ABSTRACT
OBJECTIVES: investigate whether prenatal characteristics were associated with dietary pattern of pregnant women.
METHODS: we studied 200 high-risk pregnant women in Fortaleza, Ceará. The identification of dietary patterns was performed through principal component analysis with the orthogonal Varimax rotation. Poisson regression was used to estimate prevalence ratios (PR) and respective confidence intervals (CI95%).
RESULTS: three major dietary patterns were identified: ‘common Brazilian’, ‘healthy’ and ‘energy-dense’. After adjustments conducted with multivariate analysis, pregnant women who had not received dietary guidance in prenatal consultations (34%) were less likely to adhere to the ‘healthy’ pattern (PR = 0,81; CI95%= 0,67-0,95). Pregnant women who attended an appropriate number of consultations (≥ 6 consultations) (41%) showed greater adherence to the ‘healthy’ pattern (PR = 1,15; CI95%= 1,01-1,32) and lower adherence to the ‘energy-dense’ pattern (PR = 0,85; CI95%= 0,74-0,99).
CONCLUSION: it was observed that the high-risk pregnant women who attended an adequate number of consultations during the prenatal care had a higher chance to adhere to the ‘healthy’ pattern and a lower chance to adhere to the ‘energy-dense’ pattern. Not receiving guidelines on prenatal nutrition was inversely associated with the healthy pattern. Thus, the importance of high-risk pregnant women undergoing an appropriate prenatal care is reinforced.
Keywords:
Dietary patterns, Pregnancy, high-risk, Prenatal care
RESUMO
OBJETIVOS: investigar o efeito potencial das características de acompanhamento do pré-natal em padrões alimentares identificados em gestantes de alto risco.
MÉTODOS: foram estudadas 200 gestantes de alto-risco de Fortaleza, Ceará. Os padrões alimentares foram identificados pela análise de componentes principais seguida de rotação ortogonal Varimax. Utilizou-se Regressão de Poisson para estimar as razões de prevalência (RP) e os intervalos de confiança (IC95%).
RESULTADOS: três padrões alimentares foram identificados: ‘comum brasileiro’, ‘saudável’ e ‘denso em energia’. Após a realização de ajuste com análise multivariada, as gestantes que não receberam orientação sobre alimentação nas consultas do pré-natal (34%) apresentaram menores chances de adesão ao padrão ‘saudável’ (RP = 0.81, IC95%= 0.67-0.95). Aquelas que realizaram um número de consultas adequado (≥ 6 consultas) (41%) apresentaram maior adesão ao padrão ‘saudável’ (RP = 1.15, IC95%= 1.01-1.32) e menor adesão ao padrão ‘denso em energia’ (RP = 0.85, IC95%= 0.74-0.99).
CONCLUSÃO: observou-se que as gestantes de alto risco que compareceram a um número adequado de consultas no pré-natal tiveram maior chance de aderir ao padrão ‘saudável’ e menor chance de aderir ao padrão ‘denso em energia’. Não receber orientações sobre nutrição durante o pré-natal foi inversamente associado ao padrão ‘saudável’. Reforçando a importância das gestantes de alto risco realizarem um pré-natal adequado.
Palavras-chave:
Padrões alimentares, Gravidez de alto risco, Cuidado pré-natal
IntroductionPregnancy is a phase that comprehends profound physical, social and emotional changes in a woman’s life.
1 Although it is a natural and routine event, it can be said that every pregnancy can involve some risk,
1,2 which can range from low to high risk.
1Therefore, when factors associated with a poor maternal and perinatal prognosis are present, requiring more frequent assessments by a specialized multidisciplinary health team, followed by the use of procedures with greater technological density, the pregnancy is defined as a high-risk one.
1During the gestational period, inadequate diets characterized by ahigh consumption of ultraprocessed foods, mainly those rich in sugar, can interfere with placental development, affect fetal development, in addition to generating a greater risk for the development of gestational diabetes mellitus, nutritional deficiencies and excessive weight gain,
3 affecting not only maternal health, but also the child’s, as it favors the increase of adipose tissue in children, and the occurrence of non-communicable chronic diseases.
4Among all pregnant women, it is estimated that 15% will have some form of complication that increases the chance of an unfavorable evolution, requiring some type of clinical intervention such as hospitalization or anticipation of delivery.
2Gestational risk may be related to factors present before and/or during the pregnancy. Pre-pregnancy risk factors can be grouped into individual and socioeconomic characteristics, previous reproductive history and pre-existing clinical conditions,whereas gestational factors include exposure to teratogenic agents, obstetric diseases and clinical complications.
5Adequate prenatal care, capable of detecting and providing early intervention in risk situations, is essential to prevent maternal or perinatal death.
5 The late start of prenatal care and having onlya few prenatal consultations can hinderthe diagnosis and treatment of some diseases, in addition to compromising health promotion.
6During prenatal care, the health professional needs to assess the nutritional status and monitor weight gain, guiding the pregnant woman’s diet.
7 Excessive weight gain or maternal obesity increases the risksduring pregnancy, which can lead to adverse results such as: gestational diabetes, gestational hypertension, preeclampsia, premature rupture of membranes (PROM), prolonged delivery, cesarean section, fetal macrosomia and depression.
