ABSTRACT
OBJECTIVES: to describe the prevalence of malnutrition (underweight, low height, and overweight) in children aged six to 59 months and its spatial distribution in the city of Beira, Mozambique.
METHODS: an exploratory cross-sectional study was conducted between October and November 2019, involving 407 children aged six to 59 months. The sample size calculation was based on the prevalence of height-for-age deficit. Anthropometric data were analyzed using Anthro version and the prevalence of malnutrition was presented through thematic maps generated in Quantum Geographic Information System (QGIS).
RESULTS: the main findings revealed a prevalence of 27.0% for low height/age, 7.9% for underweight/height, and 4.7% for overweight.
CONCLUSIONS: the spatial distribution highlighted that both urban and peri-urban areas of the city showed similar prevalence rates for the three forms of malnutrition. The prevalence of malnutrition in Beira is high, with deficit height/age being the most significant expression, while overweight is diffusely distributed.
Keywords:
Malnutrition, Obesity, Child, Geographic information systems
RESUMO
OBJETIVOS: descrever a prevalência da má nutrição (baixo peso, baixa estatura e excesso de peso) em crianças de seis a 59 meses e sua distribuição espacial na cidade de Beira, Moçambique.
MÉTODOS: estudo transversal exploratório, realizado entre outubro e novembro de 2019, incluindo 407 crianças de seis a 59 meses. O cálculo da amostra foi baseado na prevalência do déficit estatura/idade. Os dados antropométricos foram analisados no Anthro e a prevalência de má nutrição apresentada por meio de mapas temáticos no Quantum Geographic Information System (QGIS).
RESULTADOS: os principais resultados mostram uma prevalência de 27,0% de baixa estatura/idade, 7,9% de baixo peso/estatura e 4,7% de excesso de peso.
CONCLUSÕES: a distribuição espacial evidenciou que as áreas urbanas e periurbanas da cidade apresentavam prevalências similares das três formas de má nutrição. A prevalência da má nutrição em Beira é alta, embora o déficit estatura/idade seja a sua maior expressão, estando o excesso de peso difusamente distribuído.
Palavras-chave:
Desnutrição, Obesidade, Criança, Sistema de informação geográfica
IntroductionMalnutrition is a global problem, with a greater impact in countries with great social inequalities.
1,2 Its manifestation can occur at a population or individual level through malnutrition, nutritional deficiencies and/or by excess weight.
3 The determinants of malnutrition have complex origins and their reproduction is associated with numerous morbidities throughout the life cycles.
4Evidence indicates that the organism of a malnourished child shows a noticeable reduction in his/her development and in its metabolic actions, when compared to children who receive adequate nutrition.
5 The consequences of malnutrition on child development are numerous, including growth retardation and cognitive impairment.
6Globally, it is estimated that 21.3% of the children under the age of five have low height for age, 5.9% low weight for height (thinness) and 5.6% overweight.
7 In 2019, Africa and Asia had the highest prevalence of malnutrition in children under the age of five, where low height for age was 54.0% and 40.0%, respectively. Weight-for-height deficit was 27.0% in Africa and 69.0% in Asia, while overweight was 24.0% and 45.0%, respectively.
3In 2015, the sub-Saharan African region recorded a prevalence of underweight children under five years of age of over 30%. However, in 2018, despite a global decrease in the rate of child stunting, the sub-Saharan region saw an increase in the number of cases of underweight, rising from 50.3 million to 58.8 million.
8 A longitudinal study carried out between 2008 and 2009 in 11 cities in Southern Africa, including Maputo, the Mozambican capital, reported that the occurrence of food insecurity in urban areas reached 15% of the population and the occurrence of growth deficit malnutrition reached 27% of children under five years old.
9In Mozambique, a sub-Saharan African country located in the Southern Africa region child malnutrition is considered one of the main public health problems up to the first five years of life
3. This scenario has been reported since the first population studies carried out in the country in 1992.
10The cost of hunger study carried out in Mozambique in 2014 showed that around 200,000 children under the age of five had deaths associated with malnutrition, which corresponded to 25.6%.
