ABSTRACT
OBJETIVOS: identificar las condiciones sociodemográficas de la comunidad y determinar la prevalencia del estado nutricional de niños menores de seis años en el Resguardo Indígena Nasa Paéz, Rionegro-Huila, Colombia.
MÉTODOS: estudio descriptivo transversal cuyos datos se obtuvieron de dos bases de datos, una de las condiciones sociodemográficas y otra de medidas antropométricas de niños menores de seis años. La muestra correspondió a la totalidad población menor seis años. Los datos se analizaron mediante estadística descriptiva utilizando el software R Studio 3.4.
RESULTADOS: el 98,6% de la población está inscrito en el sistema de salud. El consumo de agua proviene en un 71,6% de fuentes no potables. El 25,5% de la población tiene acceso a sistemas de eliminación de aguas residuales. En cuanto al estado nutricional, la prevalencia de retraso en el crecimiento y riesgo de retraso en el crecimiento es del 43,3% en la población menor de seis meses y del 69,4% en edad entre los seis meses a seis años. Además, el 34,3% de los niños menores de seis meses estaban en riesgo de tener sobrepeso.
CONCLUSIONES: las condiciones sociodemográficas están determinadas por diferentes inequidades, bajos niveles de educación, vivienda inadecuada, consumo de agua no potable, así como por una alta prevalencia de malnutrición infantil.
Keywords:
Pueblos indígenas, Estado nutricional, Niño, Factores culturales, Factores socioeconómicos
RESUMO
OBJECTIVES: identify the sociodemographic conditions of the community and determine the prevalence of the nutritional status of children under six years of age in the Nasa Paéz Indigenous Reserve, Rionegro-Huila, Colombia.
METHODS: cross-sectional descriptive study whose data was obtained from two databases, one of sociodemographic conditions and other anthropometric measurements of children under six years of age. The sample corresponded to the total population of less than six years. The data was analyzed using descriptive statistics using the R Studio 3.4 software.
RESULTS: 98.6% of the population is enrolled in the health system. Water consumption comes from 71.6% of non-potable sources. 25.5% of the population has access to wastewater disposal systems. Regarding nutritional status, the prevalence of delay in growth and risk of delay in growth is 43.3% in the population under six months and 69.4% in those aged between six months and six years. Furthermore, 34.3% of children under six months of age are at risk of being overweight.
CONCLUSIONS: sociodemographic conditions are determined by different inequities, low education levels, inadequate housing, drinking water consumption, as well as a high prevalence of child malnutrition.
Palavras-chave:
Indigenous peoples, Nutritional condition, Child, Cultural factors, Socioeconomic factors
IntroductionIn Latin America, the indigenous population represents 7.8% of the total population. Countries such as Mexico, Peru, Brazil, Guatemala and Bolivia represent just over 80% of the indigenous population.
1 In these countries, indigenous communities show indicators of inequality and a higher prevalence of malnutrition and malnutrition in children under six years of age compared to the non-indigenous population.
2 International organizations that recognize health as a fundamental issue for the well-being of indigenous peoples around the world have pointed out such inequalities,
3 highlighting the notable disadvantages of these peoples in terms of socioeconomic and health indicators.
4In Colombia, indigenous peoples make up 13.6% of the total population, according to the 2018 census.
5 At the same time, they represent ethnic minorities and a priority for development and public health plans due to the vulnerability and social and historical inequality of this population.
6 Proof of this situation is that four of the five Colombian departments with the highest prevalence of poverty are also the departments with the largest indigenous or Afro-descendant population: Chocó, Cauca, Córdoba, Guajira and Magdalena.
6 This scenario is related to negative indicators on food, nutrition and hunger, which have led to international and national food security and sovereignty policies, such as the Sustainable Development Goals 2015-2030.
7The 2015 National Survey of the Nutritional Situation (ENSIN) showed alarming nutritional indicators in Colombia. In 2015, the prevalence of stunting among indigenous children under the age of six was 29.6 per cent, which was considerably high compared to 10 per cent among children under the age of six with no ethnic affiliation.
8 Underweight (low weight-for-age) among children under six years of age had a prevalence of 7.2% in indigenous children compared to 3% in the general population; These figures are consistent with the report that high food insecurity is present in 77 per cent of indigenous households compared to 52.3 per cent of households in the general population.