8Thus, the monitoring of the nutritional status and weight gain are important not only for maternal health, the evolution of pregnancy, fetal growth and development. These can assist in the recovery from childbirth and influence the success of breastfeeding.
5,9Studies indicate that both the isolated effect of foods or nutrients, as well as adherence to dietary patterns are related to the maternal and child health.
10 However, dietary patterns have been adopted in studies to assess food consumption and in food recommendations, due to their greater scope, considering that the chemical compounds resulting from a diet can be synergistic or antagonistic, altering the bioavailability of nutrients.
11In Brazil, studies that investigate dietary patterns are mostly carried out in adult populations.
12 During pregnancy, the publications are mainly associated with sociodemographic characteristics.
13,14 Even in other countries, few studies have associated dietary patterns in pregnant women with the risk of developing complications such as preeclampsia or gestational diabetes.
10 There is also a scarcity of studies investigating the association between dietary patterns and prenatal care in high-risk pregnant women.
Thus, evaluating the food consumption in high-risk pregnant women, as well as investigating possible associations with prenatal care characteristics, is important to improve prenatal care and health education, with an emphasis on nutritional care.
The present study aimed to investigate the potential effect of prenatal care characteristics on dietary patterns identified in high-risk pregnant women in the city of Fortaleza, state of Ceará, Brazil.
Methods This is a cross-sectional study,which is part of a larger research called “The maternal and child health care network in Fortaleza: taking care of pregnant women, nursing mothers and children under two years of age”.
The present study was carried out in a reference hospital belonging to the Brazilian Unified Health System (SUS,
Sistema Único de Saúde) for high-risk pregnancy, in the city of Fortaleza, capital of the state of Ceará, located in the Northeast region of Brazil. The municipality is the most populous in the state and its estimated population, in 2014, was 2,571,896 inhabitants living (100%) in the urban area.
The sample (N=200) was defined through non-probabilistic convenience sampling, recruiting all high-risk pregnant women hospitalized in the maternity hospital from October 2013 to July 2014. All pregnant women considered to be high risk by the hospital where the research was carried out were included in the study. The hospital defines high-risk pregnancy as the presence of obstetric or clinical diseases, such as: hypertensive syndromes, diabetes, problems with uterine growth and amniotic fluid volume, preterm labor, prolonged pregnancy, hemorrhages, infectious diseases, renal, hepaticand circulatory system diseases, thyroid disorders, and autoimmune diseases, among others.
Women under 19 years of age, and/or with twin or ectopic pregnancy, or with a diagnosis of molar pregnancy were excluded. Adolescents were excluded due to the need for family authorization to participate in the research, as they could have dietary characteristics particular to adolescence that would influence the definition of patterns related to adult pregnant women,in addition to requiring specific anthropometric assessment, as well as in casesof twin pregnancies. Ectopic and molar pregnancies, as they are non-viable conditions, would involve changes in prenatal care. There were no refusals by the pregnant women. Thus, 200 pregnant women (N=200) of different gestational ages participated in the study.
The data were collected by trained interviewers, two nutritionists and a nutrition student. The training was carried out by the research coordinator, aiming to standardize the technique of data collection and filling out the questionnaires, reducing information bias.
Initially, through documental search in the patient’s medical record and maternal card, the data were recorded in a standardized structured questionnaire for socioeconomic variables and prenatal care. Subsequently, until the second day of the immediate postpartum period, the participants answered questions related to dietary recommendations during prenatal consultations; and a Quantitative Food Frequency Questionnaire (QFFQ) was applied regarding their diet during pregnancy.
15,16The socioeconomic variables (age, level of schooling, years of schooling, family income, marital status and parity) were collected from the medical records and used to characterize the sample and Poisson regression adjustment. Age was categorized into: “≤35 years old” (No risk), “>35 years old” (At risk).
5The level of schooling was assessedas years of schooling and grouped for statistical analysis into the following categories: “≤9 years of schooling”, “>9 years of schooling”. Marital status was organized into the categories: “with a partner” (married, stable union) and “without a partner” (single, widowed, divorced). Family income in multiples of minimum wages received by all family members residing in the household (MW = R$724.00 in 2014) was categorized into: “≤ 3 MWs and “>3 MWs”. Parity was analyzed regarding the number of children and pregnant women were categorized as: “nulliparous” (no children) and “multiparous” (having one or more children).
The prenatal care variables comprised gestational age at the beginning of prenatal care, number of prenatal consultations and recommendations on nutrition. The gestational age at the beginning of prenatal care and the number of prenatal consultations were collected from the prenatal care card.
For statistical analysis, the gestational age at the beginning of prenatal care was collected and the pregnant women were grouped by dividing those who started prenatal care during the first trimester
1,6 "≤13 weeks" and after the first trimester ">13 weeks”. As for the number of prenatal consultations, the categories “<6 consultations” and “≥6 consultations” were created.
6The variable “recommendations on prenatal nutrition” was created in response to the question “Did you receive any dietary recommendationsduring the prenatal consultations?”. This variable was dichotomized into having received dietary recommendationsduring the prenatal consultations (yes or no). If the answer was yes, they were also asked “What were the recommendations?”
Food data were obtained through the application of a QFFQ developed and validated for pregnant women users of the Basic Health Units in Ribeirão Preto, São Paulo.
