ABSTRACT
OBJECTIVES: to evaluate patients' satisfaction of mixed prenatal care during the COVID-19 pandemic in a tertiary hospital in Lima, Peru.
METHODS: we conducted a cross-sectional evaluation of satisfaction in patients receiving mixed prenatal care that includes in-person and virtual visits. All women who gave a written consent between June and July 2021 were included. The survey was based on the Short Assessment of Patient Satisfaction (SAPS) scale which evaluated seven dimensions of satisfaction: access and facilities, effectiveness, information, technical skills, participation, relationship, and general satisfaction.
RESULTS: the overall satisfaction on mixed prenatal care was 3.28 ± 0.71. The mean SAPS score was 33.88 (SD = 5.56). In total, 144 patients (65%) preferred the mixed prenatal care. The mean maternal age of 221 included pregnant women was 30 years and the mean gestational age at the first appointment was 24 weeks. Overall, 88.2% of patients had up to 6 visits among virtual and in-person. Patients with non-health insurance had lower rates of satisfaction when compared with pregnant women with national health insurance (p=0.026).
CONCLUSIONS: women receiving the mixed prenatal care during the COVID-19 pandemic reported a high level of satisfaction. In general, pregnant women would recommend mixed prenatal care.
Keywords:
Prenatal care, Patient satisfaction, Telemedicine, COVID-19 pandemic
RESUMO
OBJETIVOS: evaluar la satisfacción de las pacientes con la atención prenatal mixta durante la pandemia de COVID-19 en un hospital terciario de Lima, Perú.
MÉTODOS: realizamos una evaluación transversal de la satisfacción en pacientes que recibieron atención prenatal mixta, que incluyó consultas presenciales y virtuales. Se incluyeron todas las mujeres que dieron su consentimiento por escrito entre junio y julio de 2021. Se aplico la escala Short Assessment of Patient Satisfaction (SAPS), que evaluó siete dimensiones de satisfacción: acceso e instalaciones, efectividad, información, habilidades técnicas, participación. relación y satisfacción general.
RESULTADOS: la satisfacción global con la atención prenatal mixta fue de 3,28±0,71. La puntuación media del SAPS fue 33,88 (DE = 5,56). En total, 144 pacientes (65%) prefirieron la atención prenatal mixta. La edad materna promedio de las 221 gestantes incluidas fue de 30 años y la edad gestacional promedio en la primera consulta fue de 24 semanas. En total, el 88,2% de los pacientes realizaron hasta 6 consultas entre virtuales y presenciales. Los pacientes sin seguro de salud tuvieron menores índices de satisfacción en comparación con las mujeres embarazadas con seguro de salud público (p=0,026).
CONCLUSIONES: Las mujeres que recibieron atención prenatal mixta durante la pandemia de COVID-19 reportaron un alto nivel de satisfacción. En general, las mujeres embarazadas recomendarían atención prenatal mixta.
Palavras-chave:
Atención prenatal, Satisfacción del paciente, Telemedicina, Pandemia de COVID-19
IntroductionPrenatal care is an important public health intervention and one of the most common preventive healthcare worldwide.
1 The traditional model involves evaluating patients every 4 weeks until the 28
th week, then every 2 weeks until the 36
th week, and then weekly until delivery. Thus, pregnant women should have at least 14 in-person visits in a routine schedule.
1-3 At the beginning of the COVID-19 pandemic, every outpatient clinic in our country was shut down and healthcare was offered exclusively in the health centers emergency departments.
4 This situation forced the healthcare institutions to implement different approaches to prenatal care to ensure access to prenatal services with less risk of exposure and spread of COVID-19,
5-8 minimizing the occurrence of adverse maternal and perinatal outcomes.
9Telemedicine was incorporated into the new model, and virtual visits provided guidance on pregnancy and psychosocial support endorsed by international institutions and experiences.
6,10The new mixed prenatal care model includes in-person visits scheduled around specific evidence-based services that could only be delivered in-person, such as ultrasounds and laboratory analysis, depending on the assessment of risk factors.
4,5,10-14While some studies support the safety of reducing the frequency of prenatal visits,
7,15 evidence on satisfaction in pregnant women receiving the mixed prenatal care model during the COVID-19 pandemic has not been found. Thus, this pandemic provides the opportunity to evaluate the new healthcare approach to modify and improve the quality and efficiency of pregnancy healthcare services, from the patients’ perspective for inclusion in monitoring care and legitimizing the health policy.