9A review of figures on the food and nutrition situation in the Colombian department of Huila in 2014 showed a prevalence of stunting in children under five years of age of 11.7%, below the national average of 12.6%.
10 However, this indicator was higher among indigenous children under six years of age in the department of Huila, reaching 38.4% (sample of the municipalities of Íquira, La Plata and La Argentina).
10In contrast, children under six years of age from the Nasa Huila Indigenous Reserve, located in the department of Huila, Municipality of Iquira, urban area of Rionegro, had a prevalence of stunting of 39.7% in 2019,11an indicator higher than the 8.4% in the municipality of Íquira and 38.4% in the department of Huila in 2014.
11 It is therefore clear that the food and nutritional status of indigenous children, particularly in the community under study, is worthy of investigation and intervention.
12In the same vein, another problem is directed at food processes, where a change in traditional food systems and practices is reflected as a result of the application of agricultural techniques that respond to market demands,
13 weakening the opportunities to impart ancestral wisdom and cultural legacies to younger generations.
14 Migration in search of better opportunities has incorporated new knowledge, flavors, and consumption of fast food, delegitimizing ancestral cultures.
15Under these conditions, the objective of this research was to analyze the sociodemographic conditions and nutritional status of children under six years of age in the Nasa Páez Indigenous Reserve, Rionegro-Huila, Colombia.
MethodsA quantitative, descriptive, cross-sectional study was carried out.
16 Conducted using secondary data from the family census and nutritional data for all children under six years of age for the year 2021. The study scenario included the Huila Indigenous Reserve, of the Nasa community, Colombia.
The study population consisted of records of indigenous children of both sexes under six years of age. The sample was taken into account by the entire population. Exclusion criteria were children over six years of age, or records that did not include complete information on the variables of interest. The sociodemographic conditions group the information of the families of the reservation, totaling 2402 data. The nutritional assessment is grouped into children aged 6 months and from 6 months to 6 years, totalling 456 data from children in the reserve. In the age classification, 14.6% (n=67) were less than six months old and 85.3% (n=389) were between six months and six years old.
The first source of data corresponds to the records of sociodemographic, cultural, and housing characteristics of the families in the reservation, collected with an instrument validated by the Institution Providing Indigenous Health Services of the Regional Indigenous Council of Huila (IPSI-CRIHU),
13 which is responsible for collecting this information.
The second source was the nutritional and anthropometric records of the children collected by the
Programa de Modalidad Propio e Intercultural, an educational and comprehensive nutritional care program for Colombian children based on an intercultural and indigenous approach, validated by the Colombian Institute of Family Welfare (ICBF).
11 Anthropometric data on the child population of the community are collected and recorded quarterly by a team of health professionals and entered into the database containing the anthropometric variables of nutritional classification of the World Health Organization (WHO).
17The variables examined were divided into two groups: i) Sociodemographic variables and ii) Variables related to nutritional status. Sociodemographic variables include distribution by sex, type of fuels used for cooking, sources of drinking water, water treatment, disposal of human excreta, disposal of wastewater, ownership of family productive spaces (orchards), type of productive spaces, and housing conditions (wall material, the floor and ceiling). The variables related to nutritional status are those established by the WHO, including height/for-age, weight-for-age, weight/height and Body Mass Index (BMI).
17The records in the database were validated by verifying the records documented in the database, the correct classification and integrity of the data, and the complete completion of the variables of interest. Regarding the reliability of the databases, this corresponds to data that are reported, validated and supported by government agencies such as the ICBF
11 and regulated institutions such as the IPS-CRIHU
13 on the child health of the indigenous community of Colombia.
Selection bias was controlled by working with the entire population. Information bias was addressed by cleaning the database, ensuring the removal of any records that might contain errors or be irrelevant to the study. At the same time, cross-validation of the data was carried out.
For the analysis of the variables of interest, descriptive statistics were used to analyze sociodemographic conditions (categorical variables were analyzed by proportions) and for nutritional status, measures of central tendency and dispersion were used, considering the normal distribution of the data.
18 The program used was R studio version 3.5.3.
The Research Ethics Committee of the Juan N. Corpas University Foundation approved this research through the Official Letter of the meeting held on May 9, 2022. The study also received the prior approval of the members of the Indigenous Council and the community authorities.