10 In Sofala province, central region of Mozambique, the weight-for-height deficit in children under the age of five is 7.0% and the height-for-age deficit is 48.0%.
11 This province is located in the city of Beira, below sea level and close to the Mozambique Channel in the Indian Ocean, which makes it vulnerable to floods and cyclones.
12 In March 2019, cyclone IDAI hit, causing a great deal of damage to agricultural fields, social infrastructure, the loss of hundreds of human lives and the worsening of diseases such as diarrhea and cholera, as well as the emergence of others, such as pellagra.
12Given this context, the objective is to describe the prevalence of malnutrition (low weight for height, low height for age and overweight) in children aged six to 59 months and its spatial distribution in the city of Beira, Mozambique, in 2019.
MethodsThis is an exploratory cross-sectional study of the anthropometric profile of children aged six to 59 months, carried out between October and November 2019 in the city of Beira, in the province of Sofala in Mozambique.
The city of Beira has an area of 633 km
2 and a population density of 736.04 inhabitants per km
2. It is divided into five administrative posts: Posto Administrativo Urbano Central; Munhava; Inhamizua; Manga; and Nhangau. These make up sixteen health areas: Munhava, Ponta-Gea, Macurungo, Nhaconjo, Chingussura, Mascarenhas, Marrocanhe, Cerâmica, Matadouro, Chota, Manga Loforte, Chamba, São Lucas, Inhamizua, Posto Militar and Nhangau.
13The administrative posts are located in the urban and peri-urban areas. The urban area is characterized by the existence of roads with access, public transport, easy transit to various social infrastructures. The health areas of Ponta-Gea, Macurungo, São Lucas and Posto Militar are part of the urban area, while the others are part of the peri-urban area,
12 characterized by poor or non-existent urbanization, a lack of means of transport, and a lack of roads with no access and social infrastructure.
According to the 2017 Population Census, the city of Beira had a population of 465,918 inhabitants, with 74,547 children aged between six and 59 months, which corresponds to 16.4% of the Mozambican population.
13To calculate the sample, the height/age index was taken into account, with the highest prevalence of 48.0% described in the population studies carried out between 1992 and 2014 at a provincial level. Compared to the weight/height indicator, which has a lower prevalence (7%).
14 Thus, the sample size for the study on height/age indicator is statistically adequate for the study of the weight/height indicator, since the sample obtained for the study of the first indicator is larger than it would be necessary for the second indicator.
The sample was calculated using the EpiInfo 7 statistical program using the equation for the proportion in an infinite population, with a margin error of 5.0% and a 95% confidence level. Using these references, a sample of 383 children was obtained, with the addition of a margin of 10.0% to take into account possible losses, resulting in a final sample of 421 children aged between six and 59 months.
The sample was drawn proportionally to the population and neighborhoods in each health area. To do this, two draws were made: the first of households; the second, in families with two or more children of eligible age, to select just one child. Each eligible child corresponded to one family and/or caregiver from the eligible households selected per block, counting the households clockwise. In areas where the block was better urbanized (structure and distance between homes), the variation of every fifth house was considered. In non-urbanized blocks (with no access to roads, or no structuring of houses, or with houses very close to each other), the variation of every ten houses was considered.
The final sample obtained in the field was 407 children, distributed as follows by health area: Munhava (68), Ponta-Gea (68), Macurungo (33), Nhaconjo (40), Chingussura (45), Mascarenhas (24), Marrocanhe (9), Cerâmica (10), Matadouro (11), Chota (16), Manga Loforte (25), Chamba (21), São Lucas (10), Inhamizua (16), Posto Militar (11), and the Nhangau health area was not included due to logistical problems.
The anthropometric equipment and interview procedures were pre-tested at the Ponta-Gea Health Center, in the city of Beira, with 46 children aged between six and 59 months. These were not included in the final sample.
