ABSTRACT
OBJECTIVES: to investigate the association of nutritional status with urinary iodine deficiency in pregnant women attending the Basic Health Units in the city of São Luís - Maranhão.
METHODS: cross-sectional study carried out with 261 pregnant women. Urine samples were collected for analysis of determination of urinary iodine. Iodine deficiency was considered as <150 µg/L and adequate as ≥150 µg/L. Weight and height measurements were taken at the time of collection and investigation of pre-pregnancy weight calculate BMI). Continuous variables were presented as mean, standard deviation, median, 25th and 75th percentiles, and categorical variables as simple and relative frequencies and percentages. Multivariate analyses investigate the association between pre-pregnancy and current BMI and UIC (urinary iodine concentration).
RESULTS: the mean pre-pregnancy BMI was 24.3 ± 4.5 kg/m2, and the current BMI was 27.2 ± 6.5 kg/m2. The median UIC was 181.3 µg/L (113.2-271.7), and 40.6% of the sample showed iodine deficiency. The increase in pre-pregnancy and current BMI was associated with a reduction in the prevalence of iodine deficiency in pregnant women (PR = 0.94; (CI95% = 0.88; 0.99) and PR = 0.95; (CI95% = 0.88 – 0.99), respectively).
CONCLUSION: high BMI is positively associated with UIC and provides a reduction in iodine deficiency prevalence in pregnant women.
Keywords:
Iodine deficiency, Nutritional status, Pregnant women, Overweight, Ultra processed foods
RESUMO
OBJETIVOS: investigar a associação do estado nutricional com deficiência de iodo urinário em gestantes atendidas em Unidades Básicas de Saúde do município de São Luís – MA.
MÉTODOS: estudo transversal, realizado com 261 gestantes. Foram coletadas amostras de urina para análise de determinação do iodo urinário, considerou-se deficiência o valor <150 µg/L e adequado, valor ≥150 µg/L. Foram aferidas as medidas de peso e altura no momento da coleta e investigação do peso pré-gestacional para cálculo do IMC. As variáveis contínuas foram expressas em média, desvio padrão, mediana, percentil 25 e 75 e as categóricas em frequência simples e relativa e em percentual. Análises multivariadas investigaram associação entre IMC pré-gestacional e atual e UIC (Concentração urinária de iodo).
RESULTADOS: a média do IMC pré-gestacional foi 24,3 ± 4,5 kg/m2 e do IMC atual 27,2 ± 6,5 kg/m2. A mediana de concentração de iodo urinário foi de 181,3 µ/L (113,2-271,7) e 40,6% da amostra possuía deficiência de iodo. O aumento no IMC pré-gestacional e atual foi associado à redução da prevalência de deficiência de iodo em gestantes (RP = 0,94; (IC95% = 0,88; 0,99) e RP = 0,95; (IC95% = 0,88 – 0,99), respectivamente).
CONCLUSÃO: o IMC elevado está positivamente associado à UIC e proporciona redução na prevalência de deficiência de iodo em gestantes.
Palavras-chave:
Deficiência de iodo, Estado nutricional, Gestantes, Sobrepeso, Alimentos ultraprocessados
IntroductionMaternal nutritional status can induce changes that affect the health of the mother-child binomial beyond the gestational period.
1 The current prevalence of overweight and obesity during pregnancy is high,
2 and in developed countries, overweight is already a fact for women of childbearing age even before becoming pregnant.
1 It is assumed that obesity increases the risk of pregnant women developing iodine insufficiency.
3Iodine is an essential micronutrient for humans.
4 Iodine deficiency during pregnancy can lead to disorders such as spontaneous abortion, premature birth, and stillbirth.
5 The effect of weight gain on the amount of iodine may be associated with modifying the sodium-iodine symporter (NIS) caused by increased inflammatory markers in obesity.
6,7 A study carried out with adults found the association between the increased presence of the interleukin 1 (IL-1) and low iodine levels in overweight and obese individuals.
7A survey conducted in the United Kingdom found iodine insufficiency prevalence of 70% among obese women in the 2
nd trimester of pregnancy. However, this sample was composed only of pregnant women with BMI ≥30 kg/m
2, hence without a control group.
8 In Brazil, the maternal nutritional profile
9 and the nutritional status of iodine during pregnancy
10 have been evaluated separately. Consequently, there is a lack of studies that examine the association of maternal nutritional status with iodine deficiency in the gestational period.
In this sense, the growing prevalence of overweight women in the gestational period
2 indicates the importance of further studies concerning the effects of changes in nutritional status on maternal health. In addition, investigating the association of gestational nutritional status with iodine deficiency is important because it is an essential nutrient for a good perinatal outcome. Furthermore, consequences of iodine deficiency on the mother-child binomial have been reported, including preeclampsia
11 and neurological deficiencies in the child.
