ABSTRACT
OBJECTIVES: to investigate how social support for the nuclear family, extended family and extra-family influences the functioning indexes of the mothers of the State of São Paulo.
METHODS: data collection took place via an online form, posted in maternity groups on social networks. A structured questionnaire was used to identify the profile of the puerperal woman and her support network, as well as WHODAS 2.0 to assess functioning.
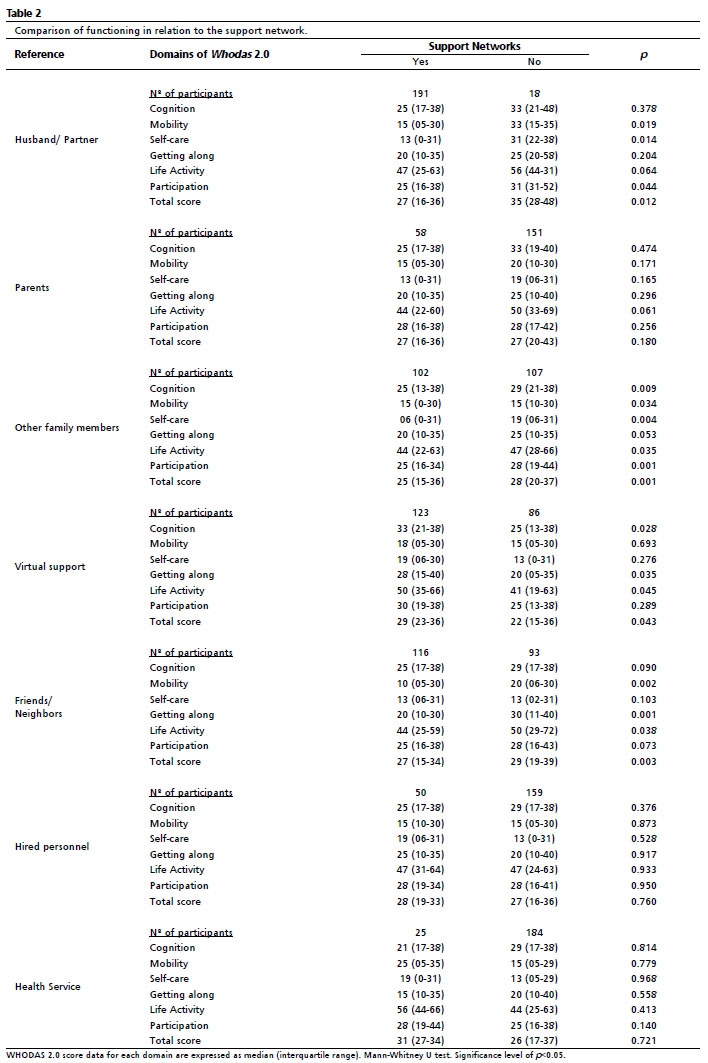
RESULTS: support of husband/partner (p=0.012), other family members (p=0.001), friends/neighbors (p=0.003) were translated into better functioning of puerperal woman, while virtual support (p=0.043) was related to worse rates in the domains contemplated by WHODAS 2.0. Regarding health professionals, the result was not significant (p=0.721), indicating a low frequency for this type of support (12%).
CONCLUSIONS: the presence of support acted positively on the functioning of women in the puerperium.
Keywords:
Postpartum period, Social support, Health promotion, Social determinants of health, International classification of functioning, disability and health
RESUMO
OBJETIVOS: investigar como o suporte social pela família nuclear, família estendida e extrafamiliar influenciam nos índices de funcionalidade das puérperas do Estado de São Paulo.
MÉTODOS: a coleta de dados ocorreu via formulário online, divulgado em grupos de maternidade em redes sociais. Foi utilizado um questionário estruturado para a identificação do perfil da puérpera e de sua rede de apoio, bem como o Whodas 2.0 para avaliação da funcionalidade.
RESULTADOS: o suporte do marido/companheiro (p=0,012), outros familiares (p=0,001), amigos/vizinhos (p=0,003) representaram melhor funcionalidade da puérpera, enquanto o apoio virtual (p=0,043) estava relacionado a piores índices nos domínios contemplados pelo Whodas 2.0. Em relação aos profissionais da saúde, o resultado não foi significativo (p=0,721), indicando frequência baixa deste tipo de apoio (12%).
CONCLUSÃO: a presença de apoio atuou positivamente na funcionalidade da mulher no puerpério.
