ABSTRACT
OBJECTIVES: to estimate the correlation between birth weight, breastfeeding, and body mass index in six-year-old children in the city of Palhoça/SC, Brazil.
METHODS: a cross-sectional study involving 502 children. Data were collected through interviews with mothers at home and anthropometric assessments at schools. The child's current body mass index was the dependent variable. The independent variables were birth weight, breastfeeding duration, and exclusive breastfeeding duration. Correlations among variables were estimated using Pearson's correlation coefficient and respective coefficients of determination. Multiple linear regression analysis was performed to observe the independence among the variables.
RESULTS: birth weight and body mass index at six years of age showed a statistically significant positive correlation (r= 0.115; p=0.008). Breastfeeding duration was not correlated (r= -0.018; p=0.683). The duration of exclusive breastfeeding showed a statistically significant negative correlation (r= -0.103; p=0.018). However, multiple linear regression analysis showed an independent and significant positive correlation only between birth weight and body mass index at six years of age (r= 0.142; p= 0.003).
CONCLUSION: higher birth weight was significantly and independently positively correlated with increased body mass index at six years of age.
Keywords:
Birth weight, Breastfeeding, Pediatric obesity, Body mass index
RESUMO
OBJETIVOS: estimar a correlação entre peso ao nascer, amamentação e índice de massa corporalem crianças de seis anos de Palhoça/SC, Brasil.
MÉTODOS: estudo transversal envolvendo 502 crianças. Os dados foram coletados por entrevistas com mães nos domicílios e avaliação antropométrica nas escolas. O índice de massa corporalatual da criançafoi a variável dependente. As variáveis independentes foram peso ao nascer, tempo de amamentação, tempo de amamentação exclusiva. As correlações entre as variáveis foram estimadas pelo coeficiente de correlação de Pearson e respectivos coeficientes de determinação. Foi realizada análise de regressão linear multivariada para observação da independência entre as variáveis.
RESULTADOS: o peso ao nascer e o índice de massa corporal aos seis anos mostraram correlação positiva estatisticamente significativa (r= 0,115; p= 0,008). O tempo de amamentação não se mostrou correlacionado (r= -0,018; p= 0,683). Já o tempo de amamentação exclusiva mostrou correlação negativa estatisticamente significativa (r= -0,103; p= 0,018). Entretanto, a análise de regressão linear multivarida mostrou correlação positiva independente e significativa somente entre o peso ao nascer e o índice de massa corporal aos seis anos de idade (r= 0,142; p= 0,003).
CONCLUSÃO: o maior peso ao nascer correlacionou-se positivamente de forma significativa e independente com o aumento do índice de massa corporal aos seis anos de idade.
Palavras-chave:
Peso ao nascer, Amamentação, Obesidade pediátrica, Índice de massa corporal
IntroductionObesity is characterized as the abnormal or excessive accumulation of fat that can cause damage to the health.
1 Its etiology is multifactorial and its genesis may be related to the first thousand days of life, this phase being susceptible to predisposing factors for body composition and neuroendocrine regulation.
2The prevalence of obesity has increased in recent decades, almost tripling since 1975. According to the World Health Organization (WHO), one in five children is overweight
1 and Brazil is close to the global figure. According to the
Estudo Nacional de Alimentação e Nutrição Infantil de 2019 (ENANI-2019) (National Study of Food and Nutrition in Children) report, 10.1% of the Brazilian children under the age of five are overweight.
3 This is a concerning data, since childhood obesity contributes to the development of chronic non-communicable diseases such as type 2 diabetes mellitus, systemic arterial hypertension and early atherosclerosis.
4 Furthermore, excess weight in childhood leads to obesity in adulthood, due to long-term cardiovascular and metabolic changes.
4From another perspective, obesity is preventable
1 and the benefits of breastfeeding against the subsequent development of this disease have been studied.
5 Breast milk contains hormones in its formulation such as leptin and ghrelin, besides having a lower amount of proteins and electrolytes, which prevents kidney overload.
6 These hormones present in breast milk have the action of inhibiting appetite and anabolic pathways and stimulating catabolic pathways, thus playing a primary role in controlling the body weight.
7WHO guidelines recommend that children should be exclusively breastfed for the first six months and that breastfeeding should be supplemented for the first two years.
8 However, less than half (45.8%) of the Brazilian children under six months are exclusively breastfed.
3 Complementary feeding introduced early, before six months, can be directly related to future obesity, given that it is often done inappropriately, with food of low nutritional quality and associated with deprivation of the nutrients and hormones present in breast milk.
