ABSTRACT
OBJECTIVES: to evaluate changes in pregnant women's food consumption and at postpartum during COVID-19 pandemic and its related factors.
METHODS: a cross-sectional study, collecting anthropometric, sociodemographic, clinical and food consumption data on women who gave birth during the months of the highest incidence of COVID-19 in three Brazilian public hospitals.
RESULTS: 459 women participated in the study, with a median age of 28 years (Interquartile Range 9) and family income of up to one minimum wage (38.6%). A reduction was identified in a regular consumption of ready-to-eat food prepared outside the home (20.9% vs 31.6%; p<0.001), processed meat (34.9% vs 39.9%; p=0.011), stuffed cookies and sweets (40.5% vs 45.3%; p=0.016) and meat (75.8% vs 84.3%; p<0.001) during the pandemic. There was no association of these changes with the investigated variables.
CONCLUSIONS: there was a reduction in the consumption of ultra-processed food and meat during COVID-19 pandemic among the participants. Such findings may be positive given the harmful effects of consuming ultra-processed food and excess on meat on maternal and child's health. Changes in lifestyles and access to food received in the pandemic context may have influenced the results, requiring monitoring and new studies on this group's food consumption to understand the changes and their long-term impacts.
Keywords:
Maternal Nutrition, Puerperium, Food consumption, COVID-19
RESUMO
OBJETIVOS: avaliar mudanças no consumo alimentar de gestantes e puérperas durante a pandemia da COVID-19 e seus fatores relacionados.
MÉTODOS: estudo transversal, com coleta de dados antropométricos, sociodemográficos, clínicos e de consumo alimentar em mulheres que tiveram seus partos nos meses de maior incidência de COVID-19 em três hospitais públicos brasileiros.
RESULTADOS: participaram do estudo 459 mulheres, com mediana de 28 anos de idade (Intervalo Interquartil 9) e renda familiar de até um salário mínimo (38,6%). Identificou-se redução do consumo regular de alimentos prontos para consumo preparados fora de casa (20,9% vs 31,6%; p<0,001), embutidos (34,9% vs 39,9%; p=0,011), biscoitos recheados e doces (40,5% vs 45,3%; p=0,016) e de carnes (75,8% vs 84,3%; p<0,001) durante a pandemia. Não houve associação dessas alterações com as variáveis investigadas.
CONCLUSÕES: houve redução do consumo de ultraprocessados e de carnes durante a pandemia de COVID-19 entre as participantes. Tais achados podem ser positivos visto os efeitos deletérios do consumo de ultraprocessados e excesso de carnes para a saúde materno-infantil. Alterações nos modos de vida e acesso aos alimentos advindas do contexto pandêmico podem ter influenciado os resultados, demandando monitoramento e novos estudos sobre o consumo alimentar desse grupo para compreensão das mudanças e seus impactos em longo prazo.
Palavras-chave:
Nutrição materna, Puerpério, Consumo alimentar, COVID-19
IntroductionIn March 2020, the World Health Organization (WHO) declared that SARS-CoV-2 outbreak was characterized as a pandemic, a phenomenon that has become one of the greatest health challenges of recent years.
1 Due to the lack of specific treatments and high transmissibility, non-pharmacological measures were recommended to control the disease,
2 such as wearing masks, hygiene of the hands, closing establishments and social distancing.
3The adoption of these measures implied changes in the lifestyle of the population,
2 including food consumption. In several countries, there has been an increase in unhealthy food consumption,
4 and in Brazil, Malta
et al.
2 found an increase in ultra-processed food in 2020. In addition, food insecurity grew, affecting 59.4% of the Brazilian households between August and December, 2020.
5 Thus, the pandemic has not only been a health problem, but has also accentuated challenges related to social inequalities and inequities in different contexts.
6In addition to the adoption of control measures, some groups, such as pregnant women, were considered to be at greater risk of the disease, due to the tendency to worsen in the event of COVID-19.
7 Pregnancy and the processes that occur after it, such as the puerperium and lactation, are times when different transformations arise in the woman's body, involving major physiological and immunological changes.
8,9 Food is one of the factors that have a major impact on these processes, requiring special attention to the quality of the diet in these women.
Adequate nutrition promotes women's health and reduces gestational risks, such as gestational diabetes, hypertension, excessive or insufficient weight gain
7 and in the puerperium it favors, among other things, a healthy return to pre-pregnancy weight. In addition, the creation of healthy eating habits during pregnancy also fosters the proper development of the child, since it is part of the first 1000 days of life, which are crucial for promoting the individual's growth and development due to the high speed of cell multiplication.
10The pregnant women and parturient's diet should include a daily intake of fresh food and a restriction on the consumption of sugary beverages and ultra-processed food.
7 The
Pesquisa de Orçamentos Familiares (POF) (Household Budget Survey) in 2017-2018 indicates that Brazilian pregnant women predominantly consume fresh or minimally processed food, with a lower consumption of ultra-processed food compared to non-pregnant women.