12 Our hypothesis is that the pregnant nutritional status influences the level of urinary iodine. Therefore, this study aimed to investigate the association of nutritional status with urinary iodine deficiency in Brazilian pregnant women.
MethodsA cross-sectional study was carried out in the city of São Luís – MA, Brazil, from February 2019 to February 2020. São Luís is located in the Northeast of Brazil and had about 1,109,000 inhabitants in 2020.
The sample size was determined from a minimum proportion of 8%, with a relative error of 4% (range 4 to 12%) and a 95% confidence level, which led to a simple random sample of 177 pregnant women. As the sample was selected by a primary health care unit, a design effect of 1.5 was included, which increased the sample size to 266 pregnant women. For this study, data from 261 pregnant women aged ≥18 years, residing in urban and rural areas of São Luís and who were users of the public health network at Basic Health Units (UBS) during the research. Pregnant women with a history of thyroid disease and/or surgery and a reported diagnosis of hypothyroidism or hyperthyroidism were not included.
Twelve UBS were selected in the city, and a list of pregnant women attending each one was obtained. The pregnant women were randomly selected from this list to participate in the research.
Data were collected by trained research assistants. The interviews took place at the UBS or at the pregnant women's residences when they were located at home. Information on pregnant women's socioeconomic, demographic, and health profile was collected with a semi-structured questionnaire. Data included maternal age (years), skin color (self-reported), maternal education (complete elementary school/incomplete elementary school; incomplete high school; complete high school or higher education), marital status (with a partner and without a partner), family income (categorized into tertiles), residence location (rural or urban), number of residents in the household, use of nutritional supplement (yes or no), use of a nutritional supplement containing iodine (yes or no), consumption of ultra-processed foods (percentage of consumption in relation to the energy value of the diet evaluated in tertiles), and gestational age (in weeks). Electronic questionnaires were answered using the RedCap
® software on a tablet.
Food consumption was assessed by 24-hour recalls (24hR), utilizing the multiple pass technique of the 24-hour dietary recall method. The multiple-pass 24-h recall
13 was applied to assess food consumption of pregnant women the day before the interview. All 24hR were entered to the GloboDiet software, Brazilian version, using DataEntry mode. All foods consumed were classified according to the NOVA system. This study only used the tertile of the percentage of consumption of ultra-processed foods, which are foods produced industrially, using substances totally or partially removed from other foods, derived from food constituents, or formulated in laboratory.
14For iodine analysis, 20 ml of urine were collected from pregnant women in a sterile container, tightly closed, labeled, and stored at -20ºC.
Iodine in urine was determined in an Elan DRC II inductively coupled plasma mass spectrometer (ICP-MS) (Perkin-Elmer, Norwalk, CT), operating with high purity argon (99.999%, White Martins, Brazil). Quality control analysis used the certified reference material of urine from the National Institute of Standards and Technology (NIST), SRM 2670a - Toxic Elements in Freeze-Dried Urine.
The nutritional status of iodine in pregnant women was classified considering the median value < 150 µg/L as iodine deficiency.
15 Urinary iodine concentration (UIC) was also used as a continuous variable in the statistical analyses.
To assess the nutritional status of pregnant women, weight and height were measured according to the World Health Organization (WHO) standardized protocols and used to calculate the Body Mass Index [BMI = weight (kg)/height
2 (m)], as well as surveying pre-gestational weight. The pre-gestational weight (PGW) was obtained from the Pregnant Woman's Booklet or self-reported. The current weight (CW) was measured on an anthropometric digital platform scale, 0.1 kg precision, and 180 kg capacity. Height was measured on an AlturaExata
® mobile stadiometer, 0.5 cm precision.
Pre-gestational nutritional status cutoff points were recommended by the Institute of Medicine
16 and adopted by the Brazilian Ministry of Health, as follows: underweight (<18.5 kg/m
2), normal weight (18.5 to 24.9 kg/m
2), overweight (25.0 to 29.9 kg/m
2) and obesity (≥ 30 kg/m
2). Current nutritional status was assessed using the classification by Atalah et al.,
17 considering BMI according to gestational week, categorized as underweight, adequate, overweight, and obesity. Current and pre-pregnancy BMI were used as continuous variables in the regression models.
Directed Acyclic Graphs (DAG) were used for identifying the confounding factors included in the adjusted analyses. DAG is an approach to configure a theoretical model aiming to demonstrate the relationships between the explanatory and independent variables. This model identifies which variables require statistical adjustment. Thus, besides DAG avoiding unnecessary adjustments, it minimizes confounding and selection bias.
18The DAG was built in the Dagitty
® browser. A theoretical model was developed describing the relationships between the exposure variables (pre-pregnancy BMI – Figure 1A – and current BMI – Figure 1B) and the outcome variable (iodine deficiency or urinary iodine concentration during pregnancy) along with other covariates.
