ABSTRACT
OBJECTIVES: to analyze neonatal deaths according to avoidability and to analyze the temporal trend of neonatal mortality rate (NMR) in Niterói/RJ, 2012-2022.
METHODS: ecological time series study. Data from Sistema de Informação sobre Nascidos Vivos and Sistema de Informação sobre Mortalidade. NMRs were calculated according to maternal and neonatal variables and trends were estimated using the joinpoint regression.
RESULTS: the annual number of live births (LB) fell, with a decreasing trend among adolescents and those with low education level. Of the 324 deaths, most occurred early (0-6 days), by preventable causes in 68.6%, predominating those reducible by adequate care during pregnancy. The overall NMR remained stable, ranging from 4.2 to 6/1,000 LB, being higher at the extremes of maternal age (12.7 and 8.6/1,000 LB in 2022, adolescents and over 35 years old, respectively), in low education level mothers (27.6/1,000 LB in 2022), in neonates <1,500g and <32 weeks (293.1 and 250/1,000 LB in 2022, respectively). NMR trend was upward in low schooling women, white-colored, adolescents and those ≥35 years, in babies weighing <1,500g and >2,500g, and for avoidable causes.
CONCLUSIONS: the high proportion of preventable causes reveals the reduction potential. There was inequality in NMR and its trend, demanding more equitable health actions.
Keywords:
Neonatal mortality, Health information systems, Causes of death, Time series study, Health inequities
RESUMO
OBJETIVOS: analisar os óbitos neonatais segundo evitabilidade e a tendência temporal da taxa de mortalidade neonatal (TMN) em Niterói/RJ, de 2012-2022.
MÉTODOS: estudo ecológico de série temporal. Dados provenientes do Sistema de Informações sobre Nascidos Vivos e Sistema de Informação sobre Mortalidade. As TMN foram calculadas segundo variáveis maternas e neonatais e as tendências estimadas pela regressão joinpoint.
RESULTADOS: o número anual de nascidos vivos (NV) diminuiu, com tendência decrescente entre mães adolescentes e de baixa escolaridade. Dos 324 óbitos, a maioria ocorreu precocemente, por causas evitáveis (68,6%), predominando aquelas reduzíveis por adequada atenção à gestação. A TMN global mostrou estabilidade, entre 4,2 e 6,0/1000NV, mais elevada nos extremos etários maternos (12,7 e 8,6/1.000 NV em 2022, adolescentes e maiores de 35 anos, respectivamente), nas mães com baixa escolaridade (27,6/1.000 NV em 2022), nos neonatos <1.500g e <32 semanas (293,1 e 250/1.000 NV em 2022, respectivamente). A tendência da TMN foi crescente entre mulheres de baixa escolaridade, brancas, adolescentes e ≥35 anos, nas faixas de peso <1.500g e >2.500g, e por causas evitáveis.
CONCLUSÕES: a elevada proporção de causas evitáveis revela o potencial de redução. Houve desigualdade da TMN e sua tendência, demandando ações de saúde mais equânimes.
Palavras-chave:
Mortalidade neonatal, Sistemas de informação em saúde, Causas de morte, Estudo de séries temporais, Desigualdades em saúde
IntroductionThe monitoring of infant deaths is still a priority worldwide
1. During childhood, the neonatal period is the most vulnerable and, globally, neonatal mortality accounts for over half of infant deaths.
1 In the context of the Sustainable Goals, the goal for Neonatal Mortality Rate (NMR) is the reduction, until 2030, to a maximum of 12 per 1,000 live births (LB). Some European countries (Germany, Denmark, France, Finland, Italy, Norway, Portugal, England, Scotland, Wales, Northern Ireland and Sweden), and the United States and Canada, in North America, have NMR under or equal to 3 per 1,000 LB, whilst in Latin America, Chile, Uruguay (4.0/1000 LB) and Cuba (2/1000 LB) have the lowest values.
1The most recent estimate in Brazil is from 2021 and registered a NMR of 8.0/1,000 LB, which represents a great advance, since in 2000, the value was 19/1000 LB.
1 Still, socioeconomic inequalities within Brazilian regions lead to different scenarios in a national perspective. For the year 2020, these rates were 9.9 in the North Region, 9.4 in the Northeast, 7.9 in the Midwest, 7.6 in the Southeast and 6.8/1,000 LB in the South Region.
2The state of Rio de Janeiro demonstrated the highest rates of infant and neonatal mortality among the other states that compose the Southeast Region in 2020: 14.3 and 8.8 per 1000 LB, respectively.
2The causes of neonatal death are mostly avoidable, with the presence of qualified healthcare during the prenatal and delivery period, and for the newborn.
3 In Brazil, from 2000 to 2018, the most frequent causes of avoidable neonatal death were respiratory distress syndrome, asphyxia at birth and sepsis, and a decreasing trend of mortality due to these causes was observed in Brazilian regions from 2000 to 2008, mostly in the beginning of the analyzed period, with rare exceptions.
3,4The use of information systems related to vital statistics has been increasingly relevant in the study of infant mortality.
4-9 The Live Birth Information System (Sinasc – Portuguese acronym) and the Mortality Information System (SIM – Portuguese acronym) are global information systems from the Ministry of Health (MH), which have demonstrated a relevant increase in quality for the last years, mainly the Sinasc.
