ABSTRACT
OBJECTIVES: to carry out the cross-cultural adaptation of The Postpartum Childcare Stress Checklist scale to be used in Brazil.
METHODS: the cross-cultural adaptation process followed internationally defined guidelines: double translation, synthesis and back-translation, analysis by a committee of experts, proposal for a pre-final and pre-test version, analysis of the psychometrics properties and generation of the final version. The reliability and validity of the final version were analyzed through a cross-sectional epidemiological study involving 190 women in the postpartum period. Cronbach's α indicator for reliability analysis and exploratory factor analysis with main component extraction were estimated for validity analysis.
RESULTS: α-Cronbach's was 0.894. The tested Brazilian version proved to be one-dimensional and the factor analysis pointed to four factors that were very closely distributed and explained 57.8% of the variance. All items of the original instrument were maintained in the proposed final version.
CONCLUSIONS: the proposed Brazilian version proved to be valid and reliable for application in Brazilian populations.
Keywords:
Maternal and child health, Depression postpartum, Scales, Questionnaires
RESUMO
OBJETIVOS: proceder a adaptação transcultural da escala The Postpartum Childcare Stress Checklist para ser utilizada no Brasil.
MÉTODOS: o processo de adaptação transcultural seguiu diretrizes definidas internacionalmente: dupla tradução, síntese e retrotradução, análise por comitê de especialistas, proposta de uma versão pré-final e pré-teste, avaliação das propriedades psicométricas e geração da versão final. A confiabilidade e validade da versão final foram analisadas por meio de estudo epidemiológico transversal envolvendo 190 mulheres em período pós-parto. Foram estimados o indicador α-Cronbach para análise da confiabilidade e análise fatorial exploratória com extração de componentes principais para análise da validade.
RESULTADOS: o indicador α-Cronbach foi de 0,894. A versão brasileira testada mostrou-se unidimensional e a análise fatorial apontou quatro fatores distribuídos de maneira muito próxima e que explicaram 57,8% da variância. Todos os itens do instrumento original foram mantidos na versão final proposta.
CONCLUSÃO: a versão brasileira proposta mostrou-se válida e confiável para aplicação em populações brasileiras.
Palavras-chave:
Saúde materno-infantil, Depressão pós-parto, Escalas, Questionários
IntroductionWith motherhood, significant changes occur in the family’s lifestyle, especially the mother’s, encompassing both the rearrangement of marital and social life, in addition to bodily changes.
1,2 There is a need for continuous maternal stimuli, especially in the first 18 months of the child’s life, and theirabsence can impact child development.
1 These stimuli help the child to develop his/her social and motor skills. This is the time when children start to develop important skills for their future social integration.
3 The postnatal period is therefore an important and potentially risky stage for maternal mental health. Women feel largely affected by the level of stress resulting from the sudden change in lifestyle they go through.
4 Mental disorder during this period is not only restricted to depression, which occurs in 15 to 20% of puerperal women. Anxiety may also occur in 16% of puerperal women, post-traumatic stress disorder in 4% and postpartum psychosis in less than 1%.
5Early diagnosis of maternal stress allows not only an effective treatment, but also identification and preventionof psychological diseases development, such as maternal anxiety and depression. Thoseillnesses show great potential to generate child development and mother’s mental health complications.
6,7In this connection, the Postpartum Childcare Stress Checklist (PCSC) has been proposed in Canada.
7 The scale, designed to be self-administered, aims to assess the level of maternal stress in connection with the care of the child in the postpartum period using 19 questions about stressors experienced in the four previous weeks. According to the authors, the instrument is valid and reliable for the construct in question that takes a unidimensional form with α-Cronbach index of 0.960. A database search did not find any similar instrument. In Brazil, there is no known scale or validated questionnaire for measuring maternal stress in connection withchildcare, which would allow knowingmore about this phenomenon and, consequently, enable preventive interventions at the individual and collective level.
