ABSTRACT
OBJECTIVES: to analyze the relationship between breastfeeding within the first hour of life and the duration of exclusive and continued breastfeeding, as well as its impact on complementary feeding.
METHODS: a longitudinal study of mother-child pairs recruited from two public hospitals (2011-2016), with follow-up at six months and between three and five years. Comparisons of exclusive breastfeeding, continued breastfeeding, and complementary feeding were performed using the log-rank test, Kaplan-Meier curves, and Mann-Whitney test.
RESULTS: a total of 352 infants were followed, of whom 198 (56.25%) were breastfed within the first hour. Breastfeeding within the first hour was associated with exclusive breastfeeding at two months (p=0.024) but not with continued breastfeeding at one year (p=0.183). The probability of offering salt, sugar, and honey during complementary feeding was lower among children who were breastfeeding within the first hour (p=0.035). However, no significant difference was found in the introduction of ultra-processed (p=0.263), processed (p=0.162), and in natura (p=0.900) foods.
CONCLUSION: breastfeeding within the first hour was associated with exclusive breastfeeding at two months and lower probability of offering salt, sugar, and honey during complementary feeding.
Keywords:
Breastfeeding, Child nutrition, Infant nutritional physiological phenomena, Human milk, Newborn
RESUMO
OBJETIVOS: analisar a relação entre a amamentação na primeira hora de vida e a duração da amamentação exclusiva e continuada, bem como seu impacto na alimentação complementar.
MÉTODOS: estudo longitudinal com pares mãe-filho recrutados em dois hospitais públicos (2011–2016), com acompanhamento aos seis meses e entre três a cinco anos. As comparações de amamentação exclusiva, amamentação continuada e alimentação complementar foram realizadas utilizando o teste log-rank, curvas de Kaplan-Meier e o teste de Mann-Whitney.
RESULTADOS: um total de 352 bebês foi acompanhado, dos quais 198 (56,25%) foram amamentados na primeira hora de vida. A amamentação na primeira hora de vida foi associada à amamentação exclusiva aos dois meses (p=0,024), mas não com a amamentação continuada até um ano (p=0,183). A probabilidade de oferecer sal, açúcar e mel durante a alimentação complementar foi maior entre as crianças que não foram amamentadas na primeira hora de vida (p=0,035). No entanto, não houve diferença significativa na introdução de alimentos ultraprocessados (p=0,263), processados (p=0,162), e in natura (p=0,900).
CONCLUSÃO: a amamentação na primeira hora de vida foi associada à duração da amamentação exclusiva aos dois meses e a uma menor probabilidade de oferecer sal, açúcar e mel durante a alimentação complementar.
Palavras-chave:
Amamentação, Nutrição infantil, Fenômenos fisiológicos nutricionais do lactente, Leite humano, Recém-nascido
IntroductionBreastfeeding within the first hour of life, known as the 'golden hour', is recommended by the World Health Organization (WHO) due to evidence suggesting that this practice can reduce neonatal mortality and is positively associated with the duration of breastfeeding (BF), including exclusive breastfeeding (EBF).
1-3 Additionally, early initiation of sucking stimulates the production of oxytocin and prolactin by the mother's pituitary gland, increasing milk production and release, as well as providing immunological and psychosocial benefits for the baby, and strengthening the bond between mother and child. This practice also enhances the likelihood of the baby receiving colostrum, which is highly nutritious, easy to digest, rich in immunological properties, and essential for the maturation of the intestinal mucosa.⁴
Recent studies have also explored the relationship between breastfeeding within the first hour of life and the duration of both EBF and continued BF.⁵
,⁶ A cohort study found that children breastfed within the first hour of life consumed significantly fewer sweets, indicating a potential protective role of early breastfeeding on later dietary habits.⁵
The quality of foods introduced during complementary feeding (CF) is crucial, as it is associated with nutritional status and the prevention of overweight, obesity, and other diseases in both the short and long term.⁷
,⁸ Early introduction of ultra-processed foods tends to increase their consumption throughout childhood.⁹
Although there is growing evidence that breastfeeding within the first hour of life provides benefits for the duration of EBF and continued breastfeeding, the impact of early breastfeeding on CF remains a knowledge gap. While some recent studies suggest positive effects, further research is needed to solidify this understanding. Therefore, the aim of this study was to analyze the association between breastfeeding within the first hour of life and the duration of EBF, continued breastfeeding, and the quality of foods introduced during CF.