15,16 The relative validation study concluded that the QFFQ is an adequate method for categorizing the estimation of nutrients intoconsumption quartiles, as most nutrients had 70% or more of the pregnant women categorized in the same quartile or adjacent quartile.
16The instrument contained 85 food items and was related to food consumption during pregnancy. The QFFQ included the consumption frequency, time unit and portion size. The daily frequency of consumption, the dietary variable used in the analysis of the derivation of dietary patterns, was obtained from the reported food consumption frequency, multiplying the number of times the food was consumed (N) by the unit of time (U). The N in the QFFQ ranges from 0 to 10, and the time unit is a day, a week and a month.
15,16Although some foods were grouped in the QFFQ, when asked to the patients, the women specified which food had been consumed and, for the analysis of dietary pattern identification, were considered separately,such as whole milk, skim milk; fried or boiled cassava; fried or boiled potato; fried, grilled, or ground beef; pork shank, sausage; boiled, or fried egg, omelet.
In addition to these items, 14 types of foods (couscous, tapioca, brown sugar, kiwi, dry soupmix, cooked lamb, oats, linseed, sushi, pancakes,
baião de dois, eggplant, manioc flour, granola) were also included in the analysis of the derivation of the dietary patterns, as they were mentioned in the answer to the final question of the QFFQ that allowed reporting the consumption of other foods that were not included in the list.
The dietary variable used in the analysis of the derivation of dietary patterns was the daily frequency of consumption. To identify the dietary patterns, the 105 food items, including the initial 85 items of the QFFQ, added to the foods mentioned at the end of the questionnaire and those that were broken down, were arrangedin groups, according to their nutritional composition. Three food items (sushi, pancakes and
baião de dois) consumed by only 0.5% of the sample were excluded, and the items mentioned by at least 80% of the participants (white bread, white rice, cooked beans) were kept separate. Thus, the 102 food items were arrangedin 29 groups, considering the nutritional composition and characteristics of the foods (Table 1).
For the identification of the dietary patterns, the exploratory factor method using the principal components analysis (PCA) was used, followed by the Varimax orthogonal rotation.
The methods used to assess whether the data were adequate for carrying out the factor analysis were the Kaiser-Meyer-Olkin (KMO) coefficient, using values ≥ 0.6 as the cutoff point and the Bartlett’stest of sphericity (BTS), with a value of
p≤0.05.
The amount of retained factors was defined by three criteria: components with eigenvalues >1.0, point with the highest slope of the scree plot and the subjective interpretation of the conceptual meaning of the identified dietary patterns.
17The components were interpreted through the factor loadings, which are the correlation coefficients between the dietary variables and the factors. Factor loadings ≥ 0.3 or ≤ -0.3 were considered important contributions to the pattern.
18 When the loads are positive, there is a direct association of the food item with the factor, that is, greater consumption of the food; when they are negative, there is an inverse association, that is, lower consumption of that food.
18The main components were named according to the nutritional composition of the food items retained in each factor, in addition to checking in the literature the names used for patterns with similar composition. Each assessed pregnant woman received a score for each factor that was retained. Subsequently, the factorial scores of each dietary pattern were categorized into quartiles, with the upper quartile of the distribution representing greater adherence to the pattern. The program used to perform the statistical analyses was the STATA software, version 10.0.
First, a descriptive analysis of the socioeconomic variables (age, level of schooling, marital status, family income, parity) and prenatal care (gestational age at the beginning of prenatal care, dietary advice in prenatal consultations and number of prenatal consultations) was carried out.
Poisson regression with robust variance estimation was used to estimate the prevalence ratios (PR) between the independent variables (number of prenatal consultations, dietary advice in prenatal consultations, gestational age at the start of the prenatal care)and the dependent variables (dietary patterns).
Initially, a bivariate analysis was performed between each independent variable and each identified dietary pattern. Then, for each identified dietary pattern (dependent variable), a multivariate analysis was performed, in which all independent variables were included in the model, as well as adjustment for socioeconomic variables (age, level of schooling, marital status, family income, parity). The dependent variables, i.e., food consumption patterns, were classified as dichotomous: low adherence (1
st, 2
nd and 3
rd quartiles) and high adherence to the pattern (4
th quartile).
Estimates were calculated by points and by 95% confidence intervals (CI95%), with the significance level being set at 5%. The study was approved by the Research Ethics Committee of Universidade Estadual do Ceará (n. 388.016).
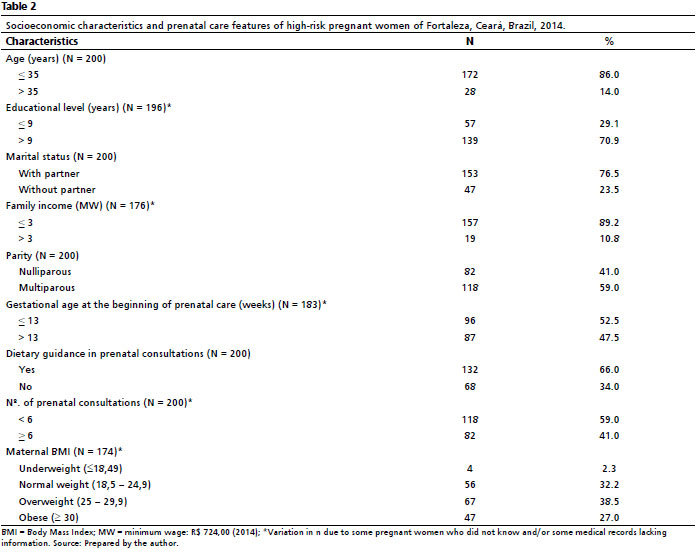
ResultsMost (86.0%) of the pregnant women were 35 years old or younger, lived with a partner (76.5%) and were multiparous (59.0%). Maternal age ranged from 19 to 45 years and the median was 27.5 years. The majority (70.9%) had more than nine full years of schooling, but only 10.8% had a family income above three minimum wages (Table 2).