7,11 However, data on food consumption markers for pregnant women from the
Sistema de Vigilância Alimentar e Nutricional (SISVAN) (Food and Nutrition Surveillance System) indicated high consumption (76%) of ultra-processed food among pregnant women in 2020.
11 In the postpartum period, dietary adequacy seemed to worsen due to the adaptations inherent to the new routine. Freitas
et al.
12 showed total low consumption of fruit, cereals, wholegrains and milk and dairy products among nursing mothers in the countryside of the Southeast, Brazil.
Given the importance of a healthy diet during pregnancy and the postpartum period, as well as the scarcity of studies on diets during these periods, especially in the context of COVID-19 pandemic, this study aims to assess changes in the dietary intake of pregnant women and postpartum during the pandemic and its associated factors.
MethodsThis cross-sectional study is part of a larger research project entitled
"Parto e Aleitamento Materno em filhos de mães infectadas por SARS-CoV-2" (Childbirth and Breastfeeding in Children of Mothers Infected with SARS-CoV-2). Additional information on the project can be found in Menezes
et al.
13 The sample includes women from three public hospitals that are references in maternal and child care in a Brazilian city, who gave birth in the first three months of the highest incidence of COVID-19 in Brazil (May, June and July 2020).
13 All adult women (≥18 years) with a single pregnancy who gave birth in these hospitals and had live newborns (NB) with a gestational age of 22 weeks or more, weighing more than 500 grams at birth, were included in this study. Data collection was carried out at two different times: 1. participants' medical records (n=1921) and 2. telephone collection (period ≥6 months after childbirth), where telephone contact was successful with n=492. Of these, participants with missing data on food consumption (n=33) were excluded, totaling 459 participants.
In order to estimate the sample required for this study (n=350), an expected proportion of change in food consumption of 50% was used, given the greater variability achieved and any prevalence of change in this variable. The number of women treated at these three hospitals during the period analyzed was used for the calculation (n= 3,839). A margin of error of 5% and a 95% confidence interval were adopted.
Data collection from medical records included sociodemographic data which was later checked and supplemented by telephone collection, including age (in years and categories: 18-24 years, 25-35 years and over 35 years), marital status (with and without a partner), self-declared skin color (white, black, mixed, yellow, indigenous), schooling (completed or not high school) and family income (in minimum wages, the salary of R$1045.00 being in force at the time: up to one minimum wage, one to three minimum wages, three to five, minimum wages and more than five minimum wages).
14 The categorization of this data was based on national studies or studies with similar samples.
15,16The telephone survey also collected anthropometric, clinical and food consumption data. In terms of anthropometry, self-reported postpartum weight and height were used to calculate the Body Mass Index (BMI=weight/height
2). This was categorized for adult women as "not overweight" (BMI <24.9 kg/m
2 and "overweight" (BMI ≥24.9 kg/m
2.
17 These categories were also used for adolescents (18 and 19 years old, n=18), after BMI/age had been properly assessed according to WHO parameters.
18 With regard to behavioral data, the current consumption of cigarettes and alcoholic beverages was investigated without determining the type and quantity. In addition, the practice of physical activity in the pre- or postpartum period (number of days per week and duration) was questioned, with "adequate" being considered when it was equal to or greater than 150 minutes per week.
19 The existence of nutritional monitoring during pregnancy or in the postpartum period was also requested. As for COVID-19 infection, only the presence of corresponding symptoms after childbirth was assessed, since at the beginning of the pandemic there were no tests available for the entire population.
20Food consumption was assessed using a questionnaire with food consumption markers adapted from SISVAN health care instruments and national surveys
15,21 covering nine food groups: 'food prepared outside the home that is ready to eat'; 'beans, peas, chickpeas or other legumes', 'fresh fruit (in its natural form)'; 'vegetables (potatoes, cassava, and yams were not considered)'; 'processed meat (hamburger, ham, bologna, salami, sausage, frankfurters)'; 'sweetened beverages (fruit juice with sugar, soda, boxed juice, powdered juice, boxed coconut water, guarana/gooseberry syrups)'; 'instant noodles, packet snacks or salty crackers'; 'stuffed cookies and sweets (candy/chocolate, chewing gum, jelly, sweet pies)'; 'beef, pork, chicken or fish'. The frequency was asked ''before the pandemic period'' (stating that it would be the gestational period before March 2020) and ''during the pandemic period'' (referring to the puerperium, since telephone data collection began six months after childbirth).
For each food group, the consumption frequencies presented were: 'never', '1-2 times/month', '1 time/week', '2 times/week', '3-4 times/week', '5-6 times/week' and 'every day'. The interviewers were trained to guide the participants in reporting the frequency of consumption. In order to characterize the consumption of these food groups, the food were organized according to the degree of processing into 'fresh food or minimally processed' (those obtained directly from plants or animals and which are purchased for consumption without any alteration or minimal alterations), 'cooking ingredients' (oils, fat, salt and sugar used in cooking preparations) 'processed food' (products made essentially by adding salt or sugar to fresh food or minimally processed food) and 'ultra-processed food' (products in which manufacture involves various stages and processing techniques and ingredients, many of which are used exclusively industrializd).