ResultsA total of 2402 records were analyzed on the socio-demographic conditions of the inhabitants of the Nasa indigenous community, of which 93.8% are affiliated with state health insurance, 6.2% do not have this insurance
; In terms of gender distribution, 50.2 per cent were men and 49.8 per cent were women
; the most spoken language is Nasayuwe with 94% of the population, followed by Spanish with 6%; In terms of education, 85.2% of the population has attained secondary education, while 11.3% stated that they have no education at all. Regarding the element used for cooking food, the most used fuel is propane gas (34.2%), followed by natural gas (33.5%) and firewood (31.7%).
Regarding drinking water sources in the community, 64.6% obtain water from the distribution network (pipes or hoses that come directly from water sources such as rivers or wells), 27.2% from streams. At the same time, this data contrasts with the fact that more than half of the population consumes water without any type of treatment, followed by a minority who reported boiling it, 25.8% do so and 21.3% filter it (Table 1). 67.2% of human excrement is disposed of in septic tanks, followed by 5.8% in the open air. Regarding wastewater disposal, 57.7% of the population uses grease traps; 30.2% go directly to nearby rivers, and 10.1% go directly to sewers (Table 1).
Regarding food production in the community, 93.3% of households tend to have productive plots such as vegetable gardens and most of them are family gardens in 93.7% of households (Table 1).
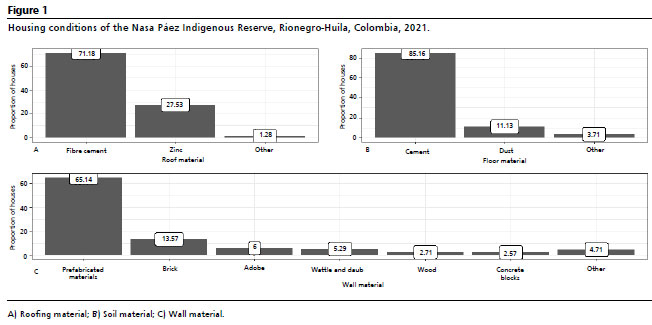
Regarding housing conditions, 71.1 per cent of the population has roof made of fibre cement sheets; Regarding the floors, 85.1% correspond to cement, followed by dirt floors 13.1%, as for the materials of the walls, most of the houses are made of prefabricated materials 65.5% and brick 13.5% (Figure 1).
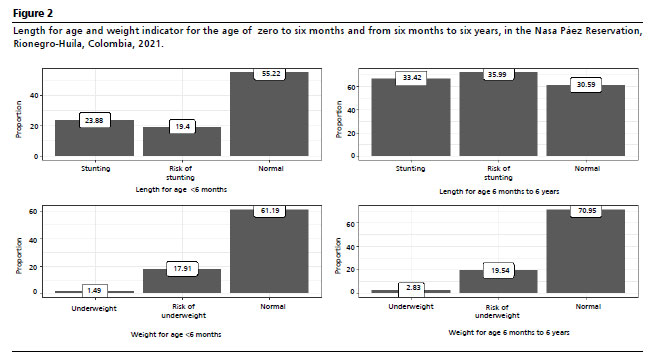
Regarding early childhood nutritional parameters, 55.2% of children under six months of age had adequate Length for their age, followed by stunting in 23.9% of cases and the risk of stunting in 19.4%. On the other hand, children between six months and six years of age showed a significant variation with respect to length, as 69.4% of the population presented some alteration in height, comprised of 33.4% due to low height for age, followed by 36% risk of short stature.
With the weight for age indicator, the main nutritional alterations found, within the age range of children under six months, were the risk of underweight with 17.9% and underweight with 1.5% respectively. For the population aged six months to six years, 19.5% were at risk of being underweight, followed by 2.8% who were underweight (Figure 2).