Palavras-chave:
Período pós-parto, Apoio social, Promoção da saúde, Determinantes sociais da saúde, Classificação internacional de funcionalidade, incapacidade e saúde
IntroductionThe pregnancy-puerperal cycle alters the functioning and routine of women due to several biopsychosocial factors.
1 In the postpartum period, the return to pre-gestational conditions interfere with health from hormonal fluctuations and readaptations of the body.
2 The risks of emotional vulnerability are also included in this perspective, since anxiety, stress, fear, instability and fatigue are all present,
3 together with the adaptation of the new routine and the care of the neonate.
4 Nevertheless, the physical and social environment generates reactions that, depending on the context, can be negative or positive.
5 It is necessary, therefore, to understand the determinants and conditioning factors of puerperal women’s health and how the physical, social, and attitudinal aspects influence health in the puerperium, taking distance from the biomedical model still used by health professionals.
6As per Marin and Piccinini,
7 in addition to the support network, women’s profile also modifies the performance of the maternal role and the women’s health. Among other factors, the socioeconomic level, age, ethnicity, and education are social determinants capable of generating emotional destabilization also limiting the creation of the parental bond between mother and baby.
7The support network can be made up of family, friends, neighbors, health professionals, among others. The nuclear family (husband/partner and children) and the extended family (other relatives) are included as an available support to be tapped, bringing meaning and regarded as who is really present.
8 Health professionals, on the other hand, have been considered only as informative agents, distant from a possible bond.
9 For the health and well-being of the woman and the effectiveness of the relationship with the new member of the family, the support network plays a positive role; social support helps to ease or overcome difficulties and to cope with the care of the newborn.
8Therefore, the objective of the study was to investigate the functioning of puerperal women according to the assistance of the support networks of the nuclear family, extended family and extra-family, and how they contribute to a new look at health conditions in puerperium and care strategies in the Maternal and Child Network beyond the newborn.
MethodsThis is a cross-sectional study, with a quantitative and descriptive approach and was approved by the Ethics Committee on Research with Human Beings of the Federal University of São Paulo (CEP-UNIFESP - opinion 1206/2017, CAAE 78025717.4.0000.5505). The present study was based on responses to an online structured form. This was disseminated in groups of a social network focused on pregnant women and/or maternity, encompassing approximately 25 groups for pregnant women and/or maternity on the social network Facebook. The initial posting was also shared on the social network by several profiles. Therefore, it was not possible to measure the final repercussions of the initial publication.
The study included women over 18 years of age, residents of the State of São Paulo, between the 10th and 180th day of the puerperium. All participants of the study agreed to the terms of the Informed Consent Form (ICF). Participants who answered the forms incompletely and did not meet the inclusion criteria of the study (postpartum period) were excluded from the study.
The online form consisted of open questions about the profile of puerperae, containing age, gender, race, education, city, marital status, family income, questions related to pregnancy, type of delivery, postpartum period, number of children and previous pregnancies, return to work, type of breastfeeding, and the use of artificial feeding bottles to understand the determinants and conditioning factors of puerperal women’s health.
Aiming to understand the presence or not of the support network, the online form had structured questions about the emotional, financial, domestic activities, baby care, and leaving home support, with pre-established options: nuclear family (husband/partner), extended family (parents and other relatives), and extra-family (friends, neighbors, hired personell, health professionals, virtual support).
In order to evaluate functioning, we applied the self-administered 36-question version of the WHODAS 2.0 questionnaire, and the activities were rated among “none”, “mild”, “moderate”, “severe”, and “extreme or cannot do”. This instrument contemplates the domains based on the International Classification of Functioning, Disability, and Health (ICFDH) in relation to mobility, cognition, self-care, getting along, life activities (household and work) and participation. Higher scores mean impairments in functioning.
The response variable considered for sample sizing was the WHODAS 2.0 questionnaire and data from the study by Silveira
et al.2 who used this instrument in a population similar to the present study to assess maternal morbidity. The sample size calculation was based on the effect size and standard deviation, resulting in 64 individuals for each group of puerperal periods.
The total sample reached was 209 puerperae, being divided into two groups: late puerperal and remote. The results of the groups were evaluated according to the time of days after delivery. From the 10
th to the 45
th day after, delivery is considered late puerperal, after the 46
th until the 180
th day after delivery is remote puerperal.
