ABSTRACT
OBJECTIVES: to assess the association between mothers age and the presence of acute respiratory infections (ARIs) and acute diarrhea (AD) in Peruvian children under five years old.
METHODS: secondary analysis of the database of the "Demographic and Family Health Survey" of 2015 and 2019. We analyzed data from children under five and their reproductive-age mothers who live in the same household. Poisson regression models were used to generate adjusted prevalence ratios (aPR) with 95% confidence intervals (95%CI) to assess the association between mothers' age group and the presence of ARIs and AD in their children.
RESULTS: 84,671 mother/child data were analyzed. In the adjusted regression model, being a young mother (aPR= 1.18; 95%CI= 1.11-1.25; p<0.001) or an teenage (aPR= 1.11; 95%CI= 1.01-1.22; p=0.045) were associated with a higher prevalence of ARIs in their children. In addition, being a young mother a teenage (aPR= 1.18; 95%CI= 1.11-1.25; p<0.001) or a teenage (aPR= 1.22; 95%CI= 1.10-1.35; p<0.001) were also associated with a higher prevalence of AD cases in their children.
CONCLUSIONS: mothers' age was found to be associated with the prevalence of ARIs and AD in Peruvian children under five, with teenagers and young mothers having the greatest probability of ARIs and AD.
Keywords:
Respiratory tract infections, Diarrhea, Maternal age, Maternal health, Child health, Peru
RESUMO
OBJETIVOS: evaluar la asociación entre la edad materna y la presencia de infecciones respiratorias agudas (IRAs) y enfermedades diarreicas agudas (EDAs) en niños peruanos menores de cinco años.
MÉTODOS: análisis secundario de la base de datos de la “Encuesta Demográfica y de Salud Familiar” de 2015 y 2019. Se analizaron datos de niños menores de cinco años y sus madres en edad reproductiva que viven en el mismo hogar. Se utilizaron modelos de regresión de Poisson para calcular razones de prevalencia ajustadas (RPa) con sus intervalos de confianza del 95% (IC95%) para evaluar la asociación entre el grupo de edad de las madres y la presencia de IRAs y EDAs en sus hijos.
RESULTADOS: se analizaron 84,671 datos madre/hijo. En el modelo de regresión ajustado, ser madre joven (RPa= 1,18; IC95%= 1,11-1,25; p<0,001) o adolescente (RPa= 1,11; IC95%= 1,01-1,22; p=0,045) se asoció con una mayor prevalencia de IRAs en sus hijos. Además, ser madre joven (RPa= 1,18; IC95%= 1,11-1,25; p<0,001) o adolescente RPa= 1,22; IC95%= 1,10-1,35; p<0,001 también se asoció con una mayor prevalencia de EDAs en sus hijos.
CONCLUSIONES: la edad de las madres se asoció con la prevalencia de IRAs y EDAs en niños peruanos menores de cinco años, siendo las madres adolescentes y jóvenes las que presentaron mayor probabilidad de IRAs y EDAs.<
Palavras-chave:
Infecciones del tracto respiratorio, Diarrea, Edad materna, Salud materna, Salud infantil, Perú
IntroductionIn Peru, acute diarrhea (AD) and acute respiratory infections (ARIs) are two pediatric diseases with the highest frequency in children under five years old.
1 The National Center for Epidemiology, Prevention, and Disease Control reported that in Peru, the cumulative incidence of pneumonia in 2023 was 1.2 episodes every 10,000 children under five years of age,
2 while that of acute diarrhea in 2021 was 184.6 and 124.8 episodes every 10,000 children under one year and one to five years, respectively.
3 The factors associated with these diseases are multiple. For example, a systematic review of demographic and health surveys from 34 sub-Saharan countries conducted between 2009 and 2018 showed that young age, educational level, and socioeconomic level were factors associated with diarrhea.
4 Another systematic review of studies published in East Africa between 2000 and 2019 evidenced that using biomass as a fuel source, cooking in an environment not separated from the living room, the presence of the children during the process of cooking, and non-vaccination were associated with pneumonia.
5Teenage pregnancy as a risk factor for children’s health is a controversial factor. Some studies conducted in different countries between 2002 and 2012, together, have found that this factor is associated with different adverse outcomes regarding mothers’ and children’s health.
6 In Peru, the National Institute od Statistics and Informatics (INEI – Spanish acronym) considers mothers under 20 years old to be a high-risk group concerning infant mortality because, in 2019, their rate is higher compared to mothers between 20 and 39 years old (incidence of 17 per a thousand versus 13 per a thousand children).
7 Hence, ideally, it is recommended that the first pregnancy should occur between 20 and 30 years old, as the risk related to complications is the minimum in this age group.
8 However, in 2021, a study showed that this effect might be confounded by variables for which it is not adjusted in most studies, and a decrease in pregnancy among mothers under 18 years would not be an effective strategy to improve child health.
9Latin America has one of the highest levels of prevalence of adolescent pregnancy in the world.
10 Peru, in 2015, had a rate of 52.1 births per 1000 women in the age group from 15 to 19 years old, and it is a problem, mainly with pregnancy in minors under 15 years old. A study conducted by Planned Parenthood Global in 2015 in Ecuador, Guatemala, Nicaragua, and Peru reported that pregnancy in women between nine and 14 years has increased in the last 10 years.