Thus, our study aimed to proceed with the cross-cultural adaptation of the PCSC scale to be used in Brazilin order to provide a reliable and valid instrument to assess the maternal stress level associated withchildcare. It is believed that a validated Brazilian version could be used both in pregnant women care in the postpartum period and as a research instrument in different health areas.
MethodsThe cross-cultural adaptation process followed the guidelines defined by Beaton
et al.
8 and Wild
et al.
9 and complied with the methodological criteria proposed by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR).
10In the first stage, the translation of the original instrument written in English into Portuguese spoken in Brazil was carried out. The translation was performed by two independent translators, one of Brazilian nationality and the other a native English speaker. The second stage consisted in the translation synthesis. The two translations were compared and synthesized into a single Brazilian version by the research authors. In the third stage, a back-translation was performed by two native English teachers without any medical knowledge and without knowledge of the original scale. An expert committee was set up by the researchers composed by an obstetrician, an epidemiologist and a nurse specialized in pregnant women care, with the objective of evaluating the semantic, idiomatic, experiential and conceptual equivalence in a theoretical and cultural way, based on clinical experience and on the expected understanding of the populationaccording to the experts’ experience. In addition, the grammatical rules of the Portuguese language were reviewed. The compilation of the steps was carried out by the committee’s participants.
After identifying and discussing any discrepancies, the pre-final version (PCSC-Br) was suggested and was applied to ten postpartum women, up to eight weeks after giving birth. Participants were asked to give their opinion on the understanding of the items and responses, in addition to the adequacy of the language. The researchers evaluated possible interpretation difficulties, potential constraints and inadequacy of the answers given. After any necessary adjustment, the researchers approved the suggested Brazilian version.
In order to assess the psychometric properties of the suggested Brazilian version, an epidemiological cross-sectional study was carried out. The study population consisted of women in the postpartum period, up to eight weeks after giving birth. The sample consisted of 190 women, which corresponds to the proportion of ten women included for each item on the scale.
11-13 Sample selection was performed by the consecutive method, on the established days of data collection, from May to October 2019. Inclusion criteria were women aged at least 18 years; Brazilian; with fluency to read and write in Portuguese; who took their babies to the postpartumvisit at the Polyclinic of the
Universidade do Sul de Santa Catarina pediatric service in the city of Palhoça, SC. Caretakers who took the child for the puerperal visit, but who were not the child’s biological mother, were excluded from the investigation. In addition to the application of the PCSC-Br, in which women directly filled out the questionnaire, information about age, education, whether they lived with a stable partner, whether the delivery had been in a public institution, whether they had already undergone a previous cesarean section and loss of pregnancy and precocious pregnancy were also collected, through direct interviews.
The information was entered into the Excel program and the data were exported to the SPSS 18.0 computer program, where they were reviewed. To measure the reliability of the scale, its stability was evaluated using the α-Cronbach indicator, calculated for the general analysis and in case each item wasremoved from the scale. A second application of the scale was performed after a one-week interval, in 20% of the total sample, for stability analysis in the two applications using Pearson’s correlation coefficient and the intraclass correlation coefficient. In addition, the correlation between the differences between both applications and the averages of the results were observed using the Bland-Altman plot. Content validity was assessed by the opinion of the experts involved in the study. Exploratory Factor Analysis (EFA) with extraction of principal components was used to review the construct validity of the proposed version, after verifying the suitability of the set of data obtained in the collection, through a linear correlation matrix, using the Kaiser-Meyer-Olkin (KMO) test and the Bartlett test of sphericity. The Kaiser criterion for eigenvalues greater than or close to one and the scarp plot were used to define the number of factors extracted. To minimize the number of questions with high loads on each factor, the extraction of principal components by rotation of Varimax allowed defining the items commonalities of the suggested Brazilian version.
All participants were invited to sign an informed consent form, after being informed about the objectives and importance of the research. Non-participation caused no harm to mother and child. The research project was approved by the Research Ethics Committee of the
Universidade do Sul de Santa Catarina, through Opinion number 3.397.812.
