ABSTRACT
OBJECTIVES: to identify the factors and variables that interfere with the maternal perception of security at postpartum.
METHODS: a cross-sectional study, carried out in three Portuguese hospital units, with a non-probabilistic sample of 352 puerperal women, recruited from the postpartum units on the day of hospital discharge after delivery. Maternal sociodemographic and obstetric characteristics, as well as data on monitored pregnancy, childbirth and infant feeding, were collected through the application of a questionnaire developed by the researchers. For the analysis of maternal perception of security, the instrument "Parents' postnatal sense of security" (PPSS) was used. Descriptive and inferential statistics were used for data analysis.
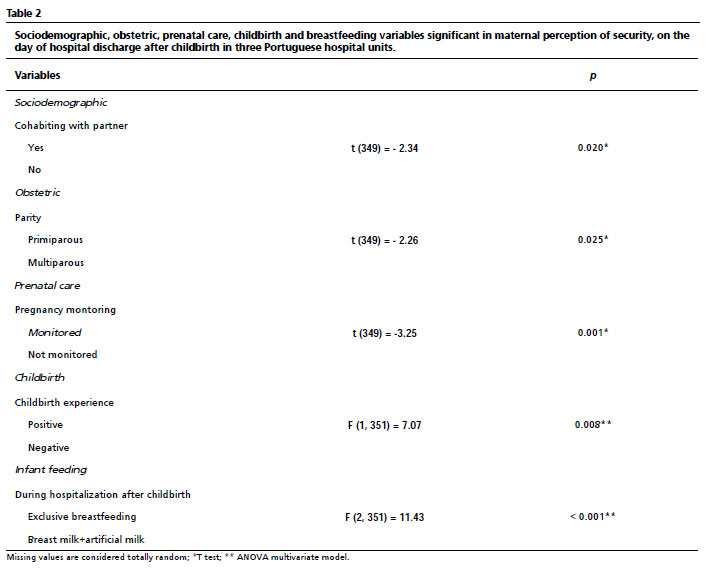
RESULTS: women who lived with their partner (t (349) = - 2.34, p=0.020), were multiparous (t (349) = - 2.26, p=0.025), had pregnancy monitored (t (349) = -3.25, p=0.001), had a positive childbirth experience (F (1, 351) = 7.07, p=0.008) and those who exclusively breastfed during hospitalization (F (2, 351) = 11,43, p<0.001), presented greater perception of security at postpartum.
CONCLUSIONS: the factors that affect the maternal perception of security at postpartum are cohabitation with a partner, parity, monitored pregnancy, childbirth experience and infant feeding. Defining which factors interfere with maternal security at postpartum may contribute to the construction of intervention programs that promote the maternal perception of security at the time of hospital discharge after delivery.
Keywords:
Parenting, Postpartum period, Mothers, Nurse midwives, Perception security
RESUMO
OBJETIVOS: identificar os fatores que interferem na percepção de segurança materna no pós-parto.
MÉTODOS: estudo transversal, realizado em três unidades hospitalares portuguesas, com uma amostra não probabilística de 352 puérperas recrutadas nos serviços de internamento, no dia da alta hospitalar após o parto. As caraterísticas sociodemográficas e obstétricas maternas, assim como os dados relativos aos cuidados pré-natais, ao parto e ao tipo de aleitamento, foram recolhidos através da aplicação de um questionário desenvolvido pelas investigadoras. Para a análise da percepção de segurança materna foi usado o instrumento "Parents' Postnatal Sense of Security" (PPSS). Foi utilizada estatística descritiva e inferencial para a análise de dados.
RESULTADOS: as mulheres que viviam com o companheiro [t (349) = - 2,34, p=0,020], as multíparas (t (349) = - 2,26, p=0,025), as que vigiaram a gravidez [t (349) = -3,25, p=0,001], as que tiveram uma experiência de parto positiva [F (1, 351) = 7,07, p=0,008] e as que amamentaram em exclusivo durante o internamento [F (2, 351) = 11,43, p<0,001], apresentaram maior percepção de segurança no pós-parto.