The theoretical model indicated that the minimum set of variables for adjusting the effect of pre-pregnancy BMI on iodine deficiency or urinary iodine concentration includes maternal age, maternal education, family income, residence location, and marital status. Considering current BMI as exposure, the suggested minimum adjustment was as follows: maternal age, maternal schooling, family income, residence location, marital status, current consumption of ultra-processed foods, and gestational age.
All statistical analyses were performed using Stata
® 14. Continuous variables were summarized as mean and standard deviation or median and interquartile range, depending on the distribution. The categorical variables were presented as simple and relative frequencies. As the prevalence of iodine deficiency in the sample was greater than 10%, the Poisson regression with robust variance adjustment was used to calculate the Prevalence Ratio (PR) in bivariate and multivariate models when the outcome was categorical. To assess the association between pre-pregnancy BMI or current BMI and urinary iodine concentration during pregnancy, linear regression analysis was used in multivariate models. A significance level of 5% was used in all analyses.
This study was approved by the Research and Ethics Committee of the University Hospital of the Federal University of Maranhão (HU-UFMA), opinion No. 2.982.185, from October 25, 2018, CAEE 80172617.0.2005.5086.
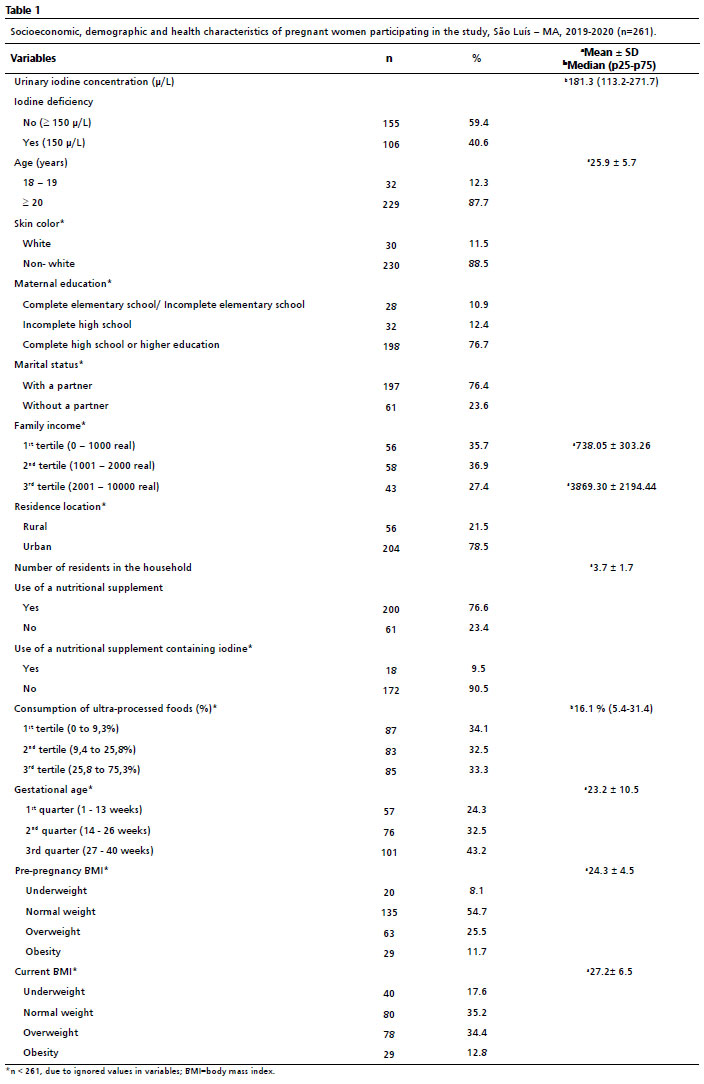
ResultsThe study included 261 pregnant women with a mean age of 25.9 ± 5.7 years: being 18 the minimum age and 42 the maximum age. The median urinary iodine concentration among the investigated pregnant women was 181.3 µg/L (113.2 - 271.7), and 40.6% of the sample showed iodine deficiency. The socioeconomic and demographic characteristics showed that 88.5% were non-white, 76.7% of respondents completed high school, and 76.4% lived with a partner. The average family income in the 1
st and 3
rd tertiles was 738.05 ± 303.26 BRL and 3869.30 ± 2194.44 BRL, respectively. Most pregnant women lived in the urban area (78.5%), and the average number of people living in the household was 3.7 ± 1.7 people.
Among the participants, 76.6% used some supplementation during pregnancy, and of these, only 9.5% consumed supplements that contained iodine. The median of ultra-processed foods consumption was 16.1% (5.4 – 31.4).
The third gestational trimester had the highest number of pregnant women, 43.2% of the total. The mean gestational age was 23.2 ± 10.5 weeks. The mean pre-pregnancy BMI was 24.3 ± 4.5 kg/m
2, while the current BMI presented an average of 27.2 ± 6.5 kg/m
2 (Table 1).