MethodsThis is a longitudinal observational study from the birth cohort Impact of Perinatal Environment Variations on Child Health in the First Five Years of Life (IVAPSA – Portuguese acronym), phases 1 and 2. In phase 1, mothers and infants were recruited between 2011 and 2016 in two public high-complexity hospitals in Porto Alegre, Rio Grande do Sul, Brazil. In phase 2, the same children were evaluated between 2017 and 2019 in the same city. The study protocol and baseline results have already been published.
10,11Eligible children were born at term in the GHC (Portuguese acronym from Conceição Hospital Group) and the HCPA (Portuguese acronym for Porto Alegre Teaching Hospital) without congenital malformations or other diseases. Women with a positive test for HIV, multiple pregnancies, with diabetes type 1 and 2 (regardless of diagnosis period), systemic arterial hypertension, who smoke, or those who had preterm deliveries (<37 weeks) were excluded, as well as infants with acute diseases, congenital birth defects, or small for gestational age. All mothers and infants were together in the maternity ward at the time of recruitment, with no health risks identified. Infants who missed follow-up in phases 1 or 2 were also excluded.
Data on EBF, BF, and CF were collected prospectively in phase 1, between 24 and 48 hours of postpartum at the maternity ward, followed by interviews conducted through home visits at 7, 15, and 90 days. Interviews were performed at home or at the clinical research center located at the HCPA at 30 and 180 days of the postpartum period. Retrospective data were collected in phase 2 through interviews and assessments at the Clinical Research Center of the HCPA of Porto Alegre, Rio Grande do Sul, Brazil.
Sociodemographic data (maternal age, race/color, education, occupation, marital status, family income, and child sex) were obtained through postpartum questionnaires administered at the participating hospitals.
Newborns were divided into two groups: Group 1: children breastfed within 60 minutes of birth; Group 2: children breastfed only after 60 minutes. Newborns were considered to have been breastfed within the first hour of life if they received any amount of breast milk within 60 minutes of birth.
12 To assess the duration of EBF, mixed feeding (MF), infant formula use, and CF, variables were collected asking whether the infant "received any other food or liquid," "when solids or liquids were introduced," and "if not breastfeeding, when it stopped." At 15, 30, 90, and 180 days, questions included whether the infant "receives breast milk," "if not, when it stopped," "receives breast milk exclusively," and "receives or received other types of milk," and if so, "when it was introduced." A questionnaire was used to gather data on the introduction of liquids and solid foods. Mothers were asked about the introduction of sugar, chocolate, honey, coffee, fruit, food porridge, industrialized soup, vegetables, legumes, meat, eggs, processed meats, stuffed wafers, sweet wafers, petit Suisse, chocolate, candy, snacks, gelatin, ice cream, fried foods, soda, natural juice, yogurt, and artificial juice.
13Liquid and solid foods introduced during complementary feeding were categorized according to the NOVA classification, as outlined in the Food Guide for the Brazilian Population.
12 Ultra-processed foods included chocolate milk, candy, lollipops, sweet biscuits (with or without filling), chocolate, bonbons, processed meats, gelatin, petit suisse cheese, soft drinks, salty snacks, and artificial juice. Natural or minimally processed foods included natural juice, eggs, offal, legumes, fruits, and meats. Culinary ingredients were categorized as sugar, salt, and honey, while processed foods included yogurt, canned goods and fried foods.
Parametric continuous variables were expressed in mean ± standard deviation (SD). Nonparametric continuous variables were expressed in the median and interquartile range. Categorical variables were expressed in absolute numbers and percentages. To compare the samples, the square-chi test was performed for categorical variables and Mann-Whitney test, for nonparametric continuous variables. For the analysis of the time of exclusive breastfeeding, breastfeeding and its relationship with the complementary food introduction, the log-rank test and Kaplan-Meier curves were used. For the analyses, a significance level of 5% (
p<0.05) and a 95% confidence interval were considered. The data were analyzed with the statistical program Statistical Package for the Social Sciences (SPSS) version 21.0.