22 Considering that the current guidelines do not address quantitative parameters, but rather guide the prioritization of the consumption of fresh food and minimally processed food,
22 "regular" consumption of these foods (beans, peas, chickpeas or other legumes, fresh fruit, legumes and/or vegetables; meat) was adopted when the frequency mentioned was '5-6 times/week' or 'every day'.
2,15 For ultra-processed food (food prepared outside the home that come ready for consumption; processed meat; sweetened beverages; instant noodles, salty snacks or stuffed and sweet cookies), it was called "regular" when described on two or more days a week
2 since these guidelines also advise limiting the consumption of ultra-processed food.
22After checking for consistency, the data was analyzed using the Statistical Package for the Social Sciences (SPSS Inc) version 21.0. A descriptive analysis of the data was carried out, with categorical variables presented with their respective frequencies and numerical variables as medians and interquartile ranges (IQR). The Kolmogorov-Smirnov test was applied to assess whether the variables adhered to the normal distribution.
We analyzed whether there were significant differences in regular food consumption during the pandemic compared to the pre-pandemic period (before March 2020) by comparing consumption frequency with McNemar's test. Associations between categorical variables and changes in food consumption were tested using chi-square, with Bonferroni correction when necessary. The significance level was 5%.
The research project was approved by the Research Ethics Committee of the
Universidade Federal de Minas Gerais (Opinion no. 5.735.679, CAAE 32378920.6.0000.5149, approval date November 2, 2022).
ResultsA total of 459 women took part in the study, with a median age of 28 years (IQR 9), the majority having completed high school (75.2%) and a family income of up to one minimum wage (47.3%). 56.4% of the women were overweight and 14.2% mentioned nutritional monitoring during pregnancy or postpartum. The manifestation of COVID-19 symptoms in the postpartum period was reported by 34.9% of the participants (Table 1).
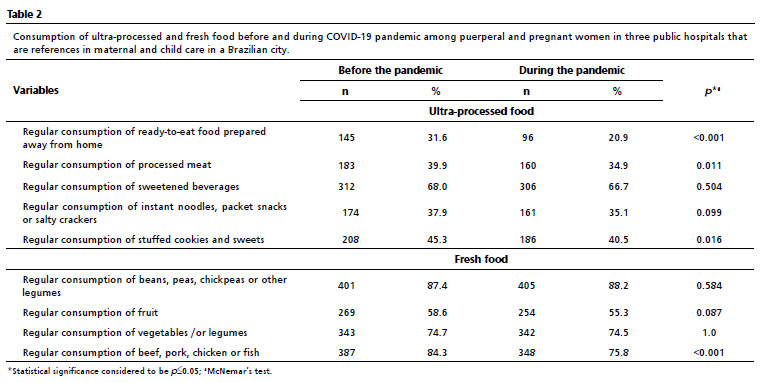
Regarding food consumption, before the pandemic it was observed that regular consumption of fresh food was described by most women: 87.4% reported regular consumption of legumes; 58.6% of fruit; 74.7% of vegetables and 84.3% of meat. This consumption has not changed significantly during the pandemic, with the exception of regular meat consumption (84.3%
vs 75.8%;
p<0.001) (Table 2).
In addition, in the ultra-processed food group, there was a reduction during the pandemic in the regular consumption of ready-to-eat food prepared away from home (31.6%
vs 20.9%;
p<0.001), processed meat (39.9%
vs 34.9%;
p=0.011), stuffed cookies and sweets (45.3%
vs 40.5%;
p=0.016) (Table 2).