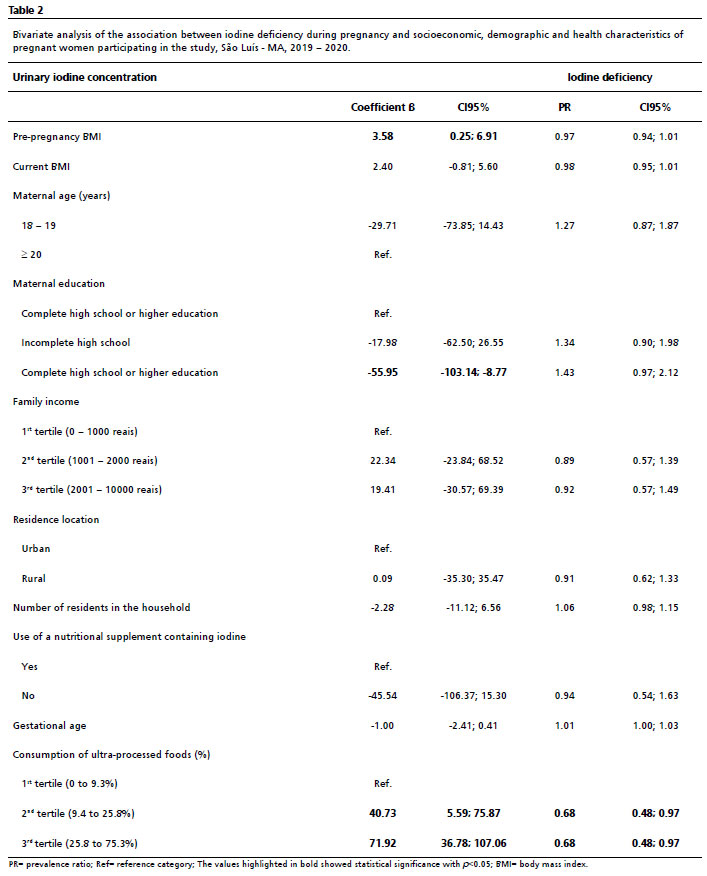
In the bivariate analysis, pregnant women with complete elementary school or incomplete elementary school had lower urinary iodine levels (β = -55.95; CI95%= -103.14; -8.77). Pre-pregnancy BMI (β = 3.58; CI95%=0.25; 6.91) and the second and third tertiles of the percentage of ultra-processed foods consumption (β=40.73; CI95%=5.59; 75.87 and β=71.92; CI95%=36.78; 107.06, respectively) were associated with the increase in iodine levels. Ranking within the highest percentage of consumption of ultra-processed foods and classified in the second and third tertiles (PR=0.68; CI95% = 0.48; 0.97 and PR=0.68; CI95% = 0.48; 0.97, respectively) was associated with the lowest prevalence of iodine deficiency (Table 2).
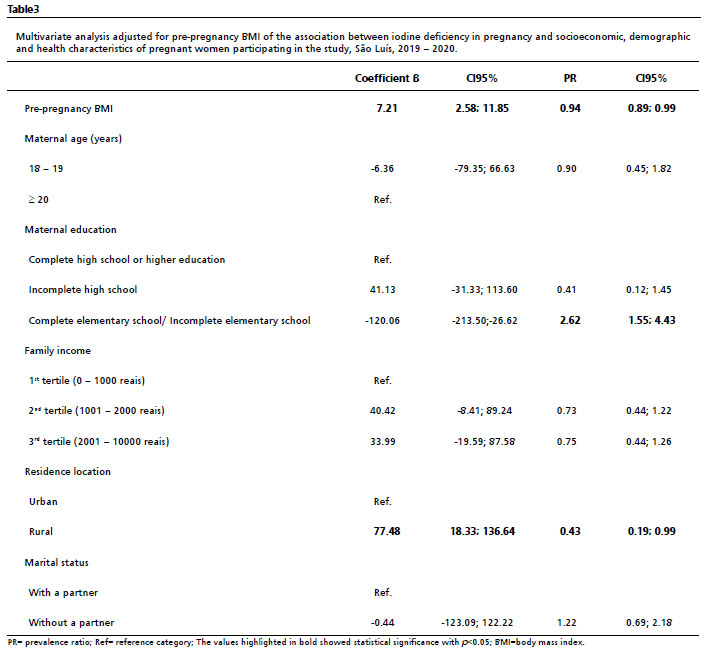
The multivariate analysis showed that a 1 kg/m
2 increase in pre-pregnancy BMI resulted in a 7.21 µg (CI95% = 2.58; 11.85) increase in urinary iodine levels. Higher pre-pregnancy BMI was associated with a reduction in iodine deficiency (PR=0.94; CI95% = 0.89; 0.99) (Table 3).