11 Considering that the main pediatric diseases are ARIs and AD, it is important to know whether the mother’s age, including being a part of the age group of teenage, might be associated with a higher risk of ARIs and AD in the Peruvian children population. Given that, in Peru, these diseases are important causes of morbidity in children, it is necessary to identify what associated characteristics exist. Therefore, this study aims to evaluate whether mothers’ age is related to the presence of ARIs and AD in children under five in the Peruvian population.
MethodsWe performed a secondary analysis of the database of the Demographic and Family Health Survey (ENDES – Spanish acronym) during the period between 2015 and 2019. ENDES is a cluster sampling survey, stratified and representative at the national level, administered annually by the INEI. The survey has three questionnaires (household, individual, and health) and is administered to update the knowledge of health indicators of the Peruvian population.
12The study population was constituted of women of reproductive age (WRA) from 12 to 49 years old. ENDES used probability, balanced two-stage, stratified and independent sampling at the department level and per urban and rural area. ENDES estimations have annual representativity at the national level that covers urban/rural areas per geographic domain (Lima Metropolitan Area, Coast, Highlands, and Jungle) and for the 24 regions of Peru and the constitutional province of Callao.
12As our interest was to evaluate the association between maternal age and the presence of ARI and AD in children under five years of age, we included data on women of reproductive age and their children under five years of age. Each child was matched to his or her mother, so 110,755 mother/child pairs were identified. After excluding 7,329 records of deceased children, the dataset was cleaned by only including information regarding the youngest child if a given mother had two or more children. This led to the exclusion of cases where two (n=12,517), three (n=1,324) or four (n=45) children living with the same mother were not the youngest child. Subsequently, 609 records of children not living with their mothers and 4,030 records lacking information on their children’s immunization records were excluded. In addition, 52 records lacking the outcome and 178 records with incomplete information on the variables of interest were eliminated. Finally, we analyzed 84,671 mother/child data (Figure 1).

We considered two outcomes: presence of ARIs, and presence of AD in children. ARIs were defined as the joint presence of cough and shortness of breath, or rapid breathing over the last two weeks prior to the survey according to the indications of the Technical Standard of Ministry of Health of Perú.
13 The questions used were: “In the last 14 days has the child had a cough?” and “Did the child breathe faster than usual, with short, choppy breaths?” On the other hand, AD was defined as the presence of diarrhea in the last two weeks prior to the survey. This variable was constructed based on the question “Has the child had diarrhea in the last two weeks?”, and considering the methodology of some previous studies.
14 All questions were answered by the mothers, the response options were yes and no.
The exposure variable was mothers’ age group. The age of the mother was collected numerically in years. For the analysis, we classified this variable into three distinct categories: teenage mother, those who are between 12 and 19 years old; young mother, those between 20 and 30 years old; and adult mother, those who are between 31 and 49.
Furthermore, other covariates were included as confounders according to the literature, such as child age (categorized into zero - 23 months old and 24 - 59 months old), child gender (female, male), and vaccination status of the child (incomplete, complete). In addition, regarding mothers, we included educational level (complete elementary education or below, high school, non-university higher education, university education), current marital status (single, live-in-parter only, married, widowed, divorced/separated), violence (no, yes), pregnancy (no, yes), number of children, wealth index (poorest, poorer, middle, richer, richest), health insurance (yes, no), residence area (urban, rural), geographic region of the mother’s residence (Lima Metropolitan Area, rest of the coast, highlands, jungle), vaccination status (according to the vaccination schedule by age group of the children, established by the Technical Health Standard (NTS) Nº141-MINSA/2018/DGIESP of the Ministry of Health of Peru,
15 considering the vaccines of children who had their vaccination cards and/or vaccines reported by their mothers), and intimate partner violence (including physical, psychological, and sexual abuse; for the creation of this variable, questions of the questionnaire were taken into account, which are described in other previously published study.
16The ENDES database, corresponding to 2015-2019, was downloaded in a .SAV format file, then exported and analyzed with STATA v16.0 (TX, StataCorp LP). All the sample patterns were analyzed according to the stratum and weighting factor, considering the complex sampling design of ENDES, using the command
svy.
In the descriptive analysis, the categorical variables were expressed in frequencies and percentages with their respective 95% confidence intervals (95%CI). The numerical variables were shown as means, with their respective 95%CI. To determine if significant differences exist between the independent variables according to the proposed outcomes, we used the chi-squared test with Rao-Scott correction for complex sampling. To determine the differences between numerical variables, we used the Wald test.
We constructed Poisson regression models to know the associations between the mothers’ age group and the presence of ARIs and AD in children and to estimate crude prevalence ratios (cPR) and adjusted prevalence ratios (aPR) with their respective 95%CI. A first crude model was performed by bivariate regressions for the variables of interest, while the second models were regressions adjusted by covariates of the study, following a statistical criterion. Those variables that showed a
p<0.05 in the crude analysis were included as adjustment variables, using the backward selection method. Collinearity was determined through the variance inflation factors, considering a cutoff point greater than 10 (it should be noted that none of the obtained factors was higher than this predefined cutoff point). In addition, we constructed stratified models according to child age to assess differences in the presence of ARIs and AD. A p-value lower than 0.05 was considered statistically significant for all the analysis.
This study analyzed available secondary data, which can be accessed on the website of INEI.