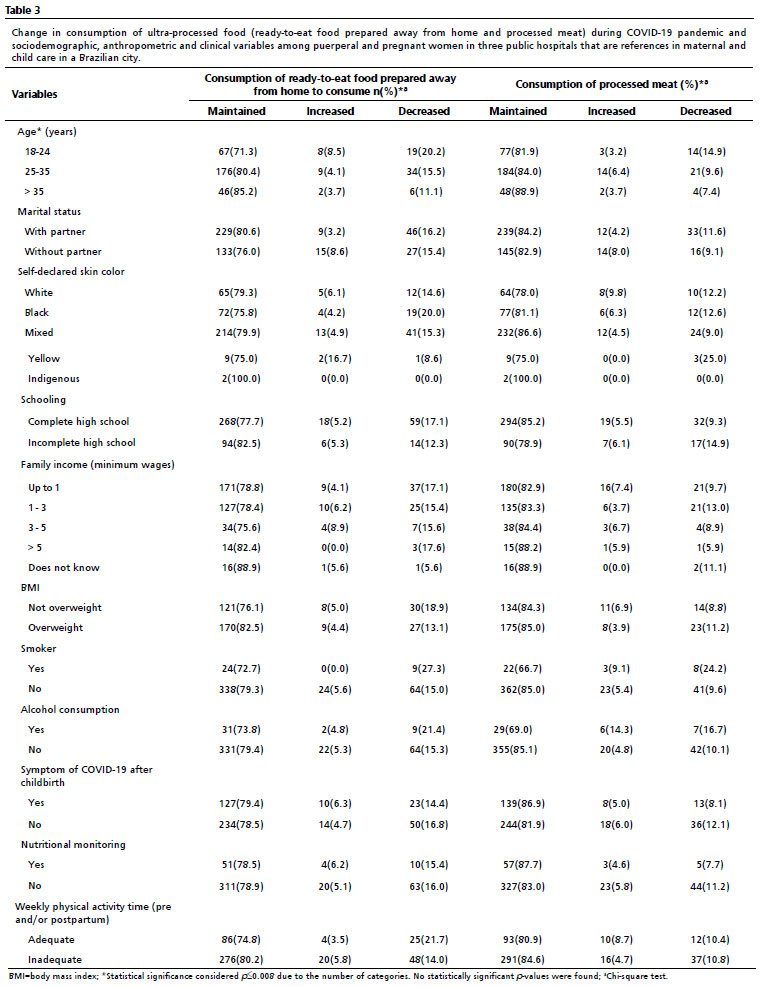
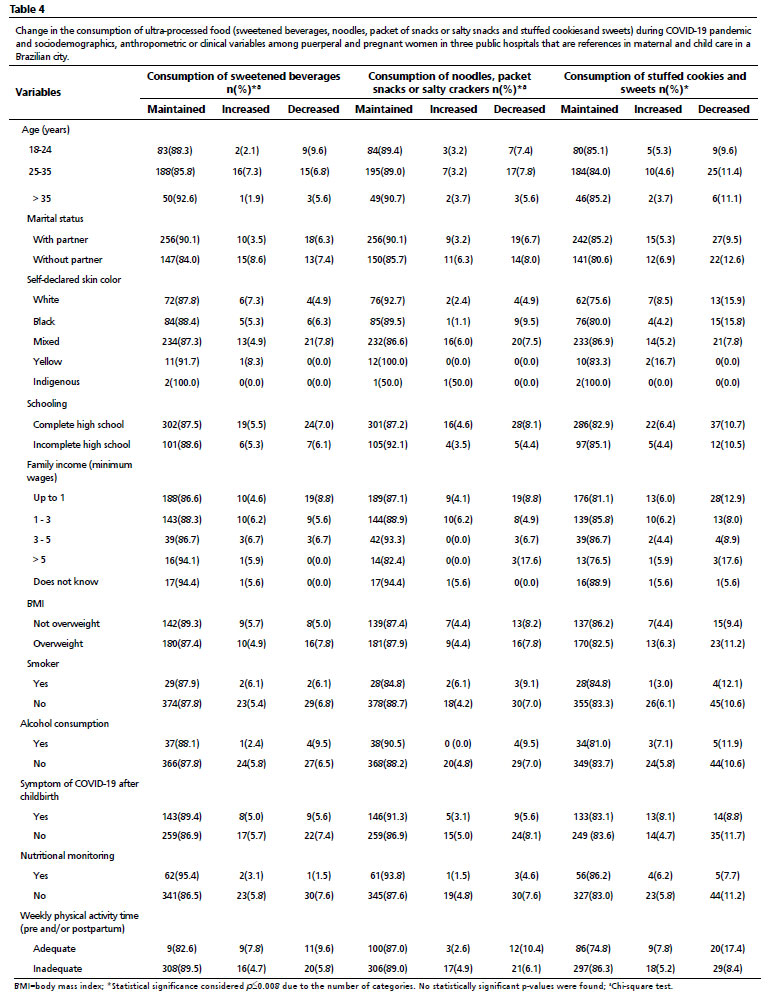
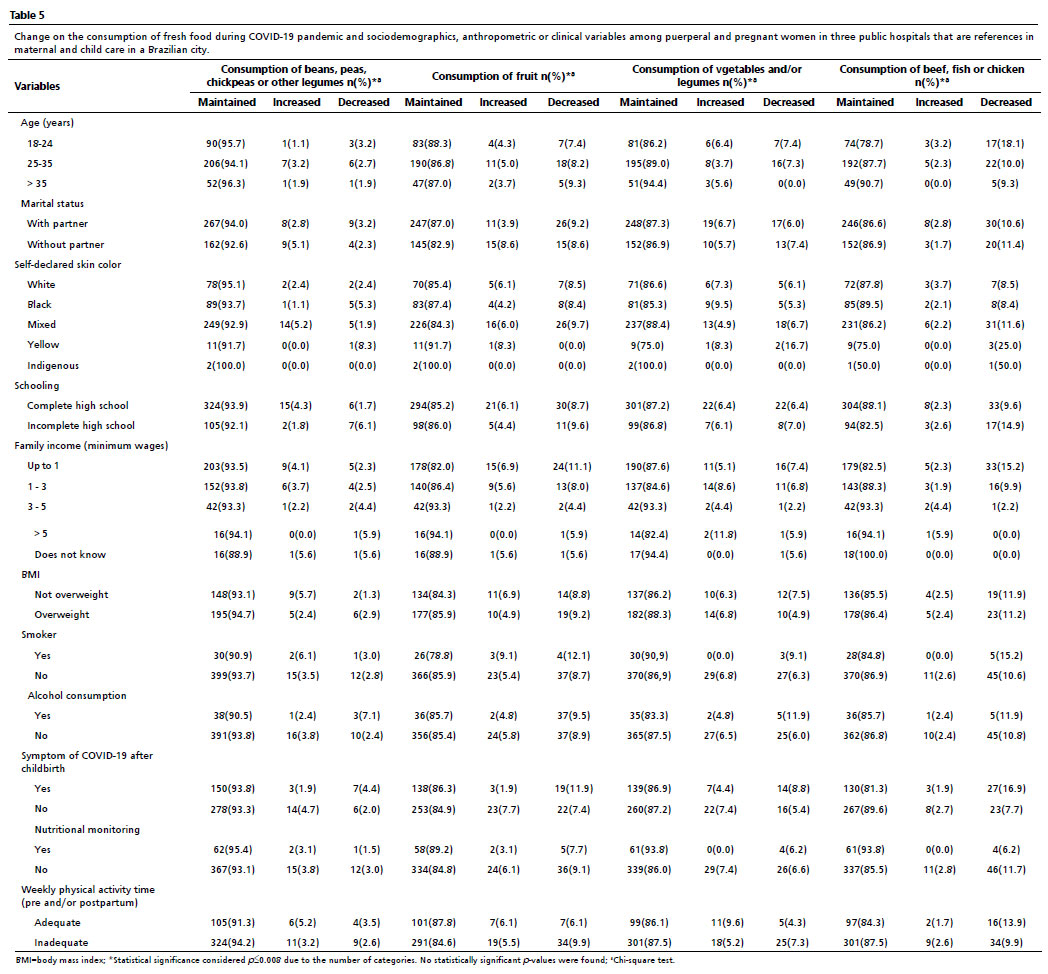
Changes in food consumption during the pandemic (Tables 3 to 5) were not associated with sociodemographic, anthropometric or clinical variables.
DiscussionThe findings of this study indicate significant reductions in the regular consumption of ultra-processed food - ready-to-eat food prepared outside the home, processed meat, stuffed cookies and sweets - and meat among pregnant and puerperal women during COVID-19 pandemic.
The reduction in the consumption of ultra-processed food can be attributed to social isolation, which encouraged homemade preparations due to more time at home and health concern. Andrade
et al.
23 reported that health concerns, the decrease in the family income and the time available for cooking were frequent reasons for dietary changes during the pandemic, including an increase in the consumption of chicken, fruit, vegetables and eggs, and a reduction in the intake of meat and ultra-processed food.
Although, the income in this study was not significantly associated with changes in food consumption, it is known that purchasing power is related to access food
24 and could imply changes in dietary choices with an impact on the consumption of ultra-processed food.
Martinez
et al.
25 showed a significant increase in the consumption of vegetables, fruit and legumes and stability in the consumption of ultra-processed food during COVID-19 pandemic in Brazil among participants (n=10,116, 78% of whom were women). However, 85.1% of the participants in this study had a high level of schooling (12 or more years of study), which may contribute to the divergence with the results found here. In the present sample, a lower percentage (75.2%) had completed high school and of these, less than 15% had 12 or more years of schooling.
Other national and international studies have also reported an increase in the consumption of ultra-processed food, such as ready-to-eat food prepared outside the home, sweets and stuffed cookies.