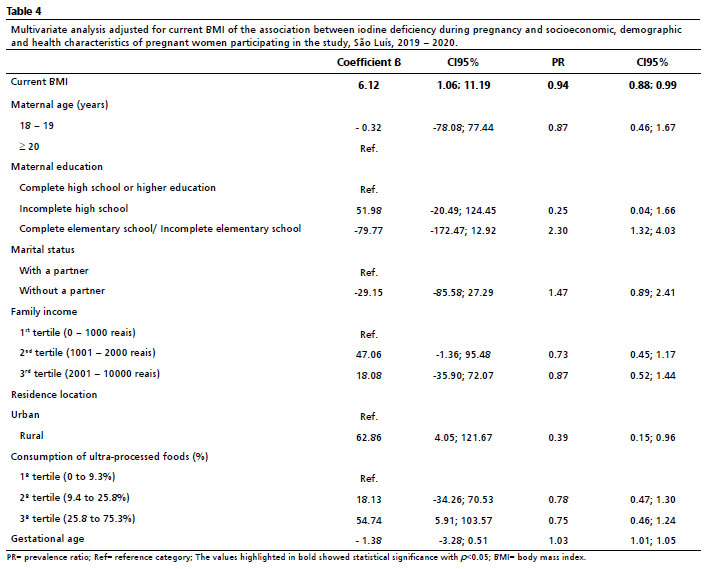
For each kg/m
2 increase in the current BMI of pregnant women, there was an increase in urinary iodine levels of 6.12 µg (CI95% = 1.06; 11.19), which was significant for a linear association. The increase in current BMI was associated with reducing the prevalence of iodine deficiency in pregnant women (PR = 0.94; CI95% = 0.88; 0.99) (Table 4).
We performed a sensitivity analysis without pregnant women who consumed iodine supplements. The association between pre-pregnancy or current BMI and urinary iodine levels remains (β=8.48; CI95%= 2.42; 14.53 and β=7.79; CI95%=1.17; 14.42). On the other hand, no difference was found in the analysis of the association between pre-pregnancy or current BMI and iodine deficiency categorized (PR=0.97; CI95% = 0.91; 1.02 and PR=0.96; CI95% = 0.90; 1.02).
DiscussionThis study investigated the relationship between pre-pregnancy and current BMI in pregnant women and levels and deficiency of iodine. It found that pregnant women with higher pre-pregnancy and current BMI are more likely to present higher urinary iodine levels. A positive association between consumption of ultra-processed foods and higher iodine content was also found in the sample. In addition, the prevalence of iodine-deficient pregnant women was high (40.6%).
The association between nutritional status and iodine deficiency has been reported by several studies.
6,7,19 However, studies on pregnant women are scarce,
3,8 and none have been found in Brazil so far. However, studies with other groups have addressed this association. A survey carried out in Spain showed that urinary iodine concentration is lower in obese (non-pregnant) women than in eutrophic women.
6 On the other hand, in line with our findings, a study with Brazilian children aged 6 to 14 years indicated that the higher the BMI, the higher the iodine level in the urine.
19 This result is attributed to the effect of the Brazilian salt fortification policy.
In Brazil, the policy of iodized salt for human consumption, in force since 1953 in endemic goiter areas, became nationally mandatory in the 1970s. It has favored iodine intake within adequate dietary Standards.
20 The present study found that pregnant women with higher BMI had higher iodine concentrations. This relationship is believed to be associated with higher iodine intake by means of ultra-processed foods, given that in this study, higher consumption of ultra-processed foods was associated with a lower prevalence of iodine deficiency. Thus, the effect of high consumption of ultra-processed foods seems to favor the reduction of iodine deficiency because these foods are high-salt sources, and consequently, of iodine.
14Thus, despite the advantage of ensuring adequate iodine nutrition, the consumption of ultra-processed foods must not be encouraged, as the harm outweighs the possible benefit. In this respect, preventing and treating the deficiency with natural sources of iodine is the most recommended conduct. The inclusion of varied and natural sources of this mineral in habitual consumption favors adherence to a healthy and adequate diet,
4 contributing to the good development of pregnancy and reducing the chances of nutritional deviations in the mother-child binomial.
11,12The lack of information discourages adherence to proper dietary recommendations for nutrient supplementation such as iodine during pregnancy. The present study showed that mothers with less education are more likely to be iodine deficient. An investigation carried out in a rural area of Hungary found that pregnant women who had studied less than or equal to eight years were at greater risk of having iodine deficiency during the gestational period than mothers with higher education.
21 Therefore, a higher level of education seems to contribute to adequate iodine nutrition during the gestational period.