17 The databases can be downloaded and do not have identifiers for the respondents, for which the information of the participants is confidential. All participants gave their informed consent terms when surveyed by the team who administered the survey.
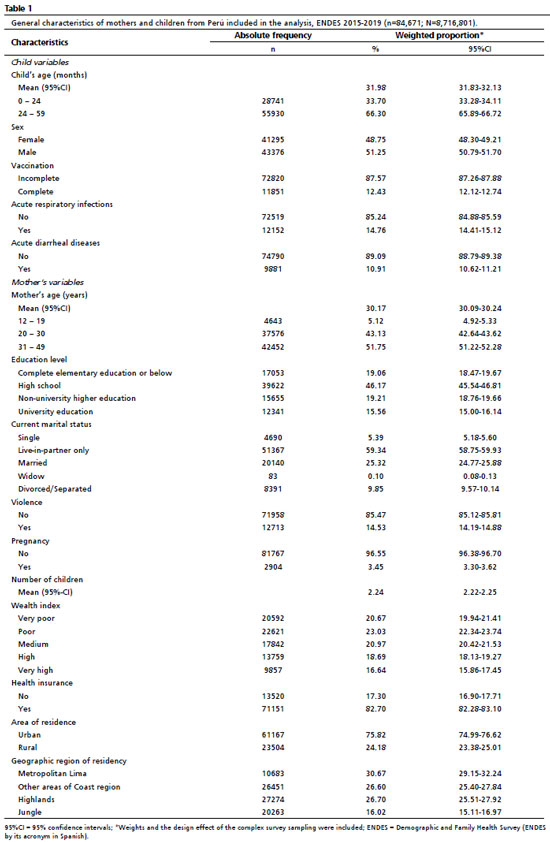
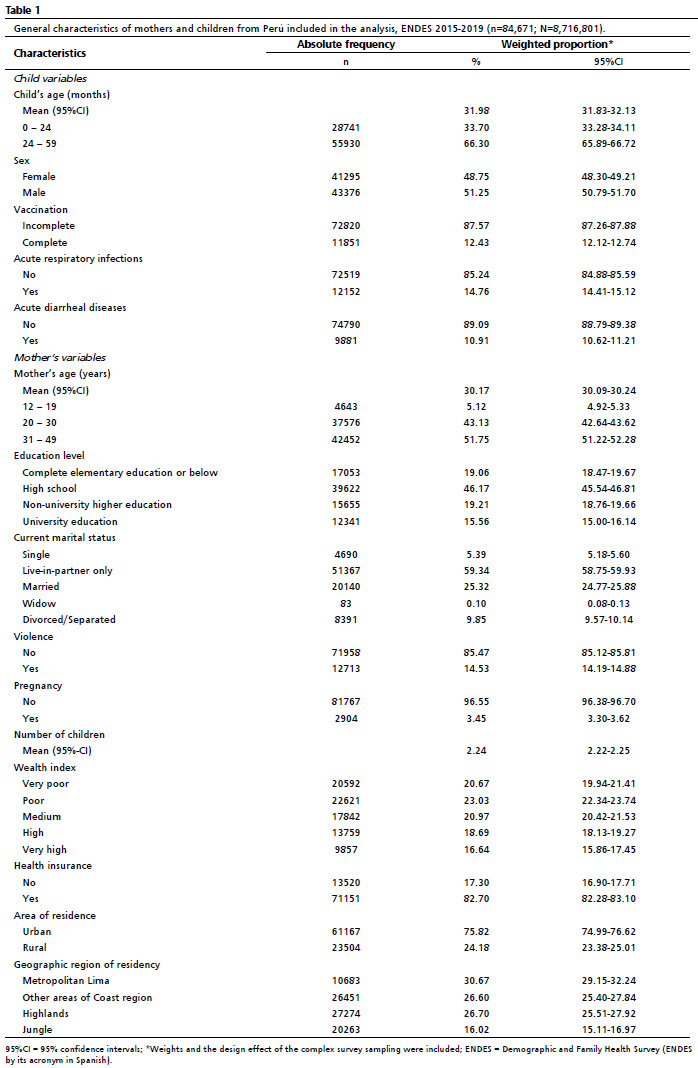
ResultsRegarding children, 51.25% were male, and the mean age was 31.98 (31.83-32.13) months old. Only 12.43% had completed their vaccination schedule according to their age. The prevalence of ARIs and AD was 14.76% and 10.91%, respectively. Regarding mothers, the mean age was 30.17 (30.09-30.24). Of them, 46.17% had a secondary level; 59.34% had a domestic partner; 82.70% had health insurance; almost half were poorer (23.03%) or the poorest (20.67%). Only 3.45% were pregnant when they were surveyed. The average number of children per mother was 2.24 (2.22-2.25). In addition, 14.53% of mothers mentioned being victims of intimate partner violence. 75.82% resided in an urban area and 30.67% in Lima Metropolitan (Table 1).