The research was approved by research ethics committees of both HCPA and GHC, respectively, under the numbers 20110097 and 2011027 (Phase 1), and 20170107 (Phase 2).
ResultsThe study included 352 mother-infant pairs, with 198 infants (56.25%) breastfed within the first hour of life (Group 1) and 154 infants (43.75%) breastfed after the first hour (Group 2). White women were the majority in both groups, representing 60% of the sample, with no significant difference in self-reported race between the groups (
p=0.496). The mean maternal age was 26.3 ± 6.6 years, and the mean years of education was 9 ± 2 in both groups (
p=0.051). Breastfeeding within the first hour was associated with vaginal delivery (
p=0.001) and having a greater number of children (
p=0.004). Additionally, a greater number of prenatal visits was associated with not breastfeeding within the first hour of life (
p=0.017) (Table 1).
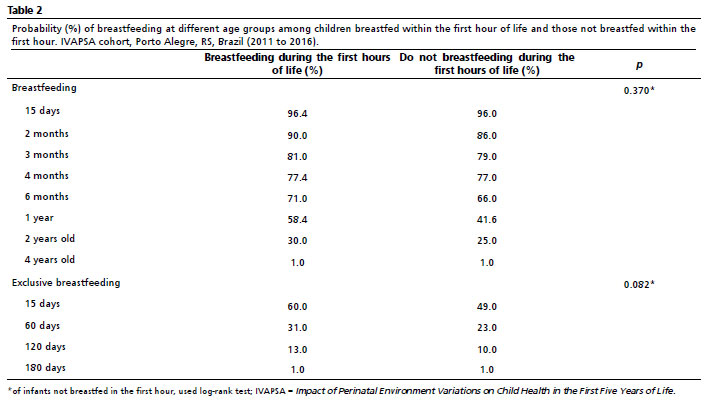
There was no significant difference between infants breastfed in the first hour and infants breastfed after the first hour regarding the time of EBF (
p=0.082) and time of BF (
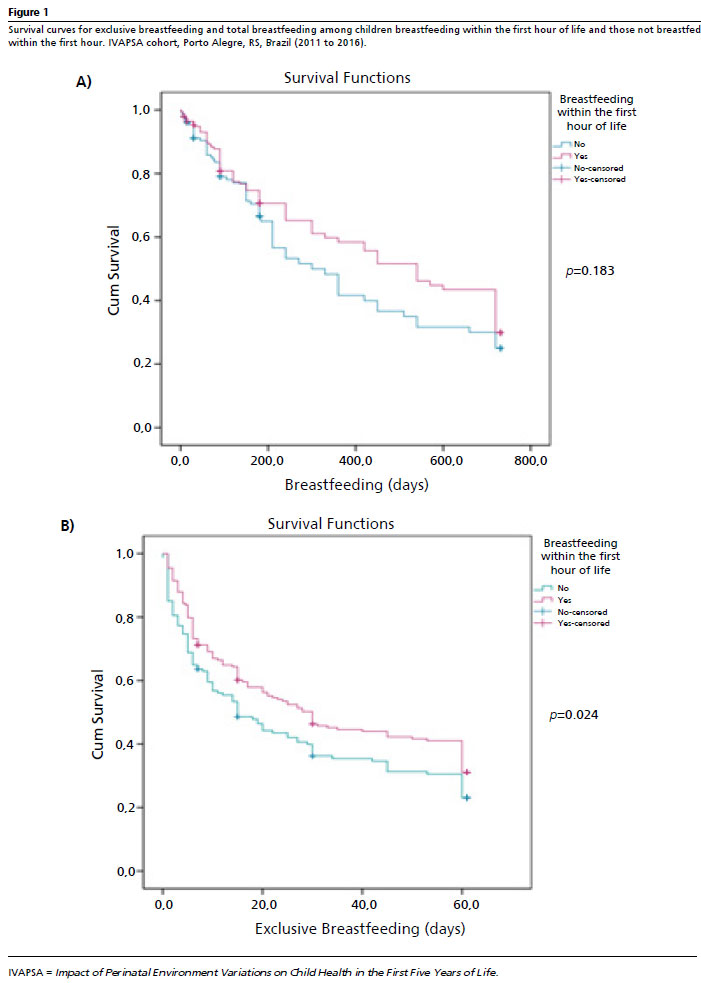
p=0.370) (Table 2). Figure 1 shows the survival curves for BF and EBF, indicating differences between children breastfed within the first hour and those breastfed later. Breastfeeding within the first hour of life was associated with exclusive breastfeeding at 2 months (
p=0.024) but not with continued breastfeeding at 1 year (
p=0.183).(Figures 1A and 1B).