9It should also be noted that breastfeeding during the first four to six months of age reduces the risk of all hospitalization causes.
5 According to Victora et al.
10 expanding breastfeeding to a universal level could prevent 823,000 deaths a year in children under five years old.
On the other hand, birth weight has been associated with being overweight at childhood. A study involving an American cohort showed that birth weight was a predictor of obesity at school age.
11 In addition, an observational study of 500 schoolchildren in Ceará State showed a positive correlation between birth weight and overweight/obesity in children, with 52.9% of those born with a high birth weight being overweight at school age.
12 Thus, birth weight is an indicator associated with the risk of developing obesity at childhood.
This study aims to contribute to the national literature on the constant need to update epidemiological data on childhood obesity and associated factors. The aim of this study was to estimate the correlation between birth weight, breastfeeding and body mass index at six years of age.
MethodsThis is a cross-sectional epidemiological study using data from children included in a longitudinal study called the
Coorte Brasil Sul13 (Brazil South cohort) which follows schoolchildren in Palhoça/SC. The study population consisted of six-year-old children living in the city of about 230,000 inhabitants located in the Greater Florianópolis region and enrolled in 55 schools. This cohort was composed of children who were in the first year of elementary school at the time of the baseline study, which is why this study refers to children at this age. Children with severe physical limitations that would make it difficult to measure anthropometric data were excluded.
The following parameters were used to calculate the sample: population of 1,756 schoolchildren,
13 unknown anticipated prevalence of obesity (P = 50%, used to generate the largest sample size given the maintenance of the other parameters), 95% confidence level and relative error of 4%, which generated a minimum sample of 448 children. Thus, all the children included in the
Coorte Brasil Sul database with the information required for this study were included (n= 502).
Data collection was carried out in 2015/2016 by a field team of researchers and community health workers trained to conduct interviews with the children's mothers or main caregivers in their homes. The retrospective phase of the cohort study provided data on pregnancy and the first two years of the child's life using an instrument designed for this purpose.
13 Follow-up of the children up to the age of six was characterized by new data collection, including anthropometry of the children at this stage.
Weight and height were collected following the recommendations of the Ministry of Health.
14 To collect the weight, each child was barefoot, wearing light clothing and without objects. With the scale zeroed beforehand, the child was positioned in the middle of the equipment, standing upright with their feet together and arms stretched out along their body and then the weight on the display was read.
To measure the height, the child stood upright, with no accessories on their head, arms stretched out, head up, legs parallel, calves, buttocks, shoulder blades and the back of the head touching the stadiometer. The mobile part of the equipment was lowered, adjusting it against the head. The individual was removed and the reading was taken, without releasing the mobile part of the equipment.
14 Anthropometric assessment was carried out using the body mass index (BMI), obtained by dividing the weight by height to a squared.
14The independent variables were birth weight in grams, breastfeeding time in months and exclusive breastfeeding time. Gender (male/female) and the child's skin color (white/black/mixed/yellow) were collected.
The database was prepared in a numerical spreadsheet and exported to SPSS Statistics for Windows software, version 18.0 (SPSS Inc., Chicago, Ill., USA). The variables were described in terms of proportions, measures of central tendency and dispersion. Correlations between the variables studied were estimated using Pearson's correlation coefficient and the respective coefficients of determination, after the distributions had been tested using the Kolmogorov-Smirnov test. Subsequently, a multivariate linear regression analysis was carried out using the stepwise strategy to observe the independence between the variables studied. The assumptions of the linear regression analysis were met, with regard to the adequacy of the sample size, the linear relation between the dependent variable and the independent variables, the absence of multicollinearity between the independent variables (exclusive breastfeeding time X birth weight r= 0.030; exclusive breastfeeding time X breastfeeding time r= 0.256 and breastfeeding time X birth weight r= 0.106), the absence of outliers, normally distributed and independent residuals (Durbin-Watson test = 1.15) and the presence of homoscedasticity. Values of p<0.05 were considered significant.
This study was approved by the Human Research Ethics Committee of the
Universidade do Sul de Santa Catarina under the protocol number 38240114.0.0000.5369.
ResultsThe study included 502 six year old schoolchildren. Of the total, 51.6% were male and 84.3% were white. Regarding to breastfeeding, 91.6% of the children were breastfed at least once, and 53.7% were exclusively breastfed for six months (Table 1). The children's average birth weight was 3,242.3g (SD= 731.1g) and the average BMI at six years of age was 16.9 kg/m
2 (SD= 2.8) (Table 2).