CONCLUSÕES: os fatores que interferem na percepção de segurança materna no pós-parto são a coabitação com o companheiro, a paridade, a vigilância da gravidez, a experiência de parto e o tipo de aleitamento. Determinar os fatores que interferem com a segurança materna no pós-parto pode contribuir para a construção de programas de intervenção promotores da percepção de segurança materna no momento da alta hospitalar após o parto.
Palavras-chave:
Parentalidade, Período pós-parto, Mães, Enfermeiras obstétricas, Percepção de segurança
IntroductionSecurity, considered as a basic human need, is influenced by individual experiences and the ability to act, and is an essential component of quality of life.
1,2In addition to dealing with illness and health promotion, modern nursing has developed theories to deal with human demands. In this context, the Theory of Transitions has emerged, which studies the individual themselves and their environment in moments of instability, often fraught with feelings of insecurity, as it is characterized as the transition to parenthood, it is due to new responsibilities.
3-5Becoming a mother has been described as one of the most challenging transitions in a human being's life, with changes on a personal, family and social level.
1 The instability generated by this new life cycle can be accompanied by insecurity
1,6 and for this reason it is important to ensure the well-being of both mother and child.
7 Ramona Mercer, in her
Teoria da Consecução do Papel Materno (Maternal Role Achievement Theory), emphasizes the construction of maternal identity as an evolutionary process, through which the acquisition of skills guarantees mastery and security in the performance of the role.
8After childbirth, early hospital discharge has become an increasingly common global practice, generating debate about its advantages and disadvantages.
9 This new reality needs more research to support its practice and to enable professionals to prepare women to return home more effectively.
10,11 However, regardless of the length of hospital stay, which in Portugal is usually 48 hours for a vaginal birth and 72 hours for a cesarean section, it is important to empower mothers so that they feel capable and safe when they return home.
Encouraging the acquisition and development of skills that give power and control in the newborn's care increases the security in the role played, which means that autonomy is directly related to maternal security at postpartum.
1,6,12 This type of knowledge about the perception of security makes it possible to develop care strategies aimed at the mothers' real needs but it is still little studied, which points to the necessity for further research.
13 For this reason, we used the "Parents' Postnatal Sense of Security" (PPSS) instrument, which assesses the perception of maternal security in the first week postpartum.
7Health professionals, nurses midwives, need to understand the factors that condition maternal perception of security in this period in order to promote a transition to positive parenting.
14 The aim of this study was therefore to identify the factors that interfere with maternal perception of security at postpartum.
MethodsThis cross-sectional study consisted of a sample of 352 puerperal women admitted to the puerperium service on the day of discharge. The inclusion criteria were: understanding and speaking Portugal Portuguese, being over 18 years old and having been co-housed with the newborn during hospitalization after childbirth. The exclusion criteria were multiple pregnancies, premature birth and health problems requiring hospitalization in intermediate or intensive care units during pregnancy, childbirth or the puerperium.
The non-probabilistic sample for this study was reached by contacting 395 puerperal women, but after checking the eligibility criteria only 365 were eligible and of these 352 women agreed to participate.
Data collection was carried out between January and June 2018 in three hospitals in North of Portugal:
Centro Hospitalar Universitário do São João (CHUSJ),
Centro Hospitalar Universitário do Porto (CHUP) and
Unidade Local de Saúde do Alto Minho (ULSAM). On the day of the discharge from the hospital after giving birth, the participants who had signed the informed consent form filled in the questionnaire in private, without any outside interference, and were handed out personally by the researcher, who gave a brief introduction to the research and the data collection instrument.
The data collection instrument used was a self-report questionnaire made up in two parts, one with questions about sociodemographic characteristics (i.e. age, area of residence, cohabitation with partner, schooling qualifications and employment), obstetrics (i.e. type of conception and parity), prenatal care (i.e. monitored pregnancy and antenatal classes), childbirth (i.e. type of delivery, skin-to-skin contact, childbirth experience and days of hospitalization) and type of breastfeeding (i.e. breastfeeding in the first hour of life and type of breastfeeding during hospitalization).