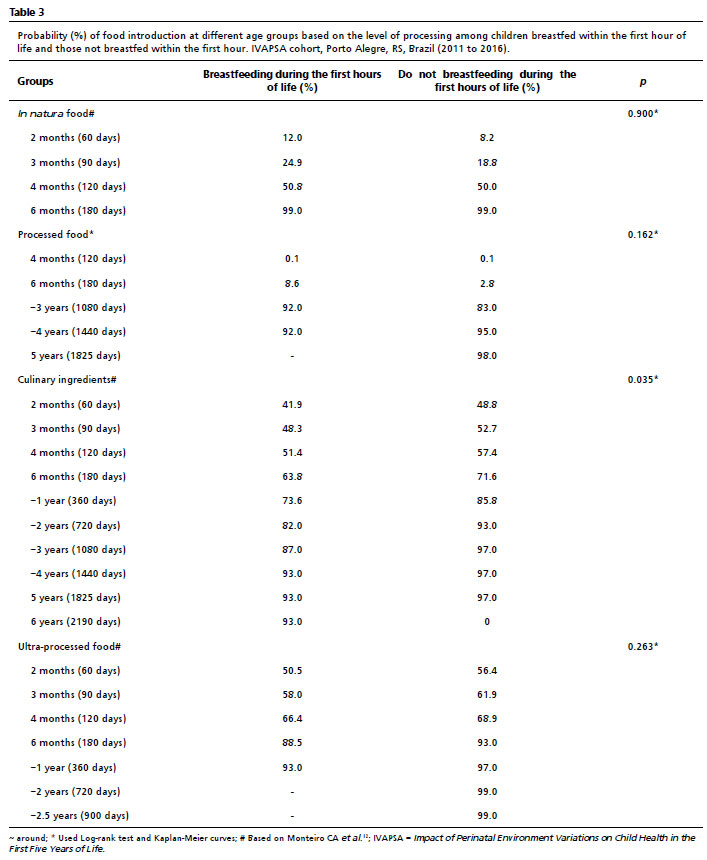
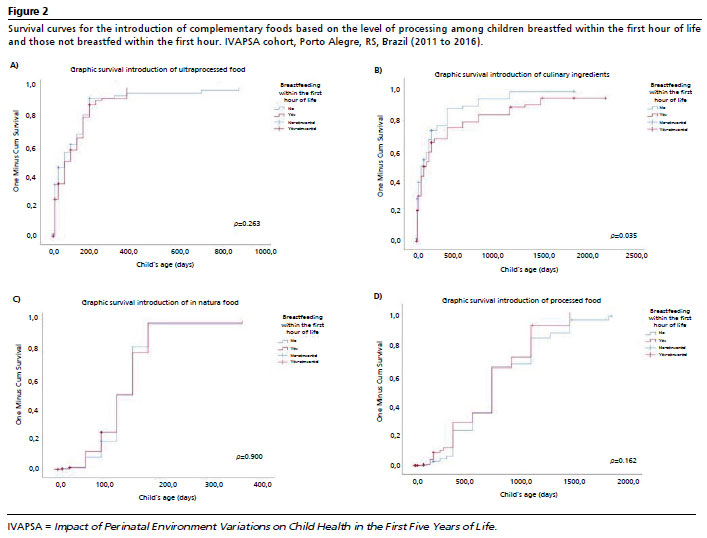
The probability of introducing complementary foods, based on their processing level (ultra-processed, processed,
in natura, and culinary ingredients), is presented in Table 3. The probability of introducing culinary ingredients was higher among children not breastfed in the first hour (
p=0.035). The introduction of other food groups was not associated with breastfeeding within the first hour. Figure 2 shows the survival curves for the introduction of complementary foods according to their processing level. Children not breastfed in the first hour had a higher probability of early introduction of culinary ingredients (
p=0.037) (Figure 2B).
