ABSTRACT
OBJECTIVES: to determine efficiency and safety of three misoprostol regimens for 2nd trimester pregnancy termination in individuals with two or more cesarean section scars.
METHODS: a cross-sectional study included 100 pregnant ladies at 13th -26th weeks gestation with previous two cesarean sections (CSs) who were scheduled for pregnancy termination using misoprostol. Patients were conveniently assigned to 100µg/3h, 200µg/3h or 400 µg/3h regimens. Primary outcome was time to abortion, secondary outcomes were side effect and complications.
RESULTS: a significant association was found between number previous CSs and longer time to abortion (p=0.01). A highly significant association was identified between earlier gestational age and longer time to abortion (p<0.001). Lower side effects and complications were associated with 200 µg misoprostol every 3 hours of (p<0.001). Incomplete abortion was the most frequent recorded complication for the successive doses of misoprostol.
CONCLUSIONS: misoprostol is an effective drug at low doses for pregnancy termination in women with prior two or more caesarean sections. However, its safety needs monitoring of the patient in the hospital to decrease morbidity and mortality behind its use.
Keywords:
Misoprostol, Pregnancy termination, Previous cesarean scar, Second trimester
RESUMO
OBJETIVOS: determinar a eficiência e segurança de três regimes de misoprostol para interrupção da gravidez no segundo trimestre em indivíduos com duas ou mais cicatrizes de cesariana.
MÉTODOS: um estudo transversal incluiu 100 gestantes entre 13ª e 26ª semanas de gestação com duas cesarianas (CEs) anteriores que foram agendadas para interrupção da gravidez com uso de misoprostol. Os pacientes foram convenientemente designados para regimes de 100 µg/3 horas, 200 µg/3 horas ou 400 µg/3 horas. O desfecho primário foi o tempo para o aborto, os desfechos secundários foram efeitos colaterais e complicações.
RESULTADOS: foi encontrada associação significativa entre o número de cesáreas anteriores e o maior tempo até o aborto (p=0,01). Foi identificada associação altamente significativa entre idade gestacional mais precoce e maior tempo para abortar (p<0,001). Menores efeitos colaterais e complicações foram associados com 200 µg de misoprostol a cada 3 horas (p<0,001). O aborto incompleto foi a complicação mais frequente registrada para as doses sucessivas de misoprostol.
CONCLUSÕES: o misoprostol é um medicamento eficaz em doses baixas para interrupção da gravidez em mulheres com duas ou mais cesarianas anteriores. Porém, sua segurança necessita de monitoramento do paciente no hospital para diminuir a morbimortalidade por trás de seu uso.
Palavras-chave:
Misoprostol, Interrupção da gravidez, Cicatriz, Segundo trimestre
IntroductionTerminating a second trimester pregnancy for maternal or fetal reasons is a frequent occurrence in obstetric practice owing to the complexities and psychological pain associated with the procedure. While numerous techniques of second-trimester termination are successful, they come with a number of dangers. Misoprostol is prostaglandin E1 synthetic analogue, is gaining widespread popularity for both induction of labor and pregnancy termination.
1 The first study on the possible impact of misoprostol on pregnancy termination was published in 1987.
2,3Abuse was motivated by the fact that it was less expensive, easier to use, and much less traumatic compared to other abortion procedures. Over the last two decades, misoprostol has been shown to be beneficial not only for terminating pregnancy at different gestational stages, but also for cervical ripening, inducing labor for term pregnancy, treating incomplete abortion,
4 and perhaps managing postpartum hemorrhage.
5 According to Royal College of Obstetricians and Gynecologists (RCOG) 2015 guidelines for comprehensive abortion care, misoprostol 800 micrograms is used at 14 weeks of gestation or more, followed by misoprostol 400 micrograms every three hours until abortion ensues.
6 While, the American College of Obstetricians and Gynecologists' (ACOG) 2013 guidelines stated that 2
nd -trimester medical abortion is performed using misoprostol 400 microgram.