5,6Local studies, in a level of smaller areas, such as a municipality, have been upheld due to their potential in the identification of health inequalities, which many times are dissimulated by national or state average statistics. Considering the municipality management, local indicators are strongly relevant to the definition of public policies.
9This study aims to analyze neonatal deaths due to avoidable causes and the temporal trend between 2012 and 2022 in the municipality of Niterói (RJ). We also expect to contribute to the identification of inequalities and to subside municipal public policies that aim at vulnerable populations.
MethodsIt is an ecological annual time series study (2012 to 2022). The population is composed of live births and neonatal deaths, of mothers residing in the city of Niterói.
The inclusion criteria of live births (LB) were single fetus pregnancy, gestational age (GA) equal or above 22 weeks, birth weight equal or above 500g. Multiple pregnancies or neonates with birth weight <500g and GA <22 weeks were excluded due to their differentiated risks and low viability, respectively.
10 The deaths were those that occurred in the neonatal period (early from 0 to 6 and late from 7 to 27 days), with the same inclusion criteria than live births.
The city of Niterói has 480 thousand inhabitants, of which 5000 are under one year of age. The city presents the best Human Development Index (HDI) in Rio de Janeiro (RJ) state, and the seventh position in the national ranking.
11 The city presents a structure of services from the primary to quaternary levels, possesses three public hospitals and three private hospitals with maternity, serving as the reference for the demand from other municipalities that compose Metropolitan Region II of the state of Rio de Janeiro.
12The source of data was the website about health information of the Health Secretariat of Rio de Janeiro state, from which it was possible to access data from Sinasc and SIM (RJ).
Annual neonatal mortality rates (NMR) were calculated with the equation [number of neonatal deaths *1,000/ number of live births].
The profile of live births and the NMRs were analyzed according to maternal sociodemographic variables and the prenatal care, and those from newborns (NB), namely:
-Maternal variables obtained from Sinasc: age (≤19 years, 20 to 34 years and ≥35 years), schooling (≤7 years, 8 to 11 years and ≥12 years) and race/color (white, black and brown), prenatal consultations (0 to 3, 4 to 6 and 7 and more).
-Newborn (NB) variables obtained from Sinasc: birth weight (<1,500g – very low weight; <2,500 – low weight and ≥2,500g non-low weight), 5
th minute Apgar score (0 to 3 – severe asphyxia; 4 to 6 – moderate asphyxia and 7 to 10 – good vitality), gestational age (<32weeks – very preterm, <37 weeks – preterm and ≥37 weeks non-preterm).
-Neonatal deaths variables obtained from SIM: maternal age (≤19 years, 20 to 34 years and ≥35 years), maternal schooling (≤7 years, 8 to 11 years and ≥12 years), color of NB, birth weight (<1,500g – very low weight; <2,500 – low weight and ≥2,500g non-low weight), gestational age (<32weeks – very preterm, <37 weeks – preterm and ≥37 weeks non-preterm).
The variables "prenatal consultations" and "5
th minute Apgar score" are only present at Sinasc. In order to assess the completeness of information selected from SIM and Sinasc, the score proposed by Romero and Cunha
13 was used, which corresponds to the following levels of evaluation, according to the percentage of absent information: excellent (lower than 5%), good (5% to <10%), regular (10% to <20%), bad (20% to <50%) and very bad (50% or more).
For the classification of death causes, the Brazilian List of Avoidable Causes of Death (LBE – Portuguese acronym) was used, by intervention of the Unified Health System in children under 5 years of age.
15 This document proposes the organization of deaths according to avoidable causes, ill-defined and not clearly avoidable. The classifications within the avoidable causes group comprises every action of mother and child care, such as immunoprevention, assistance to women in pregnancy and delivery, assistance to the fetus and to the newborn and those related to adequate diagnosis and treatment of pathologies. In addition, the frequency of specific causes were described (three digits of the ICD-10) according to LBE groups.
The maternal variables "age", "color" and "schooling" were analyzed for the characterization of inequalities of magnitude and trend of neonatal death risk. The age range of 20-34 years, white color and schooling ≥12 represented the situation of lower vulnerability.