DiscussionIn this study, breastfeeding within the first hour of life was associated with EBF at two months and a lower probability of introducing culinary ingredients, such as salt, sugar, and honey, during CF. Breastfeeding within the first hour of life was associated with maternal parity; mothers with more children were more likely to breastfeed within the first hour. Additionally, vaginal delivery and the number of prenatal visits were also associated with the practice of breastfeeding within the first hour of life.
The results also revealed a decline in breastfeeding and exclusive breastfeeding during the first year of life. Although the recommendation for exclusive breastfeeding is six months, we chose to evaluate at two months, as ENANI
14 data indicates that this is a critical age for the interruption of exclusive breastfeeding.
The probability of offering culinary ingredients during complementary feeding was higher among children who were not breastfed within the first hour. This result is supported by other studies that have demonstrated the protective role of breastfeeding within the first hour of life in shaping healthier feeding practices.
3-5Vaginal delivery was a protective factor for breastfeeding within the first hour of life, as was higher parity. This aligns with previous studies worldwide, which also reported an association between vaginal delivery and breastfeeding within the first hour of life.
15,16 Women who undergo cesarean section may experience pain and stress in the postpartum period.
17 In addition, children born via cesarean section are more likely to have respiratory distress syndrome.
18 These two factors could impair the onset of breastfeeding in the first hour of life. Thus, it is suggested that adherence to breastfeeding promotion and protection policies should be encouraged, emphasizing the importance of the multidisciplinary team and collaborative work among its members, ensuring quality care for the mother-newborn dyad during the first hour after birth.
The target prevalence for breastfeeding within the first hour of life, according to the WHO, is 70%.
1–3 In this study, more than half of the children were breastfed within the first hour. However, similar prevalence rates have been reported in other studies (43.5%; 74%).
18-20 This highlights that we are still far from the WHO's goals and underscores the need for awareness campaigns and education within communities and healthcare facilities. The WHO recommends that breastfeeding within the first hour of life should be protected and encouraged.
21 To promote breastfeeding in the first hour of life, it is also important to promote vaginal birth, as this has been associated with higher rates of breastfeeding within the first hour. For instance, a study in Tanzania showed an increase from 51% to 74% through educating pregnant women on the importance of colostrum and increasing their knowledge about the definition and timing of EBF.
22In this study, it was observed that women who did not breastfeed within the first hour of life attended a higher number of prenatal consultations. While the data do not allow for determining the cause of this association, factors such as gestational complications, greater adherence to medical follow-up, or differences in access to healthcare services may have influenced this finding. This relationship highlights the need for further studies to investigate the possible reasons that may impact the initiation of breastfeeding within the first hour of life. Other studies have demonstrated that access to information is crucial for the successful initiation of breastfeeding.
22,23 Therefore, it is essential to protect and promote breastfeeding by ensuring that guidance and support are provided during prenatal care by all healthcare professionals involved.
Breastfeeding within the first hour of life was associated with exclusive breastfeeding at two months. The majority of early weaning or breastfeeding interruptions occur within the first 90 days after birth, particularly during the second month of the child's life. This finding highlights the protective role of breastfeeding in the first hour, which helps prevent weaning during this critical period. As a key factor in supporting continued breastfeeding, the WHO recommends breastfeeding within the first hour of life. However, it is important to note that while early breastfeeding plays a protective role, it is not the only factor influencing breastfeeding duration. Other variables, such as birth weight, gestational age, maternal smoking, and education also play a significant role in breastfeeding outcomes.
24–26Breastfeeding within the first hour of life was not associated with a longer duration of breastfeeding throughout the first year of life. In both groups - those breastfed and not breastfed within the first hour - a significant decline in breastfeeding rates was observed. Several factors may contribute to the early interruption of breastfeeding, particularly socioeconomic factors such as maternal employment and income. In this study, mothers were recruited from public hospitals, the majority coming from low-income backgrounds. It is likely that the decline in breastfeeding rates is influenced by these socioeconomic factors.
Breastfeeding within the first hour of life was associated with a lower likelihood of introducing culinary ingredients, such as sugar, salt, and honey, during complementary feeding. A similar study also demonstrated the early introduction of liquids, honey, sugar, and sweets, and reported significantly lower consumption of sweets among children who were breastfed within the first hour of life.⁵ Although evidence supporting the protective role of breastfeeding in the first hour against inappropriate practices in complementary feeding is limited, the benefits of early breastfeeding likely extend to complementary feeding. Moreover, maternal socioeconomic conditions may also influence the provision or omission of this type of food.