In the second part, the Parent's Postnatal Sense of Security (PPSS) instrument was used to analyze maternal perception of security at postpartum.
7 The PPSS assesses the perception of security of both fathers and mothers during the first week after the birth of their child.
9This instrument consists of 18 items in the maternal version, assessed on a four-point Likert scale. A total score ranging from 18 to 72 can be obtained, with higher scores meaning higher levels of maternal perception of security at postpartum. It consists of four important dimensions for maternal perception of security at postpartum: Dimension I - Empowerment of parental behavior by the nurse midwives, which includes items 1, 2, 3, 4, 5 and 6; Dimension II - Feeling of general well-being, made up of items 7, 8, 9, 10 and 11; Dimension III - Feeling of affinity in the family, with items 12, 13, 14 and 15. Finally, Dimension IV - Breastfeeding, includes items 16, 17 and 18.
The PPSS was translated and adapted for the Portuguese population and showed very similar results to the original versions in terms of reliability and validity.
6 In the reliability study, the internal consistency analysis revealed Cronbach's alpha values of 0.79 for the maternal version
6 and in the present study, the value obtained was 0.801. Methodologically, we opted for an instrument already used in various international contexts and which had been translated and adapted to the Portuguese reality, since this approach allows us to compare results between the scientific community. We chose to use only the PPSS, since the four dimensions behaved in a general way like the total scale. The study was carried out in three Portuguese hospital units and, as there were no differences between the groups related to the place of data collection, it was therefore considered a single group.
Descriptive analysis was used to present the information on the variables included in each of the groups under analysis (sociodemographic, obstetric, prenatal care, childbirth and infant feeding).
Firstly, t-tests were used to analyze the dichotomous variables, namely: age (≤35/˃35), area of residence (urban/rural), cohabitation with a partner (yes/no), schooling qualifications (basic: ≤12 years/higher education: ˃12 years), employment relationship (employed/unemployed), type of conception (spontaneous/medically assisted reproduction), parity (primiparous/multiparous), monitored pregnancy (monitored/not monitored), antenatal classes (attended/not attended), type of delivery (vaginal/cesarean), skin-to-skin contact after birth (yes/no), childbirth experience (positive/negative), number of days in hospital after delivery (2/≥3) and breastfeeding in the first hour of the newborn's life (yes/no). Analysis of variance (ANOVA) was applied to the non-dichotomous variables (type of breastfeeding during hospitalization - exclusive breastfeeding/breastfeeding+artificial milk/artificial milk).
Once the univariate analysis had been completed, in the groups (sociodemographic, obstetric, prenatal care, childbirth and breastfeeding) where there was more than one variable with statistical significance, a multivariate ANOVA model was used to control these variables within each group. In this way, the relationship between them regarding to maternal self-perception of security at postpartum will be clear. The Bonferroni post-hoc test was used after the analysis of variance.
The level of statistical significance was set at 0.05. Statistical analysis was carried out using SPSS for Windows version 27.
The study was approved by the ethics committees (Opinion no. 31-18 - CES of CHUSJ; Opinion no. 04/2018 of the CES of CHUP and 036-DEFI/036-CES of ULSAM).
ResultsTable 1 shows the participants' ages ranged from 18 to 46, with an average of 31.22 years (SD=5.26). Most of the women were aged 35 or under (78.0%, n=273), had a basic level of schooling (60.2%, n=212), lived in an urban area (65.6%, n=231), lived with a partner (88.9%, n=313), were employed (86.9% n=299), became pregnant spontaneously (93.7%, n=329), were primiparous (50.9%, n=179), monitored their pregnancy (84.7%, n=298), were prepared for parenthood (68.9%, n=241), had a vaginal birth (71.6%, n=252), had a positive birth experience (86.4%, n=304), had skin-to-skin contact with the newborn immediately after birth (77.0%, n=271), was hospitalized for 3 or more days after birth (55.4%, n=195), breastfed during the first hour of the newborn's life (73.30%, n=258) and breastfed exclusively during hospitalization (79.8%, n=281).