16,17The aim of this study is to evaluate the patients’ satisfaction of the new mixed prenatal care, which our institution implemented during the COVID-19 pandemic in Peru.
MethodsWe conducted a cross-sectional evaluation of satisfaction among patients receiving the new mixed prenatal care.
8 The
Instituto Nacional Materno Perinatal is the largest public, academic and referral center in Lima-Peru for perinatal care. It is fully dedicated in providing health care to women, particularly for high-risk pregnant women and their newborns, and houses approximately 16,000 deliveries per year. The new model was implemented in August 2020, in agreement with published national and international guidelines
5,18-20 (Figure 1).
All women receiving prenatal care at our institution at any gestational age, with at least one virtual and one in-person visit and who gave a written consent to participate in the survey were included in the study. Instruments with incomplete information were excluded. We conducted the survey from June to July 2021.
The satisfaction survey was conducted at the end of the in-person medical consult. It was a short, paper-and-pencil based survey in a comprehensive language. It was based on an instrument used previously in satisfaction with health care treatment by Hawthorne
et al.16and was validated in focus groups with patients to improve vocabulary and understanding of the questions. The survey was divided into two sections: the first section includes questions about epidemiological characteristics. The second section includes 11 questions that were measured on a 5-point Likert scale, which varies for each question from “strongly disagree” to “strongly agree” (0 to 4) and one open question about suggestions to improve the mixed prenatal care. Based on the Short Assessment of Patient Satisfaction (SAPS) scale,
16 our survey evaluated seven dimensions of satisfaction: i)
access and facilities (3 questions), ii)
effectiveness (1 question), iii)
information (1 question), iv)
technical skills (2 questions), v)
participation (1 question), vi)
relationship (2 questions), and vii)
general satisfaction (1 question). We added four questions to the original SAPS scale in order toevaluate the two components of mixed prenatal care: virtual and in-person visits. (Supplemental 1) Therefore, the range of total score was 0–44, where higher scores represent higher levels of patients’ satisfaction. We added two questions about prenatal care-type preferences and whether the patient would recommend anew care model. Risk factors and additional information about pregnancy characteristics were obtained directly from the patients and electronic records.
We performed a descriptive analysis, and the distribution of absolute and relative frequencies of categorical variables was calculated. For numerical variables, summary measures were applied as averages and ranges. All the information from paper surveys were transferred into MS Excel 2013. The satisfaction was evaluated by summing the answers of all participants for each point on the Likert scale and represented as mean and standard deviation. In the bivariate analysis, the Mann–Whitney U-test for continuous data that are not normally distributed was used to analyze the SAPS score for the questions on the level of satisfaction and the characteristics of the obstetric population. A relevant significance level less than0.05 was used. Statistical analysis was performed using the Stata Statistical Software 14.0 (Stata Corp. 2015, College Station, TX, USA).
This study was part of a larger institutional study on COVID-19 (reference number: 063-2020-DG-N°20-OEAIDE/INMP), which was approved by the local Ethical Institutional Board (reference number: 027-2021-CIEI/INMP) on May 31, 2021.