The clinical diagnoses, as they were not mutually exclusive, admit that each pregnant woman could have more than one pathology that classified her as being at high risk. On hospital admission, hypertensive syndrome was the most frequent pathology (60.5%), followed by PROM (24.5%) and alterations in amniotic fluid volume (13.5%).
The gestational age at the start of prenatal care ranged from 3 to 38 gestational weeks and the median was 15.34 gestational weeks. An average of 4.64 prenatal consultations were performed (SD = 2.53), ranging from none to a maximum of nine consultations. During the follow-up consultations carried out in the prenatal period, most pregnant women (66.0%) received dietary advice (Table 2), and 65.9% (N=54) of them had more than six consultations.
The KMO coefficient (0.63) and Bartlett’s test of sphericity (
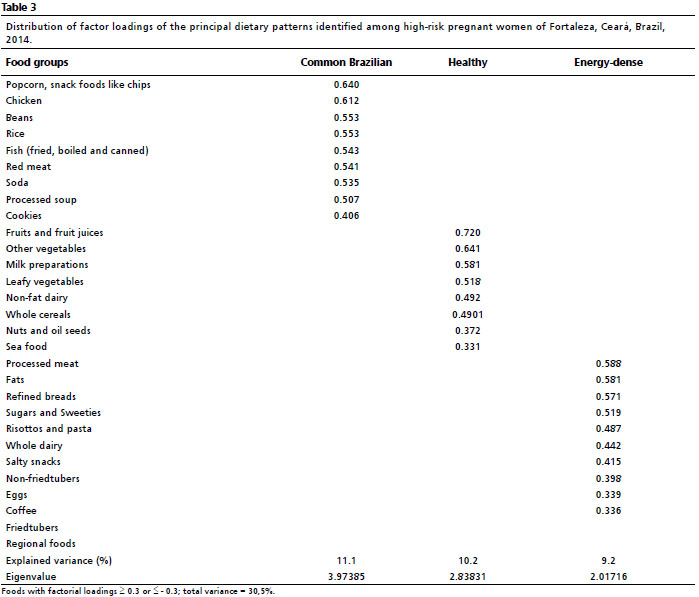
p<0.01) indicated satisfactory confidence for carrying out the factor analysis. Ten factors with eigenvalues ≥ 1.0 were retained and the inflection of the scree plot indicated three factors that, after the analysis of the conceptual meaning, were retained and explained 30.5% of the total variance. Only these three retained patterns had eigenvalues ≥ 2.0 (Table 3).
The dietary patterns were defined as follows: ‘common Brazilian’ (popcorn and chips, chicken, beans, rice, fish, beef, soft drinks, industrialized soups, cookies); ‘healthy’ (fruits and fruit juices, other vegetables, dairy foods, leafy vegetables, low-fat dairy products, whole grains, nuts, seafood); and ‘energy-dense’ (processed meats, fats, refined flour breads, sugar and sweets, risottos and pasta, full-fat dairy products, savory foods, non-fried tubers, eggs, coffee). The Brazilian common pattern explained most of the variance (11.1%) (Table 3).
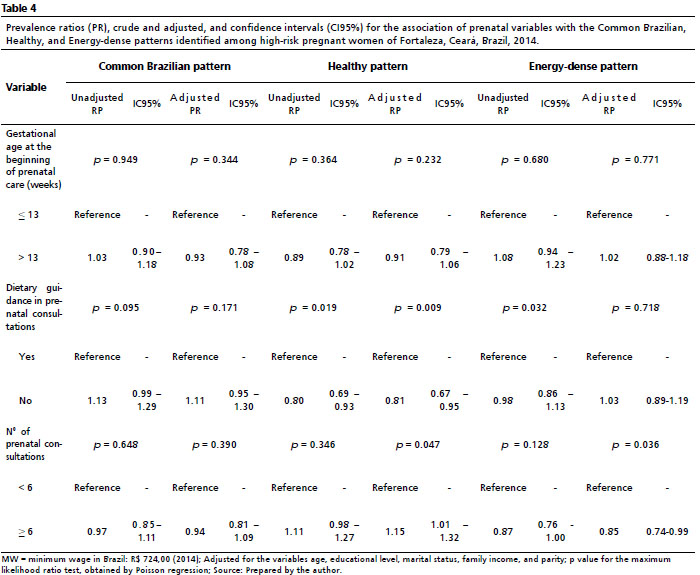
The analyses were performed without adjustment (bivariate) and with adjustment (multivariate), demonstrating that only the independent effects remained in the model (Table 4).