7 Unfortunately, many recent studies have shown outstanding success with misoprostol intravaginal usage for 2
nd trimester pregnancy termination, but the majority of the research omitted patients who had already had caesarean delivery.
8 Induction of labor with prostaglandins during 2
nd or 3
rd trimester is considered risky for these women owing to possibility of uterine rupture. As the prevalence of caesarean births has grown over the previous two decades, number of women with this obstetric history who are offered pregnancy termination has increased as well.
9 Thus, the objective of the study is to determine efficiency and safety of three misoprostol regimens for 2
nd trimester pregnancy termination in women with two or more cesarean section scars.
MethodsThis is a cross sectional study, conducted at Al-Elwiya Maternity Teaching Hospital, from January 2019 to December 2019.
One hundred pregnant ladies at 13-26 weeks of gestation with previous two scars and more who were scheduled for pregnancy termination for the following reasons were included: 1) congenital fetal abnormalities incompatible with life such as severe nervous system disorder; 2) preterm premature rupture of membranes with chorioamnionitis determined by clinical features and laboratorial tests which include fever, uterine fundal tenderness, maternal tachycardia (>100/min), fetal tachycardia (>160/min) and purulent or foul amniotic fluid,
2,5 in addition to leukocytosis and high CRP
10; 3) mid-trimester missed miscarriage which is defined as a situation when there is a non-viable fetus within the uterus, without symptoms of a miscarriage during the second trimester (between 13–24 weeks of gestation) according to ultrasound measurements for gestational age. Indications of pregnancy termination was revised by an Iraqi board-certified gynecologist and agreed by Committee of Termination of Pregnancy in the hospital and the decision to start misoprostol was taken by the specialist and consultant on call after admission of the patient. All patients were given an informed written consent. Patient were excluded if they refused to take the medication.
All patients were fully assessed regarding history and examination. Gestational age dating was based on the last menstrual cycle and confirmed by ultrasound examination. Investigations done to the patients included blood group, complete blood count and plasma fibrinogen level.
Dose and regimens: three doses of misoprostol were used (100 µg, 200 µg and 400 µg) vaginally. The dose was determined according to the gestational age and fetus status. A 3-hour regimen was followed for all patient with a maximum of 6 doses and 2,400μg.
11Outcomes measured: 1) induction to abortion time which is defined as the time between misoprostol treatment and full fetal expulsion; 2) adverse effect of the drug such as nausea, vomiting and diarrhea and complications such as incomplete abortion, postpartum hemorrhage, infection and ruptured uterus.
All patients were monitored during the induction and six-24 hours post abortion. Vital signs, adverse events, vaginal bleeding, uterine contractions, and cervical dilatation were observed hourly after misoprostol administration. No additional intervention was performed if the placenta looked to be complete. If the placenta was partial or did not discharge after one hour of fetal expulsion, the uterus was surgically evacuated through curettage. All women were offered a follow-up consultation within two weeks of termination.
Statistics Data were analyzed using computerized statistical software, namely SPSS version 21. The descriptive statistics are presented as (mean and standard deviation) and the frequencies as percentages. The Kolmogorov Smirnov test determined the normality of the data set. Multiple contingency tables were created and relevant statistical tests were run, including the chi-square test for categorical variables (the Fishers exact test was used when the anticipated variable represented less than 20% of the total). The threshold of significance (
p value) for all statistical analyses is set to 0.05, and the results are displayed as tables and/or graphs. The community medicine expert conducted the study's statistical analysis.
The research was approved by the ethical and scientific committee of the Al-Kindy College of Medicine, University of Baghdad, Iraq, (Ethical clearance letter number: ECL-N190324).
ResultsA total of 100 pregnant women in their 2
nd trimester were included with a mean age of 28.1±5.3 years; most of them (58%) were 20-29 years old.