The literature shows that longer durations of EBF and BF are associated with healthier dietary patterns in early childhood, including higher consumption of healthy foods and better acceptance and variety of fruits, vegetables, and greens.
27–29 Conversely, shorter breastfeeding periods have been linked to an increased introduction of ultra-processed foods in the first year of life, along with higher rates of early introduction of honey, sugar, and sweets.⁵
,⁶ According to the WHO, breastfeeding within the first hour of life is directly related to breastfeeding success throughout the first year.
12 Additionally, the practice is associated with faster colonization of the infant's microbiota, improved development of sucking and latch-on reflexes, stronger mother-infant bonding, better glycemic control, and a reduced incidence of respiratory infections and sudden infant death syndrome.
30This study had some limitations. One of the main limitations was that information on breastfeeding at 1 year and CF was self-reported by the mother retrospectively, which may introduce recall bias. However, EBF was assessed prospectively, mitigating this concern for that outcome. Another limitation is that the sample was recruited from a high-complexity public hospital that primarily serves high-risk pregnancies, which could reflect lower rates of breastfeeding within the first hour of life.
On the other hand, it is important to highlight the strengths of this study. Key positive aspects include the longitudinal design and detailed monitoring of the children during critical periods, such as the puerperium, the months following birth, and early childhood, providing valuable insights into breastfeeding and the introduction of complementary foods.
The findings of this study demonstrated that breastfeeding within the first hour of life was associated with exclusive breastfeeding at two months and a lower likelihood of introducing culinary ingredients, such as sugar, salt, and honey, during complementary feeding. These results reinforce the benefits of early breastfeeding for both EBF and CF. Further longitudinal studies are needed to explore this relationship in other populations.
AcknowledgmentsWe would like to thank the Coordination for the Improvement of Higher Education Personnel (CAPES – Portuguese acronym) the National Council for Scientific and Technological Development (CNPq – Portuguese acronym), and the Porto Alegre Teaching Hospital /Research and Event Incentive Fund (FIPE – Portuguese acronym) for their financial support.
Author's contributionFicagna CR, Menezes VM, Kretzer DC, Moreira PR, : data analysis, literature review, writing and review of the manuscript.
Goldani MZ, Silva CH, Bernardi JR: research coordinator, data analysis, review of the manuscript. All the authors approve the final version of the article and declare no conflict of interest.
References1. World Health Organization (WHO). 3 in 5 babies not breastfed in the first hour of life. [Internet]. Geneva: WHO; 2018. [access in 2023 Abr 6]. Available from:
https://www.who.int/news/item/31-07-2018-3-in-5-babies-not-breastfed-in-the-first-hour-of-life2. Braga VS, Vítolo MR, Kramer PF, Feldens EG, Feldens CA. Breastfeeding in the First Hours of Life Protects Against Pacifier Use: A Birth Cohort Study. Breastfeeding Med. 2020 Aug 1; 15 (8): 516-21.
3. Belo MNM, Azevedo PTÁCC, Belo MPM, Serva VMSBD, Batista Filho M, Figueiroa JN, et al. Aleitamento materno na primeira hora de vida em um Hospital Amigo da Criança: prevalência, fatores associados e razões para sua não ocorrência. Rev Bras Saúde Mater Infant. 2014 Mar; 14 (1): 65-72.
4. Lucchese I, Góes FGB, Soares IAA, Goulart MCL, Silva ACSS, Pereira-Ávila FMV. Amamentação na primeira hora de vida em município do interior do Rio de Janeiro: fatores associados. Esc Anna Nery. 2023; 27: e20220346.
5. Feldens CA, Vítolo MR, Maciel RR, Baratto PS, Rodrigues PH, Kramer PF. Exploring the risk factors for early-life sugar consumption: A birth cohort study. Int J Paediatr Dent. 2021 Mar 15; 31 (2): 223-30.
6. Porto JP, Bezerra VM, Pereira Netto M, Rocha DS. Aleitamento materno exclusivo e introdução de alimentos ultraprocessados no primeiro ano de vida: estudo de coorte no sudoeste da Bahia, 2018. Epidemiol Serv Saúde. 2021; 30 (2): e2020614.