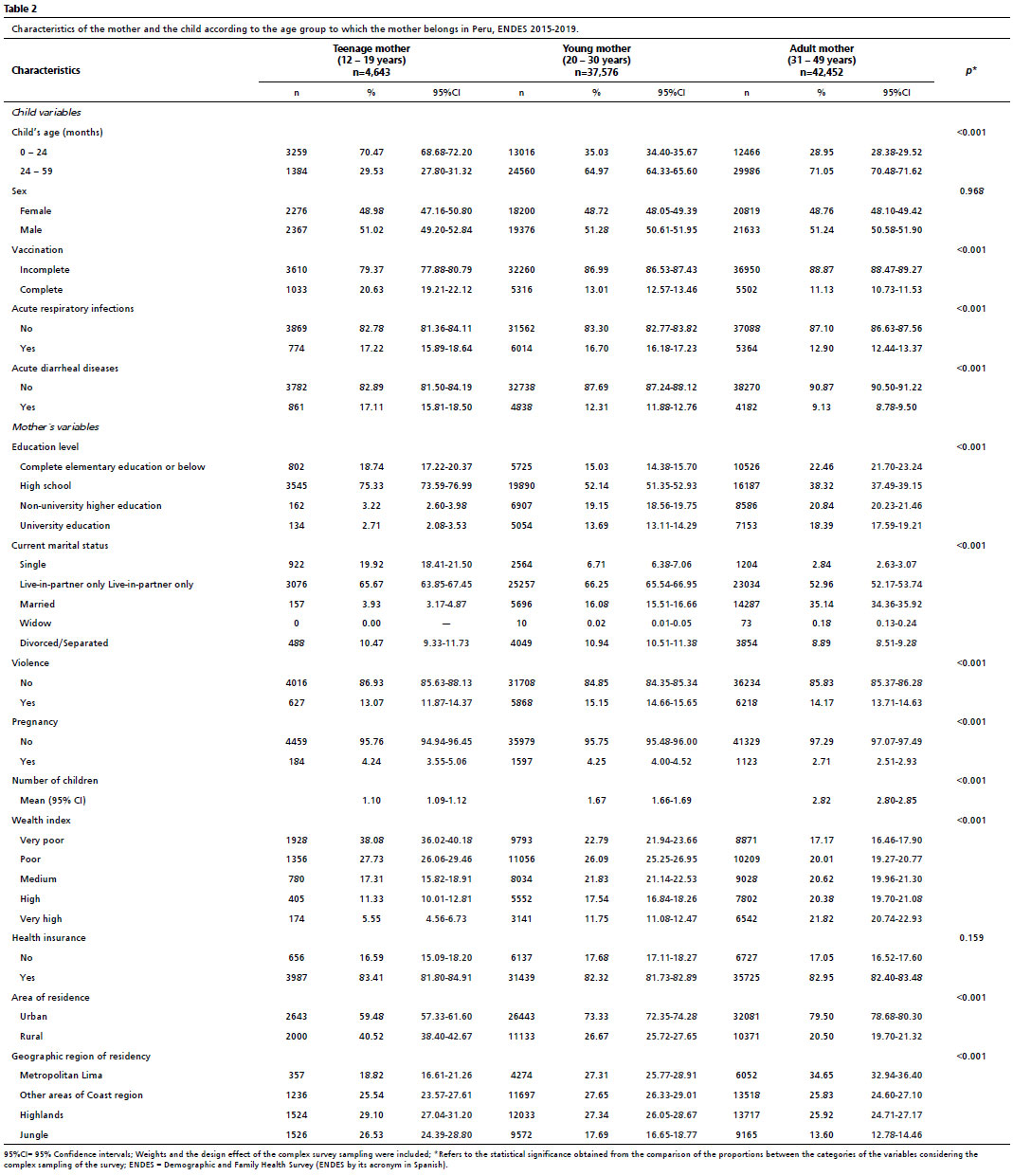
Regarding ARIs, the prevalence of this condition was 17.22%, 16.70%, and 12.90% in children under five of teenage, young, and adult mothers, respectively. Concerning AD, the prevalence in these children was 17.11%, 12.31%, and 9.13% in children under five of teenage, young, and adult mothers, respectively. Bivariate analysis by mothers’ age group showed statistically significant differences for all variables, except children’s sex and health insurance (Table 2).
