ABSTRACT
OBJECTIVES: microbiological quality of raw human milk (HM) from donors at the HMB (Human Milk Bank) of Santa Casa de Misericórdia de Ouro Preto was evaluated.
METHODS: the microbiological quality of milk from each of 10 donors in triplicate (30 samples) was evaluated by enumeration of Staphylococcus aureus and total aerobic mesophiles (surface plating) and total and thermotolerant coliforms (Most Probable Number - MPN). A questionnaire and a checklist were applied after the end of sample collection to verify the compliance of milk extraction and storage procedures by the donors.
RESULTS: inadequacies in the procedures for expression and storage of donated HM were observed. The presence of all microorganisms studied were verified in the milk of all donors, and in some cases exceeded the safety limits. The checklist indicated that some necessary hygienic-sanitary procedures were not carefully performed, making it important to properly guide the donors.
CONCLUSIONS: this study points to an unfavorable scenario for the safety and quality of donated HM, and it is important to encourage further studies to be conducted so that the Brazilian network of HMB adopts stricter criteria for instructions on procedures and support for HM donors.
Keywords:
Donor, Food microbiology, Human milk, Milk banks, Quality control
RESUMO
OBJETIVOS: avaliou-se a qualidade microbiológica do leite humano (LH) cru de doadoras do Banco de Leite Humano (BLH) da Santa Casa de Misericórdia de Ouro Preto.
MÉTODOS: a qualidade microbiológica do leite de cada uma das 10 doadoras em triplicata (30 amostras) foi avaliada por meio da enumeração de Staphylococcus aureus e mesófilos aeróbios totais (plaqueamento em superfície) e coliformes totais e termotolerantes (Número Mais Provável - NMP). Para verificar a conformidade dos procedimentos de extração e armazenamento do leite pelas doadoras, aplicou-se um questionário e um checklist após o término da coleta das amostras.
RESULTADOS: observou-se inadequações nos procedimentos de expressão e armazenamento do LH doado. A presença de todos os microrganismos estudados foram verificados no leite de todas as doadoras e, em alguns casos, excedeu os limites de segurança. O checklist indicou que alguns procedimentos higiênico-sanitários necessários não foram realizados criteriosamente, tornando importante orientar adequadamente as doadoras.
CONCLUSÕES: este estudo aponta um cenário desfavorável para a segurança e a qualidade do LH doado, sendo importante incentivar mais estudos a serem realizados para que a rede brasileira de BLH adote critérios mais rigorosos de instruções sobre procedimentos e suporte para doadoras de LH.
Palavras-chave:
Doadora, Microbiologia de alimentos, Leite humano, Bancos de leite, Controle de qualidade
IntroductionHuman milk has antimicrobial properties that delay the spoilage caused by primary microbiota, however, it has little efficacy against secondary contaminants from the environment, kitchenware, and mothers.
1 As it is rich in nutrients, it is an excellent culture medium for the growth of several microorganisms, therefore, HM must be handled in hygienic-sanitary conditions to prevent its microbiological contamination.
2According to Grazziotin
et al.,
3 the number of samples of HM that are discarded in HMB is still quite high, possibly because of errors that occur in the manipulation and processing steps that result in microbiological contamination. The causes behind the increase in the quantity of microorganisms in HM may be related to improper hygiene conditions of the donor, the environment, and utensils; inadequate expression techniques; and maintaining milk outside the cold chain during its transport.
In Brazil, as in other countries, the expression of HM in the donor’s home is permitted and encouraged, being regarded as a safe and effective way to obtain higher milk volumes.
4 According to the World Health Organization
5 the feeding of preterm infants with mother’s own milk is recommended as the first choice and if this is not available pasteurized donated HM from an established milk HMB should be the next alternative. Thus, a higher donor registration is ensured and, consequently, greater donation of HM that can meet the needs of Neonatal Intensive Care Units, which, in addition to special care, provides preterm and/or diseased newborns with HM which will guarantee the important benefits of this nourishment.
6It is important to emphasize that milk expression at home should be performed in an environment that does not entail risk to the microbiological and nutritional quality of the milk, and the mother should follow the guidelines conveyed by the HMB team of her city to clean and disinfect utensils, for personal hygiene, expression, and storage.