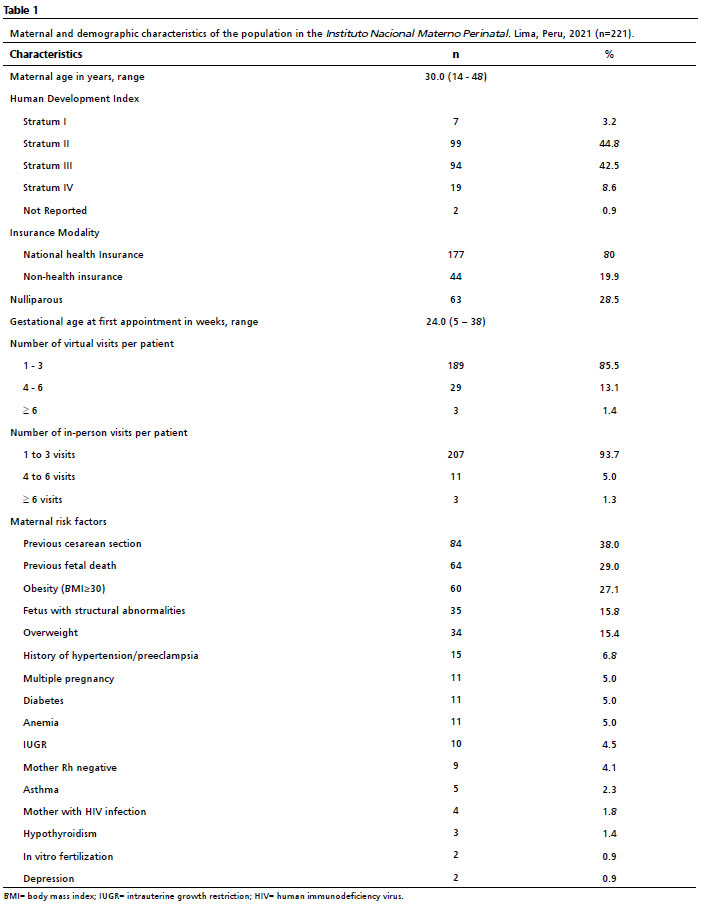
ResultsTable 1 shows the characteristics of 221 pregnant women receiving mixed prenatal care who met the inclusion criteria and agreed to participate in the study. The mean maternal age was 30 ± 6.9 years. The mean gestational age at the first appointment was 24 ± 8.9 weeks. The distribution according to trimester was as follows: 15 (6.8%) during the first trimester, 64 (29.0%) during the second trimester, and 142 (64.2%) during the third trimester. The average duration of mixed prenatal care was 4.8 weeks; 189 patients (85.5%) had between 1 and 3 virtual visits and 207 patients (93.7%) had between 1 and 3 in-person visits. Overall, 88.2% of patients had up to 6 visits among virtual and in-person. The most common maternal risk factor was previous cesarean sections, that was present in 84 out of 221 patients (38.0%).
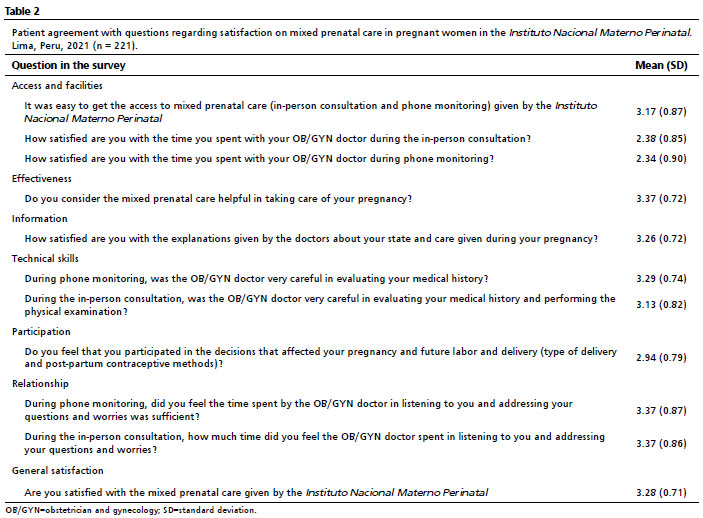
Table 2 shows the seven dimensions of satisfaction on mixed prenatal care. Pregnant women were satisfied with the
access and facilities,
effectiveness,
information,
technical skills, participation and
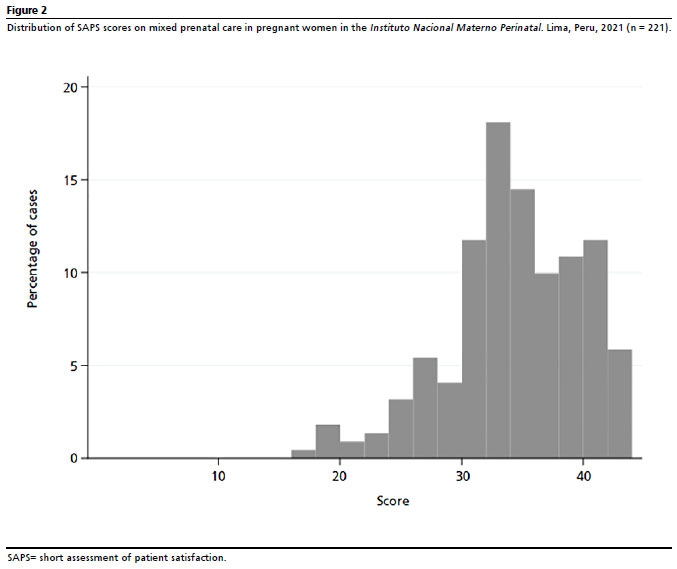
relationship. The overall satisfaction on mixed prenatal care was 3.28 ± 0.71. The distribution of SAPS scores is presented in Figure 2. The study found that no pregnant women was dissatisfied (no patient with a score less than 16). The mean SAPS score was 33.88% (SD = 5.56), which was at the 75
th percentile of the possible score range. Seven patients (3.2%) obtained the ceiling score.