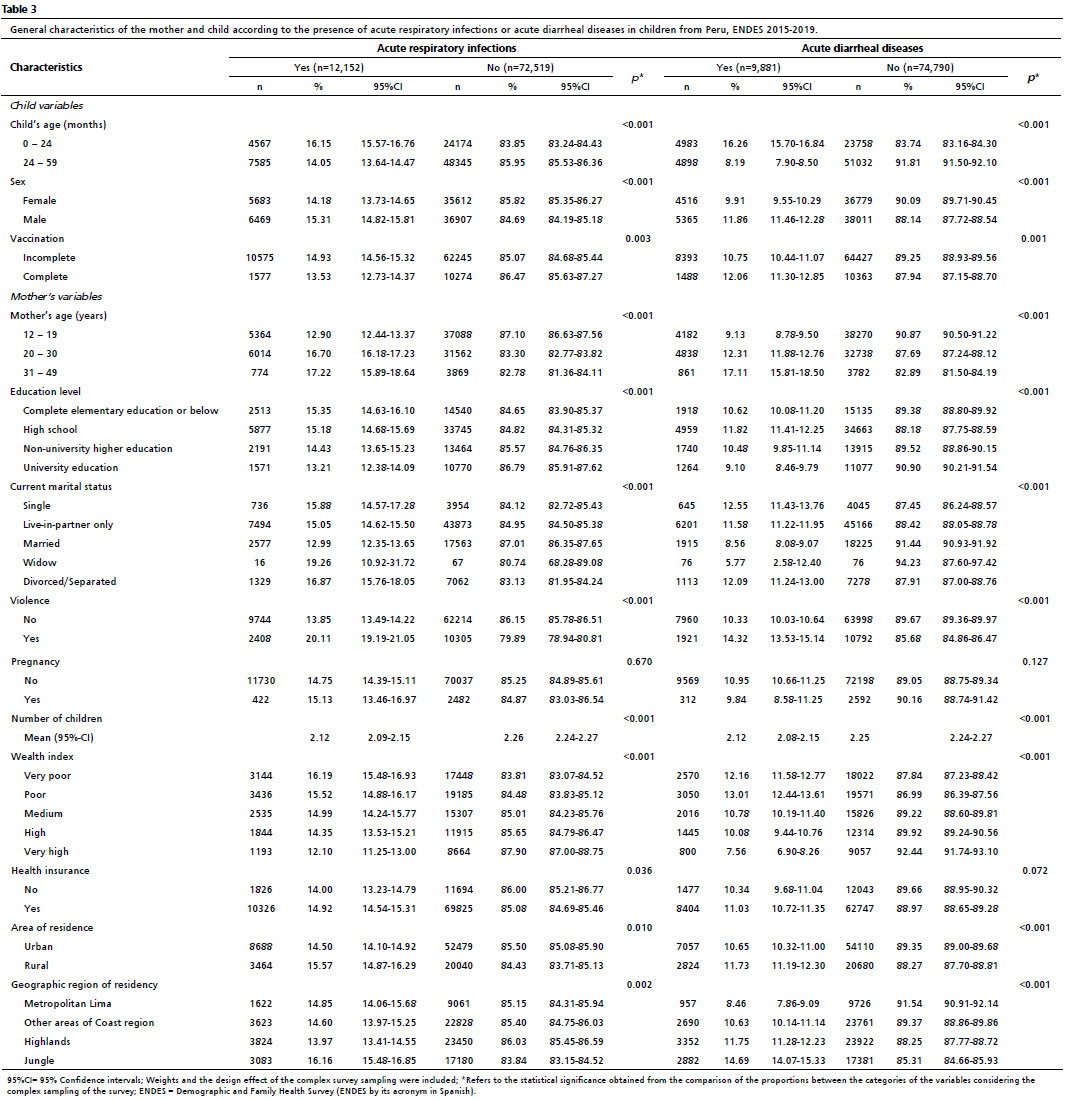
Bivariate analysis according to the presence of ARIs in children showed statistically significant differences for all variables except for pregnancy, while the bivariate analysis according to the presence of AD in children showed statistically significant differences for all variables except for pregnancy and health insurance (Table 3).
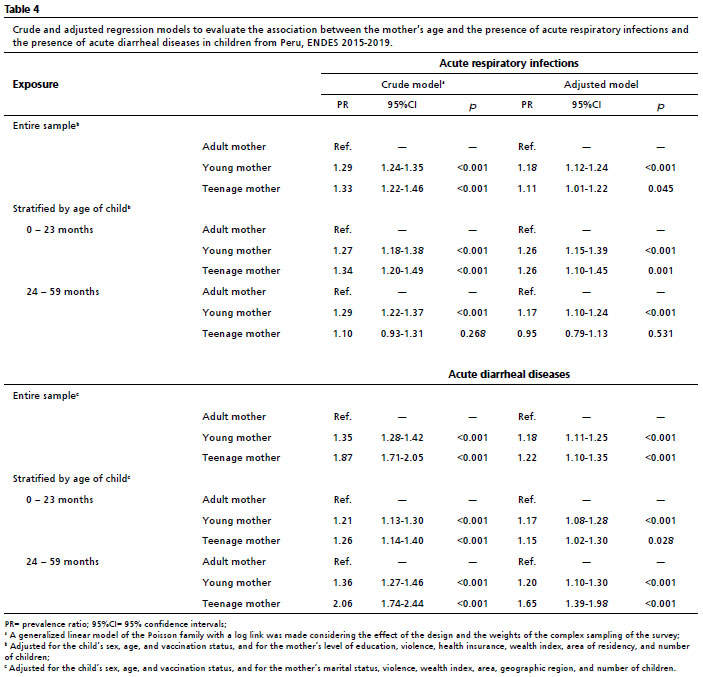
In the adjusted model, being a young (aPR= 1.18; 95%CI= 1.12-1.24;
p<0.001) or teenage mother (aPR= 1.11; 95%CI= 1.01-1.22;
p=0.045) was associated with ARIs in children, in comparison with adult mothers’ children. In the stratified analysis according to children’s age, in children under 23 months old, the association with ARIs remained in children whose mothers are young (aPR= 1.26; 95%CI= 1.15-1.39;
p<0.001) or teenage (aPR= 1.26; 95%CI= 1.10-1.45;
p=0.001), in comparison with adult mothers’ children. In children from 24 to 59 months old, the association with ARIs was only found in young mothers’ children (aPR= 1.17; 95%CI= 1.10-1.24;
p<0.001) in comparison with adult mothers’ children (Table 4).