The multivariate analysis, adjusted for the socioeconomic variables, disclosed a significant association with the number of prenatal consultations and dietary advice during prenatal consultations. Pregnant women who did not receive dietary recommendationsduring the prenatal consultations had a lower chance of adherence to the healthy pattern (PR= 0.81; CI95%= 0.67-0.95). The pregnant woman who had an adequate number of prenatal consultations1 (≥6) showed greater adherence to the 'healthy' pattern (PR= 1.15; CI95%= 1.01-1.32) and lower adherence to the ‘energy dense’pattern (PR=0.85; CI95%=0.74-0.99) (Table 4).
DiscussionThree main dietary patterns were identified among the 200 high-risk pregnant women included in the study, namely ‘common Brazilian’, ‘healthy’ and ‘energy-dense’. This is the first study, in the searched literature, that identified dietary patterns in a specific group of pregnant women classified as high risk in Brazil. Prenatal characteristics were associated with the ‘healthy’ and ‘energy-dense’food patterns, but not with the ‘common Brazilian’ one.
The variance explained by these factors (30.5%) was close to the values found in other studies that maintained three dietary patterns, which ranged from 25.8%
12 to 36.1%.
13 The proportion of the variation explained by a set of components depends on the number of variables that entered the principal components analysis and on the number of retained components, and should be compared through the literature with caution, since there are methodological differences between the studies.
19The ‘common Brazilian’ dietary pattern, which explained the highest percentage of variance, consisted of foods typical of the diet of the Brazilian population, as observed by Hoffmann
et al.,
20 Vilela
et al.,
13 Castro
et al.
21 and Ternus
et al.
12 Brazilian meals usually include rice and beans, beef or chicken, and an artificial juice.
20 The pattern found in this study includes some foods that do not fit into the traditional Brazilian diet, representing a modern and more current diet of Brazilian individuals, so the common denomination was more appropriate.
A dietary pattern with similar composition and the same denomination “common-Brazilian” was found in a study carried out with women in the pre-gestational period.
13 Dietary patterns with similar characteristics called “traditional pattern” were also found in menopausal women;
20 “traditional Brazilian” in pregnant women in Ribeirão Preto, state of São Paulo;
22”Brazilian” in adult women from São Leopoldo, state of Rio Grande do Sul;
12 and “mixed” in a study carried out with puerperal women in the city of Rio de Janeiro, state of Rio de Janeiro,
21indicating a national habit associated with the pregnant women’s food consumption.
The ‘healthy’ pattern has healthy foods in its composition with a lower level of processing, such as fruits, vegetables and whole grains, similar to other patterns reported in the literature with the same name, in Portuguese
12,22and in English.
21 Another study with pregnant women
23 identified a pattern with a different composition that was called “healthier” (“healthierdietary pattern”). The presence of this pattern shows adherence to healthier and essential eating behaviors during pregnancy and other life cycles.
The ‘energy-dense’ pattern was so named because it has several foods with high energy density, rich in simple carbohydrates, sugar and fat in their composition. This dietary pattern is similar to the “processed” pattern mentioned in a national study
13 and to the “risk” pattern of another Brazilian study.
12In the study carried out by Zuccolotto et al.
22, two dietary patterns called “snacks” and “coffee” were identified, which combined have characteristics that are similar to our “energy-dense” pattern. This pattern characterizes adherence to a diet associated with the presence of obesity and chronic diseases in all studied groups.
These variations in the names and the food items that constitute the patterns can be explained by the subjective decisions that must be made to carry out the analysis,
24 which include choosing the most appropriate method, the decision to group food items, the ideal treatment of variables that will be used (frequency of consumption, gram/mL, % calories), the number of factors retained, the value from which factor loadings are considered important, and the designation of the patterns.
24In the present study, high-risk pregnant women who did not receive dietary advice during prenatal care consultations had lower adherence to the ‘healthy’ pattern. Moreover, those who received an adequate number of prenatal consultations showed lower adherence to the ‘energy-dense’ pattern. Only the ‘common Brazilian’ pattern was not associated with any of the investigated prenatal characteristics.
These findings reinforce the importance of having pregnant women attend adequate prenatal care, and receivingrecommendations on healthy eating,
25 since it is during pregnancy that women are more concerned with diet and food options.
26 Thus, pregnancy is the ideal period for encouraging healthy habits, and frequent prenatal follow-up consultations allow the health professionals to constantly reinforce the importance of thesechanges.
27In an international cohort,
28 carried out in the North Carolina region, with pregnant women in the second trimester of pregnancy, birth outcomes showed that greater adherence to a healthy dietary pattern reduced the chances of preterm birth. While greater adherence to a poorer quality dietary pattern increased the chances of preterm birth.
28 Therefore, the quality of the diet is an important modifiable risk factor that can be a useful tool in dietary interventions and strategies aimed at improving childbirth outcomes.
28Therefore, encouraging changes in the diet, aiming at healthy eating habits, such as moderately increasing the consumption of vegetables and foods of plant origin, in addition to their low cost and low risk, can bring benefits to the health of the mother and the fetus.
26The Brazilian Ministry of Health advises that pregnant women should reduce the consumption of foods rich in fat, because when consumed in excess, they are associated with the development of obesity, hypertension and heart disease.