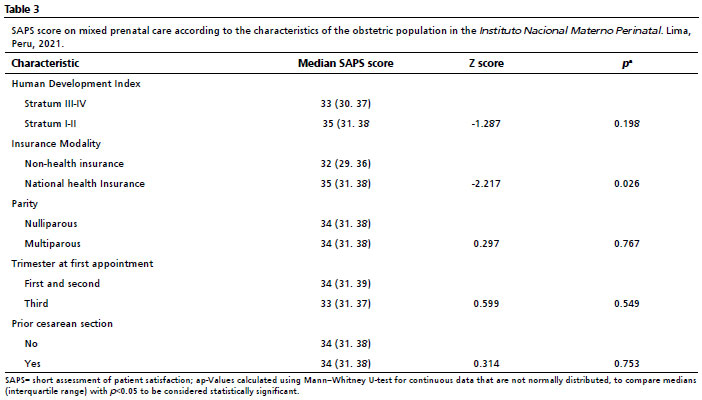
Only the characteristics related to insurance modality had a statistically significant difference with lower rates of satisfaction from those with non-health insurance when compared with pregnant women with national health insurance (
p=0.026) (Table 3). Though statistically significant, none of these categories were found to be clinically significant since the median for both was in the SAPS score range of being satisfied.
In total, 144 patients (65%) preferred the mixed prenatal care and 71 (32%) were in favor of in-person visits. In addition, 198 (89.5%) would recommend mixed prenatal care to their family and friends.
DiscussionThis study evaluates satisfaction in patients receiving the mixed model of prenatal care that consists of in-person visits combined with telephone consultation during the COVID-19 pandemic. The assessment of satisfaction was mostly positive with an overall satisfaction of 3.28 ± 0.71.
Some new models of prenatal care implemented with telemedicine have reported positive maternal and fetal outcomes.
15,21-24 However, there is a need to determine the time and frequency of visits and assess the prenatal care that could be given entirely through phone calls.
10 Furthermore, alternative visit schedules and telemonitoring could be integrated into the healthcare system without compromising the patients’outcomes or satisfaction .
21 Thus, exploring patient satisfaction is crucial before further implementing any mixed prenatal care.
Research in nonpregnant population, conducted prior to the COVID-19 pandemic, has shown that telemedicine is effective in providing patient care, improving access, and reducing costs, but high-quality evidence is lacking.
25 For the general population, advantages of telemedicine included reducing waiting time, ease of scheduling, and increased feeling of connections with healthcare providers; however, lack of training with technology, lack of privacy at home, and connectivity issues are reported as disadvantages.
26Regarding the pregnant women population, Balk
et al.27 on a systematic review with low-strength evidence could not report differences in rates of preterm births or neonatal intensive care unit admissions between patients who had mixed care or traditional antenatal care. However, they did suggest high satisfaction with antenatal care in patients having mixed care.
27 With this evidence that provided no sign of harm of nontraditional antenatal care (fewer scheduled visits and use of telemonitoring), it was observed that maternal health units, healthcare providers, and patients had greater comfort in following alternative care models.
27 Previously, we reported feasibility and acceptability among healthcare providers on mixed prenatal care
9 and highly accepted introduction of a novel mobile app as a tool of a mixed model of prenatal care by the patients.