Weight measurements were performed by using an AVANUTRI® electronic central tare scale with a maximum capacity of 200 kg and 50g sensitivity. This scale is also suitable for checking weight by weighing the child on the mother's/caregiver's lap using the tare function. In this study, only children under 24 months of age were weighed on their mother's lap. Each child's weight had to be measured twice and without clothing, by anthropometrists who had been trained and qualified by the research coordination team. The final weight in grams was obtained from the average between the two weighings. When the difference between the two weighings was greater than 50g, a third weighing was carried out and the average of the three values was calculated.
Height was measured using a wooden stadiometer with a 1mm reguluation and a maximum capacity of 150cm. Length was assessed in the supine position for children up to 24 months of age and the other children were assessed in the orthostatic position. Height was measured twice and the average of the two measurements was performed as the final value.
14,15 When the difference between the two measurements was greater than 2.5cm, a third measurement was performed and the average of the three measurements was calculated.
The anthropometric data was analyzed using the Anthro program version 3.2.2, which is used by WHO to assess the growth and development of children up to the age of five.
15Low height for age (height deficit) was assessed using the height/age index and classified when the z-score was <-2. Underweight and overweight were assessed using the weight/height index, with a cut-off point of z-score ≤-2 and z-score ≥+2, respectively.
15To assess the distribution of the prevalence of malnutrition indicators, the database was exported to the Statistical Package for the Social Sciences (SPSS) program, version 21, using which frequency distribution tables were built and the chi-square test was applied to compare proportions. All conclusions were drawn considering a significance level of 5.0%.
The prevalence of malnutrition found was described according to spatial location in the city of Beira, using the Quantum Geographic Information System (QGIS) program, version 3.10.0, a geographic information system (GIS) built on free and open source software used to create the cartographic maps. To build the maps, we used the cartographic base of the city of Beira, in shapefile format, in the geographic projection system (latitude/longitude) and in the WGS-84 geodetic reference system, collected from the website of the
Instituto Nacional de Estatística (INE) (National Statistics Institute) of the Mozambican government.
To visualize and understand the dynamics of spatial distribution, thematic maps were generated using the spatial method for generating continuous surfaces called
Ponderação pelo Inverso da Distância (IDW) (Inverse Distance Weighting). This type of interpolated surface is often called a statistical surface.
16 After the maps were made, descriptive and exploratory data analysis was carried out to describe the distribution of the study variables, atypical observations of the type of distribution, and patterns in spatial distribution.
The study was approved by the Research Ethics Committee of IAM/Fiocruz and by the
Comissão Nacional de Ética em Pesquisa do Ministério da Saúde do Brasil (National Research Ethics Commission of the Brazilian Ministry of Health) under the reference CAAE 13744519.3.0000.5190. It was also approved by the
Comitê Nacional de Bioética para Saúde do Ministério da Saúde de Moçambique (National Bioethics Committee for Health of the Ministry of Health of Mozambique) under the reference number 476/CNBS/19.
ResultsTable 1 shows that of the 407 children who took part in the study, 139 (34.2%) lived in urban areas and 268 (65.8%) lived in peri-urban areas. Most were between the ages of 24 and 56 months (n=220; 56.6%), followed by 12 to 23 months (n=112; 25.1%) and six to 11 months (n=75; 18.3%). Most of the children were female (n=209; 51.4%) and many of the children were cared for by their biological mothers (n=337; 82.8%).
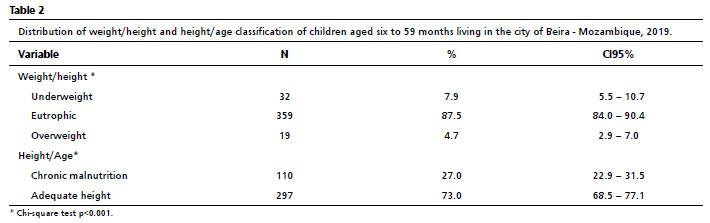
Table 2 shows the analysis of weight/height and height/age. The weight/height index showed that 7.9% of children aged between six and 59 months were underweight, 87.5% were normal weight and 4.7% were overweight. Analysis of the height/age index showed that 27.0% of the children were chronically malnourished and 73.0% had adequate height.