In the adjusted model, we found that being a young mother (aPR= 1.18; 95%CI= 1.11-1.25;
p<0.001) or a teenage one (aPR= 1.22; 95%CI= 1.10-1.35;
p<0.001) was also associated with higher prevalence of AD cases in their children, in comparison with adult mothers’ children. The stratified analysis showed a higher prevalence of AD in children under 23 months old whose mothers are young (aPR= 1.17; 95%CI= 1.08-1.28;
p<0.001) or teenage (aPR= 1.15; 95%CI=1.02-1.30;
p=0.007), in comparison with adult mothers’ children. Similarly, in children from 24 to 59 months old, we found a higher prevalence of AD cases in young mothers’ children (aPR= 1.20; 95%CI= 1.10-1.30;
p<0.001) and teenage mothers’ children (aPR= 1.65; 95%CI= 1.39-1.98;
p<0.001), in comparison with adult mothers’ children (Table 4).
DiscussionThis study aimed to assess the association between mother’s age and the presence of ARIs and AD in children under five years old. We found that ARIs cases as well as AD cases showed a greater proportion in children of teenage and young mothers, in comparison with children of adult females. Thus, we could identify a group of children in which these health problems would be more prevalent and would demand the development of strategies oriented to the prevention of these groups of diseases.
In relation to mother’s age and the presence of AD in children under five years old, it was found that being a young or adolescent mother is related to a higher proportion of AD in children. Previous studies indicate that low educational level, as well as lack of hygiene, are related to higher prevalence of AD in children under the age of five.
18,19 The study’s finding could be explained by the fact that an adolescent mother would probably have fewer years in the educational system than older mothers, which could translate into lower access to knowledge of AD, hygiene measures, and preventing diseases in infancy. In addition, given the current dynamic and fertility rate in Peru, it is more probable that a young mother has fewer children than an adult mother or that the analyzed information corresponds to her only child, which implies a lower experience concerning childcare; this could increase the risk of infections. Given that most of the factors associated with AD development in children under five years old are preventable, strategies should be implemented to limit the development of this disease, focused on groups such as teenage and young mothers.
20 These strategies should promote the increase of knowledge about the prevention and treatment of the disease, as well as hygiene measures for mothers and children, which would be useful for controlling AD.
21Concerning ARIs, it was found that the children of mothers in younger age groups (teenage and young people) had a greater probability of presenting this outcome. In the literature, it is described that educational level, specifically a low educational level of parents, is a factor related to the presence of ARIs in children under the age of five, which is present in low- and middle-income countries.
22 As it was described for AD, the lower age of a mother could be related to a lower level of knowledge of preventive measures and hygiene for children under five years old, which is a possible explanation for the reported finding. A higher educational level would not only be related to a lower number of ARIs cases but also to a higher identification of alarm signs in children under five years old with ARIs.
23 Hence, educational strategies to face this problem should focus on increasing the knowledge about this disease in teenage and young mothers. This knowledge should include preventive measures and alarm sign identification since it is relevant in the Peruvian population, as ARIs continues to be one of the main causes of death in Peru’s children under five years old.
24,25 In addition, ARIs prevention is important in times of low temperatures, when, historically, higher morbidity and mortality rates are evidenced due to this problem in the Peruvian population under the age of five.
25In Peru, there is a decrease in the number of AD episodes in children under five years old attended annually (2014 to 2019: decrease from 600,000 to close to 400,000 cases).
26 Similarly, there is a reduction in the number of ARIs medical attention.
25,27 Despite this, both health problems constitute part of Peru’s leading cause of morbidity and mortality in children under five. After 2019, during the COVID-19 pandemic in Peru, there has been a decrease in AD and ARIs cases in children under five years old, which can be attributed to lower exposure to social contact in this population subgroup, at school as well as at home and in public places
28,29 and due to the measurements to control COVID-19 transmission in the general population.
28 Because of this, identifying a children subgroup (those with adolescent or young mothers) with a higher probability of presenting ARIs or AD is crucial to the development of strategies to regulate or decrease the expected increase in cases of ARIs and AD in children under five years after COVID-19 pandemic was controlled.
Regarding the study limitations, given that in this study a secondary database was used (ENDES), some characteristics that can allow a better characterization of the study population could not be considered as covariates for the adjusted analysis used to evaluate the association between the variables of interest since they were not available. In addition, memory bias and social desirability bias could be present because the respondent mothers self-reported information on many characteristics included in the study. Moreover, the study’s cross-sectional design does not allow the analysis of causality between the variables of interest. Despite the above, we consider that the use of a database (ENDES), whose methodology is widely used in the world (Demographic Health Survey methodology),
30 which has methodological quality controls whose sample allows the obtaining of representative results of the Peruvian population at the national and regional level, and that is used for the study of different health indicators in Peruvian populations, is an adequate source of information for the studied problem.
In conclusion, mothers’ age was found to be associated with the presence of ARIs and AD in children under five. Children under five years old whose mothers are teenagers or youngsters show greater proportions of ARIs and AD compared to adult mothers’ children. Thus, being a child of an adolescent or young mother is related to the presence of respiratory and digestive infectious diseases in children under five years old. Hence, strategies to reduce ARIs and AD, including the enhancement of promotion of healthy lifestyles and prevention of infectious diseases, can be developed, prioritizing resources for the children of teenage and young mothers.
References1. Sevillano Jimenez JA, Contreras Pulache HL. Pediatric diseases more frequently: a peruvian perspective. Rev Fac Med Hum. 2021 Sep; 21 (4): 905-6.