7,8 HM expressed in the household of the donor is forwarded to the HMB for its processing under a controlled transport chain at low temperatures, according to established technical standards.
4The exposure of newborns to pathogenic bacteria present in HM, such as Staphylococcus aureus, can cause diarrheal diseases, neonatal sepsis, meningitis, and necrotizing enterocolitis.
9 Moreover, the growth of other bacteria in milk leads to acidification and fermentation, which may reduce wthe nutritional and immunological components due to the use of milk nutrients by contaminating microbiota.
3,10,11Accordingly, the objective of this study was to evaluate the microbiological quality of raw HM from donors of the
Santa Casa de Misericórdia Hospital in Ouro Preto. This study is highly relevant because it reveals the hygienic-sanitary quality profile of the donors through a microbiological evaluation of their milk, verifying if they follow the correct expression procedures that were properly oriented by professionals of the HMB. According to the results obtained, if necessary, the HMB may adopt more efficient protocols for training and awareness of donors, improving the quality of the milk received, and consequently, the safety for the children who will receive it.
MethodsThe study was carried out with the participation of all donors registered at the HMB of
Santa Casa de Misericórdia de Ouro Preto. Participants (10) were recruited by telephone contact, after being approved by the Research Ethics Committee of the Federal University of Ouro Preto, under the number CAAE 71251517.9.0000.5150.
The participating women who provided their breast milk gave their consent for it to be used, signing a free and informed consent form (ICF) and were characterized by means of a structured applied questionnaire and a checklist of procedures for milk expression, prepared by professionals from the HMB of
Santa Casa de Misericórdia de Ouro Preto, in order to verify the adequacy of nursing mothers in relation to the expression and storage procedures of HM that are recommended by the Ministry of Health.
4 Importantly, in order not to interfere with the procedures commonly performed by the donors at the moment of expression, the questionnaire and the checklist were applied immediately after the last milk expression.
Immediately upon arrival of the milk at the laboratory, the samples were individually analyzed for
Staphylococcus aureus, total and thermotolerant coliforms, and total aerobic mesophiles.
4 The results were presented individually in three replicates.
A total of 10 mL of HM of each of the 10 donors was used to perform the analyses. Donors were provided in their household with a previously sterilized wide mouth transparent glass bottle with a screwable plastic cap. On the day of the expression, the bottles containing the HM were transported to the microbiology laboratory of the School of Nutrition of the Federal University of Ouro Preto, in a cool box containing ice to maintain a maximum temperature of 5°C, not exceeding 6 hours as instructed by the HMB.
4The microorganisms
Staphylococcus aureus, total and thermotolerant coliforms, and total aerobic mesophiles were determined according to methods established by Normative Instruction 62, published in 2003 by the Ministry of Agriculture, Livestock and Supply.
12 The Total and Thermotolerant Coliforms were determined by the Most Probable Number (MPN) method.
12ResultsThe characteristics of the donors and their infants are described in Table 1. All lived in the capital of the municipality of Ouro Preto - MG and were in the production phase of mature milk. The age of the donors ranged from 21 to 32 years, with an average of 26.6 years. Regarding education, 50% had complete secondary education and 20% had complete higher education. Regarding employment, 70% of the donors were employed and the most common income range was between 1 and 3 minimum wages (40%). With regard to birth weight, 60% of children were born with adequate weight, i.e., between 3,000 to 3,9999 g and there were no premature births.
13 Regarding the microbiological quality of donated milk, as shown in Table 2, the counts of
Staphylococcus aureus ranged from < 102 and 2.9×104 CFU/mL. The contamination of milk by total and thermotolerant coliforms ranged from < 0.3 to > 103 MPN/mL. The count of total mesophilic aerobes ranged from 0.5×10² to 1.7×104 CFU/mL.