28Here, we considered seven domains of patients’ satisfaction, of which five had the highest points with an overall satisfaction on mixed prenatal care in the 75
th percentile of the possible score range. Women who prefer traditional care rather than mixed care are highly motivated by a desire to interact face to face with the healthcare provider at every opportunity and not to have all consultations by phone. Thus, Pflugeisen
et al.23 suggested that we must uphold a choice-based model for patients. Further work is needed to better understand the motivating factors for the selection of virtual and traditional care paradigms. In fact, some patients may prefer fewer visit and mixed visit options, thereby reducing the cost of frequent visits. However, with increased evidence on the alternative models causing no harm, it is likely that many patients and healthcare providers would choose the mixed prenatal care.
We attempted to assess the heterogeneity of patients’ satisfaction by evaluating the subgroups. There were lower rates of satisfaction in patients with non-health insurance. However, we did not analyze how mixed visit structures may adversely affect pregnant women due to factors such as internet access, type of pathologies in pregnancy, and other social determinants of health since socioeconomically or medically disadvantaged patients may face difficulty in having successful virtual consultations.
29The main strength of our study is that this is the first report on patients’ satisfaction in pregnant woman receiving the mixed prenatal care during the COVID-19 pandemic in our region. Some limitations are as follows: first, the instrument used (SAPS scale) has not been evaluated for its psychometric properties and its adaptation to Spanish, however, although SAPS scale needs further validation in another context, Howthorne
et al.16 report that it is based on a firm theoretical model of patients’ satisfaction and may be used in a wide range of settings. Second, our population is heterogeneous with regard to the number of in-person and virtual visits, which potentially could influence the experience on mixed perinatal care; third, most patients had the first appointment during the third trimester of pregnancy; and fourth, there was no comparison between patients’ satisfaction on traditional prenatal care and mixed prenatal care.
In conclusion, women receiving the mixed prenatal care during the COVID-19 pandemic reported a high level of satisfaction. The lowest rates of satisfaction were reported in patients with non-health insurance. Overall pregnant women would recommend mixed prenatal care.
Referencias1. Guidelines for Perinatal Care. 8
th edition. American Academy of Pediatrics and American College of Obstetricians and Gynecologists (ACOG). [
Internet] Washington (DC): ACOG; 2017. [access in 2022 Dez 9]. Available from:
https://www.acog.org/clinical-information/physician-faqs/-/media/3a22e153b67446a6b31fb051e469187c.ashx2. Ministerio de Salud (Peru). Norma Técnica de Salud para la Atención Integral de Salud Materna, aprobada por Resolución Ministerial N° 827-2013/MINSA. Lima-Perú: Ministerio de Salud; 2014. [access in 2022 Dez 9]. Available from:
https://cdn.www.gob.pe/uploads/document/file/202170/198935_RM827_2013_MINSA.pdf20180926-32492-1iuyz6n.pdf3. Alexander GR, Kotelchuck M. Assessing the role and effectiveness of prenatal care: history, challenges, and directions for future research. Public Health Rep. 2001; 116 (4): 306-16.
4. Aziz A, Zork N, Aubey JJ, Baptiste CD, D’Alton ME, Emeruwa UN,
et al. Telehealth for High-Risk Pregnancies in the Setting of the COVID-19 Pandemic. Am J Perinatol. 2020; 37: 800-8.
5. Peahl AF, Smith RD, Moniz MH. Prenatal care redesign: creating flexible maternity care models through virtual care. Am J Obstet Gynecol. 2020; 223: 389.e1-e10.
6. Fryer K, Delgado A, Foti T, Reid CN, Marshall J. Implementation of obstetric telehealth during COVID-19 and beyond. Matern Child Health J. 2020; 24: 1104-10.
7. Alves DS, Times VC, Silva EMA, Melo PSA, Araújo Novaes M. Advances in obstetric telemonitoring: a systematic review. Int J Med Inform. 2020; 134: 104004.
8. Meza-Santibañez L, Novoa RH, Torres-Osorio J, Jáuregui-Canchari V, Rodríguez-Hilario N, Guevara-Ríos E,
et al. Implementation of a mixed model of inperson and virtual prenatal care during the COVID-19 pandemic at the National Maternal Perinatal Institute in Lima-Peru. Rev Peru Ginecol Obstet. 2021; 67: 1-8.
9. Novoa RH, Meza-Santibañez L, Melgarejo WE, Huang-Yang X, Guevara-Ríos E, Torres-Osorio J,
et al. Maternal perinatal telemonitoring in the context of the coronavirus disease 2019 pandemic in a tertiary health center in Peru. Am J Perinatol. 2022 Nov; 39 (15): 1711-8.