The average PPSS score in this sample was 58.45 (SD = 6.90), ranging from 36 to 72.
The average scores for the four dimensions of the PPSS in this sample were: I - 21.63 (SD=3.11); II - 11.95 (SD=3.20); III - 15.05 (SD=2.02) and IV - 9.82 (SD=10.44). Cronbach's alpha values were 0.860; 0.587; 0.879; 0.730, respectively for each of the dimensions.
Regarding to maternal perception of security at postpartum, there were significant differences between women who lived with their partner and those who did not [t(349) = - 2.34,
p=0.020], with those who lived with their partner had higher scores on the perception of security at postpartum. None of the other sociodemographic variables in this group were statistically significant.
In relation to the group of obstetric variables, there were significant differences according to parity [t(349) = - 2.26,
p=0.025], with multiparous women had higher scores on the perception of security at postpartum. The other variables were not statistically significant.
Regards to the group of prenatal care variables, there were significant differences between women who monitored and those who did not [t(349) = -3.25,
p=0.001], with those who monitored had higher scores on the perception of security at postpartum. The other variables were not statistically significant.
In the group of variables related to childbirth, had significant differences in the maternal perception of security between women who had a vaginal birth and those who had a cesarean section [t(349) = 2.68,
p=0.008], between those who had skin-to-skin contact with the newborn and those who had not [t(349) = 3.35,
p<0.001], between those who reported a positive birth experience and those who reported a negative experience [t(349) = 4.39,
p<0.001], between those who were hospitalized for only two days and those who were hospitalized for three or more days [t(349) = 1.98,
p=0.048]. In the group of infant feeding variables, there were significant differences in the maternal perception of security at postpartum between women who breastfed in the first hour of the newborn's life and those who did not [t(349) = 2.51,
p=0.013]; during hospitalization, there were significant differences between women who breastfed exclusively and those who had to supplement feeds with artificial milk [F (2, 348) = 11.87,
p<0.001]. Women who breastfed their newborn in the first hour of life and those who exclusively breastfed during hospitalization had higher scores on perception of security at postpartum.
A multivariate ANOVA model was then applied in situations where more than one significant variable was found within each group: the childbirth group, where only childbirth experience [F (1, 351) = 7.07,
p=0.008] remained statistically significant and the breastfeeding group, where only the type of breastfeeding during hospitalization [F (2, 351) = 11.43,
p<0.001] remained statistically significant.
DiscussionIn this study, the results suggest a number of factors related to maternal feelings of security and rule out others with no statistically significant relationship.
With regard to sociodemographic characteristics, cohabitation with a partner was a significant variable in maternal perception of security at postpartum. The relationship with the child's father is identified as a relevant factor for women and is recognized by them as essential. The importance of the partner's presence and support, not only during pregnancy, but also during labor and delivery, as well as after childbirth, is undeniable,
1,2,15,16 which corroborates the results found in this study. The attitude and participation of the partner throughout pregnancy, including in antenatal classes, can contribute to better management of labor pain and to making this experience a positive life event, with repercussions on the perception of security at postpartum.
1,2,14 In addition, sharing responsibilities, especially in the postpartum period and directed towards childcare, supporting the acquisition of skills is related to the promotion of maternal security.
17Referring the data to obstetric variables, the major findings are related to parity, with multiparous women having a higher perception of security at postpartum. This relationship has already been found in the evaluation of the PPSS by the authors of the instrument themselves, who reinforce that primiparous women experience lower levels of security than more experienced mothers.
2 Becoming a mother is an event that triggers wide-ranging changes, and it is presumable how much more challenging and insecure it can be to experience motherhood for the first time.
Women who monitored their pregnancy had a greater perception of security at postpartum. Some authors state that monitoring pregnancy can be translated into feelings of tranquillity when mother and baby are physically well, which triggers feelings of security in this phase and in subsequent ones, such as childbirth and at postpartum.
1,18 On the other hand, and contrary to other studies, no statistically significant relationship was identified between being prepared for parenthood and the perception of security at postpartum. Preparation for parenthood has become an integral part of pregnancy monitoring in health care in Portugal.