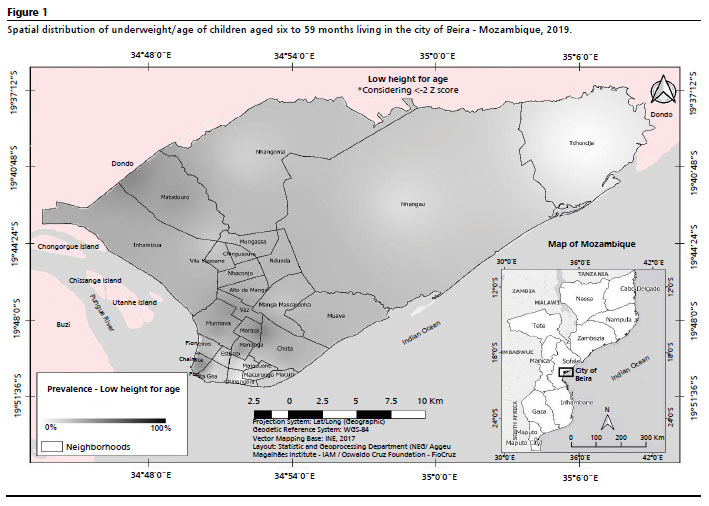
Figure 1 shows that the more urban parts of the city have a low prevalence of height deficit, with the exception of Chaimite neighborhood, which belongs to the Ponta-Gea health area. In the central part of the city and in the peri-urban areas, there is a moderate increase in the prevalence of low height/age, particularly in the neighborhoods of Munhava, Mananga and Maraza, all belonging to Munhava health area. It is worth noting that the lowest prevalence of stunting is observed in the most peripheral areas, located in the North of the city.
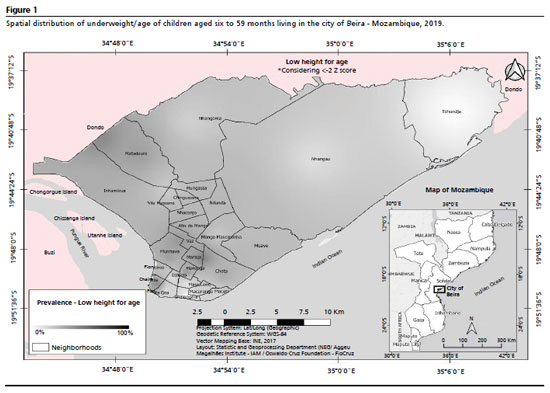
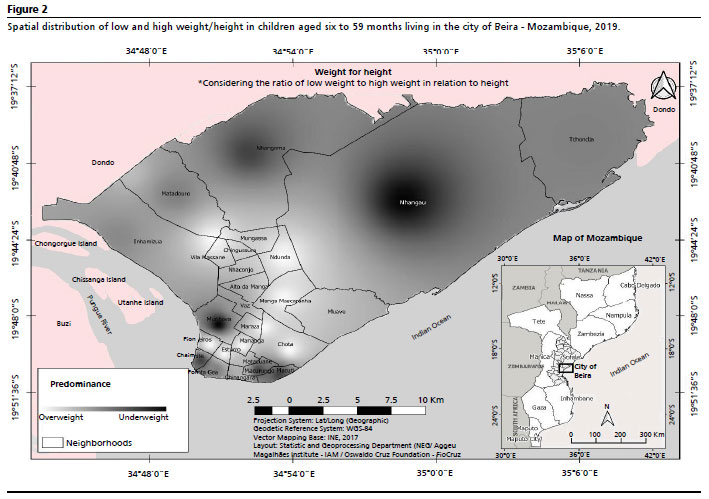
Figure 2 shows that there is a prevalence of overweight and underweight in both urban and peri-urban areas. In general, the distribution of underweight is mostly located in urban neighborhoods such as Chaimite and Macute (Ponta-Gea health area), Macurungo (Macurungo health area) and Matacuane (Posto Militar health area). In the peri-urban area, there is a high prevalence of underweight in the neighborhoods of Munhava (Munhava health area), Nhangoma and Nhangau (Matadouro health area). Overweight is observed in the urban areas of Pioneiro and Esturro (belonging to the Ponta-Gea health area) and the peri-urban areas of Mananga and Maraza (belonging to Munhava health area), Chota (Chota health center area), Bairro Manga Mascarenha (Mascarenhas health center), Ndunda (Ndunda health center area) and the Chingussura neighborhood (Chingussura health center).
