development of infants of adolescent and adult mothers: longitudinal study. Rev Bras Cineantropom Desempenho Hum. 2015; 17: 438-49.
35. Pereira JF, Alves MB, Santos LMS, Lima SV, Silva JN, Costa IM,
et al. Influência dos fatores biológicos e socioeconômicos no desenvolvimento neuropsicomotor de pré-escolares. Saúde Pesq (Impr). 2017; 10 (1): 135-44.
36. Bortagarai FM, Moraes AB, Pichini FDS, Souza APR. Risk factors for fine and gross motor development in preterm and term infants. Codas. 2021; 33 (6): e20200254.
37. Pamplona M, Carvalho PM, Silva JF, Oliveira AK, Figueiredo E, Ferreira JA,
et al. Influence of exposure and vertical transmission of HIV-1 on the neuropsychomotor development in children. Rev Soc Bras Med Trop. 2019; 52: e20180263.
38. Schiavo RA, Perosa GB. Child Development, Maternal Depression and Associated Factors: A Longitudinal Study. Paidéia. 2020; 30: e3012.
39. Silva ÂCDD, Engstron EM, Miranda CTD. Factors associated with neurodevelopment in children 6-18 months of age in public daycare centers in João Pessoa, Paraíba State, Brazil. Cad Saúde Pública. 2015; 31: 1881-93.
40. Caetano SC, Ribeiro MVV, Askari MS, Sanchez ZM, Rosário MC, Perissinoto J,
et al. An epidemiological study of childhood development in an urban setting in Brazil. Braz J Psychiatry. 2020; 43 (1): 43-54.
41. Correia LL, Rocha HAL, Sudfeld CR, Rocha SGMO, Leite ÁJM, Campos JS,
et al. Prevalence and socioeconomic determinants of development delay among children in Ceará, Brazil: a population-based study. PloS One. 2019; 14 (11): e0215343.
42. Black MM, Walker SP, Fernald LCH, Andersen CT, DiGirolamo AM, Lu C,
et al. Lancet Early Childhood Development Series Steering Committee. Early childhood development coming of age: science through the life course. Lancet. 2017; 389 (10064): 77–90.
43. Walker SP, Wachs TD, Gardner JM, Lozoff B, Wasserman GA, Pollitt E,
et al. Child development: risk factors for adverse outcomes in developing countries. Lancet. 2007; 369 (9556): 145-57.
44. United Nations Educational, Scientific and Cultural Organization (UNESCO). Youth and skills: putting education to work. Understanding and challenging boys' disadvantage in secondary education in developing countries. Paris: UNESCO; 2012. [access in 2024 May 25]. Available from:
http://unesdoc.unesco.org/images/0021/002178/217868E.pdf45. Buczyłowska D, Ronniger P, Melzer J, Petermann F. Sex similarities and differences in intelligence in children aged two to eight: Analysis of SON-R 2-8 scores. J Intell. 2019; 7 (2): 11.
46. Hillemeier MM, Morgan PL, Farkas G, Maczuga SA. Perinatal and socioeconomic risk factors for variable and persistent cognitive delay at 24 and 48 months of age in a national sample. Matern Child Health J. 2011; 15 (7): 1001-10.
47. Aarnoudse-Moens CS, Weisglas-Kuperus N, Van Goudoever JB, Oosterlaan J. Meta-analysis of neurobehavioral outcomes in very preterm and/or very low birth weight children. Pediatrics. 2009 Aug; 124 (2): 717-28.
48. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas e Estratégicas. Parto cesariano: recomendações para a redução de cesáreas desnecessárias. Brasília (DF): Ministério da Saúde; 2016. [access in 2024 Jun 18]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/recomendacoes_reducao_cesariana_desnecessarias.pdf.49. Altafim ERP, Souza M, Teixeira L, Brum D, Velho C. O Cuidado Integral e a Parentalidade Positiva na Primeira Infância. Brasília (DF): Fundo das Nações Unidas para a Infância (UNICEF); 2018. [access in 2024 Jun 18]. Available from:
https://www.unicef.org/brazil/biblioteca50. Sousa MJA, Ribeiro EGM, Nogueira GM, Marques IA, Ferreira KG, Oliveira LST,
et al. Impact of maternal depression on child health. BJHR. 2021 Jul; 4 (4): 15409-22.