19 Implemented both in primary health care and in private settings, these programs aim to improve care for parents and children based on their individual needs, with the goal of autonomous and positive parenting, where the early empowerment of parents contributes to a healthy transition adapted to the new role.
8Primiparous women, due to the novelty and inexperience of the situation, are the ones who seek out these programs the most, but this intervention may be insufficient since they do not yet feel able to ask questions during pregnancy about what may come up in the post-birth.
20 Factors such as attendance, content, motivation, availability and accessibility of pregnant women may also be considered as conditioning factors for the full enjoyment of the benefits offered by these interventions.
19 Future studies should explore this variable and its influence on maternal security at postpartum, in order to better understand its impact and adjust professional practices accordingly.
Regarding to childbirth data, all the variables initially showed statistical significance in relation to maternal security at postpartum period, but after applying the multivariate model, only childbirth experience remained statistically significant. Women who rated their childbirth experience as positive had higher scores on perception of security at postpartum.
However, it would be important to know what a positive birth experience means. An Investigation in this area has recognized some associations. One of the studies points to women who gave birth vaginally as having a higher perception of security at postpartum.
18 Cesarean section is a surgical procedure that inevitably carries more maternal and perinatal risks when compared to vaginal delivery and, as such, is likely to be associated with higher levels of maternal anxiety and insecurity.
21Other authors also add the first skin-to-skin contact between mother and child as a contributing factor to a positive childbirth experience.
22 Based on the literature, it is reasonable to assume that the women studied in this research, who had a vaginal birth and had skin-to-skin contact, may have translated these experiences into a positive childbirth experience.
In the present study, it was found that the length of hospitalization was irrelevant to the maternal perception of security at postpartum, which raises questions about the support and preparation for discharge, since longer hospitalizations would mean more time for anticipatory care for returning home.
Dichotomous data has emerged from the analysis of the advantages and disadvantages of early discharge. If, on the one hand, it increases maternal and child morbidity and parents' lack of knowledge, on the other hand, it creates opportunities for family-centered care in their environment, constituting a more cost-effective postnatal intervention.
12,20 These dissonances are related to the variable quality of preparation for discharge, which highlights the necessity to deepen assessments and interventions in order to better identify women in need of additional support.
23In regard to the type of infant feeding, research in this area confirms that there is a reciprocal relationship between the maternal perception of security and breastfeeding, influencing each other mutually and positively in terms of adherence to and maintenance of this practice.
1,24 These data are corroborated by our study, in which women who exclusively breastfed had higher levels of security on average.
The encouragement, support and backing of the professionals involved fosters feelings of competence and self-efficacy which, in themselves, also promote confidence and security, which are essential for establishing and maintaining breastfeeding.
20,24,25Limitations were found in this study. After analyzing the variables and their significance, it is suggested that larger-scale studies should be carried out to see if they would translate into different results, as is the case in other similar studies. In addition, special attention should be paid to extrapolating the results to other contexts and considering the inclusion of paternal figures in order to enrich these results in the future.
For clinical practice, the PPSS could be a useful tool to help health professionals during the first care they provide at postpartum, screening women in need of interventions and differentiated support, in order to promote a safe return home and a positive parental transition.
Generally speaking, the maternal perception of security can be influenced by various factors, including cohabitation with a partner, pregnancy monitoring, parity, childbirth experience and type of infant feeding. The results obtained here should be taken into consideration in order to build new interventions to promote maternal security in the contexts explored, especially in the postnatal period, but also in the prenatal period.
Considering security as a basic need throughout pregnancy, childbirth and at postpartum, the permanent search for this feeling becomes a constant that characterizes the whole process.
References1. Werner-Bierwisch T, Pinkert C, Niessen K, Metzing S, Hellmers C. Mothers' and fathers' sense of security in the context of pregnancy, childbirth and the postnatal period: an integrative literature review. BMC Pregnancy Childbirth. 2018 Dec; 18(1): 473.
2. Persson EK, Dykes AK. Important variables for parents' postnatal sense of security: evaluating a new Swedish instrument (the PPSS instrument). Midwifery. 2009; 25 (4): 449-60.