DiscussionLow height deficit in the city of Beira affects 27% of children aged between six and 59 months. The prevalence of underweight and overweight showed no statistical difference and both conditions are present in urban and peri-urban areas. However, overweight is concentrated in the areas closest to the urban center.
Some studies carried out in using the same age group in urban areas of Mozambique found prevalence rates of 3.8%, 5.2% and 6.4%;
11,14 the study in the urban village of Bandja in Cameroon found a low prevalence of underweight (5.2%),
17 with prevalence rates lower than those found in this study in Beira (7.9%). However, a study carried out in an urban area of Khartoum in Sudan found that underweight affected 15.4% of the children,
18 while other studies have found a proportional increase in underweight prevalence rates as in further urban areas.
4,19The results of an integrative review, based on national surveys from 26 countries, showed that rural areas had a higher prevalence of all forms of malnutrition compared to urban areas.
19 In Brazil, a population-based study of children under five years old, observed that the causal factors for the prevalence of child malnutrition are more present in rural areas and in populations with low socioeconomical power.
20 However, a study conducted in eight cities in Southern Africa indicated that the acceleration of urbanization in this region is not having a significant impact on the reduction in the prevalence of malnutrition and urban food insecurity.
9 The results of the present study demonstrate the homogeneity in the occurrence of weight deficit in urban and peri-urban areas.
In this study, height deficit was lower than that found in Mozambique in 2014-15 (35.1%),
21 and remaining as a public health problem. In a 16-year interval, the height deficit in Mozambique increased 7.8% between 1997 (27.3%) and 2015 (35.1%).
21 The high prevalence of height deficit was also found in other African cities such as Khartoum, the capital of Sudan, with 24.9%,
18 as well as in an urban settlement in Nairobi (Kenya), where the prevalence was 47.0%.
22 Several studies have highlighted that the reduction in the prevalence of malnutrition is associated with a variety of factors, including changes in social policies, urbanization, educational levels, environmental sanitation, access to health services and improvements in family income.
3,23,24When analyzing the occurrence of overweight, we verified a lower prevalence when compared to the indicators of malnutrition in the city of Beira, although it is more widespread geographically. However, other studies have found higher prevalence rates, for example in the province of Nampula, in the North of Mozambique, where 13% of the children aged between zero and 24 months were overweight,
24 and in a population survey in Mozambique (2008) whose prevalence was 5.0% in children under five in urban areas.
25 In a Unicef report, the prevalence was 7.5% in Mozambican children, reaching 8.7% in urban areas.
26 These findings highlight the complexity of nutritional dynamics and the necessity to consider specific contexts when formulating public health strategies.
A study of children under five years old in a semi-rural area of the "Western Cape" in South Africa found a prevalence of overweight of 26% and a prevalence of low height of 14%, thus demonstrating that overweight and malnutrition coexist in the same geographical space.
27 Therefore, a study carried out in Asia states that it is not possible to create the linear concept that malnutrition is a prevalent problem in poor and rural populations and overweight is commonly associated with wealthy and urban populations, since overweight is also present in children living in remote and poorer areas, as is malnutrition in children living in urban areas.
28 In this sense, the city of Beira has already registered the coexistence of malnutrition and overweight, although the prevalence of malnutrition is higher.