1,7Additionally, they should reduce the intake of sugars and sweets, since their frequent consumption increases the risk of complications such as excess weight gain, obesity, gestational diabetes and hypertension. Sodium consumption should also be reduced, as its excessive intake increases the risk of hypertension, heart and kidney disease, in addition to increasing edema.
1,7 These recommendations suggest that pregnant women should avoid consuming foods that have the characteristics of the ‘energy-dense’ dietary pattern, identified in the present study, aiming to prevent complications during pregnancy.
A study carried out with Norwegian pregnant women, aimed to estimate the association between dietary patterns during pregnancy and the risk of developing preeclampsia, found that a dietary pattern characterized by a high intake of vegetables and vegetable oils, and a low intake of processed meats and sweet drinks can be beneficial.
26Pajunen
et al.
23 found associations between a gestational dietary pattern characterized by the intake of vegetables and rye bread, and a lower risk of gestational diabetes mellitus,whereasthe consumption of a pro-inflammatory diet was associated with a higher risk of gestational diabetes. Therefore, the authors recommend encouraging the consumption of diets that include vegetables and rye bread.
A study of Iranian pregnant women showed an inversely significant association between a healthy dietary pattern (leafy vegetables, legumes, fruits, low-fat dairy products, poultry, beef, citrus fruits, nuts, fish, olives, marinades, sweet fruits, eggs and unsaturated fat) and the risk of having preeclampsia.
29Additionally, a higher chance of developing preeclampsia was observed among pregnant women with greater adherence to the western dietary pattern, characterized by processed meats, fruit juice, citrus fruits, nuts, fish, desserts and sweets, sugar, saturated fat, fruits with high glycemic index, potatoes, legumes, coffee, eggs, pizza, high-fat dairy products, whole grains, and soft drinks.
29In Brazil, performing a more complete nutritional assessment and providing dietary recommendationsduring the prenatal follow-up consultations, is not yet a routine procedure. Although the Ministry of Health recommends this practice, health professionals, who are not specialists in nutrition, generally do not understand all the factors that influence eating habits during pregnancy, which results in variations in the dietary advicegiven to pregnant women.
30Nevertheless, the dietary advice given by non-specialized professionals was important in the present study. Most pregnant women received recommendations on nutrition during prenatal consultations. However, the minority attended an adequate number of consultations, which was associatedwith greater adherence to the ‘healthy’ pattern. Therefore, the importance of effective public policies is reinforced, by promoting the training of the health team to carry out nutritional education actions directed at women and pregnant women, aiming to promote healthy eating practices.
25The number of prenatal consultations can be considered a limitation of the present study. Although all pregnant women were evaluated in the immediate postpartum period, the number of prenatal consultations may vary, since some women had a preterm birth, which already implies a lower number of consultations, and also prolonged pregnancy, which may have resulted in a greater number of consultations. However, the categorization into fewer than six and six consultations or more was able to minimize the possible differences in the number of prenatal consultations.
The use of the QFFQ also has limitations, considering that the pregnant women’s answers could be influenced by the dietary advice they received during pregnancy, hiding information or modifying their actual dietary pattern. Therefore, the interviewers were trained to reinforce at the beginning and throughout the application of the QFFQ that they should mention what they had actually consumed.
This study used a validated food frequency questionnaire for pregnant women from another region of the country, since there is no validated QFFQ for pregnant women in the Northeast region. The choice of this QFFQ was due to the fact that the instrument permits the inclusion of other foods that are frequently consumed, allowing the addition of foods that are typically consumed in the region, reducing this bias of the validation site. We believe itminimized the effects caused by this instrument when it was decided to use the frequency of food consumption for the principal components analysis, rather thanusing grams/mL or caloric percentage, since the data of the consumed portions could be over- or underestimated.
Another limitation is related to the ability to use the QFFQ to identify dietary patterns in pregnancies of different durations.A longitudinal study detected dietary patterns in Spanish women, in the pre-gestational period, at four different moments during pregnancy, and six months after childbirth. As the patterns did not show significant changes over time, the authors concluded that the information on food consumption obtained at any time during pregnancy can provide reliable information on a common dietary pattern throughout the gestational period.
28 Thus, it is believed that the dietary patterns obtained in this study, even in pregnant women with different gestational ages, reflect the diet of these women throughout the gestational period, since the QFFQ used in the study is related to food habits throughout pregnancy.
The results of this study reinforce the information found in the literature regarding the importance of performing adequate prenatal care and having healthy eating habits. However, the dietary patterns found in the study are only representative of the assessed women population, and not of all high-risk pregnant women in Fortaleza, Ceará. Additionally, these results are the justification for health professionals to provide adviceto pregnant women about healthy eating, since those who did not receive these recommendations had a lower chance of adhering to the healthy pattern.
Three dietary patterns were identified: ‘common Brazilian’, ‘healthy’ and ‘energy-dense’. It was observed that high-risk pregnant women who had an adequate number of consultations during prenatal care had a greater chance of adhering to the healthy pattern and a lower chance of adhering to the energy-dense pattern. Not receiving dietary recommendationsduring prenatal care was inversely associated with the healthy pattern. Thus, the number of prenatal consultations, as well as the dietary advice, were able to improve the diet of the assessed pregnant women, reinforcing the importance of receiving adequate prenatal care for high-risk pregnant women.