3. Meleis AI. Transitions Theory Middle-Range and Situation-Specific Theories in Nursing Research and Practice. New York: Springer Publishing Company, LLC; 2010.
4. Barimani M, Vikström A, Rosander M, Forslund Frykedal K, Berlin A. Facilitating and inhibiting factors in transition to parenthood - ways in which health professionals can support parents. Scand J Caring Sci. 2017; 31 (3): 537-46.
5. Silva C, Carneiro M. Pais pela primeira vez: aquisição de competências parentais. Acta Paul Enferm. 2018; 31 (4): 366-73.
6. Pinto C, Martins C, Carneiro M. Tradução e adaptação cultural do Parents' postnatal sense of security (PPSS) – Versão materna e versão paterna. Rev Assoc Port Enf Obst. 2014; 14: 32-6.
7. Persson EK, Fridlund B, Dykes AK. Parents' postnatal sense of security (PPSS): development of the PPSS instrument. Scand J Caring Sci. 2007; 21 (1): 118-25.
8. Mercer RT. First-time motherhood: experiences from teens to forties. New York: Springer; 1986.
9. Persson EK, Dykes AK. Parents' experience of early discharge from hospital after birth in Sweden. Midwifery. 2002; 18 (1): 53‑60.
10. Jones E, Taylor B, MacArthur C, Bradshaw S, Hope L, Cummins C. Early postnatal discharge for infants: a meta-analysis. Pediatrics. 2020 Aug 21; 146 (2): e20193365.
11. World Health Organization (WHO). WHO recommendations on maternal and newborn care for a positive postnatal experience. Geneva: WHO; 2022. [access in 2024 Jan 10]. Available from:
https://iris.who.int/bitstream/handle/10665/352658/9789240045989-eng.pdf?sequence=112. Jones E, Stewart F, Taylor B, Davis PG, Brown SJ. Early postnatal discharge from hospital for healthy mothers and term infants. Cochrane Database Syst Rev. 2021; 6: CD002958.
13. Sirli B, Altuntuğ K. Assessment of postnatal sense of security of primipara mothers and associated factors in Turkey. Afr J Reprod Health. 2023; 27 (5): 41-9.
14. Velagic M, Mahmutovic, J, Brankovic S. Development of Mother's Postnatal Sense of Security. Mater Sociomed. 2019; 31(4): 277-81.
15. Mayers A, Hambidge S, Bryant O, Arden-Close E. Supporting women who develop poor postnatal mental health: what support do fathers receive to support their partner and their own mental health? BMC Pregnancy Childbirth. 2020; 20(1): 359.
16. Abbaspoor Z, Sharifipour F, Javadnoori M, Moghadam ZB, Cheraghian B, Najafian M. Evaluation of the effectiveness of a postnatal support education program for husbands in promotion of their primiparous wives' perceived social support: a randomized controlled trial. BMC Womens Health. 2023; 23 (1): 139.
17. Tu A, Zeng T, Yuan M, Zhang K, Chen Y, Wang X,
et al. Factors Associated with Parents' Postnatal Sense of Security in China: A Cross-sectional Study. Versão 1 [
Preprint]. Res Square. 2021; [access in 2023 Fev 13]. Available from:
https://www.researchsquare.com/article/rs-523065/v118. Koçak V, Persson EK, Svalenius EC, Altuntuğ K, Ege E. What are the factors affecting parents' postnatal sense of security? Eur J Midwifery. 2021; 5: 38.
19. Direção Geral da Saúde (DGS). Cursos de Preparação para o Parto e a Parentalidade (CPPP) e Cursos de Recuperação Pós-Parto (CRPP). Equidade na transição para a maternidade e a paternidade. Lisboa; 2020. [access in 2024 Fev 2]. Available from:
https://www.dgs.pt/documentos-em-discussao-publica/documento-em-audicao-publica-pdf.aspx20. Persson EK, Fridlund B, Kvist LJ, Dykes AK. Mothers' sense of security in the first postnatal week: interview study. J Adv Nurs. 2011; 67 (1): 105-16.