10. American College of Obstetricians and Gynecologists (ACOG).ACOG Committee Opinion Number 798. Implementing Telehealth in Practice. Obstet Gynecol. 2020; 135 (2): e73-9.
11. Nicolaides KH. A model for a new pyramid of prenatal care based on the 11 to 13 weeks’ assessment. Prenat Diagn. 2011: 31: 3-6.
12. Vivanti AJ, Deruelle P, Picone O, Guillaume S, Roze JC, Mulin B,
et al. Follow-up for pregnant women during the COVID-19 pandemic: French national authority for health recommendations. J Gynecol Obstet Hum Reprod. 2020; 49: 101804.
13. Krenitsky NM, Spiegelman J, Sutton D, Syeda S, Moroz L. Primed for a pandemic: Implementation of telehealth outpatient monitoring for women with mild COVID-19. Semin Perinatol. 2020; 44 (7): 151285.
14. Ferrara A, Hedderson MM, Brown SD, Ehrlich SF, Tsai AL, Feng J,
et al. A telehealth lifestyle intervention to reduce excess gestational weight gain in pregnant women with overweight or obesity (GLOW): a randomised, parallel-group, controlled trial. Lancet Diabetes Endocrinol. 2020; 8 (6): 490-500.
15. Butler Tobah YS, LeBlanc A, Branda ME, Inselman JW, Morris MA, Ridgeway JL,
et al. Randomized comparison of a reduced-visit prenatal care model enhanced with remote monitoring. Am J Obstet Gynecol. 2019; 221 (6): 638.e1-638.e8.
16. Hawthorne G, Sansoni J, Hayes L, Marosszeky N, Sansoni E. Measuring patient satisfaction with health care treatment using the Short Assessment of Patient Satisfaction measure delivered superior and robust satisfaction estimates. J Clin Epidemiol. 2014; 67 (5): 527-37.
17. Peahl AF, Howell JD. The evolution of prenatal care delivery guidelines in the United States. Am J Obstet Gynecol. 2021; 224 (4): 339-47.
18. Ministerio de Salud (Peru). Decreto Supremo Nº 005-2021-SA que aprueba el Reglamento de la Ley Nº 30421, Ley Marco de Telesalud, y del Decreto Legislativo Nº 1490, Decreto Legislativo que fortalece los alcances de la Telesalud. Lima-Perú: El Peruano [
Internet]. 23/01/2021; 2021. [access in 2022 Dec 9]. Available from:
https://busquedas.elperuano.pe/normaslegales/decreto-supremo-que-aprueba-el-reglamento-de-la-ley-n-30421 -decreto-supremo-n-005-2021-sa-1922320-2/19. Instituto Nacional Materno Perinatal. Resolución Directoral N° 099-2020-DG-INMP/MINSA. Plan de emergencia COVID-19 Telesalud, Teleorientacion para la atención de pacientes de bajo riesgo y atención presencial restringida para pacientes con riesgo de complicación, del Instituto Nacional Materno Perinatal. Lima-Perú: Instituto Nacional Materno Perinatal; 2020. [access in 2022 Dec 9]. Available from:
https://www.gob.pe/institucion/inmp/normas-legales/ 1204368-099-2020-dg-inmp-minsa20. Peahl AF, Powell A, Berlin H, Smith RD, Krans E, Waljee J. Patient and provider perspectives of a new prenatal care model introduced in response to the coronavirus disease 2019 pandemic. Am J Obstet Gynecol. 2021; 224: 384.e1-e11.
21. Colombo T, Todeschini LB, Orlandini M, Nascimento HD, Gabriel FC, Alves RJV,
et al. Low-risk antenatal care enhanced by telemedicine: a practical guideline model. Rev Bras Ginecol Obstet. 2022; 44 (9): 845-53.
22. Pflugeisen BM, McCarren C, Poore S, Carlile M, Schroeder R. Virtual visits: managing prenatal care with modern technology. MCN Am J Matern Child Nurs. 2016; 41: 24-30.
23. Pflugeisen BM, Mou J. Patient Satisfaction with Virtual Obstetric Care. Matern Child Health J. 2017; 21 (7): 1544-51.