Although Brazilian estimates point to broad coverage of the salt fortification program,
22 knowledge about the mother and child group needs to be further examined. In 2013, there was a decrease in the iodine content in salt because data from studies carried out with schoolchildren
23 showed that urinary samples had excess iodine. However, one must consider that the results for schoolchildren reflect the consumption of a specific population whose eating habits are often of high salt foods,
24 which consequently provides an ample supply of iodine. However, this may not be the case for pregnant women, as the high rate of iodine deficiency found in the present study demonstrates.
In recent years, studies with pregnant women have drawn attention to a significant iodine deficiency in this group.
25,26 Ferreira
et al.25 found a prevalence of 57% of iodine deficiency among pregnant women in Ribeirão Preto, SP. In the municipality of Diamantina, MG, studies found even higher rates, 73.8% of iodine deficiency among pregnant women
26. In agreement with our findings, Ning Yao
et al.27 identified 40.97% of iodine deficiency among pregnant women in southeastern China, even though the country had adopted salt fortification as a public policy since 1995.
28 Despite the widespread public policy supplementation programs in many countries, e.g., Brazil and China, the iodine deficiency in the mother and child group is worrisome.
The high prevalence of deficiency during pregnancy may be related to the increased need for iodine. Until the second half of pregnancy, the fetal supply of this trace element relies exclusively on maternal reserves because the fetal thyroid gland cannot produce thyroid hormones, which regulate essential functions for its good development.
11 Thus, the recommendation for daily intake of the mineral during pregnancy is about 30% higher than that of the general population.
15 In deficient iodine levels, the consequences for the mother-child binomial may range from unfavorable perinatal impacts such as reduced fetal growth and prematurity
11 to delays in child neurodevelopment and poor school performance.
12 For this reason, the fight against iodine deficiency in the maternal and child group must be on the agenda of public health and nutrition policies, given the high prevalence of iodine deficiency and its potential deleterious consequences.
As a limitation of this study, we should mention the application of a single 24-hour recall, as there might be memory bias in respondents over the usual food consumption of the population. However, the multiple steps method
13 was used to minimize the recall bias as well as a questionnaire review aiming at commonly underreported foods.
On the other hand, the key strengths of this study are using DAG to define a theoretical model based on heuristic rules, in order to select the minimum set of adjustments required to diminish the confounding and selection bias,
18 and urinary iodine excretion, as the most reliable measure to assess the current nutritional status of iodine in population studies.
15 Furthermore, it is important to note that a single measurement may not reflect the usual status. To our knowledge, this is the first Brazilian study to investigate the association of pre-pregnancy and current BMI with the nutritional status of iodine in pregnant women.
This study shows that a high BMI favors a reduction in the risk of iodine deficiency in pregnant women. Nevertheless, the development and/or maintenance of excess weight is not recommended, as it is related to several adverse outcomes in pregnancy that include prematurity, macrosomia, large for gestational age, among others.
29 In addition, the high consumption of ultra-processed foods during pregnancy observed in the present study can also trigger harmful health effects well documented in the literature.
30Therefore, we found a high prevalence of iodine-deficient pregnant women, and higher pre-pregnancy and current BMI were associated with higher urinary iodine levels. This association is related to the elevated consumption of ultra-processed foods in pregnant women with higher BMI. Thus, the consumption of ultra-processed foods must be discouraged among pregnant women, and the consumption of natural foods that are sources of iodine such as fish, crustaceans, milk, and eggs must be encouraged. Pregnant women with limited access to these foods are advised to take iodine supplementation under proper medical prescription.
AcknowledgementsWe would like to thank the National Council for Scientific and Technological Development (CNPq), the Maranhão Research and Scientific and Technological Development Support Foundation (Fapema) and the Coordination for the Improvement of Higher Education Personnel (Capes - Finance code 001) for their financial support.
References1. Simko M, Totka A, Vondrova D, Samohyl M, Jurkovicova J, Trnka M,
et al. Maternal body mass index and gestational weight gain and their association with pregnancy complications and perinatal conditions. Int J Environ Res Public Health. 2019; 10: 1751.
2. Barancelli MDC, Gazolla M, Schneider S. Characterization of the prevalence of excess weight in Brazil. BMC Public Health. 2022; 22 (1): 1131.
3. Andersen SL, Andersen S, Liew Z, Vestergaard P, Lundbye-Christensen S, Sorensen TIA,
et al. Maternal thyroid disease and adiposity in mother and child. Clin Endocrionol (Oxf). 2021; 94 (3): 484-93.
4. Cozzolino SMF. Nutrient bioavailability. 6ª. ed. Barueri, SP: Manoele; 2020.
5. Thyroid Disease in Pregnancy: ACOG Practice Bulletin, Number 223. Obstet Gynecol. 2020 Jun; 135 (6): e261-74.
6. Lecube A, Zafon C, Gromaz A, Fort JM, Caubet E, Baena JA, et al. Iodine deficiency is higher in morbid obesity in comparison with late after bariatric surgery and non- obese women. Obes Surg. 2015; 1: 85-9.