ResultsAfter the stages of cross-cultural adaptation of The Postpartum Childcare Stress Checklist (PCSC), the semantic, idiomatic, experiential and conceptual equivalences were discussed in the experts’ committee. No significant discrepancies were found between the synthesis obtained and the back-translation. Thus, the pre-final version was formed and was applied to ten women in the puerperal period. The participants completed the questionnaire individually, under the supervision of one of the investigators. No questions were asked regarding the understanding of the items. After this process, the investigators approved the proposed Brazilian version. The results of these steps can be seen in Table 1.
Measurement equivalence – reliability and validity:
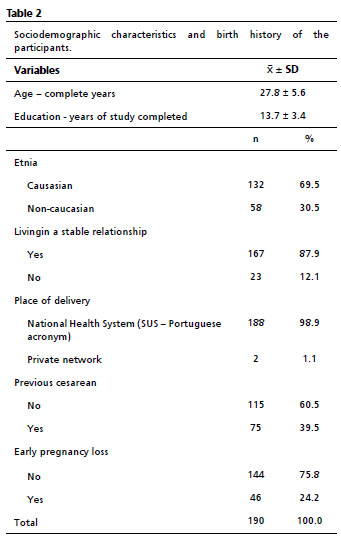
A total of 190 women completed the questionnaire and 42 (22.1%) women completed the same questionnaire one week later. The sociodemographic characteristics and birth history of the participants are shown in Table 2.
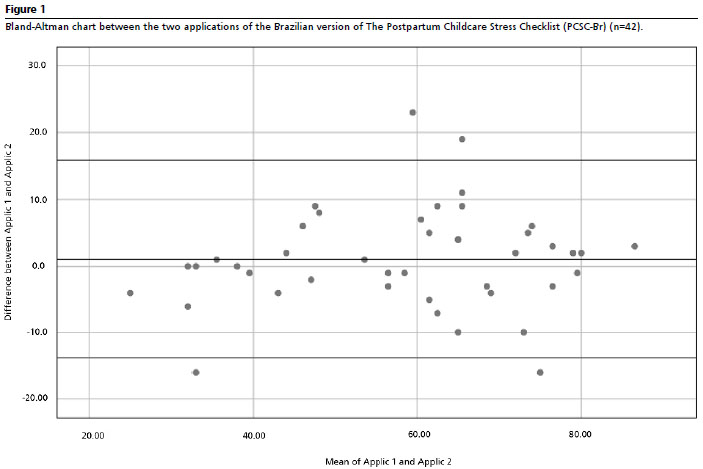
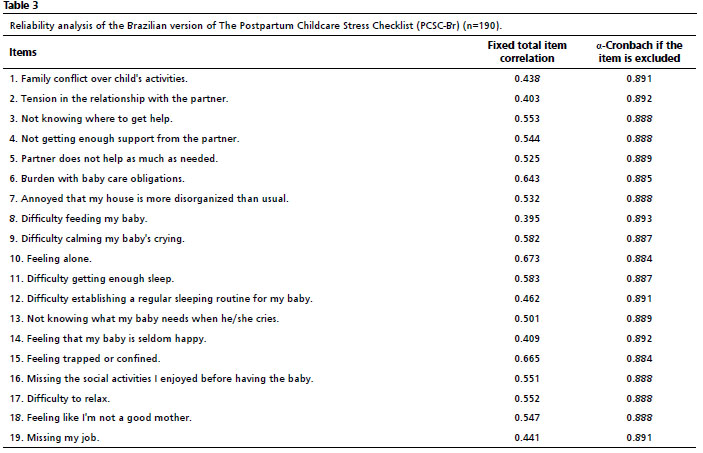
In the PCSC-Br reliability analysis, the Pearson correlation coefficient between the two applications was r=0.894. The intraclass correlation coefficient between both applications was R=0.892 (CI95%=0.811; 0.940). The correlation between the differences between both applications and the averages of the results are reported in the Bland-Altman plot (Figure 1). The overall α-Cronbachindex was 0.893. The corrected correlation values of the total item and of the α-Cronbach if any item would be excluded were also calculated (Table 3).