For data analysis, the Shapiro-Wilk normality test was used to identify the distribution of variables. For the analysis of the influence of support on functioning, the non-parametric ordinal variables obtained from the WHODAS 2.0, the analysis was done using Mann Whitney U test, and the numerical variables referring to the functioning index in the WHODAS 2.0 domains of women with or without support were presented as medians and interquartiles. The other categorical variable information was represented by percentages and frequencies. For all tests, the significance level considered was 5% (
p<0.05).
ResultsThe initial response group encompassed 369 puerperae answering the study instruments, however, 10 incomplete forms and 150 were excluded by the criterion of “postpartum period” outside the late puerperium (10 to 45 days) and remote (45 to 180 days). The final sample included 209 puerperae, and 68.4% (n=143) were in the remote puerperium period (46th to 180 days after delivery).
The sample profile was characterized by puerperal women with a median age of 31 years (between 27 and 34 years), with complete college education (52.2%, n=109), married or in a stable union (85.6%, n=179) and with per capita family income higher than 3.75 minimum wages (53.6%, n=112).
Regarding maternity, the data showed a higher number of cesarean deliveries (57.9%) compared to vaginal deliveries (42.1%). Regarding breastfeeding, the prevalence was of breast milk (75.1%), however, the replacement or supplementation by artificial milk is noticiable (Table 1).
In addition to motherhood, the presence of support influenced the functioning indices of the WHODAS 2.0 domains. Participants demonstrated better activity/participation performance when they stated support from “husband/partner”, “other family members”, and “friends/neighbors”. However, they demonstrated lower performance when they stated searching for “virtual support” (Table 2).
DiscussionThe sample profile in this study is representative of the middle class of the population of the state of São Paulo, where the majority reported having completed college education (52.2%, n=109) and per capita family income greater than R$ 3,748.00 (53.6%, n=112). It is worth noting that, despite being far from the conditions of vulnerability, they presented disabilities according to WHODAS 2.0 by the health condition observed in the postpartum period.
Puerperae who had the support of nuclear family, extended family, as well as extra-family support, achieved lower scores, i.e., better functioning when compared to no support.
In addition to providing stability in the period of women’s transformation to motherhood,
8 the support network also becomes a facilitator starting with orientations, emotional support, help with baby care, with feeding, among others.
10 Therefore, it shows the importance of strengthening the networks that foster health promotion and prevention behaviors, avoiding situations of morbidity and worsening of health.
11When there is the active presence of the father figure beyond the economic structuring of the home, the indexes of women’s functioning are better. It is seen that the domains of mobility, participation, and self-care showed lower indexes compared to the absence of this support.
The functioning of the puerperal woman is facilitated when the paternal figure provides care for the woman and the baby, helping with the domestic routine, transportation, and going to public places and medical appointments.
10,12 Likewise, the father’s understanding that lactation demands time and dedication to the baby enables to continue exclusive breastfeeding.
12The interference in the woman’s functioning when the paternal support is ineffective or absent is remarkable, because she starts to devote herself exclusively to the care and development of the child. However, when the social support is created with other characters in the puerperal woman’s life, new strategies and adaptations emerge to face the difficulties generated by the absence of the father’s figure.
7According to the results of the present study, the relevance of support from other family members and friends/neighbors was observed. These other family members and friends contributed to mobility, self-care, getting along, life activities (household and work), and participation compared to the group without support. In the study by Silveira
et al.,
2 women in the puerperium with and without severe maternal morbidity achieved high disability scores in the same WHODAS 2.0 domains as the present study; however, the authors did not analyze how social support could improve such indexes.
In Ethiopia, culture acts as a facilitator of support during the first months of the puerperium, and as a result, women tend to recover quickly.
13 Thus, it is possible to see how support is fundamental to stability and reestablishment of functioning in the puerperium.
Through the analysis of the WHODAS 2.0 functioning scores in relation to virtual support, we identified higher scores in cognition, getting along, life activities (household and work) and total score domains. Difficulties were scored in concentrating, evoking memories, solving problems, learning new tasks, understanding and maintaining a dialogue, dealing with strangers, maintaining a friendship, relating to close people, making new friends, having sex, difficulties in completing domestic and occupational responsibilities with the necessary promptness and speed.
The study by Kaufmann
et al.,
14 examined whether determinants of health and frequency of Facebook use were related to levels of mental health. Worse economic status and lower mental health quality were associated with higher social media use. Decreased functioning is not necessarily a causal effect of social media use, rather, the lower the quality of mental health, the more frequent was Facebook enjoyment. However, the reasons why the use of this social network negatively interfered with the mental health of the sample were not investigated.