7. Crus-Mejía S, López HHD, Meza MN, Rosas IXR, Peña SL, Helguera OEA. Body massindex is associated with interleukin-1, adiponectin, oxidative stress and ioduria levels in healthy adults. Nutr Hosp. 2018; 4: 841-6.
8. Farebrother J, Dalrymple KV, White SL, Gill C, Brockbank A, Lazarus JH,
et al. Iodine status of pregnant women with obesity from inner city population in the United Kingdom. Eur J Clin Nutr. 2020; 5: 801-8.
9. Tresso BD, Tavares BB. Body mass index associated with the characteristics of puerperal women and two neonates. Rev Cuid 2019; 2: 678.
10. Scherr NCG, Nogueira AI, Rajão KMAB, Leite HV. Iodine nutritional status in a group of pregnant women from the state of Minas Gerais correlated with neonatal thyroid function. Rev Bras Ginecol Obstet. 2022; 44 (10): 909-14.
11. Abel MH, Caspersen IH, Sengpiel V, Jacobsson B, Meltzer HM, Magnus P, et al. Insufficient maternal iodine intake is associated with subfecundity, reduced foetal growth, and adverse pregnancy outcomes in the Norwegian Mother, Father and Child Cohort Study. BMC Med. 2020; 1: 211.
12. Abel MH, Brandlistuen RE, Sengpiel V, Aase H, Torheim LE, Meltzer HM,
et al. Language delay and poorer school performance in children of mothers with inadequate iodine intake in pregnancy: results from follow-up at 8 years in the Norwegian Mother and Child Cohort Study. Eur J Nutr. 2019; 58: 3047-58.
13. Marchioni DML, Gorgulho BM, Steluti J. Food consumption: assessment guide. 1
st ed. Barueri: Manoele; 2019.
14. Monteiro CA, Cannon G, Moubarac JC, Levy RB, Louzada MLC, Rauber F, et al. Ultra-processed foods: whats they are and how to identify them. Public Health Nutr. 2019; 22 (5): 936-41.
15. World Health Organization (WHO). Unicef. International Council for the Control of Iodine Deficiency Disorders. Assessment of iodine deficiency disorders and monitoring their elimination: a guide for programme managers. 3
rd ed. Geneva: WHO; 2007. 108p. [access in 2021 Sep 29]. Available from:
https://apps.who.int/iris/handle/10665/4378116. Institute of Medicine (US) and National Research Council (US), Committee to Reexamine IOM Pregnacy Weight Guidelines. Rasmussen KM, Yaktine AL (editors). Weight gain during pregnancy; reexamining the gudelines. Washigton (DC): National Academic Press; 2009.
17. Atalah E, Castillo C, Castro R, Aldea A. Propuesta de um nuevo estândar de evaluación nutricional de embarazadas. Rev Med Chil. 1997; 12: 1429-36.
18. Ankan A, Wortel IMN, Textor J. Testing Graphical Causal Models Using the R Package “dagitty”. Curr Protoc. 2021; 1(2): e45.
19. Cesar JA, Santos IS, Black RE, Chrestani MAD, Duarte FA, Nilson EAF. Iodine Status of Brazilian School-Age Children: A National Cross-Sectional Survey. Rev Nutrients. 2020; 12: 1777.
20. Brazil. Law Nº 6150, of december 3, 1974. Provides for the mandatory iodization of salt, intended for human consumption, its control by health agencies and other measures. Official Diary of the Union. 1974 Dec 04. [access in 2021 Sep 29]. Available from:
https://www.planalto.gov.br/ccivil_03/leis/l6150.htm.
21. Samson L, Hircsu I, Katko M, Bodor M, Gazdag A, Gazso A, et al. Lower educational status interferes with maternal iodine intake during both pregnancy and lactation. Endocr Connect. 2021; 10: 742-9.
22. Agência Nacional de Vigiência Sanitária (ANVISA). Relatório do monitoramento da iodação do sal destinado ao consumo humano. Brasília (DF): ANVISA; 2019. 52 p. [access 2024 Jun 11]. Available from:
https://www.gov.br/anvisa/pt-br/centraisdeconteudo/publicacoes/monitoramento/programas-nacionais-de-monitoramento-de-alimentos/relatorio-iodo-em-sal-para-consumo-humano-2019-retificacao-sem-marcas.pdf23. Pretell EA. Thyromobil Project in Latina América; Report of the study in Brazil. Relatório apresentado ao Ministério da Saúde. Brasília, DF, 2000. In: Pan American Health Organization (PAHO), World Health Organization (WHO). Bibliografia sobre deficiência de micronutrientes no Brasil 1990-2000. vol. 3 – Iodo e Bócio endêmico. Santos LMP (org.). Brasília (DF): PAHO; 2002. 40 p. [access 2024 Jun 11]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/pes_vol3.pdf24. Lacerda AT, Carmo AS, Sousa TM, Santos LC. Participation of ultra-processed foods in Brazilian school children's diet and associated factors. Rev Paul Pediatr. 2020; 38: e2019034.