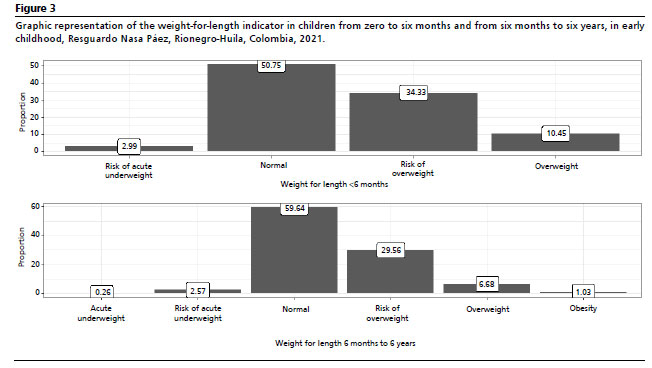
Regarding weight-for-Length (Figure 3), corresponding to that of children under six months of age, 34.3% of the population is at risk of being overweight, 10.4% is overweight and 3.0% is at risk of being acutely underweight. 50.7% were in the normal range. A similar situation was highlighted in the population aged six months to six years, since most of them had normal weight for height (59.6%), however, the risk of overweight was presented by 29.6%, overweight with 6.7% and obesity with 1.03%.
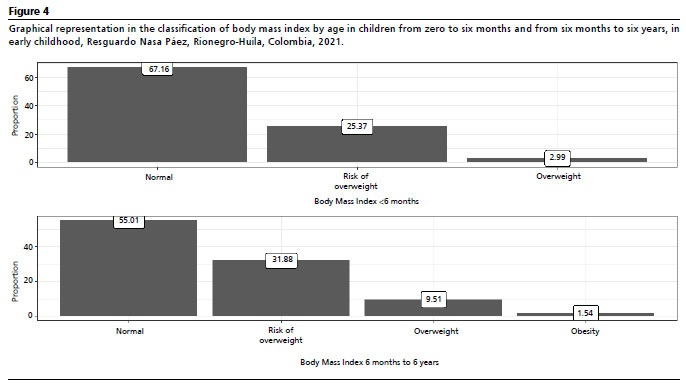
Finally, the analysis of the body mass index (BMI) in the population under six months of age showed that a significant percentage have a normal BMI for their age (67.2%). The risk of being overweight (25.4%) or overweight (3.0%) are more frequent classifications in this age group (Figure 4). A similar situation was found with children over the age of six, where the prevalence of overweight risk corresponded to 31.9%, 9.5% to overweight and 1.5% to obesity (Figure 4).
DiscussionThe main conclusions of the study highlight a predominance of the Nasayuwe language as the main language in the population studied; they live in houses with asbestos cement roofs, with dirt floors in some; they cook with wood, and many are exposed to smoke; Most get drinking water from the distribution network and others simply boil it. Regarding the nutritional status of children under six months of age, 23.9% were short in stature, 17.9% were underweight and 34.3% were at risk of being overweight. In relation to children over six months of age, the most frequent nutritional problems were related to height in 69.4%, and to the risk of chronic malnutrition, in 35.9% of them.
At the same time, a study carried out in the Wayuu indigenous community found that 33.4% of children between six months and six years of age had a higher percentage of moderate stunting and 28.1% of severe stunting,
19 describing nutritional status parameters similar to the current study.
Underweight and the risk of being underweight were identified among children under six months of age, 19.4%, and between six months and six years, with 22.3%. These figures reflect those compiled by the Pan American Health Organization (PAHO), which show that levels of child malnutrition range from 35% to 60% among Quechua and Aymara children in Bolivia and Peru, about 55% among indigenous children in Ecuador, and approximately 75% among indigenous children in Guatemala
20 with respect to the risk of underweight and underweight.
This nutritional problem is an issue that is inefficiently neglected by many governments. A sign of this neglect is the prevalence rates of malnutrition among indigenous children in Latin American countries, which tend to be higher than among non-indigenous children.
21 As a result, in Guatemala, a nutritional study found that the prevalence of chronic malnutrition among children and adolescents was higher in the poorest, in turn with lower levels of education, which mostly corresponded to the indigenous population.
20On the other hand, within the sociodemographic variables of the community, it stands out that most of the population uses untreated water distribution networks as a source of drinking water. In this regard, the study by Daza-Daza
et al.
22 found that poor water supply, purification and treatment systems affect the health and nutrition of the population. Similarly, a study carried out in Australia found that the quality of water consumed by indigenous populations is characterized by high concentrations of organic material, turbidity and heavy metals, which is associated with health problems such as gastrointestinal, in turn highlighting the limited treatment options available to the indigenous community.
23 This finding is consistent with the data from this study, in which more than 72% of the population obtained water from natural sources and 52.2% consumed untreated water.