Childhood obesity is currently one of the main public health concerns, given its rising prevalence and its far-reaching implications for physical, mental, social and economic health.
29 Although the city of Beira has a lower prevalence of overweight, the problems associated with it demand attention on the public health agenda, considering the global context marked by rapid food and nutrition transition.
30The different forms of malnutrition have historically been studied around the world, considering different geographical spaces and social strata, in relation to the dynamics of its exposure to different risk factors.
3 One study states that its occurrence may be associated with the impact of the globalization of contemporary food systems, which produce and offer high-calorie, low-cost and ultra-processed food, especially to the poorest populations.
29It is worth noting that the city of Beira has been the scene of various impacts resulting from climate change, often plagued by floods, droughts and cyclones, such as cyclone IDAI, which occurred in March, 2019. This cyclone was considered one of the largest in the Southern hemisphere in the last ten years. These climatic disasters have had a significant impact on the economy of the country, especially in the cities most prone to these phenomena.
12 Environmental issues associated with social injustices affect food systems and health and can exacerbate inequalities in the nutritional profiles of populations, with a greater impact in poorer countries.
30The limitations in this study include the fact that it did not cover the rural area and one of the health areas in the city of Beira, due to operational and logistical aspects. On the other hand, the potential of the study is that the results obtained are unprecedented and contribute to understanding the impacts of different forms of malnutrition on the local population, given that the sample was representative of the city of Beira. Furthermore, the data collection took place after the occurrence of cyclone IDAI, which ratifies the importance of this study as a milestone for monitoring this scenario.
In view of the above, it can be concluded that malnutrition in all its forms (undernutrition and overweight) is a public health problem in the city of Beira. Thus, the results achieved can help the health authorities in Mozambique, the provincial government and the city government to redefine public policies that contribute in reducing economic, social and health inequalities to promote food and nutritional security in Beira.
References1. Castro IRR. Obesidade: urge fazer avançar políticas públicas para prevenção e controle. [Editorial]. Cad Saúde Pública. 2017; 33 (7): 1-3.
2. Longhi LA. The Decade of Action for Nutrition: commitments, challenges and the health strengthening in the agenda of food and nutrition security. In: Health and Foreign Policy: 20 years of the International Health Affairs Office of the Ministry of Health of Brazil (1998-2018). São Paulo: Ministério da Saúde; 2019. p.337-49. [access in 2022 Dez 5]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/health_foreign_policy_20_years_aisa.pdf3. Fundo das Nações Unidas para a Infância (UNICEF). Situação Mundial da Infância 2019. Crianças, alimentação e nutrição: crescendo saudável em um mundo em transformação. [
Internet]. UNICEF; 2019. [access in 2022 Dez 5]. Available from:
https://www.unicef.org/brazil/media/5576/file/SOWC2019_Informacoes_America_Latina_Caribe.pdf4. Lopes AF, Frota MTBA, Leone C, Szarfarc SC. Nutrition profile of children in Maranhão state. Rev Bras Epidemiol. 2019; 22: e190008.
5. Daryanani CP, Kohen B, Manik EGW Br, Nahak JGUn. The impact of childhood malnutrition: a case report. Med Clin Update. 2023; 2 (1): 40-3.
6. Mkhize M, Sibanda M. A review of selected studies on the factors associated with the nutrition status of children under the age of five years in South Africa. Int J Environ Res Public Health. 2020; 17 (21): 7973.
7. Fundo das Nações Unidas para a Infância (UNICEF); World Health Organization (WHO); World Bank Group. Levels and trends in child malnutrition: UNICEF/WHO/World Bank Group joint child malnutrition estimates key findings of the 2020 edition. Geneva: WHO; 2020. [access in 2022 Dez 5]. Available from:
https://www.who.int/publications/i/item/97892400035768. Obasohan PE, Walters SJ, Jacques R, Khatab K. Risk factors associated with malnutrition among children under-five years in sub-saharan african countries: a scoping review. Int J Environ Res Public Health. 2020; 17 (23): 8782.