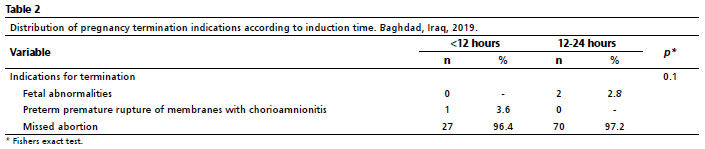
Mean previous cesarean sections (CSs) number of was 2.5±0.7, 60% of them had previous 2 CSs. Mean gestational age of participants was 16.4±3.4 weeks,72% of them were between 12-18 weeks. The most common indication of pregnancy termination was missed abortion (97%) followed by fetal abnormalities (2%) and preterm premature rupture of membranes with chorioamnionitis (1%).
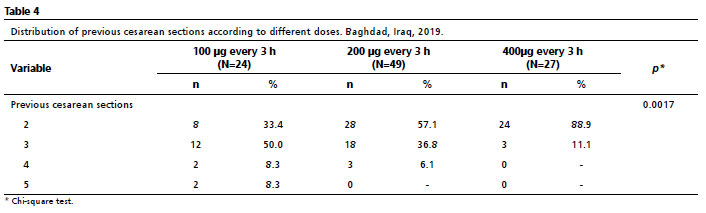
The doses of misoprostol were distributed as following; 100 µg every 3 hours (24%), 200 µg every 3 hours (49%) and 400µg every 3 hours (27%). The median total dosage of misoprostol was 1,600μg in the study (range: 800–2,400μg). Mean time from induction to abortion was 13.3±4.3 hours; 28% of women had induction time of less than 12 hours.
There was a significant correlation between women who had a higher mean of prior CSs and a longer period from induction to abortion (
p=0.01). A significant correlation between earlier gestational age and a longer induction to abortion time was observed (
p=0.001) as shown in Table 1.
Table 2 shows longer induction time among women with fetal abnormalities and missed abortion, however that was statistically not significant.
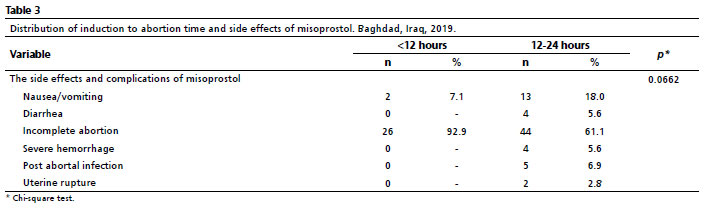
There was side effects and complications tend to be more frequent with longer time of induction to abortion time (
p=0.066), as shown in Table 3.
Two cases have ended with uterine rupture after 18h (6 doses) from the induction, both has previous three scars, with missed abortion at 18 and 25 weeks. The regimens of misoprostol were 200 µg and 100 µg/3h respectively.
Table 4 shows the different doses of misoprostol for previous scar of cesarean sections. a significant association between lower previous cesarean sections and higher doses of misoprostol (
p=0.0017).
There was a significant association between lower side effects and complications with use of 200 µg misoprostol every 3 hours (
p<0.005); the main side effects related to 200 µg misoprostol were mild like nausea, vomiting and diarrhea except for incomplete abortion and uterine rupture; while other doses were significantly related to severe hemorrhage and infection in addition to incomplete abortion. All these findings were shown in Table 5.
DiscussionMisoprostol is a very successful medication for terminating pregnancy in women who have had two or more caesarean sections, even when given at modest dosages. Nevertheless, the administration of this treatment requires vigilant patient monitoring within the hospital setting in order to reduce the occurrence of illness and death associated with its usage.
Cesarean section rates are growing globally. As a result, the incidence of women with prior cesarean surgery who need pregnancy termination is growing, and the danger of uterine rupture is increasing. Although risk of uterine rupture in women with previously damaged uteri continues to be low. (1%), obstetricians continue to see it as a hazard.
12Misoprostol offers a number of benefits over other prostaglandin preparations for 2
nd trimester termination, including its low price and being stable at room temperature. It could be administered vaginally or orally and proved to be effective at a range of various doses. Despite the overwhelming evidence that misoprostol is successful, its safety in women with a preexisting uterine scar who had a 2
nd trimester abortion remains in doubt.