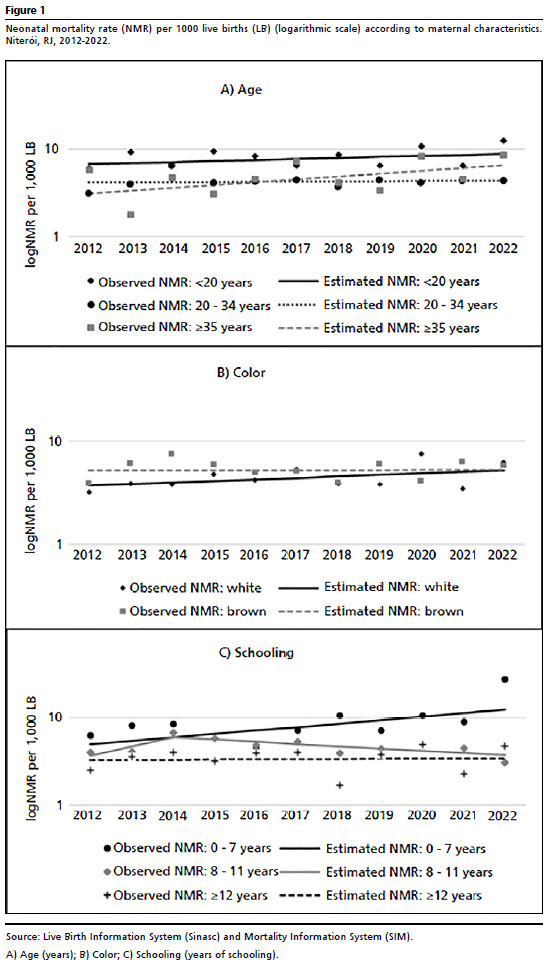
For the trend analysis in the time series, the Joinpoint regression model was used, which adjusts, in a logarithmic scale, linear trends and changes of these trends (joinpoints). For the significance test, we use the Monte Carlo Permutation Method, which adjusts the better line for each segment. Since these segments are not established, the estimated trends are represented by their respective annual percentages (MPA – Portuguese acronym). The MPA is calculated in this way: MPA = 100x (It+1 – It) / I, when I is the indicator of the year (It) and in the next year (It+1). Considering the logarithmic scale regression, log (it) = (b0 + b1t), MPA = 100 x (eb1 – 1), and the 95% confidence interval is calculated by the parametric model. The models were evaluated with and without autocorrelation term (AC), maintaining the AC term in the models in which the MPA underwent a change higher than 0.2%. We highlight that the joinpoints or trend change, if present in the time series, are not necessarily coincident between the variables and the categories of the variables, and, thus, the segmentation of periods of estimated trends may differ. The model identifies the presence and temporal location of joinpoints. The trends of annual rates of neonatal mortality according to maternal characteristics demonstrated in graphs were better visualized in logarithmic scales, allowing the observation of the percentage distance between two points.
The project was approved by the Research and Ethic Committee of the Faculty of Medicine of the Fluminense Federal University (CAE nº71323023.00.0000.5243) under opinion 6.592.725, from 12/19/2023.
ResultsThe absolute number of LB was 5721 in 2012 and 5016 in 2022, demonstrating, thus, a decrease of 15.6% for the period. The maternal and prenatal care sociodemographic information and that of the LB obtained from Sinasc had demonstrated excellent completeness, with less than 5% of ignored information.
The proportion of adolescent mothers is the lowest among the age ranges and has demonstrated a decrease, the most intense in the period from 2017 and 2022. On the other hand, there was a constant increase of pregnancies of those with 35 years or more. The schooling profile demonstrates a lower proportion of women with low schooling, with a constant trend of decrease. Inversely, the proportion of mothers with medium and high schooling has been increasing since 2014. The proportion of white mothers is the highest of the municipality, although it has been demonstrating a decreasing trend since 2012. The proportion of black mothers, the lowest in this variable, demonstrated an increasing trend. Until 2019, the registry of brown mothers had been increasing and kept stable from 2019 to 2022 (Table 1).
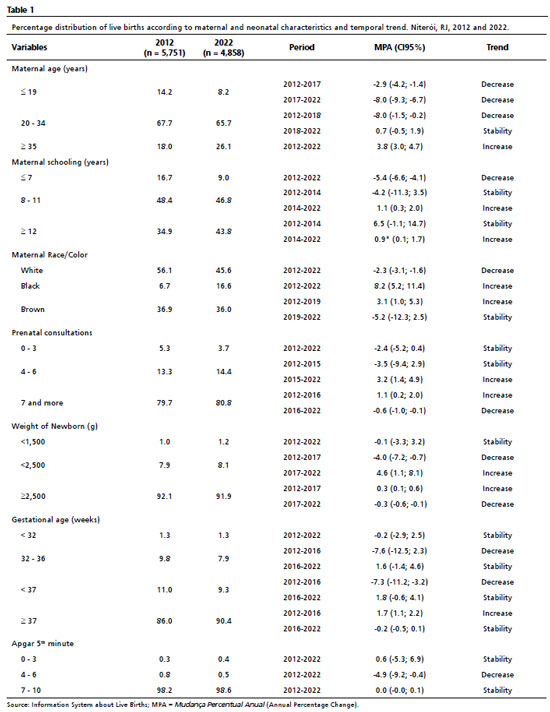
Around 80% of women performed seven or more consultations in the entire period, although, since 2016, a decreasing trend of this percentage was registered. The proportion of women with four to six consultations increased since 2015 (Table 1).
The live births concentrated on the ranges of weight ≥2,500g and gestational age ≥37 weeks. From 2017, it was observed an increase in the prevalence of neonates with low birth weight (without increase of the extreme group, of <1,500g), reaching 8.1% of the total. On the other hand, the prevalence of prematurity decreased, from 11 to 9.3% (without changes in the extreme group of <32 weeks). Most neonates are born with good vitality conditions, with only 1% of registration of asphyxia. Severe asphyxia maintained stability and moderate asphyxia decreased (Table 1).