25. Ferreira SMS, Navarro AM, Magalhães PKR, Maciele LMZ. Iodine insufficiency in pregnant women from the State of São Paulo. Arq Bras Endocrinol Metab. 2014; 3: 282-7.
26. Macedo MS. Nutritional status of maternal iodine during pregnancy and lactation and its relationship with iodine deficiency in newborns and infants in the city of Diamantina – MG [thesis]. Belo Horizonte: Faculty of Medicine the Federal University of Minas Gerais; 2017.
27. Yao N, Zhou C, Xie J, Zhou S. A cross-sectional research of iodine status of pregnant women in Chongqing, south-west China. Health Nutr. 2020; 5: 769-75.
28. Wang Z, Zang J, Shi Z, Zhu Z, Song J, Zou S. Iodine status 8 to 10 years old children within 20 years following compulsory salt iodization policy in Shangai, China. Nutri J. 2019; 18 (1): 63.
29. Xie D, Yang W, Wang A, Xiong L, Kong F, Liu Z, et al. Effects of pre-pregnancy body mass index on pregnancy and perinatal outcomes in women based on a retrospective cohort. Sci Rep. 2021; 11: 19863.
30. Pagliai G, Dinu M, Madarena MP, Bonaccio M, Iacoviello L, Sofi F. Consumption of ultra-processed foods and health status: a systematic review and meta-analysis. Br J Nutr. 2021; 3: 308-18.
Author's contributionSilva TCS: performed the research and wrote the manuscript. França AKTC, Viana KDAL and Franceschini SCC: performed the research, designed the research study, and contributed essential reagents or tools. Frota MTBA, Padilha LL, Carvalho WRC, Conceição SIO, Cantanhede NAC, Calado IL: performed the research and designed the research study. Viola PCAF: analyzed the data and wrote the manuscript. Carvalho CA: performed the research, designed the research study, analyzed the data, and wrote the manuscript.
All authors approved the final version of the article and declare no conflict of the interest.
Received on March 30, 2024
Final version presented on June 26, 2024
Approved on July 4, 2024
Associated Editor: Alex Sandro Souza


 ; Poliana Cristina de Almeida Fonseca Viola2
; Poliana Cristina de Almeida Fonseca Viola2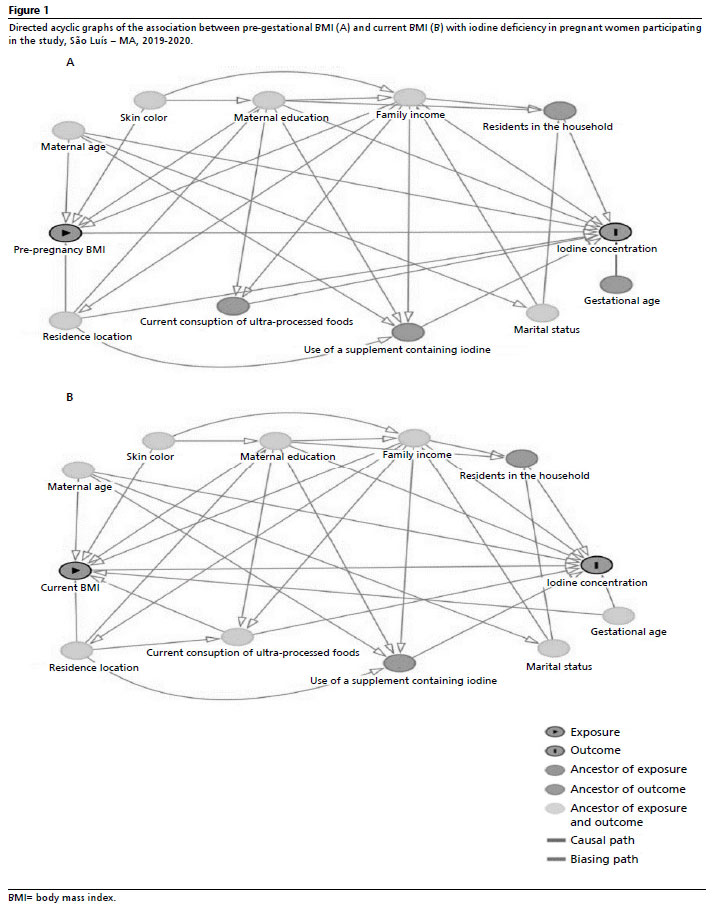






 Ler em português
Ler em português