13In this study, we used three different doses of misoprostol at three-hour intervals (100 µg/3hours, 200 µg/3hours, and 400 µg/3 hours), which is consistent with the latest International Federation of Gynecology and Obstetrics (FIGO) misoprostol regimens published on June 22/2017, which recommend 400µg pv/sl/bucc every three hours for 2
nd trimester pregnancy termination at 13-24 weeks and 200µg pv/sl/bucc every four hours for women in 25-26 weeks and those with fetal death and inevitable abortion.
14 100µg pv every three hours was additionally used in patients to examine the efficiency of low dose. Previous studies have shown equal effectiveness of 100µg and 200µg sublingual misoprostol in the second trimester abortion with less overall dose.
15 Additionally, as shown by previous research, 400g misoprostol administered vaginally every 3-6 hours is probably the optimum regimen for 2
nd -trimester abortion.
4 We gave the medication at a three-hour interval for all doses used; since many studies demonstrated that this time interval was associated with significantly shorter abortion interval and a greater effectiveness.
16,17Vaginal route of administration was selected in this study over other routes as many studies including a Cochrane review which concluded that oral regimens significantly outperformed vaginal regimens in terms of abortion rate within 24 hours.
18,19The median dosage of misoprostol used in this study was 1,600μg (range: 800-2,400μg), which was comparable to the dose used by other studies (1,200-2,400 μg) for 2
nd trimester termination with previous scar.
20,21 Average maternal age in our series was 28.1 years which was similar to most of the published studies.
20The most common cause for pregnancy termination in the current study was missed abortion (97%) other studies reported fetal abnormalities (48%) as the most frequent cause followed by missed abortion (40%) .
18,22 We had only two cases of termination for congenital anomaly that were incompatible with life (anencephaly). Iraq law has a strict stance on abortion, which prohibits termination for chromosomal abnormalities unless it is performed to save the woman's life.
An Australian study conducted by Dickinson and Doherty
23 (2009) has shown that rising gestational age was associated with a longer induction-abortion interval, which contradicts our study results, as a highly significant association was observed between women with earlier gestational age and a longer time from induction to abortion (
p=0.001), but it does comply with the Ethiopian study (2019) of Alemayehu
et al.,
24 who stated that the induction termination interval was inversely correlated with gestational age and discovered that the effects of misoprostol grow in direct proportion to parity. Dickinson and Doherty,
23 discovered that the existence of a preexisting uterine scar had no effect on the length of pregnancy termination. We found a significant association between women with a higher previous cesarean section mean and a longer induction to abortion time.
Considering adverse effects, it has been proposed that uterine rupture is more likely to occur in people with a scarred uterus after taking misoprostol.
7 Case reports documented ruptured uterus after using the standard 200 µg dose in patients with previous scar.
22,25 Low-dose Misoprostol (100 µg), however, was found to be potentially effective and safe in the management of second-trimester abortions in women with repeated cesarean deliveries.
12 We have reported two incidences of uterine rupture, with both 100 and 200µg. Both were after 18 h (6 doses) from induction beginning. After reviewing the literature, a study done in USA in 2009 by Berghella
et al.
13 found that 0.4% of women who have had one prior low transverse, 0% of women who have had two prior low transverse, and 50% of women who have had a prior classical cesarean birth experience uterine rupture after a misoprostol termination.
16 Therefore, we recommended that in women with a history of uterine scarring, abortion induction should start with lower doses of the drug (misoprostol) and not increase the dose if there is no initial reaction.
Incomplete delivery of the placenta was frequently reported in all three used doses in the current study. Delayed placenta delivery is a common complication in patients with cesarean scar. Mazouni
et al.
26 reported in their retrospective study done in France, 2009, that the incidence of retained placenta was higher in patients with previous scar compared to control (70%
vs. 52.5%, respectively,
p =0.025).