7. Rousham EK, Goudet S, Markey O, Griffiths P, Boxer B, Carroll C, et al. Unhealthy Food and Beverage Consumption in Children and Risk of Overweight and Obesity: A Systematic Review and Meta-Analysis. Adv Nutr. 2022 Oct; 13 (5): 1669-96.
8. Ribas SA, Rodrigues MCC, Mocellin MC, Marques ES, Rosa GPC, Maganha CR. Quality of complementary feeding and its effect on nutritional status in preterm infants: a cross-sectional study. J Hum Nutr Diet. 2021 Feb 26; 34 (1): 3-12.
9. Andrade EDO, Rebouças AS, Filho JQ, Ambikapathi R, Caulfield LE, Lima AÂM, et al. Evolution of infant feeding practices in children from 9 to 24 months, considering complementary feeding indicators and food processing: Results from the Brazilian cohort of the MAL-ED study. Matern Child Nutr. 2022 Oct 15; 18 (4): e13413.
10. Bernardi JR, Ferreira CF, Nunes M, Silva CH, Bosa VL, Silveira PP, et al. Impact of perinatal different intrauterine environments on child growth and development in the first six months of life - IVAPSA birth cohort: rationale, design, and methods. BMC Pregnancy Childbirth. 2012 Dec 2; 12 (1): 25.
11. Werlang ICR, Bernardi JR, Nunes M, Marcelino TB, Bosa VL, Michalowski MB, et al. Impact of Perinatal Different Intrauterine Environments on Child Growth and Development: Planning and Baseline Data for a Cohort Study. JMIR Res Protoc. 2019 Nov 12; 8 (11): e12970.
12. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Guia Alimentar para a População Brasileira. Brasília (DF): Ministério da Saúde; 2014. [access in 2023 Abr 6]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2ed.pdf13. Monteiro CA, Cannon G, Levy R, Moubarac JC, Jaime P, Martins AP, et al. NOVA. A estrela brilha. World Nutr. 2016; 7 (1–3): 28-38.
14. Alves-Santos NH, Castro IRR, Anjos LA, Lacerda EMA, Normando P, Freitas MB, et al. General methodological aspects in the Brazilian National Survey on Child Nutrition (ENANI-2019): a population-based household survey. Cad Saúde Pública. 2021; 37: e00300020.
15. Setegn T, Gerbaba M, Belachew T. Determinants of timely initiation of breastfeeding among mothers in Goba Woreda, South East Ethiopia: A cross sectional study. BMC Public Health. 2011 Dec 8; 11 (1): 217.
16. Vaz JS, Gatica-Domínguez G, Neves PAR, Vidaletti LP, Barros AJD. Early initiation of breastfeeding is inversely associated with public and private c-sections in 73 lower- and middle-income countries. Sci Rep. 2022 Dec 6; 12 (1): 21081.
17. Aguayo VM, Gupta G, Singh G, Kumar R. Early initiation of breast feeding on the rise in India. BMJ Glob Health. 2016 Sep 21; 1 (2): e000043.
18. Komatsu R, Ando K, Flood PD. Factors associated with persistent pain after childbirth: a narrative review. Br J Anaesth. 2020 Mar; 124 (3): e117–30.
19. Lyellu HY, Hussein TH, Wandel M, Stray-Pedersen B, Mgongo M, Msuya SE. Prevalence and factors associated with early initiation of breastfeeding among women in Moshi municipal, northern Tanzania. BMC Pregnancy Childbirth. 2020 Dec 11; 20 (1): 285.
20. Mgongo M, Hashim TH, Uriyo JG, Damian JD, Stray-Pedersen B, Msuya SE. Determinants of Exclusive Breastfeeding in Kilimanjaro Region, Tanzania. Sci J Public Health. 2014 Nov; 2 (6): 631-5.
21. Hashim TH, Mgongo M, Uriyo JG, Damian DJ, Stray-Pedersen B, Msuya SE. Exclusive Breastfeeding up to Six Months is Very Rare in Tanzania: A Cohort Study of Infant Feeding Practices in Kilimanjaro Area. Sci J Public Health. 2015; 3 (2): 251-8.