Another relevant condition with respect to housing in this study is that 98% of the population are poor or low-income people who live in prefabricated houses (65%) or houses with dirt floors (11%). At the same time, a study carried out in 2022 in Peru identified that the main social determinants of health in indigenous communities are the precariousness of housing, 45.2%, housing problems and extreme poverty, in addition to the structural absence of public services 24.5% lack services. This is associated with nutritional problems in the child population,
24,25 a situation that is intertwined with what was evidenced in this study.
On the influence of education on nutrition and nutritional health, a study conducted in Guatemala in 2018
26 found that a low level of education increases the prevalence of chronic malnutrition and stunting in the population. This finding is comparable to the results of the present study, which shows that 77% of the population has only completed basic levels of primary education. On the other hand, a study carried out in New Zealand in 2016 states that ethnic communities present difficulties in accessing primary health care due to variables such as unemployment, educational level and mainly language barriers as the main limiting factors.
27 We find this relevant to the findings of the study, since a significant percentage consider the mother tongue as the main language and may represent barriers to attention.
28-30.The present study has some limitations. In the first place, working with secondary sources limits the quality of the study data; secondly, the loss of some data limits the generalization of some variables in the study; thirdly, the methodological design used did not allow the establishment of a causal association of the sociodemographic variables with nutritional problems, as it is a descriptive study.
In conclusion, the socio-demographic conditions of the indigenous population are determined by poverty, low education, inadequate materials for housing, and the need for drinking water, water and sewerage. At the same time, indicators of stunting, risk of malnutrition, overweight and obesity were identified as the main nutritional problems.
AcknowledgmentsWe would like to thank Universidad Surcolombiana for its support and funding for this research.
Convocatoria de Proyectos de Investigación Mediana cuantía Periodo 2021-2022 (Project Nº 2997).
References1. Organización Panamericana de la Salud (OPS). La situación sociodemográfica de las personas indígenas en América Latina y el Caribe. Análisis en el contexto del envejecimiento y la COVID-19. Washington (DC); 2023. [access in 2023 Dec 10]. Available in:
https://iris.paho.org/bitstream/handle/10665.2/57305/9789275326473_SPA.pdf?sequence=1&isAllowed=y2. Canella DS, Duran AC, Claro RM. Malnutrition in all its forms and social inequalities in Brazil. Public Health Nutr. 2020 Aug; 23 (Supl. 1): S29-38.
3. Bubak V, Sanabria MC, Bubak V, Sanabria MC. Cambios en el estado nutricional de los niños indígenas menores de 5 años en Paraguay entre 2008 y 2016. Pediatría (Asunción). 2023 Apr; 50 (1): 27-32.
4. González-Martell AD, Sánchez-Quintanilla EE, García-Aguilar N, Contreras-Hernández T, Cilia-López VG, González-Martell AD,
et al. Vulnerability for food insecurity: Experiences of indigenous families in the Huasteca Potosina region, Mexico. Estud Soc Rev Aliment Contemp Desarro. 2022 Jan; 32 (59): 1-14.
5. IWGIA. El mundo indígena 2023: Colombia [Internet]. 2023 [access in 2023 Dec 11]. Available in:
https://www.iwgia.org/es/colombia/5083-mi-2023-colombia.html6. Ministerio de Salud (CO). Informe de población indígena Colombia [Internet]. 2022 [access in 2023 Dec 10]. Available in:
https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/PES/informe-poblacion-indigena-abril-2022.pdf7. Organización de las Naciones Unidas (ONU). La agenda 2030 y los Objetivos del Desarrollo Sostenible: una oportunidad para América Latina y el Caribe. 2
nd ed. Santiago; 2018 [access in 2022 May 22]. Available in:
https://repositorio.cepal.org/bitstream/handle/11362/40155/24/S1801141_es.pdf8. Instituto Nacional de Salud, Universidad Nacional de Colombia. Encuesta Nacional de la situación nutricional ENSIN2015 [Internet]. Marzo 2020. 2015 [access in 2021 Aug 24]. 1–683 p. Available in:
https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/ED/GCFI/libro-ensin-2015.pdf9. Organización de las Naciones Unidas (ONU). Situación de los pueblos indígenas del mundo: derechos a las tierras, los territorios, y los recursos. 5º volumen. Nueva York; 2021. [access in 2023 Dec 10]. Available in:
https://www.un.org/development/desa/indigenous-peoples-es/wp-content/uploads/sites/34/2022/06/21-00002_COVER-edit-State-of-Worlds-Indigenous-Peoples_vol5-forSP-compressed.pdf10. Sistema de Información Regional. Huila en cifras y datos [Internet]. 2022 [access in 2023 Dec 10]. Available in:
https://www.sirhuila.gov.co/uncategorized/cifras-y-datos-2005-2018/11. Gobernación del Huila. Ordenanza Nº 032/2009. Comité Departamental de Seguridad Alimentaria y Nutricional. Define la Política Nacional de Seguridad Alimentaria y Nutricional (PSAN). [access in 2023 Apr 14]; Available in:
https://www.huila.gov.co/loader.php?lServicio=Tools2&lTipo=descargas&lFuncion=descargar&idFile=2007312. Albán Achinte A. Sabor, poder y saber. Comida y tiempo en los valles afroandinos del Patía y Chota-Mira. 1
st ed. Popayan; 2013. 318 p.