The study is limited by the uneven distribution of patients among the studied groups. Due to the study's design, in which dosage was based on maternal age and fetal status per FIGO guidelines for 2017, we were unable to randomly assign patients to treatment arms. Additionally, powered study with larger sample size will be needed to confirm the current results.
In conclusion, misoprostol is an effective drug at low doses for pregnancy termination in women with prior two or more caesarean sections. However, its safety needs monitoring of the patient in the hospital to decrease morbidity and mortality behind its use.
References1. Peitsidis N, Kapetanios G, Kalogiannidis I, Tsakiridis I, Virgiliou A, Dagklis T,
et al. 346 Efficacy and safety of mifepristone and sublingual misoprostol for second trimester medical abortion. A prospective study. Eur J Obstet Gynecol Reprod Biol. 2022; 270: e97.
2. Khan R-U, El-Refaey H. Pharmacokinetics and adverse-effect profile of rectally administered misoprostol in the third stage of labor. Obstet Gynecol. 2003; 101 (5): 968-74.
3. Rabe T, Basse H, Thuro H, Kiesel L, Runnebaum B. Effect of the PGE1 methyl analog misoprostol on the pregnant uterus in the first trimester. Geburtshilfe Frauenheilkd. 1987 May; 47 (5): 324-31. [Article in German]
4. Tsakiridis I, Giouleka S, Mamopoulos A, Athanasiadis A, Dagklis T. Investigation and management of stillbirth: a descriptive review of major guidelines. J Perinat Med. 2022 Feb; 50 (6): 796-813.
5. Gallos ID, Papadopoulou A, Man R, Athanasopoulos N, Tobias A, Price MJ,
et al. Uterotonic agents for preventing postpartum haemorrhage: a network meta‐analysis. Cochrane Database Syst Rev. 2018 Apr; 4 (4): CD011689.
6. Theodosiou AA, Mitchell OR. Abortion legislation: exploring perspectives of general practitioners and obstetrics and gynaecology clinicians. Reprod Biomed Online. 2015 Feb; 30 (2): 197-202.
7. Dadhwal V, Garimella S, Khoiwal K, Sharma KA, Perumal V, Deka D. Mifepristone followed by misoprostol or ethacridine lactate and oxytocin for second trimester abortion: a randomized trial. Eurasian J Med. 2019 Oct; 51 (3): 262-6.
8. Feldman DM, Borgida AF, Rodis JF, Leo MV, Campbell WA. A randomized comparison of two regimens of misoprostol for second-trimester pregnancy termination. Am J Obstet Gynecol. 2003; 189 (3): 710-3.
9. Boerma T, Ronsmans C, Melesse DY, Barros AJD, Barros FC, Juan L,
et al. Global epidemiology of use of and disparities in caesarean sections. Lancet. 2018; 392 (10155): 1341-8.
10. Tita AT, Andrews WW. Diagnosis and management of clinical chorioamnionitis. Clin Perinatol. 2010; 37 (2): 339-54.
11. Lin C-J, Chien S-C, Chen C-P. The use of misoprostol in termination of second-trimester pregnancy. Taiwan J Obstet Gynecol. 2011 Sep; 50 (3): 275-82.
12. AlSaad D, Alobaidly S, Abdulrouf P, Thomas B, Ahmed A, AlHail M. Misoprostol for miscarriage management in a woman with previous five cesarean deliveries: a case report and literature review. Ther Clin Risk Manag. 2017 May; 13: 625-7.
13. Berghella V, Airoldi J, O'Neill AM, Einhorn K, Hoffman M. Misoprostol for second trimester pregnancy termination in women with prior caesarean: a systematic review. BJOG. 2009 Aug;116 (9): 1151-7.
14. Morris JL, Winikoff B, Dabash R, Weeks A, Faundes A, Gemzell‐Danielsson K,
et al. FIGO's updated recommendations for misoprostol used alone in gynecology and obstetrics. Int J Gynaecol Obstet. 2017 Sep; 138 (3): 363-6.