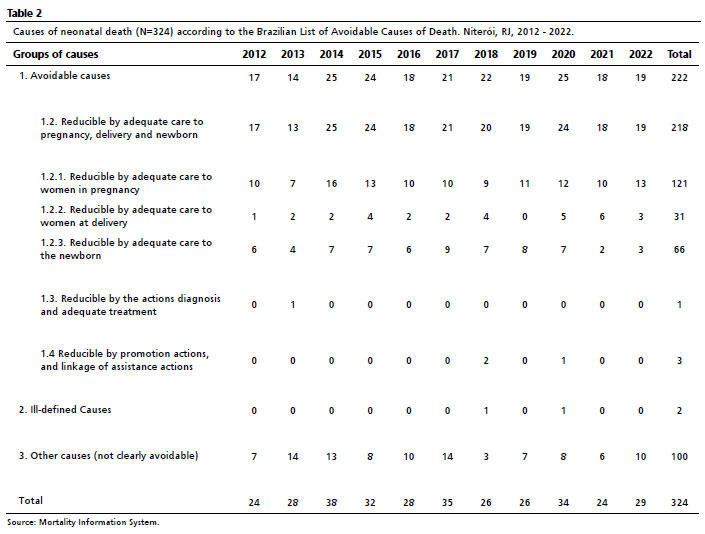
324 neonatal deaths were registered, of which, around 70% occurred in the early neonatal period (0-6 days). Most deaths are located in the groups of newborns with weight <2,500g (75.2%) and gestational age <37 weeks (72%). The annual completeness of information obtained from SIM for birth weight was classified as excellent, and for gestational age varied from excellent to good. For the maternal sociodemographic variables, the completeness of SIM varied over the period: age was between good (5 to 10% of ignored information) and excellent, and color and schooling, between regular (10 to 20%) and excellent.
According to LBE, 68.5% of deaths were clearly avoidable, whilst 30.9% were considered non-clearly avoidable (Table 2). Among the avoidable causes, the highest proportion was that of the subgroup "reducible by assistance to women during pregnancy". In second place, the subgroup "reducible by adequate care to the newborn". There were no deaths in the subgroup 1.1 (reducible by immunoprevention actions). Only for two neonatal deaths, the certified cause of death was ill-defined (Table 2).
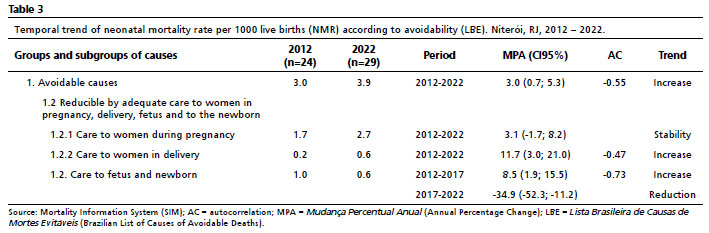
The time series of NMR according to avoidable causes demonstrated an increasing trend, 3% per year, with different behaviors: stability of causes related to pregnancy, the increase of those reducible by adequate assistance to delivery and the neonate, followed by reduction of the latter (Table 3). Causes related to codes 1.3 and 1.4 were not analyzed, due to the low frequency of deaths.
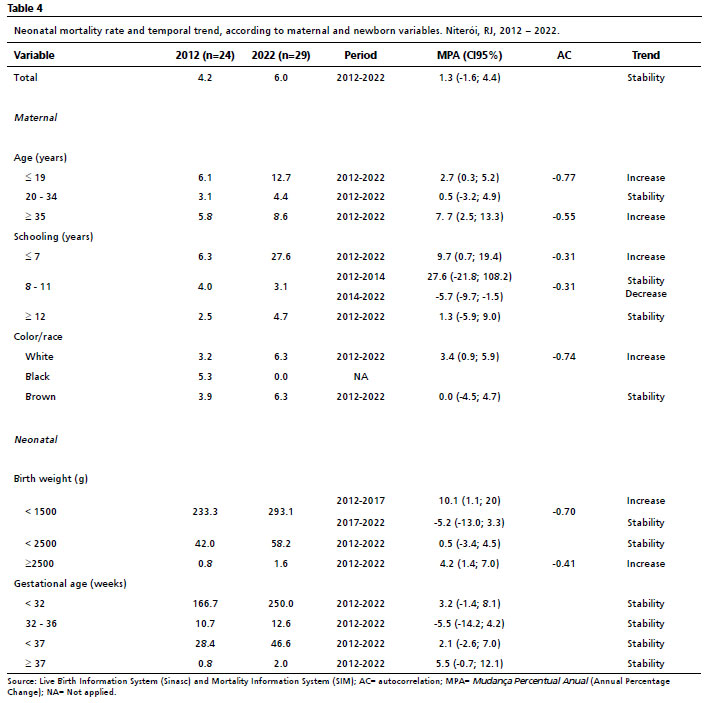
In Table 4, neonatal mortality rates are described, totally and according to maternal and NB variables. The number of neonatal deaths was 24 in 2012 and reached 29 cases in 2022. The global NMR in Niterói, maintained itself stable in the period, with oscillations.
The NMR was higher in the age extremes – adolescent mothers and those with 35 years or more, both with an increasing trend. It was also always more elevated in the range of low schooling, the only in which was observed an increase in the period. On the other hand, since 2014, NMR in mothers with intermediate schooling decreased. There was a change in NMR profile by color/race of mothers, which concentrated the highest value of neonates of black women, which, at the end of the period, possessed the lowest NMR. There was an increasing trend in the NMR among neonates of white women (Figure 1).