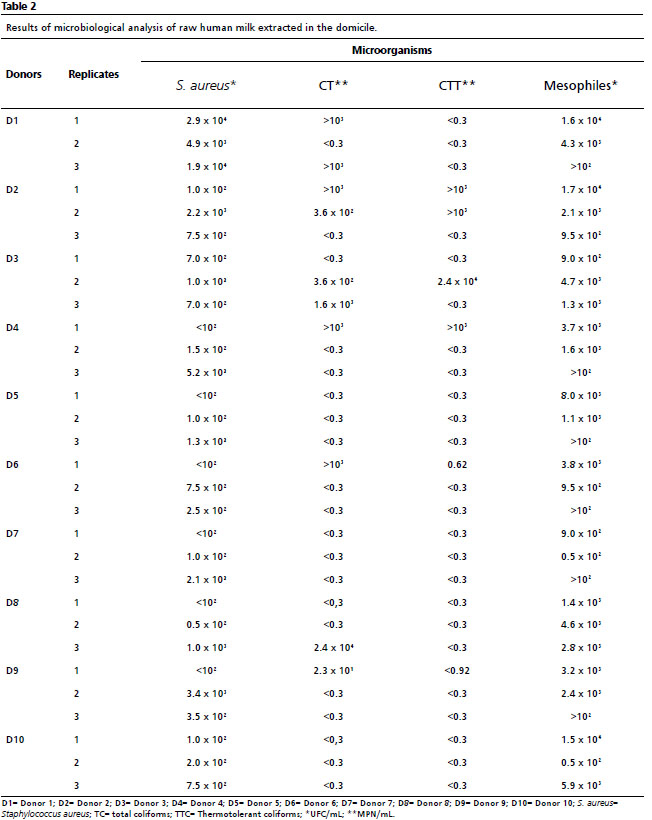
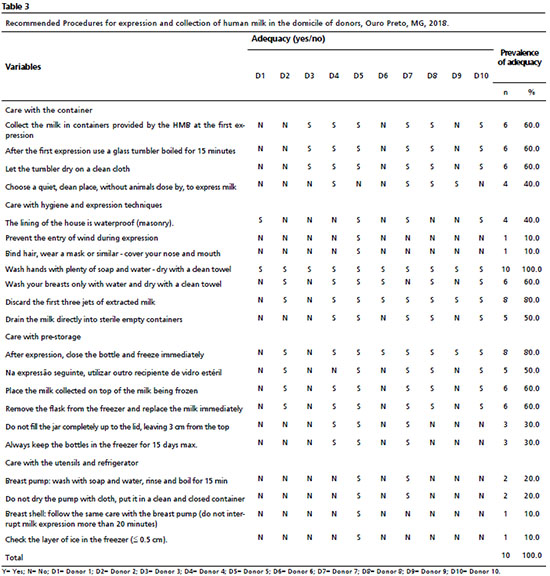
Table 3 presents the prevalence of adequacy of items that compose the checklist applied to the donors. Regarding care with the collection bottle, the item with the highest frequency of inadequacy was “choose a quiet place, clean, without animals around, when extracting the milk” with 40% adequacy. The items referring to hygiene care and milking techniques that presented less frequency of adequacy (10%) were “prevent the influence of wind during expression” and “bind hair, wear a mask or similar - cover nose and mouth”, while 100% of the donors agreed in “washing their hands with plenty of soap and running water - dry with a clean towel”. According to reports about pre-stocking care, although 80% of them affirmed closing the bottle and freezing immediately after expression, 30% affirmed not filling the bottle up to the top and keeping the bottles always in the freezer for a maximum of 15 day.
DiscussionThe quality parameters of the donated HM established by the Ministry of Health in Brazil refer to milk after its pasteurization process and in the absence of a national regulation for raw milk, a comparison with international parameters becomes interesting. According to the Austrian Ministry of Labor and Social Welfare,
14 the count of
Staphylococcus aureus in HM must be <1
4 CFU/mL and contamination above this value was found in a large part of the samples of the present study. Milk donors D1, D4, and D9 showed the highest level of
Staphylococcus aureus contamination (Table 2), and upon analyzing their responses in the checklist (Table 3), none of the three bound their hair, used a mask or similar - covering nose and mouth for milk expression. The lack of these procedures may be associated with the growth and development of the microorganism in HM. Their presence in the milk may be due to contamination by a secondary source, such as nasal passages, throat, skin and hair, common in parts of the human body or even due to unsatisfactory hygienic-sanitary conditions of utensils used in its manipulation.