4,21,23 These disagreements may have been due to the differences in sample sizes, life cycles, both sexes and different sociodemographic characteristics, as well as the fact that they covered different moments during the pandemic.
The reduction in ultra-processed food during the period analyzed may have had a positive impact on the health of these women, since current recommendations
8,23 recommend limiting consumption of these food. During pregnancy, this consumption is associated with excessive gestational weight gain
7 - which is related to the development of gestational diabetes and/or hypertensive syndrome, leading to complications in maternal and child health.
8 In the puerperium, this consumption favors postpartum weight retention, which can lead to the development of obesity in the mother and other chronic non-communicable diseases.
7 In addition, there is a consensus in the literature about the deleterious effects of these food have on health, such as promoting cardiovascular diseases, diabetes and various types of cancer, as well as increasing the risk of nutritional deficiencies and contributing to excessive calorie consumption.
In addition to a reduction in the consumption of ultra-processed food, this study found a decrease in meat consumption during the pandemic. Despite the lack of association with the sociodemographic variables tested here, it is considered that social restriction measures have fostered changes in accessing food, especially highly perishable food, and have impacted food choices due to costs.
26 A national study showed a reduction in the consumption of meat (beef and pork) and fish among those who reported a reduction in their family budget during COVID-19 pandemic.
23 In addition, there was an increase in moderate and severe food insecurity among Brazilian families earning up to one minimum wage during this period.
27Meat is known to be an important source of iron during pregnancy and the puerperium. A considerable reduction in this food in the diet in these life cycles, without adequate nutritional monitoring, can compromise the intake of this and other nutrients, contributing to iron deficiency anemia, low birth weight and reduced gestation periods.