AcknowledgementsWe would like to thank Fundação Cearense de Apoio ao Desenvolvimento Científico e Tecnológico (FUNCAP), through the Young Researchers Program (PJP), Notice 07/2012, for the financial support.
References1. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. Departamento de Ações Programáticas. Manual de Gestação de Alto Risco [
Internet]; Brasília (DF): Ministério da Saúde (BR); 2022. [access in 2022 abr 2]. Available from:
https://portaldeboaspraticas.iff.fiocruz.br/wp-content/uploads/2022/03/manual_gestacao_alto_risco.pdf2. World Health Organization (WHO). Managing complications in pregnancy and childbirth: a guide for midwives and doctors. 2
nd ed. Geneva: WHO; 2017. [access in 2020 abr 15]. Available from:
https://apps.who.int/iris/handle/10665/2557603. Renault KM, Carlsen EM, Nørgaard K, Nilas L, Pryds O, Secher NJ,
et al. Intake of carbohydrates during pregnancy in obese women is associated with fat mass in the newborn offspring. Am J Clin Nutr. 2015; 102 (6): 1475-81.
4. Das JK, Lassi ZS, Hoodbhoy Z, Salam RA. Nutrition for the Next Generation: Older Children and Adolescents. Ann Nutr Metab. 2018; 72 (Suppl. 3): 56-64.
5. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Gestação de alto risco: manual técnico. 5
a ed. Brasília (DF): Ministério da Saúde; 2012. [access in 2020 abr 15]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_tecnico_gestacao_alto_risco.pdf6. Medeiros FF, Santos IDL, Ferrari RAP, Serafim D, Maciel SM, Caardelli AAM. Acompanhamento pré-natal da gestação de alto risco no serviço público. Rev Bras Enferm. 2019; 72 (Suppl. 3): 213-20.
7. Ministério da Saúde (BR); Sociedade Beneficente Israelita Brasileira Albert Einstein. Nota técnica para organização da rede de atenção à saúde com foco na atenção primária à saúde e na atenção ambulatorial especializada: saúde da mulher na gestação, parto e puerpério; 2019. [access in 2020 abr 15]. Available from:
https://pesquisa.bvsalud.org/portal/resource/pt/biblio-12233748. Chen Z, Du J, Shao L, Zheng L, Wu M, Ai M,
et al. Prepregnancy body mass index, gestational weight gain, and pregnancy outcomes in China. Int J Gynecol Obstet. 2010 Abr; 109 (1): 41-4.
9. Arkkola T, Uusitalo U, Kronberg-Kippilä C, Männistö S, Virtanen M, Kenward MG,
et al. Seven distinct dietary patterns identified among pregnant Finnish women - Associations with nutrient intake and sociodemographic factors. Public Health Nutr. 2008; 11 (2): 176-82.
10. Chen X, Zhao D, Mao X, Xia Y, Baker PN, Zhang H. Maternal Dietary Patterns and Pregnancy Outcome. Nutrients. 2016 Jun; 8 (351):1-26.
11. Wirfalt E, Drake I, Wallstrom P. What do review papers conclude about food and dietary patterns. Food Nutr Res. 2013; 57: 20523.
12. Ternus DL, Henn RL, Bairros F, Costa JS, Olinto MTA. Padrões alimentares e sua associação com fatores sociodemográficos e comportamentais: Pesquisa Saúde da Mulher 2015, São Leopoldo (RS). Rev Bras Epidemiol. 2019; 22: e190026.
13. Vilela AMF, Farias DR, Eshriqui I, Vaz JS, Franco-sena AB, Castro MBT,
et al. Prepregnancy Healthy Dietary Pattern Is Inversely Associated with Depressive Symptoms among Pregnant Brazilian Women. J Nutr. 2014 Oct; 144 (10): 1612-8.
14. Cunha CML, Canuto R, Rosa PBZ, Longarai SL, Schuch I. Associação entre padrões alimentares com fatores socioeconômicos e ambiente alimentar em uma cidade do Sul do Brasil. Ciênc Saúde Colet. 2022; 27 (2): 687-700.
15. Oliveira T, Marquitti FD, Carvalhaes MABL, Sartorelli DS. Desenvolvimento de um questionário quantitativo de freqüência alimentar (QQFA) para gestantes usuárias de unidades básicas de saúde de ribeirão Preto, São Paulo, Brasil. Cad Saúde Pública. 2010; 26 (12): 2296-306.
16. Barbieri P, Nishimura RY, Crivellenti LC, Sartorelli DS. Relative validation of a quantitative FFQ for use in Brazilian pregnant women. Public Health Nutr. 2013; 16 (8): 1419-26.
17. Hongyu K, Federal U, Grosso M, Grosso M, Chave P. Análise Fatorial Exploratória: resumo teórico, aplicação e interpretação. Eng Sci. 2018; 4 (7): 88-103.
18. Jayasinghe SN, Breier BH, Mcnaughton SA, Russell AP, Gatta PA Della, Mason S,
et al. Dietary Patterns in New Zealand Women: Evaluating Differences in Body Composition and Metabolic Biomarkers. Nutrients. 2019; 21 (1643): 1-17.