13. Asociación de autoridades tradicionales del consejo regional indígena del Huila, (CRIHU) H. Plan de Desarrollo Departamental Huila. Diagnóstico de la situación alimentaria y nutricional de la población indígena del departamento del huila. Neiva; 2014. [access in 2023 Apr 14]. Available in:
https://www.huila.gov.co/loader.php?lServicio=Tools2&lTipo=descargas&lFuncion=descargar&idFile=286714. Calderón-Farfán JC, Dussán Chaux JD, Arias Torres D. Food autonomy: decolonial perspectives for Indigenous health and buen vivir. Glob Health Promot. 2021 Sep; 28 (3): 50-8.
15. Calderón-Farfán JC, Torres Soto MA, Quintero Montoya V, Cruz Rodríguez L, González Cerón J, Vargas Guadarrama LA, et al. Practices of food autonomy in the nasa indigenous cosmovision in Colombia. Agroecol Sust Food Syst. 2021 Feb; 45 (2): 279-95.
16. Sampieri Hernández R, Collado Fernandez C, Butista Lucio P. Metodología de la investigacón. [Internet] 6th ed. Ciudad de Mexico; p.546-9. Available in:
https://www.uca.ac.cr/wp-content/uploads/2017/10/Investigacion.pdf17. World Health Organization (WHO). WHO Anthro for Personal Computers, versão 3.2.2 de 2011: Software for assessing growth and development of the world's children. Geneva: WHO; 2010. [Internet]. 2023 [access in 2023 Dec 11]. Available in:
https://cdn.who.int/media/docs/default-source/child-growth/child-growth-standards/software/anthro-pcmanual-v322.pdf?sfvrsn=c4e76522_218. Leon Gordin. Epidemiología Gordis 5th Ed. Barcelona: Elsevier España SLU; 2014.
19. Russell EA, Daza Atehortua C, Attia SL, Genisca AE, Palomino Rodriguez A, Headrick A, et al. Childhood malnutrition within the indigenous Wayuú children of northern Colombia. Glob Public Health. 2020 Jun; 15 (6): 905-17.
20. Batis C, Mazariegos M, Martorell R, Gil A, Rivera JA. Malnutrition in all its forms by wealth, education and ethnicity in Latin America: who are more affected? Public Health Nutr. 2020 Aug; 23 (Supl. 1): S1-12.
21. Leavy P. Tensiones en torno a la (des)nutrición en poblaciones indígenas y criollas en Salta, Argentina, desde una perspectiva antropológica. Salud Colect. 2022 Mar; 18: e3839.
22. Daza-Daza AR, Serna-Mendoza CA, Carabalí-Angola A. El Recurso Agua en las Comunidades Indígenas Wayuu de La Guajira Colombiana. Parte 2: Estudio Cualitativo de las Condiciones de Higiene, Aseo y Disponibilidad de Agua. Inf Tecnol. 2018; 29 (6): 25-32.
23. Balasooriya BMJK, Rajapakse J, Gallage C. A review of drinking water quality issues in remote and indigenous communities in rich nations with special emphasis on Australia. Sci Total Environ. 2023 Dec; 903: 166559.
24. Orcotorio Figueroa R, Orcotorio Figueroa R. Pueblos indígenas y COVID-19 en el Perú: la crisis sanitaria y las deficiencias estructurales. Rev Kawsaypacha: Sociedad y Medio Ambiente. 2022; 2022 (9): 80-107.