28 Thus, a reduction in meat consumption among women who already have a low consumption of this food and others with similar nutritional characteristics, can contribute negatively to maternal and child health. However, national estimates show an increase in the average intake of meat in recent years (86g/1000 kcal in 2008; 97g/1000 kcal in 2017, especially beef).
29 The increase varied between income categories, and was lower among lower-income individuals.
29 It should be noted that these values exceed the recommendations of different institutions (around 40-70g/day).
30 Therefore, the reduction identified in this study may be positive, given that excessive consumption of meat leads to a higher intake of saturated fats and risk of cardiovascular diseases.
22 The food consumption marker applied in this study did not differentiate consumption of the different types of meat (beef, pork, chicken or fish), nor was there any quantitative measurement of these products, so it was not possible to analyze whether this reduction was different between these categories and how much this intake changed.
In addition, it is worth noting that pregnancy and the puerperium cause significant changes in mothers' food consumption patterns, since women try to follow an adequate diet in order to recover after childbirth and the quality of breast milk.
8 Thus, this concern for health may also have influenced the dietary changes found here.
Moreover, there are limitations to the study, such as the lack of association between changes in food consumption before and during the pandemic and the variables tested here, which may be justified by the homogeneity of the sample in terms of sociodemographic characteristics, as well as the evaluation at a single moment of the pandemic, given the different waves of the disease and the impacts experienced in Brazil. Furthermore, there is a memory bias, since these women may not accurately remember their diet before the pandemic and their self-reported weight and height, especially due to the family changes experienced with pregnancy and childbirth, also to the reorganizations resulting from the pandemic scenario. Additionally, the data was only obtained from three hospitals in a Brazilian city, not considering the consequences of the pandemic individually in each region of the country. It should also be noted that no validated instrument was used to collect food consumption data for pregnant/puerperal women, despite the careful construction of the data collection questionnaire.
This study identified that there have been significant changes during COVID-19 pandemic in the food consumption of pregnant women and at postpartum. It should be noted that this is one of the first studies carried out in Brazil to verify such changes among this public in the context of the pandemic. It is clear that analyzing food consumption is important to verify the maintenance or changes in dietary patterns, in order to contribute to the development of nutritional interventions with a given population. The changes shown here are positive, but they need to be monitored. Therefore, we hope to encourage longitudinal comparisons and follow-up studies with this group, using instruments validated for this population, in order to measure the relevance of the effects of the pandemic caused by SARS-CoV-2 on women's diet and health in the medium and long term.
References1. Organização Pan-Americana da Saúde (OPAS) | Organização Mundial da Saúde (OMS). OMS declara emergência de saúde pública de importância internacional por surto de novo coronavírus [
Internet]. Geneva: OPAS/OMS; 2020. [access in 2024 jun 23]. Available from:
https://www.paho.org/pt/news/30-1-2020-who-declares-public-health-emergency-novel-coronavirus2. Malta DC, Szwarcwald CL, Barros MBA, Gomes CS, Machado ÍE, Souza Júnior PRB. A pandemia da COVID-19 e as mudanças no estilo de vida dos brasileiros adultos: um estudo transversal, 2020. Epidemiol Serv Saúde. 2020; 19 (4): 1-13.
3. Ministério da Saúde (BR). Como se proteger? Confira medidas não farmacológicas de prevenção e controle da pandemia do novo coronavírus. Brasília (DF): Ministério da Saúde; 2021. [access in 2023 Jan 27]. Available from:
https://www.gov.br/saude/pt-br/assuntos/covid-19/como-se-proteger4. González MC, Gómez GI, Olarte SCM, Motrico E. Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies. Int J Environ Res Public Health. 2021. 18: 11130.
5. Galindo E, Teixeira MA, Araújo M, Motta R, Pessoa M, Mendes L, Rennó L. Efeitos da pandemia na alimentação e na situação da segurança alimentar no Brasil. [
Internet]. Food for Justice Working Paper Series, Nº4 2021. [access in 2023 Abr 7]. Available from:
https://www.epsjv.fiocruz.br/sites/default/files/files/relatorio%20pesquisa%20Berlim%20UF MG.pdf6. Matta GC, Rego S, Souto EP, Segata J. Os impactos sociais da COVID-19 no Brasil: populações vulnerabilizadas e respostas à pandemia. Rio de Janeiro: RJ. Editora FIOCRUZ; 2021.
7. Ministério da Saúde (BR). Fascículo 3: Guia Alimentar para a população brasileira na orientação alimentar de gestantes. Brasília (DF): Universidade de São Paulo; 2021. [access in 2023 Fev 4]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/protocolos_guia_alimentar_fasciculo3.pdf.8. Baião MB, Deslandes SF. Alimentação na gestação e puerpério. Rev Nutr. 2006; 19 (2) 245-53.