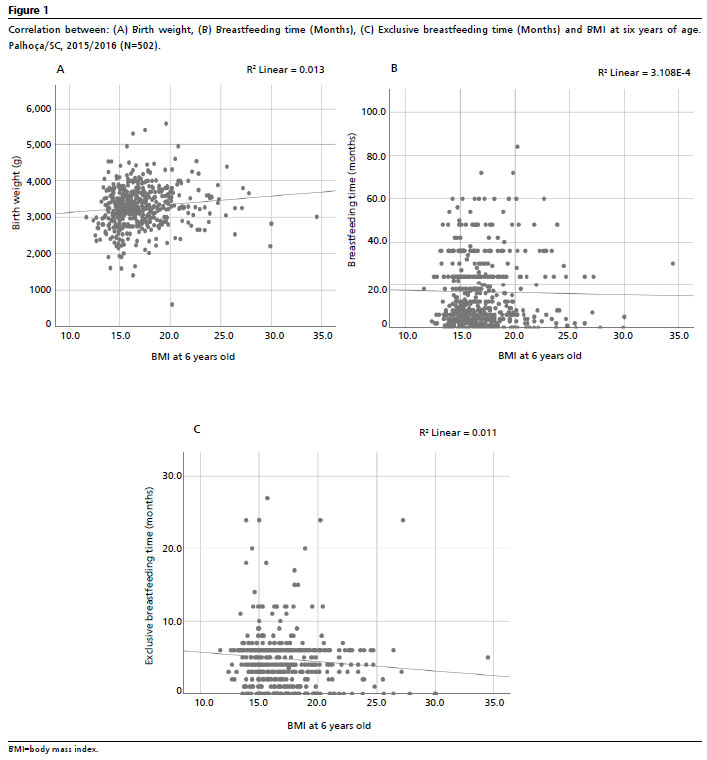
Birth weight (g) and BMI at six years of age showed a significant positive correlation (r= 0.115;
p=0.008), with a coefficient of determination of R
2=0.013 (Figure 1A). Breastfeeding time and BMI at six years of age showed no correlation (r= -0.018;
p=0.683) (Figure 1B). On the other hand, exclusive breastfeeding time and BMI at six years of age showed a significant negative correlation (r= -0.103;
p=0.018), with a coefficient of determination of R
2=0.011 (Figure 1C).
Multiple linear regression analysis resulted in a statistically significant model [F (3.452) = 3.540;
p=0.015; R
2=0.018]. Birth weight proved to be a statistically significant and independent predictor of BMI at six years of age (r= 0.142;
p=0.003) while breastfeeding time (r= 0.035;
p=0.466) and exclusive breastfeeding time (r= -0.040;
p=0.406) did not prove to be independent predictors, losing the statistical significance presented in the bivariate correlation analysis (Table 3).
DiscussionThe results of this study showed that higher birth weight correlated significantly and independently with higher BMI at six years of age, although the coefficient of determination of the adjusted model was low.
The significant positive correlation between birth weight and BMI has been pointed out in the literature. A cohort study of Uruguayan children identified a 70% increase in the prevalence of obesity among macrosomic newborns (birth weight equal to or greater than 4,000g) compared to non-macrosomic newborns.
15 Another multinational cross-sectional study in 12 countries showed a positive association between higher levels of birth weight (defined as >3,500g) and the likelihood of obesity in children aged nine to eleven.
16 In addition, the United States cohort study of 10,186 children concluded a significant association between birth weight and the risk of overweight or obesity at childhood, reinforcing the importance of birth weight as a risk factor for childhood obesity and the need for early interventions to prevent this public health problem.
11 This scenario reinforces the fact that high birth weight is a significant risk factor for obesity, making it possible to observe the relevance of care to the first thousand days of life in the genesis of obesity.
Given that in early obesogenic environments there is a greater association of genes related to obesity, gestational overnutrition, gestational diabetes mellitus (GDM) and maternal smoking are also factors that can explain the relation between birth weight and children's BMI.
17 A meta-analysis including information on more than 24,000 newborns described that those born to mothers with GDM had a higher proportion of body fat and around 62 g more fat mass compared to newborns born to mothers without GDM.
18The results of this study showed no significant and independent correlation between breastfeeding time and exclusive breastfeeding time and BMI at six years of age. However, a meta-analysis revealed a dose-response effect, with a negative correlation between the duration of breastfeeding and the risk of obesity, in which each month of breastfeeding was associated with a 4.0% reduction in the risk of obesity. The same meta-analysis also showed a 17.0% lower risk of obesity in breastfed children compared to those who were never breastfed.