The responsibilities emerging from motherhood cause women to go through a de-structuring of their own identity, often causing internal conflicts over their own unconscious desires and longings for the maternal role projected onto the world versus the self-perception of reality.
9 Furthermore, the socioeconomic and attitudinal context can amplify feelings of anxiety, fear, and insecurity.
14 When confronted with the benefits of virtual support, it is seen that it is generally linked to the search for a space for interaction, venting off, sharing information and doubts.
15However, this resource can also spread cultural myths and beliefs based on misinformation from self-perception and individual experiences.
16 Within motherhood, the alleged fake news are capable of interfering with the adaptation processes between the mother-child dyad, for example, in breastfeeding and raising children based on the attachment theory.
4In this study, the low frequency of the presence of health professionals and services was verified, in which only 12% of women in this study reported having this type of support. The puerperium demands knowledge beyond the biomedical model. In this period, health professionals must approach women to support them.
11 Despite this fact, the results show a distance established in the relationship between health professionals and service users.
17The results of the present study were not enough to make inferences about the high prevalence of virtual support and association with the absence of other types of support, especially from health professionals. Future studies that analyze whether the search for virtual support may be associated with the absence of support from health professionals and services, considering regional differences in the Health Care Network of the municipality or municipalities, complementary services of the private network and the profile of the participants would be important to advocate for continuing education policies to support breastfeeding.
According to the study by Corrêa
et al.,
17 where 18 puerperal women assisted by the Family Health Strategy of the city of Recife were interviewed, attention to the puerperal period has been ineffective. One of the reasons that the study pointed out was that in the puerperium, the attention has been focused only on care for the newborn. Moreover, the dynamics between the flows of home care and scheduled appointments and the way the professional-puerperal relationship is established have been insufficient.
According to Jordão
et al.,
9 the puerperium provides risk factors for women: inadequate adaptation to change, insufficient self-control, role ambivalence, anxiety, depression, inadequate coping strategies, helplessness, dissatisfaction with the maternal role, insufficient motivation, pessimism, tension of responsibility. For this reason, it is necessary that there are frequent home visits by health professionals, especially in the immediate puerperium, for the reception and improved listening to doubts regarding the health of the woman-mother and the child.
17 When health risks are detected from the first week of the postpartum period, through qualified listening, the creation of a patient-professional bond, and the detection of barriers and facilitators of health promotion, it is possible to intervene and prevent worsening of the woman’s functioning.
11,17Understanding the dynamics of support networks in the puerperium contributes to the development of an expanded and humanized look at the health conditions of women and the effectiveness of the health care network.
8,11 The implementation of the health action promotes breastfeeding and greater safety for the care of the baby, as well as making the individuals around the woman aware of her current health conditions.
12 It also allows the deconstruction of the biomedical vision structured within the health services and exercised over the Maternal and Child Network.
The support is able to empower women to the issues of motherhood, especially in exclusive breastfeeding.
12 Furthermore, security favors the creation of a bond between the mother-baby binomial, consequently reducing insecurity in baby care and providing better child development.
13 Facilitating strategies during the whole pregnancy-puerperal cycle must be built together with a multi professional team, having the family to be constituted as the protagonist of this action.
9 Welcoming practices need to be encouraged, establishing humanization in health services and even within the social support around a woman-mother.
17Using the results presented as a starting point, we conclude that the network of face-to-face support favors better functioning in the puerperal period. However, further studies are needed with other profiles of women, especially those who are in social vulnerability, based on collections that also include puerperae without access to the Internet.
References1. Silveira C, Parpinelli MA, Pacagnella RC, Camargo RS, Costa ML, Zanardia DM,
et al. Adaptação transcultural da Escala de Avaliação de Incapacidades da Organização Mundial de Saúde (WHODAS 2.0) para o Português. Rev Assoc Med Bras. 2013; 59 (3): 234-40.
2. Silveira C, Parpinelli MA, Pacagnella RC, Andreucci CB, Ferreira EC, Angelini CR,
et al. A cohort study of functioning and disability among women after severe maternal morbidity. Int J Gynecol Obstetr. 2016 Jul; 134 (1): 87-92.
3. Benítez NS. La experiencia de lamaternidad en mujeres feministas. Nómadas. 2016; 44: 255-67.
4. Hernandez BP. Alteraciones en el vínculo materno infantil: prevalencia, factores de riesgo, criterios diagnósticos y estrategias de evaluación. Rev Univ Ind Santander Salud. 2016; 48 (2): 164-76.