2. Minisiterio de Salud (Peru). Número de episodios de neumonías en menores de 5 años, Perú 2019–2024. Centro Nacional de Epidemiología, Prevención y Control de Enfermedades; 2024. Pagina 1. [access in 2024 Jul 5]. Available from:
https://www.dge.gob.pe/portal/docs/vigilancia/sala/2024/SE01/neumonias.pdf3. Ministerio de Salud (Peru). Distribución de episodios de EDA por grupo de edad, Perú 2021. Centro Nacional de Epidemiología, Prevención y Control de Enfermedades; 2021. Page 8. [access in 2022 Aug 30]. Available from:
https://www.dge.gob.pe/portal/docs/vigilancia/sala/2021/SE07/edas.pdf4. Demissie GD, Yeshaw Y, Aleminew W, Akalu Y. Diarrhea and associated factors among under five children in sub-Saharan Africa: Evidence from demographic and health surveys of 34 sub-Saharan countries. PLoS One. 2021 Sep; 16 (9): e0257522.
5. Beletew B, Bimerew M, Mengesha A, Wudu M, Azmeraw M. Prevalence of pneumonia and its associated factors among under-five children in East Africa: A systematic review and meta-analysis. BMC Pediatr. 2020 May; 20 (254): 1-13.
6. Azevedo WF, Diniz MB, Fonseca ES, Azevedo LM, Evangelista CB. Complications in adolescent pregnancy: systematic review of the literature. Einstein. 2015; 13 (4): 618-26.
7. Instituto Nacional de Estadística e Informática (INEI). Mortalidad Infantil en la Niñez. In: Encuesta Demográfica y de Salud Familiar; 2019. p. 12.
8. Bellieni C. The Best Age for Pregnancy and Undue Pressures. J Fam Reprod Health. 2016; 10 (3): 104-7.
9. Basu S, Gorry D. Consequences of teenage childbearing on child health. Econ Hum Biol. 2021 Aug; 42: 101019.
10. PAHO/WHO/UNFPA/UNICEF. Acelerar el progreso hacia la reducción del embarazo en la adolescencia en América Latina y el Caribe [Internet]. UNICEF; 2016 [access in 2022 Aug 30]. 56 p. Available from:
https://www.unicef.org/lac/media/1336/file/PDF_Acelerar_el_progreso_hacia_la_reducción_del_embarazo_en_la_adolescen.pdf11. Isaza XC, Cabrera O, Reingold R, Grossman D. Stolen Lives: a multi-country study on the health effects of forced motherhood on girls 9–14 years old. OSAR National Network; 2015. 104 p. [access in 2022 Aug 30]. Available from:
https://www.plannedparenthoodaction.org/uploads/filer_public/db/6d/db6d56cb-e854-44bb-9ab7-15bb7fc147c5/ppfa-stolen-lives-english.pdf12. Instituto Nacional de Estadística e Informática (INEI). Ficha Técnica – Encuesta Demográfica y de Salud Familiar. INEI; 2019. [access in 2022 Aug 30]. Available from:
http://iinei.inei.gob.pe/iinei/srienaho/Descarga/DocumentosMetodologicos/2019-5/FichaTecnica.pdf13. Ministerio de Salud (Peru). Atención Integral en Centros y Puestos de Salud del Minsa. Guía para el profesional del Serums [Internet]. 1996. [access in 2022 Aug 30]. Available from:
https://www.gob.pe/institucion/minsa/informes-publicaciones/321017-atencion-integral-en-centros-y-puestos-de-salud-del-minsa-guia-para-el-profesional-del-serums14. Hernández-Vásquez A, Vargas-Fernández R, Turpo Cayo EY. Determinants, inequalities, and spatial patterns of diarrhea in the Peruvian under-five population: findings from nationally representative survey data. Front Public Health. 2023 Jun; 11: 1170670.
15. Ministerio de Salud (Peru). N°141-MINSA/2018/DGIESP: Norma técnica de salud que establece el Esquema Nacional de Vacunación [Internet]. 2018. p. 01–105. Available from:
https://cdn.www.gob.pe/uploads/document/file/300034/d177030_opt.PDF16. Burgos-Muñoz RM, Soriano-Moreno AN, Bendezu-Quispe G, Urrunaga-Pastor D, Toro-Huamanchumo CJ, Benites-Zapata VA. Intimate partner violence against reproductive-age women and associated factors in Peru: evidence from national surveys, 2015–2017. Heliyon. 2021 Jul 1; 7 (7): e07478.
17. Instituto Nacional de Estadística e Informática (INEI). MICRODATOS. BASE DE DATOS [Internet]. [access in 2024 Apr 22]. Available from:
https://proyectos.inei.gob.pe/microdatos/18. Anteneh ZA, Andargie K, Tarekegn M. Prevalence and determinants of acute diarrhea among children younger than five years old in Jabithennan District, Northwest Ethiopia, 2014. BMC Public Health. 2017 Jan;17 (1): 99.
19. Desmennu AT, Oluwasanu MM, John-Akinola YO, Opeyemi O, Ayo AS. Maternal education and diarrhea among children aged 0-24 months in Nigeria. Afr J Reprod Health. 2017; 21 (3): 27-36.