24. DeNicola N, Grossman D, Marko K, Sonalkar S, Butler Tobah YS, Ganju N,
et al. Telehealth Interventions to Improve Obstetric and Gynecologic Health Outcomes: A Systematic Review. Obstet Gynecol. 2020; 135 (2): 371-82.
25. Ekeland AG, Bowes A, Flottorp S. Effectiveness of telemedicine: a systematic review of reviews. Int J Med Inform. 2010; 79 (11): 736-71.
26. Almathami HKY, Win KT, Vlahu-Gjorgievska E. Barriers and Facilitators that Influence Telemedicine-Based, Real-Time, Online Consultation at Patients’ Homes: Systematic Literature Review. J Med Internet Res. 2020; 22 (2): e16407.
27. Balk EM, Konnyu KJ, Cao W, Bhuma MR, Danilack VA, Adam GP,
et al. Schedule of Visits and Televisits for Routine Antenatal Care: A Systematic Review. Rockville (MD): Agency for Healthcare Research and Quality (US); 2022. [access in 2022 Dec 9]. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK582024/28. Novoa RH, Meza-Santibañez L, Rodríguez-Hilario N, Torres-Osorio J, Jáuregui-Canchari V, Huang-Yang X,
et al. Development of a Mobile Health Application Based on a Mixed Prenatal Care in the Context of COVID-19 Pandemic. Rev Bras Ginecol Obstet. 2023; 45 (4): 179-85.
29. Chang JE, Lai AY, Gupta A, Nguyen AM, B erry CA, Shelley DR. Rapid Transition to Telehealth and the Digital Divide: Implications for Primary Care Access and Equity in a Post-COVID Era. Milbank Q. 2021; 99 (2): 340-68.
Authors’ contributionNovoa RH and Ventura W: conceived of the study, planned the methodology and contributed to manuscript writing. Huang-Yang X, Gayoso-Liviac A: conceived of the study, planned the methodology and contributed to data collection and application of surveys. Meza-Santibañez L: contributed to manuscript writing. Bazo-Alvarez JC: conceived of the study and planned the methodology. Torres-Osorio J and Rodríguez-Hilario N: contributed to data collection and application of surveys. All authors contributed to relevant critical review of the intellectual content, have approved the final version of the article and declare no conflict of interest.
Received on January 6, 2023
Final version presented on June 16, 2024
Approved on July 5, 2024
Associated Editor: Leila Katz


 ; Xin Huang-Yang 2
; Xin Huang-Yang 2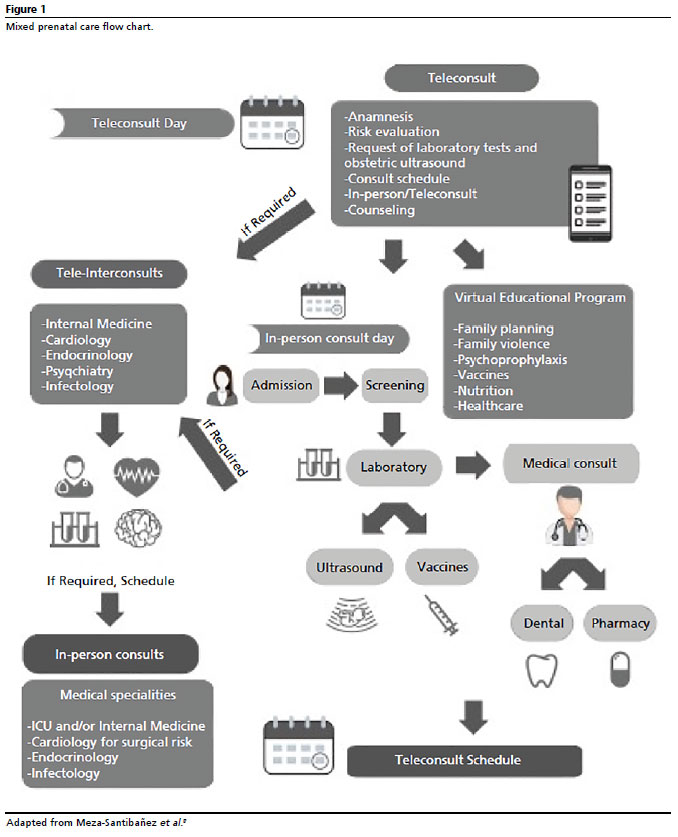






 Ler em português
Ler em português