9. Frayne B, Crush J, McLachlan M. Urbanization, nutrition and development in Southern African cities. Food Secur. 2014; 6: 101-12.
10. União Africana e Programa Mundial de Alimentação. Relatório continental sobre o custo da fome em África (COHA): Impacto Social Econômico da subnutrição infantil; 2012. [access in 2022 Dez 5]. Available from:
https://au.int/sites/default/files/documents/41660-doc-COHA_CONTINENTAL_REPORTPortuguese2021.pdf11. Ministério da Saúde (MOZ). Plano de Acção Multissectorial para a Redução da Desnutrição Crónica em Moçambique 2011 – 2014. Maputo: Ministério da Saúde; 2010. [access in 2022 Dez 5]. Available from:
https://www.pastoraldacrianca.org.br/museudavida/images/exposicoes/PAMRDC_Portugues_FINALsmall-1.pdf12. Ministério da Administração Estatal (MOZ). Instituto Nacional de Gestão de Calamidades (MOZ). Relatório Final Pós a Passagem do Ciclone Idai, Março de 2019. Beira: Ministério da Administração Estatal; 2019. [access in 2022 Dez 5]. Available from:
https://macua.blogs.com/files/relatorio-ciclone-idai-1.pdf13. Instituto Nacional de Estatística (MOZ). IV Recenciamento Geral da população e Habitação 2017. Maputo: INE; 2019. [access in 2022 Dez 5]. Available from:
https://macua.blogs.com/files/censo2017.pdf14. Ministério da Agricultura (MOZ). Secretariado Técnico de Segurança Alimentar e Nutricional (SETSAN). Relatório do estudo de base de segurança alimentar e nutricional 2013. Maputo: Ministério da Agricultura; 2014. [access in 2022 Dez 5]. Available from:
https://www.setsan.gov.mz/wp-content/uploads/2016/09/BaseLine_2013_mocambique.pdf15. World Health Organization (WHO). Department of Nutrition for Health and Development. WHO Child growth standard: length/height-for-age, weight-for-age, weiht-for-length, weight-for height and body mass index-for-age: method sand development. France: WHO; 2006. [access in 2022 Dez 5]. Available from:
https://www.who.int/publications/i/item/924154693X16. Jacob AAE, Young AF. O uso de métodos de interpolação espacial de dados nas análises sociodemográficas. In: XV Encontro Nacional de Estudos Populacionais – desafios e oportunidades do crescimento zero. Vol.15, pp.1-22 Caxambu, MG, Brasil; 2006. [access in 2021 Set 22]. Available from:
http://www.pgea.ufrpe.br/sites/ww3.pgea.ufrpe.br/files/documentos/diegoaraujo_-_dissertacao.pdf17. Nzefa LD, Monebenimp F, Äng C. Undernutrition among children under five in the Bandja village of Cameroon, Africa. South African J Clin Nutr. 2019; 32 (2): 46-50.
18. Taha HM, Musa HH, Ali EA, Musa NE. Prevalence of malnutrition among children under five years old in Khartoum State, Sudan. Polish Ann Med. 2014; 21: 1-7.
19. Pereira TC, Carneiro YVA, Lima LR, Cavalcante EGR, Duavy SMP, Damasceno SS,
et al. Nutritional status of children living in rural communities: an integrative literature review. Res Soc Dev. 2022; 11 (1): e53011125276.
20. Miglioli TC, Fonseca VM, Gomes Jr SC, Silva KS, Lira PIC, Batista Filho M. Factors associated with the nutritional status of children less than 5 years of age. Rev Saúde Pública. 2015; 49: 59.