4,8The greatest concern regarding the presence of these microorganisms at high concentrations in breast milk is the occurrence of toxin-producing strains, called enterotoxins, which are resistant to pasteurization.
15 In this case, heat treatment removes the microorganism, but not the toxin excreted in milk prior to pasteurization. The enterotoxins are thermally stable and resistant to inactivation by gastrointestinal proteases like pepsin and trypsin
16 being a very important property in terms of food poisoning
17 because they retain their biological activity even after pasteurization.
The clinical presentation of staphylococcal food poisoning includes essentially vomiting and diarrhea, and the clinical symptoms manifest after a short incubation period (on average 4 hours). In newborns, due to immunological immaturity, especially those hospitalized in an Intensive Care Unit, enterotoxins are responsible for increasing the time of hospitalization, morbidity, and mortality.
18Currently, there is no universal agreement on the safe upper limit of bacterial load or species in HM, necessitating the establishment of individual microbiological guidelines used by HMB to accept and reject HM. For example, many HMB reject any batch of HM that contains
Staphylococcus aureus or any other toxin-producing bacteria pre-pasteurization.
19 Some HMB, however, accept milk for pasteurization that contains different viable counts of
Staphylococcus aureus such as <103 colony forming unit (CFU)/ mL,
20 <104 CFU/mL
21 or <105 CFU/ mL
22,23 whereas others do not perform bacterial screening on the donated milk.
23The contamination of milk by total and thermotolerant coliforms ranged from < 0.3 to > 103 MPN/mL (Table 2). Milk from donors D2 and D3 showed higher contamination by total and thermotolerant coliforms. It should be noted that these two donors reported not binding their hair, wearing a mask or similar – covering the nose and mouth. In addition, they did not choose a quiet and clean place to express milk (Table 3). Thus, these milk samples pose a risk to the health of the newborn when the milk is not heat-treated (offered directly between mother and child), and it is therefore important to reinforce the guidelines on hygienic-sanitary procedures suitable for handling milk, for their own child or for donation to the HMB, which may be rejected after quality control.
Total coliforms have the ability to ferment lactose at 37°C, with gas production, and are represented by more than 20 species, some found in the gastrointestinal tract of humans and animals.
24 The thermotolerant coliforms, in turn, are characterized by the ability to ferment lactose and produce acid and gas at a temperature of 45°C. The coliforms are important indicators of the microbiological quality of milk donated to the HMB.
25HM is naturally more acidic due to the presence of casein, mineral salts and whey proteins. However, the elevation of this acidity can occur because of the production of lactic acid resulting from the fermentation of lactose by bacterial growth when they find favorable conditions for growth, usually when the milk is stored incorrectly, at temperatures above recommended.
26,27 According to the Manual used by the Brazilian Network of Human Milk Banks: “
Banco de Leite Humano: Funcionamento, Prevenção e Controle de Riscos - The Human Milk Bank: Operation, Prevention and Control of Risks”
4, the presence of coliforms in a sample of raw HM intended for HMB does not require that it be discarded, since this group of microorganisms is eliminated by the pasteurization process. In this case, finding contamination in the milk analyzed in this study does not necessarily imply inadequacy of milk supplied by the HMB, because they are not pasteurized, and will undergo this process in the HMB, inactivating these bacteria. However, if the initial count is very high, there will be a reduction in the microbial load, but many microorganisms will still remain. What should be emphasized is that high scores indicate failures in the expression/hygienization process adopted by donors.
Note that contamination found in raw HM generates a social concern, because the majority of donors work outside the home (70%) and express milk to feed their infants while they are absent. The milk expressed from a mother for her infant does not need to undergo pasteurization but can expose the infants to contamination that generate health risks.
The microbiological quality control of pasteurized HM practiced by HMB, which classifies milk as suitable or unsuitable for consumption, is carried out by the coliform test, being economically viable and safe, minimizing the possibility of false-negative results.
28Regarding total mesophilic aerobes, the majority of donors (D1, D4, D5, D6, D7, and D9) presented high results in at least one of the replicates. In accordance with the Brazilian Network of HMB,
29 when expression is performed in correct hygienic-sanitary conditions, raw HM has a total count of microorganisms in the order of 102 CFU/mL. Serra
et al.