15. Dilbaz S, Caliskan E, Dilbaz B, Kahraman BG. Frequent low-dose misoprostol for termination of second-trimester pregnancy. Eur J Contracept Reprod Health Care. 2004; 9 (1): 11-5.
16. Bhattacharjee N, Saha SP, Ghoshroy SC, Bhowmik S, Barui G. A randomised comparative study on sublingual versus vaginal administration of misoprostol for termination of pregnancy between 13 to 20 weeks. Austr New Zealand J Obstet Gynaecol. 2008; 48 (2): 165-71.
17. Allen R, O'Brien BM. Uses of misoprostol in obstetrics and gynecology. Rev Obstet Gynecol. 2009; 2 (3): 159-68.
18. Dickinson JE, Evans SF. A comparison of oral misoprostol with vaginal misoprostol administration in second-trimester pregnancy termination for fetal abnormality. Obstet Gynecol. 2003; 101 (6): 1294-9.
19. Wildschut H, Both MI, Medema S, Thomee E, Wildhagen MF, Kapp N. Medical methods for mid‐trimester termination of pregnancy. Cochrane Database Syst Rev. 2011 Jan; (1): CD005216.
20. Herabutya Y, Chanarachakul B, Punyavachira P. Induction of labor with vaginal misoprostol for second trimester termination of pregnancy in the scarred uterus. Int J Gynecol Obstet. 2003 Dec; 83 (3): 293-7.
21. Abbas NF, Saeed AS. Mid Trimester Termination of Pregnancy in Patients with Two or More Previous Scars by Using Safe Regime of Misoprostol. J Med Surg Pract. 2021; 7 (3): 131-43.
22. Mobusher I. Misoprostol for Second Trimester Pregnancy Termination in Women with Prior Caesarean Section. Pakistan J Med Health Sci. 2013; 7 (1): 3.
23. Dickinson JE, Doherty DA. Factors influencing the duration of pregnancy termination with vaginal misoprostol for fetal abnormality. Prenat Diag. 2009 May; 29 (5): 520-4.
24. Alemayehu B, Addissie A, Ayele W, Tiroro S, Woldeyohannes D. Magnitude and associated factors of repeat induced abortion among reproductive age group women who seeks abortion Care Services at Marie Stopes International Ethiopia Clinics in Addis Ababa, Ethiopia. Reprod Health. 2019;16 (1): 1-10.
25. Nayki U, Taner CE, Mizrak T, Nayki C, Derin G. Uterine rupture during second trimester abortion with misoprostol. Fetal Diag Ther. 2005; 20 (5): 469-71.
26. Mazouni C, Provensal M, Porcu G, Guidicelli B, Heckenroth H, Gamerre M,
et al. Termination of pregnancy in patients with previous cesarean section. Contraception. 2006;73 (3): 244-8.
Author's contribution: Reehan E: collection of data; Abid SJ: analysis of data; Sarsam S: formulation of research methodology; Abdulla TN: formulation of research methodology and writing; Zaid Al-Attar: writing and finalizing the final manuscript for submission. All authors approved the final version of the article and declare no conflict of the interest.
Received on November 15, 2022
Final version presented on September 30, 2023
Approved on October 1, 2023
Associated Editor: Aurélio Costa


 ; Sahar Jassim Abid2
; Sahar Jassim Abid2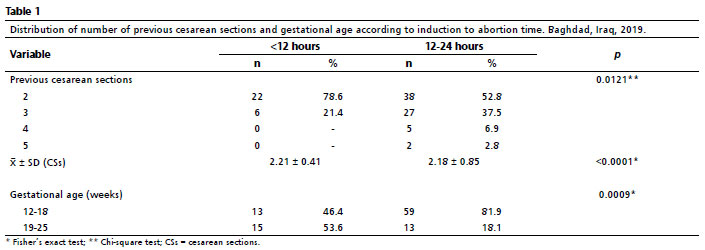







 Ler em português
Ler em português