20. Ministerio del Ambiente (Peru). INEA | Informe Nacional sobre el Estado del Medio Ambiente. 2021. Niños y niñas menores de 5 años afectados con EDA, según departamento, 2014-2019 (Número de atendidos). [access in 2022 Jul 29]. Available from:
https://sinia.minam.gob.pe/inea/indicadores/ninosas-menores-de-5-anos-afectados-con-enfermedades-diarreicas-agudas-segun-departamento-2020-2019-numero-de-atendidos/21. World Health Organization (WHO). The integrated Global Action Plan for Prevention and Control of Pneumonia and Diarrhoea (GAPPD) [Internet]. WHO & UNICEF; 2022. [access in 2022 Aug 31]. Available from:
https://www.who.int/publications/i/item/the-integrated-global-action-plan-for-prevention-and-control-of-pneumonia-and-diarrhoea-(gappd)22. Mathew JL, Patwari AK, Gupta P, Shah D, Gera T, Gogia S, et al. Acute respiratory infection and pneumonia in India: A systematic review of literature for advocacy and action: UNICEF-PHFI series on newborn and child health, India. Indian Pediatr. 2011; 48: 191-218.
23. Domínguez Anaya RD, Tapia Caez E, Hernández Escolar J, Castillo Avila IY. Edad y nivel educativo asociados al conocimiento sobre signos de alarma para infecciones respiratorias en madres adolescentes. Rev Cuid. 2017 May; 8 (2): 1628-37.
24. Organización Panamericana de la Salud (OPS). Infecciones respiratorias agudas en el Perú: Experiencia frente a la temporada de bajas temperaturas. Lima: OPS/OMS; 2014. [access in 2022 Aug 31]. Available from:
https://iris.paho.org/bitstream/handle/10665.2/28549/iras2014-spa.pdf25. Ministerio de Salud (Peru). Centro Nacional de Epidemiología, Prevención y Control de Enfermedades. Boletín Epidemiológico del Perú SE 02-2020. Lima: Ministerio de Salud; 2020. v.29 (2): 32–59. [access in 2022 Aug 31]. Available from:
http://www.dge.gob.pe/portal/docs/vigilancia/boletines/2020/02.pdf26. Ministerio del Ambiente (Peru). Informe Nacional sobre el Estado del Ambiente 2014-2019. Niños y niñas menores de 5 años afectados con Enfermedades Diarreicas Agudas según departamento, 2014-2019. 2021. Page 166. [access in 2024 Jul 5]. Available from:
https://repositoriodigital.minam.gob.pe/handle/123456789/72227. Ministerio del Ambiente (Peru). Perú: Anuario de Estadísticas Ambientales. Atenciones de niños/as menores de 5 años afectados con infecciones respiratorias agudas, según departamento, 2012-2021. 2022. Page 494. [access in 2024 Jul 5]. Available from:
https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1877/libro.pdf28. Kadambari S, Goldacre R, Morris E, Goldacre MJ, Pollard AJ. Indirect effects of the covid-19 pandemic on childhood infection in England: population based observational study. BMJ. 2022 Jan; 376: e067519.
29. Diesner-Treiber SC, Voitl P, Voitl JJM, Langer K, Kuzio U, Riepl A, et al. Respiratory Infections in Children During a Covid-19 Pandemic Winter. Front Pediatr. 2021 Oct 18; 9: 1132.
30. The DHS Program - Quality information to plan, monitor and improve population, health, and nutrition programs [Internet]. [access in 2024 Apr 22]. Available from:
https://dhsprogram.com/Authors’ contributionBenites-Meza JK, Herrera-Añazco P, Carreazo NY, Bendezu-Quispe G, Soriano-Moreno AN, Benites-Zapata VA: conceptualization, formal analysis, interpretation of results, writing-original draft, writing-review & editing. All authors approve the final version of the article and declare no conflict of interest.
Received on May 26, 2023
Final version presented on June 10, 2024
Approved on June 13, 2024
Associated Editor: Lygia Vanderlei


 ; Percy Herrera-Añazco 2
; Percy Herrera-Añazco 2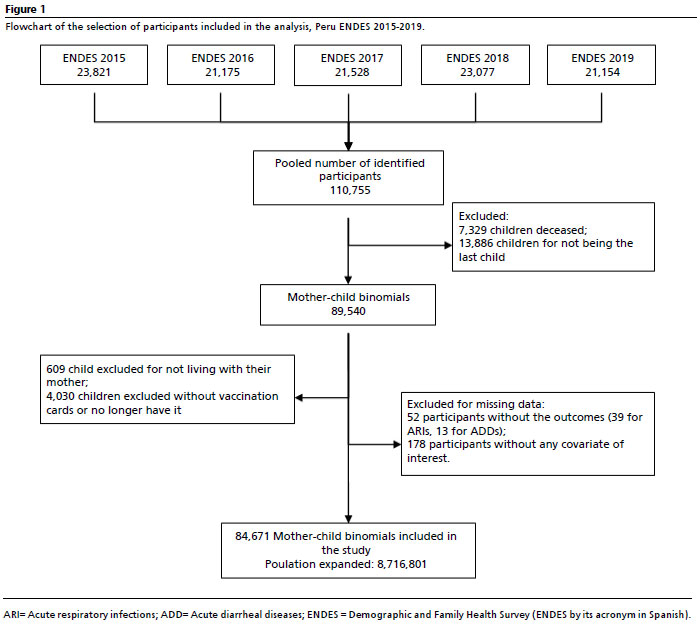






 Ler em português
Ler em português