The analysis of the correlation matrix with 19 items showed a linear correlation between most questions (
p<0.001). The KMO measure of sampling adequacy was 0.869, showing a correlation between the variables. Barlett’s test of sphericity also showed adequacy of the database for performing the EFA (
p<0.001). The commonalities analysis showed that all items shared a significant percentage of variance with the defined factors.
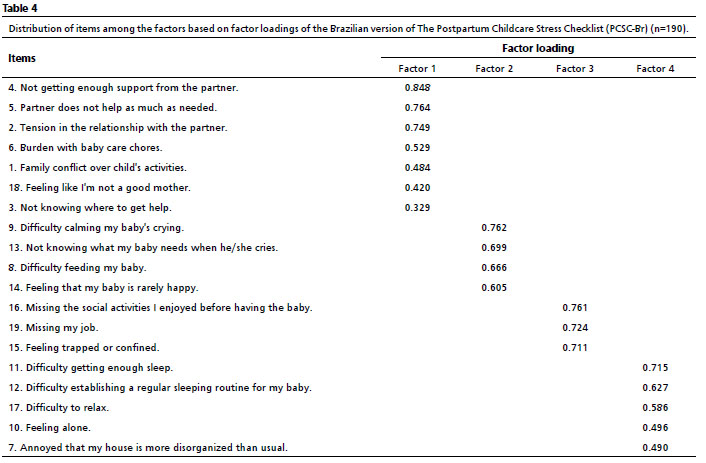
To define the number of factors that could represent the structure of the original variables, the extraction of the main components was performed. Based on the Kaiser criterion, only the factors corresponding to eigenvalues greater than one or very close to one (λ≥1) were considered. Thus, four closely distributed factors explained 57.8% of the variance. The rotation of factors by the Varimax method sought to minimize the number of variables with high loadings in one factor and maximize the variation between the weights of each main component. The component matrix, after the orthogonal rotation, aimed to put extreme loads, so that each variable would be associated with only one factor, simplifying the interpretation of factors. The assessment of factor loadings showed that all items of the instrument should be considered because they have a minimum level of 0.300 (Table 4).
DiscussionThe early diagnosis of maternal stress allows not only an effective treatment, but also the identification and prevention of maternal psychological disorders onset.
1,2 The dimensions and items used in the development of the instrument under study are consistent with the risk factors for postpartum depression documented in other studies.
13 Among them, the experience of stressful events in the last 12 months, marital conflicts, unemployment, absence or little social support, disorganization at home, poor emotional support, accumulation of tasks, among others.
14To date we are unaware of cross-cultural adaptation studies of the instrument proposed by Dennis
et al.
7 so thatour study is possibly the first initiative in this direction. The need for the availability of valid and reliable instruments on maternal stress to be applied both in the clinical practice and in research is emphasized.
The PCSC-Br presented reliability indicators similar to the original Canadian version. The overall α-Cronbach index in the present study was 0.893, showing good internal consistency. The study of behavior of the index if any of the scale items were removed pointed to the possibility of maintaining all of them in the Brazilian version. For comparison purposes, the overall α-Cronbach original version was 0.960.
7 Furthermore, the instrument proved to be stable in the comparison between applications, with an interval of one week, in the same research subjects, as demonstrated by the high intraclass correlation coefficient and the Bland-Altman plot.
Like the original instrument,
7,15 the Brazilian version also showed unidimensionality of the construct, as indicated in the scarp slope plot. The Canadian instrument, through the AFE, presented four analysis dimensions: i- relationship with the partner; ii- child care; iii- maternal social interactions; iv- establishment of new routines.
15 Similarly, the factor analysis of the present study identified four dimensions accounting for 57.8% of the variance, with all good factor loading items. Out of the 19 items, seven were grouped into one factor, accountable for 15.2% of the variance, mostly related to the partner, in addition to the feeling of not being a good mother (“Not receiving enough support from the partner (a)”; “The partner does not help as much as necessary”; “Stress in the relationship with the partner”; “Overloaded with the chores of taking care of the baby”; “Family conflict over the child’s activities”; “Feeling like I’m not a good mother” and “Not knowing where to get help”).Thus, the Brazilian version presented a similar dimension to the Canadian version.