30 found aerobic mesophilic counts ≥105 CFU/mL in their HM samples, above the majority of the values reported in this study, demonstrating even more unsatisfactory hygienic-sanitary conditions.
The Brazilian HMB Network
29 emphasizes that the inadequate hygienization of bottles and pumps for the expression of milk contributes to an increase of up to 3.5×107 CFU/mL in total bacterial counts and contamination with microorganisms such as coliforms. They recommend that in addition to routine personal hygienic care, the nursing mother should be instructed to apply her own milk over the nipple-areolar region after expression, since hindmilk is rich in esters and short chain fatty acids that have a bactericidal function.
29 The results of the present study indicate that the majority of the analyzed samples exceeded safe limits, demonstrating unsatisfactory hygienic-sanitary conditions of the expression, conditioning and storage by donors, requiring the reinforcement of good practices of expression and manipulation.
The results obtained are important not only for the HMB of the city of Ouro Preto, but for the Network of HMB of Brazil, as in the whole world, as it points out an unfavorable scenario for the safety and quality of donated MH, being important to encourage more studies to be carried out so that HMB networks adopt more stringent criteria, which can establish a training and evaluation protocol for procedures that must be followed by donors to ensure the quality of donated milk.
The presence of all the organisms studied was found in the milk samples of all donors and, in some cases, exceeded safe limits. The results of the checklist show that some sanitary-hygienic procedures required are not being performed judiciously, which may be related to the development of the microorganisms found in the samples evaluated. Therefore, it is very important that the professionals of the HMB, responsible for the orientation of the donor, are informed of these facts to reinforce the guidance to donors regarding correct sanitary-hygienic aspects.
References1. Almeida JAG, Novak FR. Amamentação: um híbrido natureza-cultura. J. Pediatr (Rio J.). 2004; 80 (Supl. 5): S119-25.
2. Novak FR, Junqueira AR, Dias MSPC, Almeida JA. Sensorial analysis of expressed human milk and its microbial load. J Pediatr (Rio J.). 2008; 84 (2): 181-4.
3. Grazziotin AL, Grazziotin MCB, Letti LAJ. Disposal of human milk donated to a human milk bank before and after measures to reduce the amount of milk unsuitable for consumption. J Pediatr (Rio J.). 2010; 86 (4): 290-4.
4. Agência Nacional de Vigilância Sanitária (ANVISA). Banco de Leite Humano: Funcionamento, Prevenção e Controle de Riscos. Brasília (DF): ANVISA; 2008. [access in 2020 Mai 18]. Available from:
https://www.anvisa.gov.br/servicosaude/manuais/manual_banco_leite.pdf5. World Health Organization (WHO). Global Strategy for Infant and Young Child Feeding. Geneva: WHO; 2003. [access in 2020 Mai 18]. Available from:
https://www.who.int/publications/i/item/92415622186. Bicalho-Mancini PG, Velásquez-Meléndez G. Exclusive breastfeeding at the point of discharge of high-risk newborns at a Neonatal Intensive Care Unit and the factors associated with this practice. J Pediatr (Rio J.). 2004; 80 (3): 241-8.
7. Agência Nacional de Vigilância Sanitária (ANVISA). Resolução RDC nº 171, de 4 de Setembro de 2006. Dispõe sobre o Regulamento Técnico para o funcionamento de bancos de leite humano. Brasília (DF): DOU de 5 de Setembro de 2006. [access in 2020 Mai 18] Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2006/res0171_04_09_2006.html8. Silva N, Junqueira VCA, Silveira NFA, Taniwaki MH, Gomes RAR, Okazaki MM. Manual de Métodos de Análise Microbiológica de Alimentos e Água. 5
th ed. São Paulo: Livraria Varela; 2010.
9. Haiden N, Ziegler EE. Human Milk Banking. Ann Nutr Metab. 2016; 69 (Supl. 2): 8-15.
10. Borges MS, Oliveira AMM, Hattori WT, Abdallah VOS. Quality of human milk expressed in a human milk bank and at home. J. Pediatr (Rio J.). 2018; 94 (4): 399-403.