The NMR was higher as the ranges of birth weight and gestational age were lower. The trend was increasing in the range of <1,500g (very low birth weight – VLBW), between 2012 and 2017, and the range >2,500g, in the entire period.
In 2020, there was an increase in the absolute number of deaths, without relevant changes in the total of live births, inversely, in 2021 and 2022, the absolute number returned to the pre-pandemic level, although the birth rate decreased in the municipality (data not shown in table). The profile of avoidability was maintained in the range >2,500g, with predominance of congenital malformations as death cause.
DiscussionWomen from Niterói that had LB were predominantly of the 20-34 years old range, with high/intermediate schooling, white color and high attendance to prenatal consultations. In the study period, there was a decrease of pregnancy in adolescence and an increase in schooling. The total neonatal mortality rates were stable, being around 70% of them avoidable, mainly due to adequate assistance during pregnancy. For adolescent mothers and those with 35 years or more, white and those with low schooling, there was an increase in NMR.
The reduction of proportion of adolescents and the increase in proportion of pregnant women with 35 years or more were already reported in the municipality, in the time series of 2000 to 2009.
15 The report
Saúde Brasil 2022also exposes, in a national level, the reduction of the fertility rate of women aged 10-19 and an increase in the 40-49 years old range.
2 According to the document, these are reverberations of the trend of delayed childbearing, which is compatible, mainly, with the demographic transition Brazil is going through since the 90s.
2The decrease of pregnancy in adolescence is beneficial, since pregnancy in this stage of life is generally associated with more severe maternal, perinatal and infant outcomes.
16 Likewise, the increase in pregnant women with 35 or more, which is considered an age change that follows development and educational level, may lead to a higher risk of unfavorable perinatal and maternal outcomes.
17,18Analyzing prenatal care, we observed that, despite the high percentage of pregnant women that attended seven or more consultations, this category demonstrated a decrease, which is concerning. It is worth highlighting that the inadequacy and/or absence of prenatal consultations are risk factors for neonatal mortality.
19Compared to the LBW prevalence in the 2000-2009 period, the current prevalence was lower.
15 In 2017, the LBW prevalence in Brazil was 8.5%, with the Southeast region demonstrating the higher values of the country, and the State of Rio de Janeiro demonstrated 9.0%.
20 On the other hand, the proportion of preterm NB, even with the drop observed in the period from 2012 to 2016, was higher than that observed in the 2000-2009 time series, when it was under 8%.
15 In Brazil, the estimate for the period from 2011 to 2018 was 9.4%.
20 It must be remembered that the gestational age variable suffered modification in the certificate of live birth, prioritizing the date of the last menstruation, although it still has validity problems.
21The NMR in Niterói was stable in the analyzed period, inferior to the national level, increasing in some specific groups. At the national level, there was a drop of NMR from 13.6 in the year 2000 for 8.5 per 1,000 LB in 2018.
3,4 In the municipality of Rio de Janeiro, from 2000 to 2018, the NMR was decreasing, reaching 7.8/1,000 LB in the last year observed.
22 If considered neonatal mortality due to avoidable causes, at national level, from 2000 to 2018, the reduction was 10.9 to 6.8 per 1,000 LB.
3 In Niterói, there was an increase of the avoidable causes rate of 3.0 to 3.9/1,000 LB, although it must be considered that it is already a significantly low level. The state with the lowest NMR due to avoidable causes was Santa Catarina, however, with a higher value (4.8) than Niterói.
3 The disruption of health services, due to the outbreak of COVID-19 pandemic, may have also affected the different moments of the prenatal and perinatal care of the municipality, although our study did not perform a profound analysis of the quality of care.
Corroborating the literature, the lower the weight and/or gestational age, the higher the NMR.
19,23 In a study of 15 countries of high/medium income, between 2000 and 2020, the NMR for the VLBW was 207/1000 LB and for the range of GA ≤32 weeks, 141/1,000 LB.
23 In Niterói, the values stood, respectively, around 275 and 215/1,000 LB, with an increasing trend for VLBW. It is worth highlighting that most studied countries had a very low NMR, under or equal to 3/1,000 LB, which indicates excellent socioeconomic conditions and perinatal care.
Besides the biological variables, already corroborated in the literature, sociodemographic conditions were observed to be associated with mortality, revealing inequality in the "neonatal death" outcome in the municipality. It should be considered that, in the period analyzed, two great epidemics affected the national birth rate, Zika virus in 2015 and COVID-19 in 2020.
2,24 In this manner, the increase of the rate for the analyzed period may be explained, partially, because of the diminish of the denominator and not only the absolute increase in the number of deaths.
2Similar results were observed in studies of national range, such as the high NMR values in the age extremes and in the low schooling population.
25 It is relevant to note the increase in NMR for non-low birth weight newborns, however, without alterations in the avoidability profile. This fact should be interpreted as a sentinel event, since these deaths can be avoided with simple and low cost interventions, in both labor and delivery. In 2018, among the neonatal deaths in the country, low birth weight and prematurity predominated, and for the early neonatal component (0-6 days), extreme low weight prevailed.
2The NMR was higher between adolescents and women aged 35 years or more, both with an increasing trend. In Brazil, between 2006 and 2016, the highest NMR values were concentrated similarly in the groups of mothers with 10-14 and 45-49 years (10.4 and 10.5 deaths/1,000 LB), with values twice higher than those found between mothers with 25-29 and 30-24 years (4.7 and 4.9 deaths/1000 LB).