9 Parizzi MR, Fonseca JGM. Nutrição na gravidez e na lactação. Rev Méd Minas Gerais. 2010; 20 (3): 341-53.
10. Sociedade Brasileira de Pediatria (SBP). Departamento de Nutrologia. Manual de Alimentação: orientações para alimentação do lactente ao adolescente, na escola, na gestante, na prevenção de doenças e segurança alimentar. São Paulo: SBP; 2018; 4ª ed. 172 p. [access in 2023 Nov 25]. Available from:
https://edisciplinas.usp.br/mod/resource/view.php?id=316098511. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. Departamento de Promoção da Saúde. Situação alimentar e nutricional de gestantes na Atenção Primária à Saúde no Brasil. Brasília (DF): Ministério da Saúde; 2022. [access in 2024 Mai 26]. Available from:
https://nutricao.saude.ms.gov.br/wp-content/uploads/2022/08/14-Situacao-alimentar-e-nutricional-de-gestantes-na-Atencao-Primaria-a-Saude-no-Brasil.pdf12. Ferreira Freitas RF, Caetano DS, Lessa AC, Macedo MS, Pinto NAVD, Teixeira RA. Calidad de la dieta de las amamantadoras utilizando el Ïndice de Alimentación Saludable. Enferm Glob. 2017; 17 (51): 144-55.
13. Menezes FR, Silva TPR, Felisbino-Mendes MS, Santos LC, Almeida PCMA, Filipe MML,
et al. Influence of the COVID-19 pandemic on labor and childbirth care practices in Brazil: a cross-sectional study. BMC Pregnancy Childbirth. 2023; 3: 23.
14. Congresso Nacional (BR). Lei nº 14.013, 10 de junho de 2020. Dispõe sobre o valor do salário-mínimo a vigorar a partir de 1º de janeiro de 2020; e dá outras providências. Brasília (DF): DOU 10 de junho de 2020. [access in 2024 Jan 3]. Available from:
https://www.planalto.gov.br/ccivil_03/_ato2019-2022/2020/lei/l14013.htm#:~:text=Disp%C3%B5e%20sobre%20o%20valor%20do,2020%3B%20
e%20d%C3%A1%20outras%20provid%C3%AAncias.&text=O%20PRESIDENTE%20 DA%20REP%C3%9ABLICA%20Fa%C3%A7o,Art.15. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Vigitel Brasil 2021: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília (DF): Ministério de Saúde; 2022. [access in 2023 Mar 15]. Available from:
https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/publicacoes- svs/vigitel/vigitel-brasil-2021-estimativas-sobre-frequencia-e-distribuicao-sociodemografica- de-fatores-de-risco-e-protecao-para-doencas-cronicas/16. Ministério do Planejamento, Orçamento e Gestão (BR). Instituto Brasileiro de Geografia e Estatística (IBGE). Características étnico-raciais da população: classificações e identidades. Rio de Janeiro: Ministério do Planejamento, Orçamento e Gestão; 2013. [access in 2023 Fev 2]. Available from:
https://biblioteca.ibge.gov.br/visualizacao/livros/liv63405.pdf17. World Health Organization (WHO). Obesity: preventing and managing the global epidemic: report of a WHO consultation on obesity, Geneva, 3-5 June 1997. [access in 2024 Fev 21]. Available from:
https://iris.who.int/handle/10665/6385418. World Health Organization (WHO). Growth reference data for 5-19 years. WHO; 2007 [access in 2024 Abr 27]. Available from:
https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age19. Organização Mundial da Saúde (OMS). Diretrizes da OMS para atividade física e comportamento sedentário num piscar de olhos. OMS; 2020 [access in 2023 Nov 25]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/337001/9789240014886- por.pdf20. Ministério da Saúde (BR). Protocolo de manejo clínico da COVID-19 na Atenção Especializada. Brasília (DF): Secretaria de Atenção Especializada à Saúde, Departamento de Atenção Hospitalar, Domiciliar e de Urgência. Brasília (DF): Ministério da Saúde; 2020. 1ª ed rev. [access in 2023 Jan 4]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manejo_clinico_covid- 19_atencao_especializada.pdf21. Fundação Oswaldo Cruz. ConVid Pesquisa de Comportamentos [
Internet]. ConVid; 2020. [access in 2024 Jun 23]. Available from:
https://convid.fiocruz.br/arquivos/QuestionarioConVidPesquisaDeComportamentos.pdf22. Ministério da Saúde (BR). Guia Alimentar para a População Brasileira. Brasília (DF): Ministério da Saúde; 2014. [access in 2023 Nov 25]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2ed.pdf23. Andrade GC, Levy RB, Leite MA, Rauber F, Claro RM, Coutinho JG,
et al. Mudanças nos marcadores da alimentação durante a pandemia de covid-19 no Brasil. Rev Saúde Pública. 2023; 57: 54.
24. Andrade GC, Caldeira TCM, Mais LA, Bortoletto Martins AP, Claro RM. Food price trends during the COVID-19 pandemic in Brazil. PLoS One. 2024 May; 19 (5): e0303777.