15 Four items were grouped in factor 2, which accounts for 14.6% of the variance associated with child care, a dimension similar to the original instrument
15 (“Difficulty in calming down my baby’s cry”; “Not knowing what my baby needs when he/she cries”; “Difficulty feeding my baby” and “Feeling that my baby is seldom happy”). Three items wereclustered in factor 3, which is accountable for 14.3% of the variance and related to maternal social interactions, as in the original instrument
15 (“Missing the social activities I had before having the baby”; “Missing my job” and “Feeling trapped or confined”). Finally, five items were clustered into factor 4, accountable for 13.7% of the variance and related to new routines
15 (“Difficulty getting enough sleep”; “Difficulty establishing a regular sleep routine for my baby”; “Difficulty relaxing”; “Feeling alone” and “Upset that my home is more disorganized than usual”). Therefore, an adjustment in the order of items was suggested, keeping them all though in the Brazilian version (Table 4).
Thus, the PCSC-Br presented properties quitesimilar to the original instrument. It proved to be valid and reliable for the construct in question, enabling preventive interventions against maternal stress at the individual and collective levels. It should be taken into account that the diagnosis of postpartum depression is continuously neglected, both by the patient and her family members, who attribute the symptoms to “fatigue and exhaustion” inherent to the moment experienced.
16,17 Therefore, this instrument demonstrates a great contribution potential, since knowing the risk factors for postpartum depression helps planning and implementing preventive actions, such as referring the mother to counseling or psychotherapy.
16Some limitations of the present study require caution in interpreting the results. The first one concerns the non-probabilistic selection of the sample. Although in sufficient numbers for this type of study,
11-13 the selection took place consecutively on the days of collection, which could imply a selection bias. Second, the study was carried out in only one region of Brazil, which implies the need for further studies involving other populations in different sociocultural frameworks.
It can be concluded that the cross-cultural adaptation process of The Postpartum Childcare Stress Checklist generated a valid and reliable Brazilian version for application in postpartum women to assess the level of maternal stress related to childcare.
References1. Silva RS, Porto MC. A importância da interação mãe-bebê. Ensaios Ciênc Biol Agrar Saúde. 2016; 20 (2): 73-8.
2. Silva LS, Pessoa FB, Pessoa DTC, Cunha VCM, Cunha CRM, Fernandes CKC. Análise das mudanças fisiológicas durante a gestação: Desvendando mitos. Rev Fac Montes Belos. 2015; 8 (1): 1-16.
3. Carvalho CA, Silva AAM, Ribeiro MRC. Sintomas depressivos e de ansiedade maternos e prejuízos na relação mãe/filho em uma coorte pré-natal: uma abordagem com modelagem de equações estruturais. Cad Saúde Pública. 2017; 33 (6): e00032016.
4. Rodrigues OMPR, Schiavo RA. Stress na gestação e no puerpério: uma correlação com a depressão pós-parto. Rev Bras Ginecol Obstet. 2011; 33 (9): 252-7.
5. Degner D. Differentiating between “baby blues,” severe depression, and psychosis. BMJ. 2017 Nov; 359: j4692.
6. Krob AD, Godoy J, Leite KP, Mori SG. Depressão na gestação e no pós-parto e a responsividade materna nesse contexto. Rev Psicol Saúde. 2017; 9 (3): 3-16.
7. Dennis CL, Brown HK, Brennensthl S. The Postpartum Partner Support Scale: Development, psychometric assessment, and predictive validity in a Canadian prospective cohort. Midwifery. 2017 Nov; 54: 18-24.
8. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976). 2000 Dec; 25 (24): 3186-91.
9. Wild D, Grove A, Martin M, Eremenco S, McElroy S, Verjee-Lorenz A,
et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005; 8 (2): 94-104.