25 In the state of Rio de Janeiro, in the period from 2004 to 2010, children of adolescent mothers and those aged ≥35 years also demonstrated higher chance of death compared to mothers in the age range of 20-34 years.
26 Veloso
et al.
19 identified maternal age range equal or above 35 years as an important risk factor for neonatal mortality.
Among adolescent mothers, the risk of neonatal mortality is increased, but cannot be analyzed independently or even with a purely biological characteristic, since pregnancy in adolescence occurs in a context of multifactorial vulnerability and is intimately associated with socioeconomic conditions of the population.
22 There was a decrease in the percentage of adolescent mothers among the live births in Niterói, but this group seem to maintain an elevated risk. Although 80% of women from the city had attended seven or more prenatal consultations, a study of the period from 2000 to 2009 demonstrated that adolescent mothers from Niterói did not reach this value.
27The highest NMR are observed in NB of mothers with low schooling and it still was observed an increasing trend, in opposition to the range of 8 years or more of schooling, which demonstrated a decreasing trend. In Brazil, from 2006 to 2016, the NMR was higher between the NB of mothers without any schooling (6.7 deaths/1,000 LB) and had the lowest value between mothers with 12 or more years of schooling (4.3 deaths/ 1,000 LB).
25 In the period from 2000 to 2018, in the municipality of Rio de Janeiro, the NMR analysis related to maternal schooling demonstrated concentration and increase in the group of women with low schooling, which reinforces the inequality in the care provided to this group from the population.
22Schooling is intimately associated with the age of puerperal women and demonstrates an isolated risk for the chance of neonatal death, however it is associated to age extremes as well.
26 The interaction between low schooling and advanced age is significant, considering that this is a group characterized by the exposition to multiple risk factors all over the life.
26 In Brazil, for the age ranges of 10-19 and 20-34, the increase of schooling corresponded directly to the reduction of NMR, whilst among mothers with age ≥35 years, the NMR was higher for those with 1-11 years of schooling, followed by those without schooling, and lastly, those mothers with 12 years or more of schooling.
25In Niterói, the NMR among white women demonstrated an increasing trend, and kept stable among brown mothers. It was not possible to evaluate the NMR trend between black women, due to the low absolute number of deaths. It was perceived that NMR, formerly higher in LB of black mothers, got closer to values of the white and brown population. That is, the inequality between racial groups diminished in the last years, partially, due to differences in the self-declaration.
28 Between 2012 and 2018, the neonatal mortality in Brazil was 37% higher (CI95% = 1.34-1.40) in children of black mothers compared to those of white mothers.
8Socioeconomic vulnerability, represented by low schooling and black or brown skin color, was also reported as an important determinant of neonatal death in other national studies.
29,30The occurrence of only two deaths by ill-defined cause is a positive advance for the quality or basic cause certificate of neonatal deaths. On the other hand, a limitation of the study regards the completeness of the fields of death certificates referring mainly to maternal color and schooling, that still need to be improved. Another limitation is inherent to data sources. In spite of the information systems used possess several amounts of information, it was not possible to analyze the quality of healthcare services and identify changes, for example, which occurred in the hospital assistance, in the study period. It was also not possible to assess the subgroup of late preterm newborns, since the categories of gestational age from Sinasc are 22-27, 28-31, 32-36, 37-41 and ≥42 weeks. Lastly, the autocorrelations demonstrated to be negative, being optional to include the respective AC terms in the model. We opted to include to highlight trends that, in the model without autocorrelation, were identified, however without achieving significance in some categories.
In the city of Niterói, in spite of good perinatal indicators, we observed stagnation of the neonatal mortality rate (NMR), inequality and the increase of avoidable causes. Although the magnitude of the neonatal mortality rate (between 4.2 and 6.0/1,000 LB) is not high, the proportion of avoidable causes reveals the potential of reduction. It is still possible to reach lower values, even for extreme weight and gestational age ranges. In these last 11 years, NMR was unequal between the population groups and increased among adolescents and older women, those with low schooling and white women. Only the racial inequality was diminished, and groups of higher vulnerability, related to maternal age and schooling, persisted. The health actions should aim at population groups of higher risk, searching for equity.
References1. United Nations Children's Fund (UNICEF). Levels and Trends in Child Mortality: Report 2022. Estimates developed by the United Nations Inter-agency Group for Child Mortality Estimation. New York: UNICEF; 2023. [access in 2023 Mar 1]. Available from:
https://childmortality.org/wp-content/uploads/2023/01/UN-IGME-Child-Mortality-Report-2022.pdf2. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise Epidemiológica e Vigilância de Doenças Crônicas não Transmissíveis. Saúde Brasil 2022: análise da situação de saúde e uma visão integrada sobre os fatores de risco para anomalias congênitas. Brasília (DF): Ministério da Saúde; 2023. p. 51-69. [access in 2023 Mar 1]. Available from:
https://svs.aids.gov.br/daent/centrais-de-conteudos/publicacoes/saude-brasil/saude-brasil-2022-anomalias-congenitas.pdf3. Prezotto KH, Oliveira RR, Pelloso SM, Fernandes CAM. Tendência da mortalidade neonatal evitável nos Estados do Brasil. Rev Bras Saúde Mater Infant. 2021; 21 (1): 301-9.