25. Gatica-Domínguez G, Mesenburg MA, Barros AJD, Victora CG. Ethnic inequalities in child stunting and feeding practices: Results from surveys in thirteen countries from Latin America. Int J Equity Health. 2020 Apr; 19 (1): 1-13.
26. Yael Milovich J, Unido Elena Villar R. La desnutrición infantil en Guatemala: factores agravantes y palancas de acción. [access in 2023 Dec 10]; Available in:
https://datahelpdesk.worldbank.org/knowledgebase/articles/90651927. Davy C, Harfield S, McArthur A, Munn Z, Brown A. Access to primary health care services for Indigenous peoples: A framework synthesis. Int J Equity Health. 2016 Sep; 15 (1): 1-9.
28. Cediel G, Perez E, Gaitán D, Sarmiento OL, Gonzalez L. Association of all forms of malnutrition and socioeconomic status, educational level and ethnicity in Colombian children and non-pregnant women. Public Health Nutr. 2020 Aug; 23 (Supl. 1): S51-8.
29. Dussán Chaux JD. Influencia de las condiciones socioculturales en la situaicón nutricional de la primera infancia del Resguardo Indígena Nasa-Huila, Colombia 2021-2022. [Internet]. Bogotá (DC): Fundación Universitaria Juan N. Corpas; 2023. 183 hojas. [access in 2023 Dec 10]. Available in:
https://repositorio.juanncorpas.edu.co/handle/001/21030. Farfán JC, Marulanda SC, Zapata IC, Cainas NE. Community Perspectives About Sociocultural Conditions Associated With Children's Health Among the Nasa People in Colombia. Prog Community Health Partnersh. 2018 Sep; 12 (3): 241-2.
Authors' contribution: Dussán Chaux JD: structuring of the manuscript, writing and interpretation of the results and final revision of the article. Ramos-Castañeda JA: quantitative analysis of the data, review of the manuscript and final review of the article. Calderón-Farfán JC: manuscript review, final review and approval. All authors approved the final version of the article and declare no conflicts of interest.
Received May 25, 2023
Final version presented on April 2, 2024
Approved April 5, 2024
Associated Editor: Nathália Souza


 ; Jorge Andrés Ramos-Castañeda2
; Jorge Andrés Ramos-Castañeda2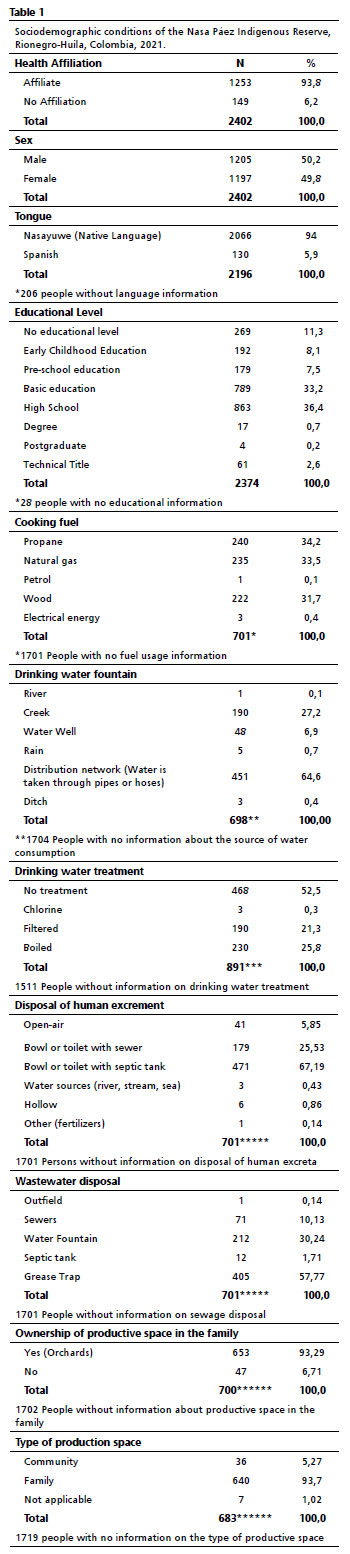






 Ler em português
Ler em português