11. Novak FR, Cordeiro DMB. The correlation between aerobic mesophilic microorganism counts and Dornic acidity in expressed human breastmilk. J Pediatr (Rio J.). 2007; 83 (1): 87-91.
12. Ministério da Agricultura, Pecuária e Abastecimento (BR). Instrução Normativa nº 62, de 26 de agosto de 2003. Oficializa os métodos analíticos oficiais para análises microbiológicas para controle de produtos de origem animal e água. Brasília (DF): DOU de 18 de Setembro de 2003. [access in 2020 Mai 18] Available from:
https://www.normasbrasil.com.br/norma/instrucao-normativa-62-2003_75166.html13. World Health Organization (WHO). An evaluation of infant growth: the use and interpretation of antropometry in infants. Bull World Health Organ. 1995; 73 (2): 165-74.
14. Austria Federal Ministry of Labour, Social Affairs, Health and Consumer Protection. Leitlinie für Errichtung und Betrieb einer Humanmilchbank. Wien, 2017. [access in 2020 Mai 18]. Available from: HMB_Leitlinie_BMSGPK_CD_2020.pdf
15. Almeida JAG, Novak FR, Almeida CHG, Serva VB. Avaliação da flora microbiana do leite humano ordenhado no IMIP. Rev IMIP. 1998; 03: 13-6.
16. Rall VLM, Vieira FP, Rall R, Vieitis RL, Fernandes Jr A, Candeias JMG,
et al. PCR detection of staphylococcal enterotoxin genes in
Staphylococcus aureus strains isolated from raw and pasteurized milk. Vet Microbiol. 2008 Dec; 132 (3-4): 408-13.
17. Toubar SME, Elbialy AA, Zaky MMM, El-Shafey AA. Prevalence of Staphylococcus aureus in Raw Milk and Some Dairy Products in Port Said Governorate. Amer J Zoo. 2018; 1 (2): 40-6.
18. Pereira VC, Cunha MLRS. Coagulase-negative staphylococci strains resistant to oxacillin isolated from neonatal blood cultures. Mem Inst Oswaldo Cruz. 2013; 108 (7): 939-42.
19. Almutawif Y, Hartmann B, Lloyd M, Lai CT, Rea A, Geddes D.
Staphylococcus aureus Enterotoxin Production in Raw and Pasteurized Milk: The Effect of Selected Different Storage Durations and Temperatures. Breastfeed Med. 2019; 14 (4): 256-61.
20. Balmer, JH. Guidelines for the establishment and operation of human milk banks in the UK. Arch Dis Child Educ Pract Ed. 2004; 89: ep27–8.
21. Dewitte C, Courdent P, Charlet C, Dumoulin D, Courcol R, Pierrat Vet. Contamination of human milk with aerobic flora: Evaluation of losses for a human milk bank. Arch Pediatr. 2015; 22 (5): 461–7.
22. Arslanoglu S, Bertino E, Tonetto P, De Nisi G, Ambruzzi AM, Biasini A,
et al. Guidelines for the establishment and operation of a donor human milk bank. Italian Association of Human Milk Banks. J Matern Fetal Neonatal Med. 2010; 23 (2): 1-20.
23. Omarsdottir S, Casper C, Akerman A, Polberger S, Vanpée M. Breast milk handling routines for preterm infants in Sweden: A national cross sectional study. Breastfeed Med. 2008; 3 (3): 165-70.
24. Madigan MT, Martinko JM. Microbiologia de Brock. Porto Alegre (RS): Artmed; 2010
.25. Serafini AB, André MCDPB, Rodrigues MAV, Kipnis A, Carvalho CO, Campos MRH,
et al. Microbiological quality of human milk from a Brazilian milk bank. Rev Saúde Pública. 2003; 37 (6): 775-9.
26. Moossavi S, Sepehri S, Robertson B, Bode L, Goruk S, Field CJ,
et al. Composition and variation of the human milk microbiota are influenced by maternal and early-life factors. Cell Host Microbe. 2019; 25 (2): 324-35.