5. Castro SS, Castaneda L, Araújo ES, Buchalla CM. Aferição de funcionalidade em inquéritos de saúde no Brasil: discussão sobre instrumentos baseados na Classificação Internacional de Funcionalidade, Incapacidade e Saúde (CIF). Rev Bras Epidemiol. 2016; 19 (3): 679-87.
6. Brasil ACO. Promoção de Saúde e a Funcionalidade Humana. Rev Bras Prom Saúde. 2013; 26 (1): 1-4.
7. Marin A, Piccinini CA. Famílias uniparentais: a mãe solteira na literatura. Psico. 2009 [access in 2020 jul 27]; 40 (4): 422-9. Available from:
https://revistaseletronicas.pucrs.br/ojs/index.php/revistapsico/article/view/26838. Rapoport A, Piccinini CA. Apoio social e experiência da maternidade. J Hum Growth Dev. 2006; 16 (1): 85-96.
9. Jordão RRR, Cavalcanti BMC, Marques DCR, Perrelli JGA, Mangueira SO, Guimarães FJ,
et al. Acurácia das características definidoras do diagnóstico de enfermagem Desempenho do Papel Ineficaz. Rev Eletr Enf. 2017 [access in 2020 jul 27]; 19: 1-10.
10. Cremonese L, Wilhelm LA, Prates LA, Paula CC, Sehnem GD, Ressel LB. Social support from the perspective of postpartum adolescents. Esc Anna Nery. 2017; 21 (4): e20170088.
11. Li Y, Long Z, Cao D, Cao F. Social support and depression across the perinatal period: a longitudinal study. J Clin Nurs. 2017 Sep; 26 (17-18): 2776-83.
12. Rêgo RMV, Souza AMA, Rocha TNA, Alves MDS. Paternidade e amamentação: mediação da enfermeira. Acta Paulista Enferm. 2016; 29 (4): 374-80.
13. Senturk V, Hanlon C, Medhin G, Dewey M, Araya M, Alem A,
et al. Impact of perinatal somatic and common mental disorder symptoms on functioning in Ethiopian women: The P-MaMiE population-based cohort study. J Affect Disord. 2012 Feb; 136 (3): 340-9.
14. Kaufmann R, Buckner MM, Ledbetter AM. Having Fun on Facebook?: Mothers’ Enjoyment as a Moderator of Mental Health and Facebook Use. Health Commun. 2017 Aug; 32 (8): 1014-23.
15. Holtz B, Smock A, Reyes-Gastelum D. Connected Motherhood: Social Support for Moms and Moms-to-Be on Facebook. Telemed J E Health. 2015 May; 21 (5): 415-21.
16. Sacramento I. A saúde numa sociedade de verdades. Rev Eletrôn Comun Inf Inov Saúde. 2018; 12 (1): 4-8.
17. Corrêa MSM, Feliciano KVO, Pedrosa EN, Souza AI. Acolhimento no cuidado à saúde da mulher no puerpério. Cad Saúde Pública. 2017; 33 (3): e00136215.
Received on October 18, 2020
Final version presented on May 13, 2022
Approved on June 7, 2022
Authors’ contributionAlves AB was responsible for preparing the research project, collecting the data, tabulating the variables, interpreting and analyzing the data, writing and reviewing the article. Pereira TRC and Aveiro MC were responsible for the data analysis and review of the final writing. Cockell FF was the project advisor and supervisor, contributing to the study design, writing review, and data analysis. All authors approved the final version of the article and declared no conflict of interest.


 ; Thalita Rodrigues Christovam Pereira 2
; Thalita Rodrigues Christovam Pereira 2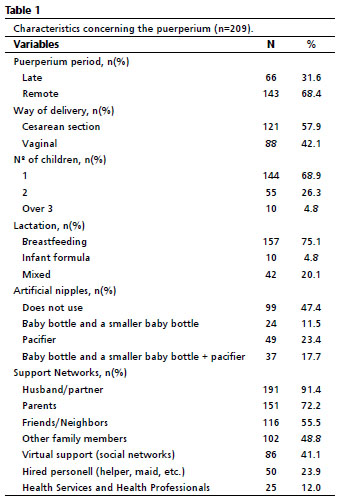






 Ler em português
Ler em português