19. Crozier SR, Robinson M, Godfrey KM, Cooper C, Inskip HM. Women’ s dietary patterns change little from before to during pregnancy. J Nutr. 2009 Oct; 139 (10): 1956-63.
20. Hoffmann M, Mendes K, Canuto R, Garcez A. Padrões alimentares de mulheres no climatério em atendimento ambulatorial no Sul do Brasil. Ciênc Saúde Colet. 2015; 20 (5): 1565-74.
21. Castro MBT, Sichieri, Rosely Brito FSB, Nascimento S, Kac G. Un patrón dietético mixto se asociaconun menor declive enel cambio del peso corporal durante elpuerperioen una cohorte de mujeresbrasileñas. Nutr Hosp. 2014; 29 (3): 519-25.
22. Zuccolotto DCC, Crivellenti LC, Franco LJ, Sartorelli DS. Padrões alimentares de gestantes, excesso de peso materno e diabetes gestacional. Rev Saúde Pública. 2019; 53: 52.
23. Pajunen L, Korkalo L, Koivuniemi E, Houttu N, Pellonperä O, Mokkala K. A healthy dietary pattern with a low inflammatory potential reduces the risk of gestational diabetes mellitus. Eur J Nutr. 2022; 61 (3): 1477-90.
24. Hearty ÁP, Gibney MJ. Comparison of cluster and principal component analysis techniques to derive dietary patterns in Irish adults. Br J Nutr. 2009; 101 (4): 598-608.
25. Niquini RP, Bittencourt SA, Lacerda EM de A, Saunders C, Leal MC. Avaliação do processo da assistência nutricional no pré-natal em sete unidades de saúde da família do município do Rio de Janeiro. Ciênc Saúde Colet. 2012; 17 (10): 2805-16.
26. Brantsæter AL, Haugen M, Samuelsen SO, Torjusen H, Trogstad L, Alexander J,
et al. A dietary pattern characterized by high intake of vegetables, fruits, and vegetable oils is associated with reduced risk of preeclampsia in nulliparous pregnant Norwegian Women. J Nutr. 2009; 139 (6): 1162-8.
27. Rayburn WF, Phelan ST. Promoting healthy habits in pregnancy. Obstet Gynecol Clin North Am. 2008; 35 (3): 385-400.
28. Martin CL, Sotres-Alvarez D, Siega-Riz AM. Maternal dietary patterns during the second trimester are associated with preterm birth. J Nutr. 2015; 145 (8): 1857-64.
29. Hajianfar H, Esmaillzadeh A, Feizi A, Shahshahan Z, Azadbakht L. The association between major dietary patterns and pregnancy-related complications. Arch Iran Med. 2018; 21 (10): 443-51.
30. Hoffmann JF, Nunes MAA, Schmidt MI, Olinto MTA, Melere C, Ozcariz SGI,
et al. Dietary patterns during pregnancy and the association with sociodemographic characteristics among women attending general practices in southern Brazil: the ECCAGe Study. Cad Saúde Pública. 2013; 29 (5): 970-80.
Received on May 21, 2020
Final version presented on June 11, 2022
Approved on July 14, 2022
Authors’ contribution: Cruz IFS, Maia CSC, Arruda SPM and Azevedo DV contributed to the article conception and study design. Cruz IFS, Carvalho NS and Arruda SPM were responsible for data analysis and interpretation. Statistical analysis was performed by Arruda SPM. Cruz IFS and Oliveira DL performed the data collection. Cruz IFS and Maia CSC wrote the manuscript. Cruz IFS, Azevedo DV, Arruda SPM and Maia CSC reviewed the manuscript. All authors approved the final version of the article, are publicly responsible for its content and declare that there are no conflicts of interest related to the study.


 ; Denise Fernandes Lima de Oliveira2
; Denise Fernandes Lima de Oliveira2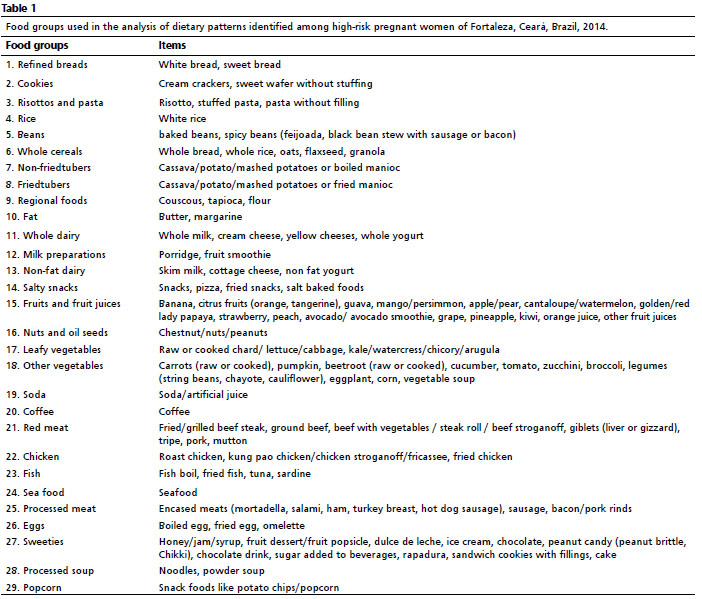






 Ler em português
Ler em português