51. Koutra K, Chatzi L, Bagkeris M, Vassilaki M, Bitsios P, Kogevinas M. Antenatal and postnatal maternal mental health as determinants of infant neurodevelopment at 18 months of age in a mother-child cohort (Rhea Study) in Crete, Greece. Soc Psychiatry Psychiatr Epidemiol. 2013 Aug; 48 (8): 1335-45.
52. Rich-Edwards JW, Mohlajee AP, Kleinman K, Hacker MR, Majzoub J, Wright RJ,
et al. Elevated mid-pregnancy corticotropin-releasing hormone is associated with prenatal, but not postpartum, maternal depression. J Clin Endocrinol Metab. 2008 May; 93 (5): 1946-51.
53. Mulder EJ, Robles de Medina PG, Huizink AC, Van den Bergh BR, Buitelaar JK, Visser GH. Prenatal maternal stress: effects on pregnancy and the (unborn) child. Early Hum Dev. 2002; 70 (1-2): 3-14.
54. Conroy S, Marks MN, Schacht R, Davies HA, Moran P. The impact of maternal depression and personality disorder on early infant care. Soc Psychiat Epidemiol. 2010 Mar; 45 (3): 285-92.
55. Jones PC, Pendergast LL, Schaefer BA, Rasheed M, Svensen E, Scharf R; MAL-ED Network Investigators. Measuring home environments across cultures: Invariance of the HOME scale across eight international sites from the MAL-ED study. J Sch Psychol. 2017; 64: 109-27.
56. Associação Brasileira pelo Direito de Brincar (IPA Brasil). Artigo 31 da Convenção dos Direitos da Criança, o desenvolvimento e o direito de brincar. São Paulo: IPA Brasil; 2019,47. [access in 2024 Jun 18]. Available from:
https://biblioteca.fmcsv.org.br/biblioteca/artigo-31-da-convencao-dos-direitos-da-crianca-o-brincar/57. Souza Morais RL, Castro Magalhães L, Nobre JNP, Pinto PFA, Rocha Neves K, Carvalho AM. Quality of the home, daycare and neighborhood environment and the cognitive development of economically disadvantaged children in early childhood: A mediation analysis. Infant Behav Dev. 2021; 64: 101619.
58. Fundo das Nações Unidas para a Infância (UNICEF). Pobreza na infância e na adolescência, 13 de agosto de 2018. [access in 2024 Jun 18] Available from:
https://www.unicef.org/brazil/media/156/file/Pobreza_na_Infancia_e_na_Adolescencia.pdf59. Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B,
et al. Developmental potential in the first 5 years for children in developing countries. Lancet. 2007; 369 (9555): 60–70.
Authors' contribution: Martins IM: conception, study design, analysis, interpretation of data, writing of the manuscript, and critical and intellectual review of the manuscript. Corrêa-Faria P: analysis and critical and intellectual review of the manuscript. Santos IG, Mateus AC, Tavares NO: conception, study design, analysis and critical and intellectual review of the manuscript. Fernandez AMS: conception, study design, and critical and intellectual review of the manuscript. Perazzo MF: analysis and critical and intellectual review of the manuscript. Costa LR: conception and study design, acquisition, analysis and interpretation of data, critical and intellectual review of the study. All authors approved the final version of the article and declare no conflict of interest.
Received on June 22, 2024
Final version presented on February 7, 2025
Approved on February 10, 2025
Associated Editor: Karla Bomfim


 ; Matheus França Perazzo2
; Matheus França Perazzo2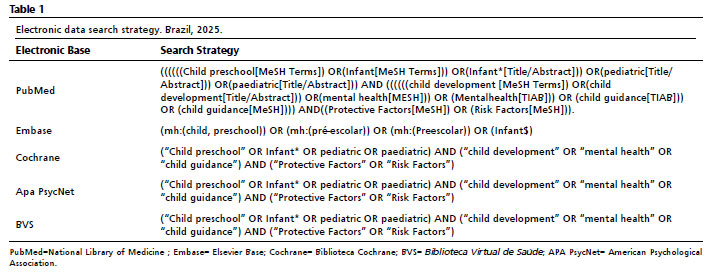






 Ler em português
Ler em português