4. Prezotto KH, Bortolato-Major C, Moreira RC, Oliveira RR, Melo EC, Silva FRT, et al. Mortalidade neonatal precoce e tardia: causas evitáveis e tendências nas regiões brasileiras. Acta Paul Enferm. 2023; 36: eAPE 02322.
5. Maia LTS, Souza WV, Mendes ACG, Silva AGS. Use of linkage to improve the completeness of the SIM and SINASC in the Brazilian capitals. Rev Saúde Pública. 2017; 51: 112.
6. Szwarcwald CL, Leal MC, Pereira APE, Almeida WS, Frias PG, Damacena GM. Avaliação das informações do Sistema de Informações sobre Nascidos Vivos (SINASC), Brasil. Cad Saúde Pública. 2019; 35 (10): e00214918.
7. Kale PL, Fonseca SC. Mortalidade neonatal específica por idade e fatores associados na coorte de nascidos vivos em 2021, no estado do Rio de Janeiro, Brasil. Rev Bras Epidemiol. 2022; 25: e220038.
8. Rebouças P, Goes E, Pescarini J, Ramos D, Ichihara MY, Sena S. Ethnoracial inequalities and child mortality in Brazil: a nationwide longitudinal study of 19 million newborn babies. Lancet Glob Health. 2022; 10 (10): e1453-e1462.
9. Malta DC, Almeida MF, Ribeiro ALP. Estimates in small geographic areas: a necessary step towards reducing health inequalities. Rev Bras Epidemiol. 2021; 24 (Suppl. 1): e210001.
10. Santana DS, Silveira C, Costa ML, Souza RT, Surita FG, Souza JP, et al; WHO Multi-Country Survey on Maternal and Newborn Health Research Network. Perinatal outcomes in twin pregnancies complicated by maternal morbidity: evidence from the WHO Multicountry Survey on Maternal and Newborn Health. BMC Pregnancy Childbirth. 2018; 18 (1): 449.
11. Instituto Brasileiro de Geografia e Estatística (IBGE). Síntese de Indicadores Sociais: uma análise das condições de vida da população brasileira: 2012. Rio de Janeiro: IBGE; 2013. [access in 2023 Mar 1]. Available from:
https://biblioteca.ibge.gov.br/visualizacao/livros/liv62715.pdf12. Governo do Estado do Rio de Janeiro. Secretaria de Saúde RJ. Subsecretaria Geral. Planejamento em Saúde - Regiões de Saúde. Planejamento Regional Integrado. [Internet]. [access in 2023 Mar 1]. Available from:
https://www.saude.rj.gov.br/planejamento-em-saude/regioes-de-saude/planejamento-regional-integrado13. Romero DE, Cunha CB. Avaliação da qualidade das variáveis socioeconômicas e demográficas dos óbitos de crianças menores de um ano registrados no Sistema de Informações sobre Mortalidade do Brasil (1996/2001). Cad Saúde Pública. 2006; 22 (3): 673-81.
14. Malta DC, Sardinha LMV, Moura L, Lansky S, Leal MC, Szwarcwald CL. Atualização da lista de causas de mortes evitáveis por intervenções do Sistema Único de Saúde do Brasil. Epidemiol Serv Saúde. 2010; 19 (2): 173-6.
15. Rozario S, Brito AS, Kale PL, Fonseca SC. Série temporal de características maternas e de nascidos vivos em Niterói, RJ. Rev Bras Saúde Matern Infant. 2013; 13 (2): 137-46.
16. Marvin-Dowle K, Soltani H. A comparison of neonatal outcomes between adolescent and adult mothers in developed countries: a systematic review and meta-analysis. Eur Obstet Gynecol Reprod Biol X. 2020 Feb; 6: 100109.
17. Carreira GB, Dutra VGP, Silva JHCM, Guimaraes RM. Desigualdade social, desenvolvimento humano e padrão de fecundidade no Brasil, 2000-2010. Rev Bras Saúde Mater Infant. 2019; 19 (1): 217-32.
18. Pinheiro RL, Areia AL, Mota Pinto A, Donato H. Advanced maternal age: adverse outcomes of pregnancy, a meta-analysis. Acta Med Port. 2019 Mar; 32 (3): 219-26.
19. Veloso FCS, Kassar LML, Oliveira MJC, Lima THB, Bueno NB, Gurgel RQ, et al. Analysis of neonatal mortality risk factors in Brazil: a systematic review and meta-analysis of observational studies. J Pediatr (Rio J). 2019; 95 (5): 519-30.
20. Paixão ES, Blencowe H, Falcao IR, Ohuma EO, Rocha ADS, Alves FJO. Risk of mortality for small newborns in Brazil, 2011-2018: a national birth cohort study of 17.6 million records from routine register-based linked data. Lancet Reg Health Am. 2021 Nov; 3: None.
21. Henriques LB, Alves EB, Vieira FMDSB, Cardoso BB, D'Angeles ACR, Cruz OG. Acurácia da determinação da idade gestacional no Sistema de Informações sobre Nascidos Vivos (SINASC): um estudo de base populacional. Cad Saúde Pública. 2019; 35 (3): e00098918.