22. Hashim TH, Mgongo M, Katanga J, Uriyo JG, Damian DJ, Stray-Pedersen B, et al. Predictors of appropriate breastfeeding knowledge among pregnant women in Moshi Urban, Tanzania: a cross-sectional study. Int Breastfeed J. 2016 Dec 14; 12 (1): 11.
23. Tewabe T. Timely initiation of breastfeeding and associated factors among mothers in Motta town, East Gojjam zone, Amhara regional state, Ethiopia, 2015: a cross-sectional study. BMC Pregnancy Childbirth. 2016 Dec 19; 16 (1): 314.
24. Condò V, Cipriani S, Colnaghi M, Bellù R, Zanini R, Bulfoni C, et al. Neonatal respiratory distress syndrome: are risk factors the same in preterm and term infants? J Matern Fetal Neonatal Med. 2017 Jun; 30 (11): 1267-72.
25. Eilers MA, Hendrick CE, Pérez-Escamilla R, Powers DA, Potter JE. Breastfeeding Initiation, Duration, and Supplementation Among Mexican-Origin Women in Texas. Pediatrics. 2020 Apr 1; 145 (4): e20192742.
26. Lechosa-Muñiz C, Paz-Zulueta M, Sota SM, Adana Herrero MS, del Rio EC, Llorca J, et al. Factors associated with duration of breastfeeding in Spain: a cohort study. Int Breastfeed J. 2020 Dec 9; 15 (1): 79.
27. Oliveira DS, Boccolini CS, Faerstein E, Verly-Jr E. Breastfeeding duration and associated factors between 1960 and 2000. J Pediatr (Rio J). 2017 Mar; 93 (2): 130-5.
28. Armstrong J, Abraham EC, Squair M, Brogan Y, Merewood A. Exclusive Breastfeeding, Complementary Feeding, and Food Choices in UK Infants. J Hum Lact. 2014 May 20; 30 (2): 201-8.
29. Perrine CG, Galuska DA, Thompson FE, Scanlon KS. Breastfeeding Duration Is Associated With Child Diet at 6 Years. Pediatrics. 2014 Sep; 134 (Suppl. 1): S50–5.
30. Soldateli B, Vigo A, Giugliani ERJ. Effect of Pattern and Duration of Breastfeeding on the Consumption of Fruits and Vegetables among Preschool Children. PLoS One. 2016 Feb 4; 11 (2): e0148357.
Received on November 29, 2023
Final version presented on December 6, 2024
Approved on December 10, 2024
Associated Editor:Gabriela Buccini


 ; Vanessa Machado Menezes2
; Vanessa Machado Menezes2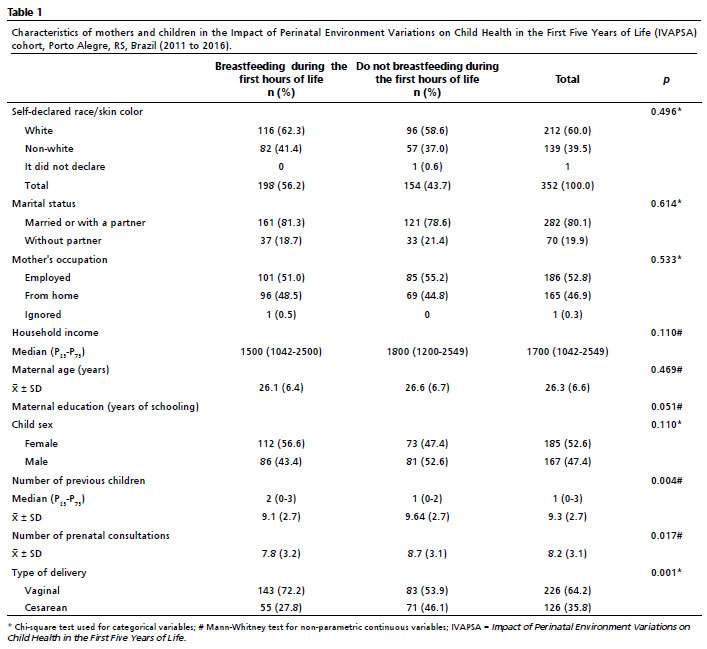






 Ler em português
Ler em português