10. ISPOR. The leading professional society for health economics and outcomes research (HEOR) globally. The Society’s mission is to promote HEOR excellence to improve decision making for health globally. [access in 2020 out 8]. Available from:
https://www.ispor.org11. Laros JA. O uso da análise fatorial: algumas diretrizes para pesquisadores. In: Pasquali L, editor. Análise fatorial para pesquisadores. Brasília (DF): LabPAM Saber e Tecnologia; 2012. p.141-60.
12. Anthoine E, Moret L, Regnault A, Sébille V, Hardouin J. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health Qual Life Outcomes. 2014 Dec; 12: 176.
13. Mokkink LB, de Vet HCW, Prinsen CAC, Patrick DL, Alonso J, Bouter LM,
et al. COSMIN Risk of bias checklist for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018 May; 27 (5): 1171-9.
14. Gomes LA, Torquato VS, Feitoza AR, Souza AR, Silva MAM, Pontes RJS. Identificação dos fatores de risco para depressão pós-parto: importância do diagnóstico precoce. Rev Nev. 2010; 11: 117-23.
15. Dennis CL, Brown HK, Brennensthl S. Development, psychometric assessment, and predictive validity of the postpartum Childcare Stress Checklist. Nurs Res. 2018; 67 (6): 439-46.
16. Nascimento LFC. Perfil de gestantes atendidas nos períodos pré-natal e perinatal: estudo comparativo entre os serviços público e privado em Guaratinguetá, São Paulo. Rev Bras Saúde Mater Infant. 2003; 3(2): 187-94.
17. Law KH, Dimmock J, Guelfi KJ, Nguyen T, Gucciardi D, Jackson B. Stress, depressive symptoms, and maternal self-efficacy in first-time mothers: modelling and predicting change across the first six months of motherhood. Appl Psychol Health Well Being. 2019 Mar; 11 (1): 126-47.
Received on February 11, 2021
Final version presented on March 15, 2022
Approved on April 4, 2022
Authors’ contributionAbreu RC, Nunes RD, Traebert E and Traebert J contributed to the analysis, interpretation of data and writing of the manuscript. Traebert J, Nunes RD, Traebert E contributed to the conception, study design and critical review of the manuscript. All authors approved the final version of the article and declared that there is no conflict of interest.


 ; Rodrigo Dias Nunes 2
; Rodrigo Dias Nunes 2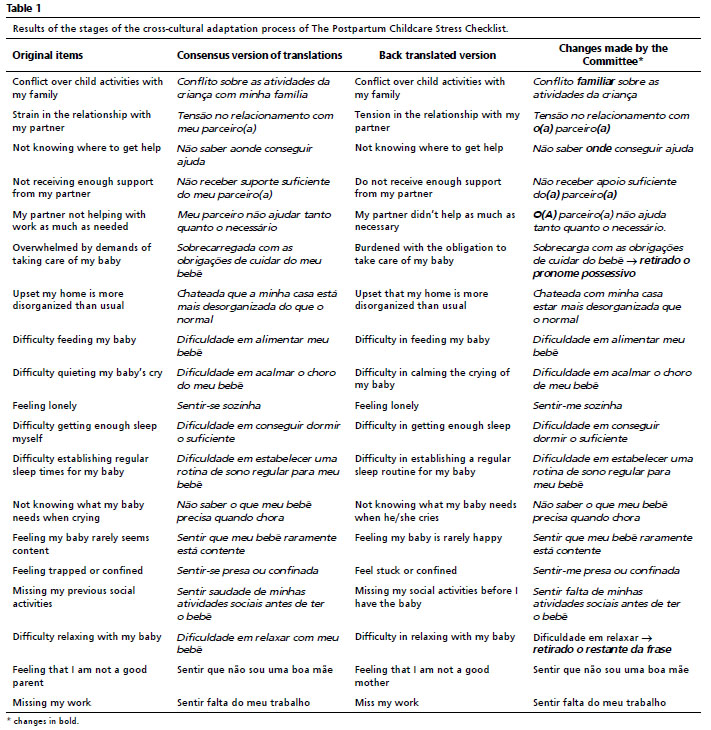






 Ler em português
Ler em português