21. Hassan IAS, Hamza LK. Unique Case of a Tenth Cesarean Section in an Emirati Woman. Dubai Med J. 2020; 3 (1): 5-7.
22. Konieczka J, Tomczyk K, Wilczak M, Chmaj-Wierzchowska K. Factors Affecting Women's Assessment and Satisfaction with Their Childbirth. Medicina (Kaunas). 2024 Jan; 60 (1): 86.
23. Harvey CM, Smith H, Portela A, Movsisyan A. Stakeholder's perspectives of postnatal discharge: a qualitative evidence synthesis. BMJ Glob Health. 2023; 8 (Suppl. 2): e011766.
24. Pérez-Escamilla R, Tomori C, Hernández-Cordero S, Baker P, Barros AJD, Bégin F,
et al. Breastfeeding: crucially important, but increasingly challenged in a market-driven world. Lancet. 2023 Feb; 401 (10375): 472-85.
25. Zhu Y, Zhou X, Yin X, Qiu X, Sun N, An R,
et al. Parenting sense of competence and its predictors among primiparous women: a longitudinal study in China. BMC Pregnancy Childbirth. 2022; 22: 548.
Authors' contribution: All the authors contributed to the development of the ideas, conception, design, analysis and interpretation of the data, as well as the writing and final revision of the version submitted.
All the authors have approved the final version of the article and declare no conflicts of interest.
Received on April 20, 2023
Final version presented on February 6, 2024
Approved on February 8, 2024
Associated Editor: Gabriela Sette


 ; Sónia Brandão2
; Sónia Brandão2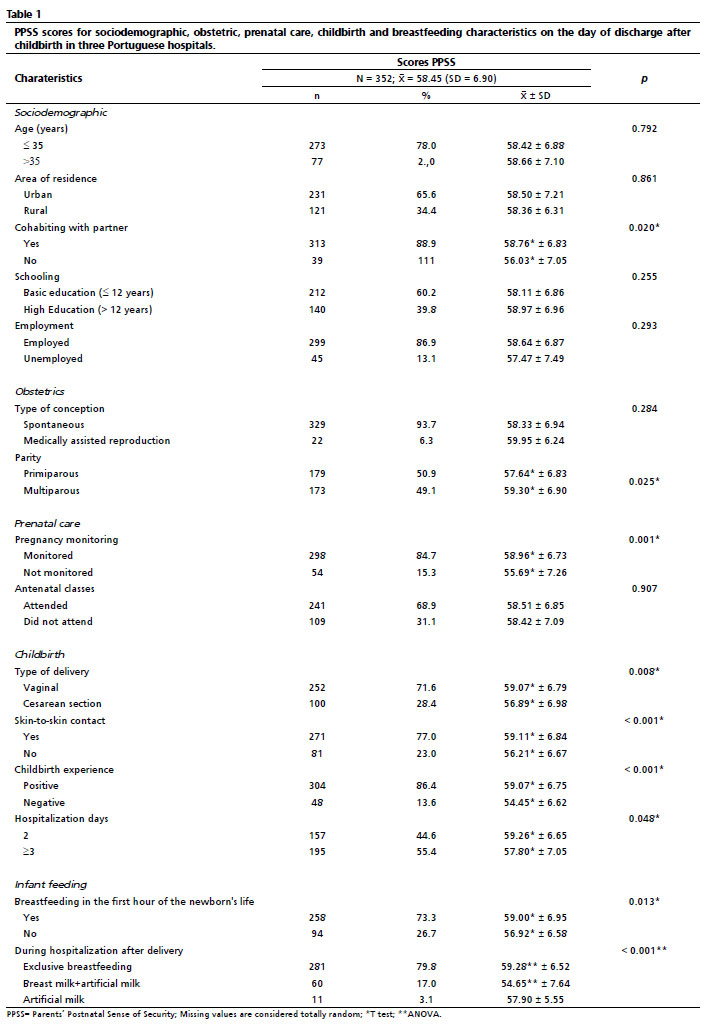






 Ler em português
Ler em português