22. Kale PL, Fonseca SC, Oliveira PWM, Brito ADS. Fetal and infant mortality trends according to the avoidability of causes of death and maternal education. Rev Bras Epidemiol. 2021; 24 (Suppl. 1): e210008.
23. Suárez-Idueta L, Blencowe H, Okwaraji YB, Yargawa J, Bradley E, Gordon A, et al.; National Vulnerable Newborn Mortality Collaborative Group and Vulnerable Newborn Measurement Core Group. Neonatal mortality risk for vulnerable newborn types in 15 countries using 125.5 million nationwide birth outcome records, 2000-2020. BJOG. 2023 May 8.
24. Marteleto LJ, Sereno GF, Coutinho RZ, Dondero M, Alves SV, Lloyd R, et al. Fertility trends during successive novel infectious disease outbreaks: Zika and COVID-19 in Brazil. Cad Saúde Pública. 2022; 38 (4): EN230621.
25. Costa PH, Alves LC, Beluzo CE, Arruda NM, Bresan RC, Carvalho T. Maternal characteristics and the risk of neonatal mortality in Brazil between 2006 and 2016. Int J Popul Studies. 2020; 5 (2): 24-33.
26. Fonseca SC, Flores PVG, Camargo Jr. KR, Pinheiro RS, Coeli CM. Maternal education and age: inequalities in neonatal death. Rev Saúde Pública. 2017; 51: 94.
27. Fonseca SC, Monteiro DS, Pereira CM, Scoralick AC, Jorge MG, Rozario S. Desigualdades no pré-natal em cidade do Sudeste do Brasil. Ciên Saúde Colet. 2014; 19 (7): 1991-8.
28. Caldas ADR, Santos RV, Cardoso AM. Iniquidades étnico-raciais na mortalidade infantil: implicações de mudanças do registro de cor/raça nos sistemas nacionais de informação em saúde no Brasil. Cad Saúde Pública. 2022; 38 (4): e00101721.
29. Rocha NM, Kale PL, Fonseca SC, Brito AS. Neonatal near miss and mortality and associated factors: cohort study of births in the city of Rio de Janeiro, RJ, Brazil. Rev Paul Pediatr. 2023; 41: e2021302.
30. Varela AR, Schneider BC, Bubach S, Silveira MF, Bertoldi AD, Duarte LSM. Mortalidade fetal, neonatal e pós-neonatal e fatores associados na coorte de nascimentos de 2015 de Pelotas, Rio Grande do Sul, Brasil. Cad Saúde Pública. 2019; 35 (7): e00072918.
Author's contribution: Machado SSV and Fonseca SC: conceptualization, data collection, formal analysis, investigation, method, management of the project and writing of the manuscript. Kale PL: collaboration in the formal analysis, writing and review of the manuscript.
All authors approved the final version of the article and declare no conflict of interest.
Received on October 24, 2023
Final version presented on April 22, 2024
Approved on April 23, 2024
Associated Editor: Karla Bomfim


 ; Pauline Lorena Kale2
; Pauline Lorena Kale2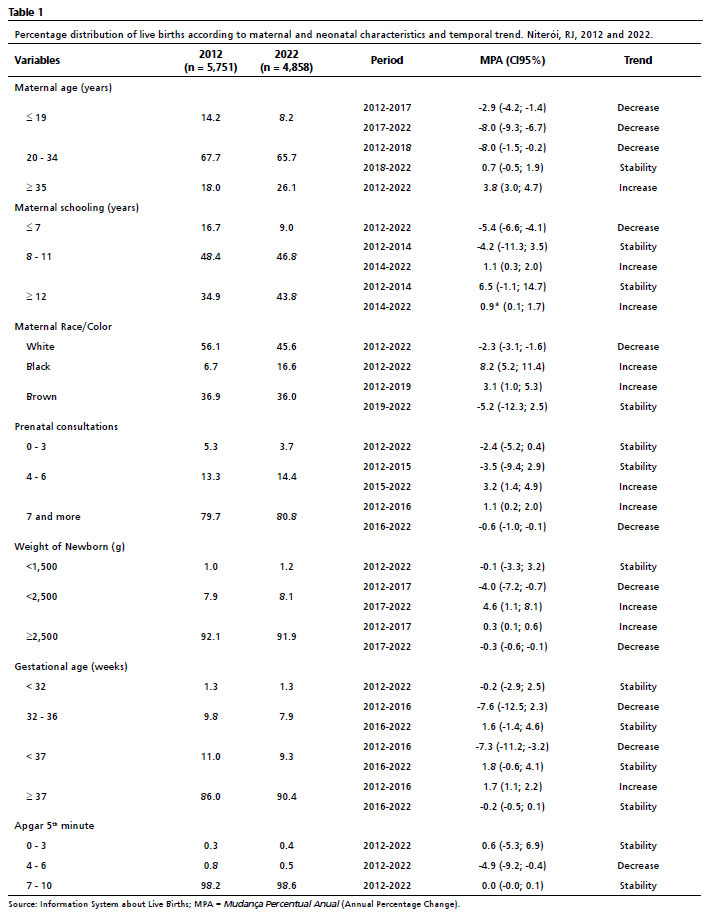






 Ler em português
Ler em português