19In an integrative review, the authors found a positive correlation between breastfeeding and a reduction in excess weight only when exclusive breastfeeding was involved. The authors also showed that supplemented breastfeeding was not protective in terms of weight gain. They argued that the data from the studies evaluated were from children over six months old who were already using complementary feeding, which influenced in the results.
20A review published in 2016 highlights the crucial role of breastfeeding in preventing childhood obesity. In assessing the available evidence, the authors emphasize that exclusive and prolonged breastfeeding is associated with a lower risk of obesity in childhood. This association suggests that breastfeeding not only provides essential nutrients, but may also influence behavioral and metabolic factors that contribute to weight regulation throughout life.
21Thus, the hypothesis arises that the difference between the results presented here and the evidence related to the benefits of breastfeeding may be the result of different methodological approaches, such as differences in the age groups studied, socioeconomic differences between the groups, gestational weight gain, gestational BMI and the presence or absence of GDM.
It is also important to highlight the association between eating habits and lifestyle and childhood obesity. According to WHO, increased consumption of food rich in fat and sugar, an increase in sedentary lifestyles, growing urbanization and socioeconomic conditions are among the main factors influencing obesity.
22 Furthermore, the reduction of outdoor activities correlated with the advance of technological means of entertainment can contribute to children remaining in more sedentary occupations
23 and can interfere with the increase in BMI. Thus, the importance is to develop an early behavioral and healthy eating routine.
The results of this study should be interpreted with caution. One important limitation refers to the few independent variables included, even for adjusting the model presented, in view of the intrinsic multifactoriality in determining childhood obesity. Another limitation refers to the retrospective data collection, such as the “breastfeeding time” variable, which may have generated memory bias with a possible impact in the results. Furthermore, although significant, the result showed a very low coefficient of determination. On the other hand, it is believed that this study has the potential to stimulate the development of more populational surveys to complement the data in health information systems. National population-based epidemiological data is extremely important for major public policies, but local data such as that presented here has enormous potential for planning adequate health care for people in cities, where the
Sistema Único de Saúde (SUS) (Public Health System) is effective.
It can be concluded that in the population studied, higher birth weight was significantly and independently correlated with higher BMI at six years of age. There is a need for more studies on the subject, including other variables related to pregnant women, such as age, income, schooling, nutritional status, comorbidities, smoking, alcohol or illicit drug use. We also encourage studies to be carried out in different Brazilian regions, since it is essential to obtain epidemiological data from the country, which has marked climatic, socio-cultural and economic differences.
References1. World Health Organization (WHO). Commission on Ending Childhood Obesity. World Health Organization [serial on the Internet]. 2021 [access in 2022 Jan 22]. Available from:
https://www.who.int/publications/i/item/97892415100662. Sociedade de Pediatria de São Paulo. Enfrentando a Obesidade Infantil - Setembro Laranja. Bol Soc Pediatr São Paulo. 2019; 4 (2): 5-14. [access in 2022 Jan 22]. Available from:
https://www.spsp.org.br/site/asp/boletins/AtualizeA4N2.pdf3. Universidade Federal do Rio de Janeiro (UFRJ). Estado Nutricional Antropométrico da Criança e da Mãe: Prevalência de indicadores antropométrico de crianças brasileiras menores de 5 anos de idade e suas mães biológicas: ENANI-2019. [access in 2024 Jan 30]. Available from:
https://enani.nutricao.ufrj.br/index.php/relatorios4. Corica D, Aversa T, Ruggeri RM, Cristani M, Alibrandi A, Pepe G,
et al. Could AGE/RAGE-related oxidative homeostasis dysregulation enhance susceptibility to pathogenesis of cardio-metabolic complications in childhood obesity? Front Endocrinol. 2019; 10 (426): 1-8.
5. Kim JH, Lee SW, Lee JE, Ha EK, Han MY, Lee E. Breastmilk feeding during the first 4 to 6 months of age and childhood disease burden until 10 years of age. Nutrients. 2021; 13 (8): 2825-40.
6. Kouwenhoven SMP, Muts J, Finken MJJ, Goudoever JBV. Low-protein infant formula and obesity risk. Nutrients. 2022; 14 (13): 2728-39.
7. Palou M, Picó C, Palou A. Leptin as a breast milk component for the prevention of obesity. Nutr Rev. 2018; 76 (12): 875-92.
8. World Health Organization (WHO). Breastfeeding [
Internet]. 2021 [acesso em 2023 Jan 24]. Disponível em:
http://www.who.int/topics/breastfeeding/en/9. Ortega-García JA, Kloosterman N, Alvarez L, Tobarra-Sánchez E, Cárceles-Álvarez A, Pastor-Valero R,
et al. Full breastfeeding and obesity in children: A prospective study from birth to 6 years. Child Obes. 2018; 14 (5): 327-37.
10. Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J,
et al. Breastfeeding in the 21
st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016; 387 (10017): 475-90.
11. Kapral N, Miller SE, Scharf RJ, Gurka MJ, DeBoer MD. Associations between birthweight and overweight and obesity in school-age children. Pediatr Obes. 2018; 13 (6): 333-41.
12. Lopes EMS, Queiroz EF, Cavalcante NNAM, Silva VC. Associação do peso ao nascer no desenvolvimento de sobrepeso/obesidade em escolares com idade entre 5-9 anos em Fortaleza, Ceará, Brasil. Resid Pediatr. 2021; 11 (2): 1-8.
13. Traebert J, Lunardelli SE, Martins LG, Santos KD, Nunes RD, Lunardelli AN,
et al. Methodological description and preliminary results of a cohort study on the influence of the first 1,000 days of life on the children's future health. Acad Bras Cienc. 2018; 90: 3105-14.
14. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Coordenação Geral da Política de Alimentação e Nutrição. Incorporação das curvas de crescimento da Organização Mundial da Saúde de 2006 e 2007 no SISVAN [access in 2015 Mai 10]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/orientacoes_coleta_analise_dados_antropometricos.pdf15. Pereyra I, Gomez A, Jaramillo K, Ferreira A. Birth weight, weight gain, and obesity among children in Uruguay: a prospective study since birth. Rev Paul Pediatr. 2021; 39: e2019088.
16. Qiao Y, Ma J, Wang Y, Li W, Katzmarzyk PT, Chaput JP,
et al. Birth weight and childhood obesity: a 12-country study. Int J Obes Suppl. 2015; 5 (Suppl. 2 ): S74-9.
17. Larqué E, Labayen I, Flodmark CE, Lissau I, Czernin S, Moreno LA,
et al. From conception to infancy - early risk factors for childhood obesity. Nat Rev Endocrinol. 2019; 15: 456-78.
18. Logan KM, Gale C, Hyde MJ, Santhakumaran S, Modi N. Diabetes in pregnancy and infant adiposity: systematic review and meta-analysis. Arch Dis Child Fetal Neonatal. 2017; 102 (1): 65-72.
19. Caldeira KMS, Souza JMP, Souza SB. Excesso de peso e sua relação com a duração do aleitamento materno em pré-escolares. Rev Bras Crescimento Desenvolv Hum. 2015; 25 (1): 89-96.
20. Baldissera AI, Bortoli CF. Aleitamento materno na prevenção da obesidade infantil: uma revisão integrativa. Santé. 2023; 1 (2): 104-18.
21. Santos LP, Assunção MCF, Matijasevich A, Santos IS, Barros AJD. Dietary intake patterns of children aged 6 years and their association with socioeconomic and demographic characteristics, early feeding practices and body mass index. BMC Public Health. 2016; 16 (1): 1055-66.
22. World Health Organization (WHO). Obesity and overweight. 2024 [
Internet] [access in 2024 Abr 27]. Available from:
https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight23. Hayes JF, Fitzsimmons-Craft EE, Karam AM, Jakubiak J, Brown ML, Wilfley DE. Disordered eating attitudes and behaviors in youth with overweight and obesity: implications for treatment. Curr Obes Rep. 2018; 7 (3): 235-46.
Acknowledgements: We would like to thank the
Fundação de Amparo à Pesquisa e Inovação do Estado de Santa Catarina (FAPESC) (Santa Catarina Research and Innovation Foundation) and the
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (National Council for Scientific and Technological Development) for the financial support.
Authors' contribution: Dorigatti A, Padilha I and Flôres APR: data collection and analysis, writing of the manuscript. Traebert J and Traebert E: conception of the study, methodological design, data collection and analysis, writing of the manuscript. All the authors have approved the final version of the article and declare no conflicts of interest.
Received on April 1, 2024
Final version presented on June 5, 2024
Approved on June 10, 2024
Associated Editor: Lygia Vanderlei


 ; Isabelle Padilha2
; Isabelle Padilha2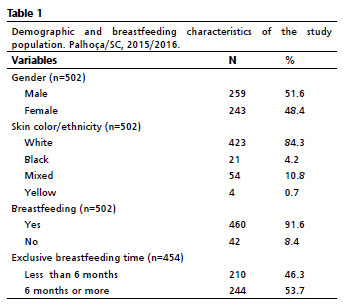








 Ler em português
Ler em português