25. Martinez SE, Rauber F, Costa CS, Leite MA, Gabe KT, Louzada ML,
et al. Mudanças alimentares na coorte NutriNet Brasil durante a pandemia de covid-19. Rev Saúde Pública. 2020; 54: 51
26. Malta DC, Gomes CS, Allana GS, Sá ACMGN, Prates EJS, Freitas MIF,
et al. Mudanças no estilo de vida em adultos durante a pandemia de COVID-19 em Minas Gerais. Rev Bras Epidemiol. 2021; 24: e210009.
27. II Inquérito Nacional sobre Insegurança Alimentar no Contexto da Pandemia da COVID-19 no Brasil [livro eletrônico]: II VIGISAN : relatório final/Rede Brasileira de Pesquisa em Soberania e Segurança Alimentar – PENSSAN. São Paulo (SP): Fundação Friedrich Ebert : Rede PENSSAN; 2022. [access in 2024 Mar 25]. Available from:
https://olheparaafome.com.br/wp-content/uploads/2022/06/Relatorio-II-VIGISAN-2022.pdf28. World Health Organization (WHO). WHO guideline on use of ferritin concentrations to assess iron status in individuals and populations. Geneva: WHO; 2020. [access in 2024 Mai 29]. Available from:
https://iris.who.int/bitstream/handle/10665/331505/9789240000124-eng.pdf?sequence=129. Ueta MH, Tanaka J, Marchioni DML, VJ Eliseu, Carvalho AM. Food sustainability in a context of inequalities: meat consumption changes in Brazil (2008–2017). Environ Dev Sustain .2023; 26: 6377-91.
30. Instituto Nacional de Câncer (INCA). Alimentos, nutrição, atividade física e prevenção de câncer: uma perspectiva global. Rio de Janeiro: INCA; 2011. [access in 2024 Jun 5]. Available from:
https://www.inca.gov.br/sites/ufu.sti.inca.local/files/media/document/resumo-alimentos-nutricao-atividade-fisica-e-prevencao-de-cancer-2011.pdfAcknowledgements: We would like to thank the
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (National Council for Scientific and Technological Development) and the
Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) (Minas Gerais Research Foundation) for their financial support.
Authors' contribution: Souza Mendes LS: conceptualization, data curation, formal analysis, methodology, project management, validation, visualization, writing, reviewing and editing the manuscript. Faria PKT: conceptualization, data curation, formal analysis, methodology, project management, validation, visualization, writing, reviewing and editing the manuscript. Armani BC: formal analysis, methodology, supervision, revision and editing of the manuscript. Matozinhos FP: acquisition of funding, resources, review and editing of the manuscript. Santos LC: supervision, revision and editing of the manuscript. All the authors have approved the final version of the article and declare no conflict of interest.
Received on August 22, 2024
Final version presented on December 20, 2024
Approved on January 10, 2025
Associated Editor: Paola Mosquera


 ; Paula Ketlen Teodoro Faria2
; Paula Ketlen Teodoro Faria2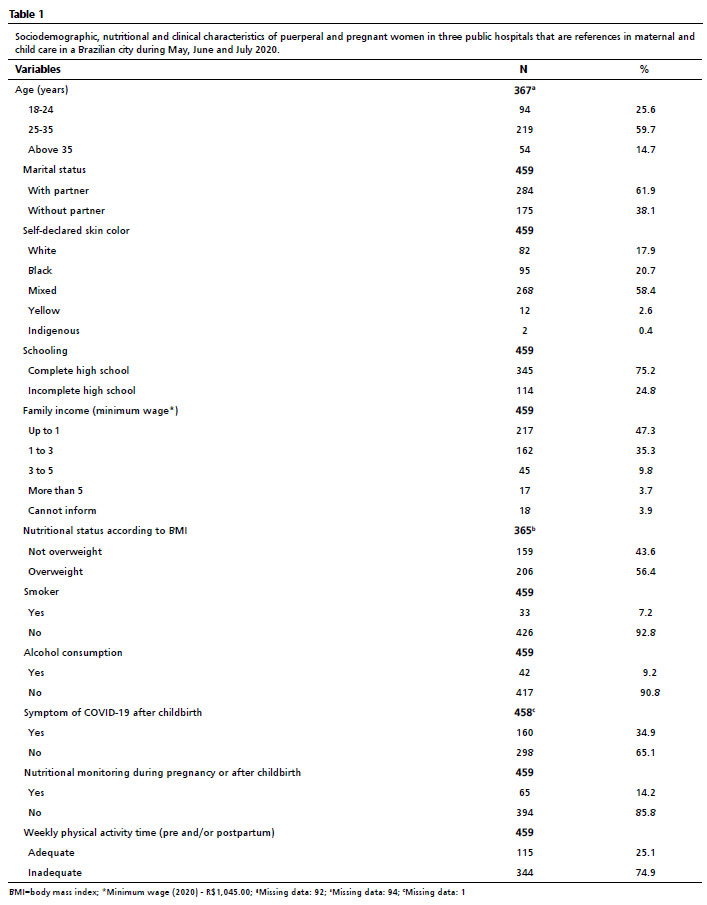






 Ler em português
Ler em português