27. Salerno T, Siqueira AK, Pinto JPAN, Da Cunha MLRS, Silvestre PK, Condas LAZ,
et al. Safety issues of raw milk: evaluation of bacteriological and physicochemical characteristics of human milk from a bank in a teaching hospital, focusing on Staphylococcus species. Rev Inst Med Trop São Paulo. 2021; 63: e54
28. Novak FR, Almeida JAG, Asensi MD. Resistência antimicrobiana de coliformes isolados de leite humano ordenhado. Cad Saúde Pública. 2001; 17 (3): 713-7.
29. Rede Brasileira de Bancos de Leite Humano (RBBLH). Determinação de acidez titulável - método Dornic. Rio de Janeiro: FIOCRUZ/IFF-BLH; 2005. [access in 2020 Mai 18]. Available from:
https://rblh.fiocruz.br/sites/rblh.fiocruz.br/files/usuario/79/nt_29.11_determinacao_acidez_lho.pdf30. Serra VV, Teves S, López De Volder A, Ossorio F, Aguilar N, Armadans M. Comparison of the risk of microbiological contamination between samples of breast milk obtained at home and at a healthcare facility. Arch Argent Pediatr. 2013; 111(2): 115-9.
Received on July 20, 2020
Final version presented on May 31, 2022
Approved on July 7, 2022
Author’s contribution: Chaves JO and Menezes CC: Conceptualization (Equal); Data curation (Equal); Formal analysis (Equal); Funding acquisition (Equal); Investigation (Equal); Methodology (Equal); Project administration (Equal); Resources (Equal); Software (Equal); Supervision (Equal); Validation (Equal); Visualization (Equal); Writing – original draft (Equal); Writing – review & editing (Equal).
Fernandes AMF and Parreiras PM: Investigation (Supporting); Methodology (Supporting).
Passos MC: Project administration (Equal) Supervision (Equal); Writing – original draft (Equal); Writing – review & editing (Equal).
Cunha LR: Conceptualization (Equal); Data curation (Equal); Formal analysis (Equal); Investigation (Equal); Methodology (Equal); Project administration (Equal); Supervision (Equal); Validation (Equal); Visualization (Equal); Writing – original draft (Equal); Writing – review & editing (Equal).
All authors approved the final version of the article and declare no conflicts of the interest.


 ; Angélica Maria de Freitas Fernandes2
; Angélica Maria de Freitas Fernandes2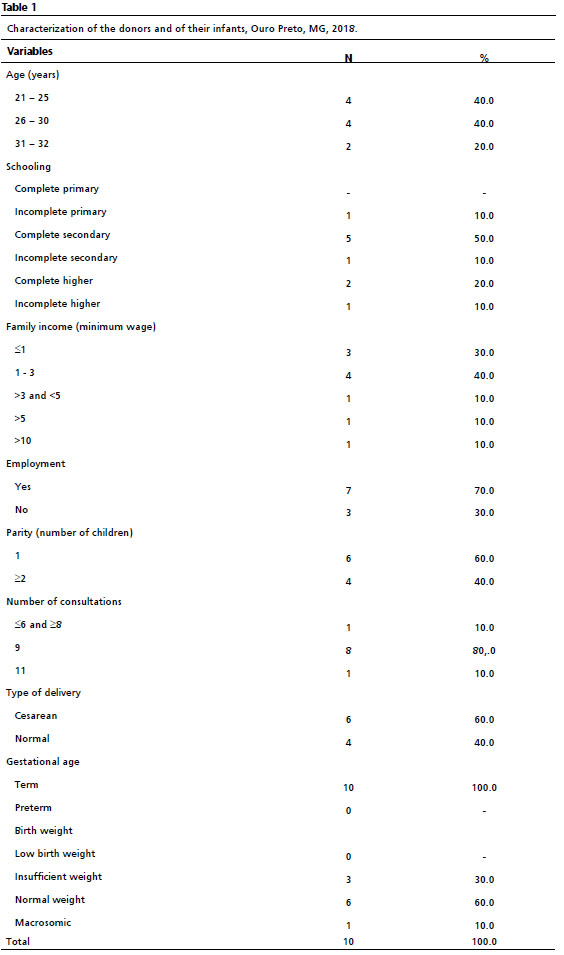






 Ler em português
Ler em português