21. Instituto Nacional de Estatística - INE (MOZ). Direcção de Estatísticas Demográficas, Vitais e Sociais. Relatório Final do Inquérito ao Orçamento Familiar – IOF 2014/15. Maputo: INE; 2015. [access in 2021 Set 22]. Available from:
https://www5.open.ac.uk/technology/mozambique/sites/www.open.ac.uk.technology.mozambique/
files/files/IOF_2014_15_Relatorio_2015_FINAL_24-05-2016.pdf22. Olack B, Burke H, Cosmas L, Bamrah S, Dooling K, Feikin DR,
et al. Nutritional status of under-five children living in an informal urban settlement in Nairobi, Kenya. J Health Popul Nutr. 2011 Aug; 29 (4): 357-63.
23. International Food Policy Research Institute (IFPRI). Relatório sobre a Nutrição Mundial 2016. Da Promessa ao impacto: Erradicar a má nutrição até 2030. Washington (DC): IFPRI; 2016. [access in 2021 Set 22]. Available from:
https://globalnutritionreport.org/documents/11/Portugese_full_report.pdf24. Erlito D. Avaliação do estado de nutrição e dos hábitos alimentares no 1 ano de vida de crianças dos 0 aos 24 meses da província de Nampula, Moçambique (dissertação). Porto: Universidade de Porto; 2014.
25. Instituto Nacional de Estatística – INE (MOZ). Inquérito de indicadores múltiplos (MICS) 2008. Moçambique: INE, 2008. [access in 2020 Out 10]. Available from:
https://mics-surveys-prod.s3.amazonaws.com/MICS3/Eastern%20and%20Southern%20Africa/
Mozambique/2008/Final/Mozambique%202008%20MICS_Portuguese.pdf26. UNICEF, WHO, WORLD BANK GROUP. Mozambique country overview, malnutrition burden; 2019. [access in 2020 Out 10]. Available from:
https://www.unicef.org/media/90401/file/Republic-of-Mozambique-2019-COAR.pdf27. Loots R, Yan B, Vember H. Factors Associated with Malnutrition among Children Aged Six Months to Five Years in a Semi-Rural Area of the Western Cape, South Africa. Child Care Practice. 2022; 28 (4): 625-38.
28. Baker P, Friel S. Processed foods and the nutrition transition: evidence from Asia. Obes Rev. 2014; 15 (7): 564-77.
29. Mendenhall E, Singer M. The global syndemic of obesity, undernutrition, and climate change. Lancet. 2019 Feb; 393 (10173): 741.
30. World Health Organization (WHO). The 2020 global nutrition report in the context of COVID-19; 2020. [access in 2022 Out 15]. Available from:
https://globalnutritionreport.org/43147fAuthors' contribution: Culpa MJ: conception and design of the study, literature review, data analysis and writing of the article. Oliveira e Silva D and Cesse EAP: data acquisition, critical review of the manuscript and approval of the final version. Souza NP: data analysis and critical revision of the article. Silva Santos AH: data analysis and design. Oliveira ALS: spatial analysis. All the authors have approved the final version of the article and declare no conflict of interest.
Received on January 25, 2023
Final version presented on December 4, 2023
Approved on December 5, 2023
Associated Editor: Lygia Vanderlei


 ; Denise Oliveira e Silva2
; Denise Oliveira e Silva2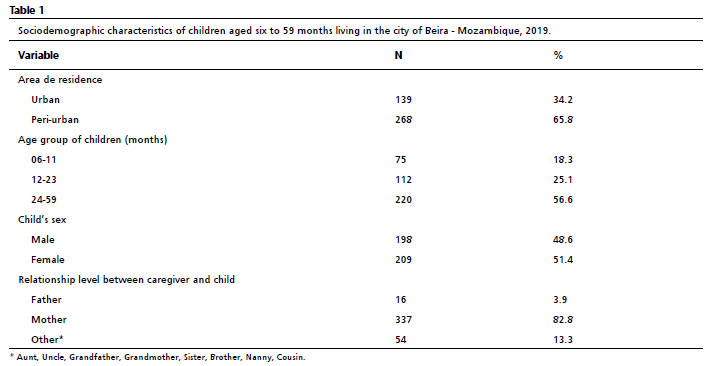






 Ler em português
Ler em português