ABSTRACT
OBJECTIVES: to assess factors associated with early weaning and the pattern of spatial distribution of breastfeeding in the ascription territory of a Basic Health Unit (BHU).
METHODS: analytic cross-sectional study performed with 47 mothers of children under 2 years of age in a BHU from Vitória de Santo Antão, Pernambuco. The association of independent variables and early weaning was verified using bivariate and multivariate analysis. For spatial analysis of cases of breastfeeding, we applied Kernel density estimation, proximity analysis buffers of the addresses of participants to the Health Unit and flow map.
RESULTS: the prevalence of early weaning was 61.7% (CI95% = 47.8-75.6). Factors associated with early weaning were: distance of residence to the BHU higher than 500 meters, not being primiparous, non-participation in educational groups for pregnant women during prenatal period and use of nursing bottles. Being beneficiary of welfare program Bolsa Família and residing in a home with piped water constituted a protective factor for this outcome. Two clusters of early weaning cases were found in locations further away from the BHUs.
CONCLUSIONS: there was high prevalence of early weaning and association of this outcome with the home-health unit displacement, being primiparous, non-participation of pregnant women in educational activities during prenatal period and use of nursing bottles.
Keywords:
Breastfeeding, Weaning, National Health Strategies, Spatial analysis
RESUMO
OBJETIVOS: avaliar os fatores associados ao desmame precoce e o padrão de distribuição espacial do aleitamento materno no território de adscrição de uma Unidade Básica de Saúde (UBS).
MÉTODOS: estudo analítico transversal realizado com 47 mães de crianças menores de dois anos em uma UBS, de Vitória de Santo Antão, Pernambuco. A associação entre as variáveis independentes e o desmame precoce foi verificada por meio de análise bivariada e multivariada. Para análise espacial dos casos de aleitamento materno, empregou-se a técnica de densidade de Kernel, buffers de proximidade dos endereços das participantes à Unidade de Saúde e mapa de fluxo.
RESULTADOS: a prevalência de desmame precoce foi de 61,7% (IC95%= 47,8-75,6). Os fatores associados ao desmame precoce foram: distância da residência para a UBS maior de 500 metros, não ser primípara, não participação no grupo educativo de gestante durante o pré-natal e o uso de mamadeira. Receber bolsa família e residir em domicílio com água encanada constituíram fator de proteção a esse desfecho. Encontrou-se dois aglomerados de casos de desmame precoce em locais mais afastados da UBS.
CONCLUSÕES: houve alta prevalência de desmame precoce e associação deste desfecho com o deslocamento domicílio-unidade de saúde, primiparidade, não participação da gestante em atividades educativas durante o pré-natal e utilização de mamadeira.
Palavras-chave:
Aleitamento materno, Desmame, Estratégia saúde da família, Análise espacial
IntroductionBreast milk is the most adequate food in the early months of life, once it gathers all nutrients necessary to children in this period, besides immunological factors that promote healthy growth and development, and a better beginning of life. Due to this, World Health Organization (WHO) and Ministry of Health (MH) preconize that newborns receive exclusive breastfeeding (EBF) during the first six months of life and breastfeeding with supplementary foods until 2 years of life or more.
1It is estimated that the expansion of breastfeeding practices could prevent 823,000 annual deaths or 13.8% of all deaths of children under 2 years of age. Approximately half of all diarrhea episodes and one third of respiratory tract infections could be avoided by breastfeeding. The protection against hospitalizations due to these diseases is even higher: breastfeeding can prevent 72% of hospitalizations for diarrhea and 57% of those for respiratory tract infections.
2Breastfeeding has essential nutrients, favors cognitive, oral-motor, emotional and social development and intelligence quotient, as well as provides children with immunological protection, mainly at their first year of life. Breastfed children show lower rates of allergies, cardiovascular diseases, malnutrition, diabetes mellitus and gastrointestinal diseases. Furthermore, breastfeeding gives brings immediate and long-term benefits for mother’s health and for the environment, standing out as sustainable nutrition source, viable, non-polluting and non-predatory in regard of natural resources in face of the absence of energy and water outgoings, as well as the use of packages, nursing bottles and bottle nipples. Contributes to the reduction of poverty, hunger and social inequalities.
1-3In spite of all benefits, the early interruption of this practice still being a quotidian reality standing out as one of the most concerning problems in Brazilian public health.
4 Breastfeeding is a challenge for many women, for in addition of assistance difficulties experienced during the birth process and the clinical management of breastfeeding, they suffer severe social, cultural, political and economic influences, and significant variations according to the location and population characteristics. Among others, the reinsertion of the mother to work environment, home-to-work or home-to-health unit displacement and lack of knowledge or maternal self-efficacy in regard of the practice has been mentioned by the literature as determinant factors of early weaning.
3,5,6Preliminary data from the National Survey on Infant Diet and Nutrition (ENANI – Portuguese acronym) that assessed 14,505 children under five years of age in national territory, identified the prevalence of only 45.7% of EBF in Brazil within children up to six months of age, being more frequent in the South Region (53.1%) and less frequent in the Northeast region (38%), rising to 60% in children under 4 months of age.
7 The exposed scenario shows that the prevalence of EBF is still significantly far from what is preconized.
In this context, it is indispensable the comprehension of relationships between urban space and clinical and sociodemographic aspects regarding the practice of breastfeeding, attempting to understand the territorial characteristics of exclusive breastfeeding, locating areas where educational and support interventions should be guided by health policies formulators, observing actual demands of the population.
Starting from the assumption that collective aspects such as attributes of the location of residence and the established relationships in the territory represent an array of constraints and possibilities for the success of breastfeeding, although scarcely studied, this study aimed to assess factors associated with the early weaning and the standard of spatial distribution of breastfeeding in the ascription territory of a Basic Health Unit (BHU).
MethodsAnalytical cross-sectional study conducted in a BHU in the municipality of Vitória de Santo Antão, located at Zona da Mata region in Pernambuco, Brazil. The mentioned municipality has an estimated population of 139,583 people and a territorial area of 335,942 km
2. The choice for this unit occurred in virtue of a higher amount of children assisted by the neonatal nursing service, according to the list provided by the municipal administration. Furthermore, this health service is inserted in an area of high social vulnerability. The instrument selected for methodological orientation was “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE).
Mothers of children with up to 2 years of age, users of neonatal nursing service of the BHU, residing in the coverage area of the service participated in the research, with convenience sampling. Each woman was interviewed once, and the questions were related to the youngest child. Were excluded from the test: mothers without cognitive autonomy to answer the questionnaire; mothers with formal contraindication for breastfeeding (positive HIV or positive HTLV) and adoptive mothers.
Data were collected within December 19 and March 2020. At the time of collection, according to information provided by the health team, 108 children in the age range of 0 to 2 years were enrolled at the BHU. However, data collection needed to be enclosed before the expected period due to social distancing measures required during the outbreak of COVID-19 pandemic, preventing the execution of surveys with presential interviews, as well as the planned range of sample size.
Given the above, the selection of mothers that composed the sample were not probabilistic. Therefore, all mothers of children under 2 years of age that showed up at the healthcare service, before the neonatal nursing consultations at the period of data collection, were invited to participate in the study. Data were obtained by a single researcher, by means of the applying of a structured adapted form, previously validated, composed by sociodemographic, obstetric and behavioral characteristics and variables related to pregnancy, delivery and puerperium.
8 In addition, there was extraction of complementary information contained at the child health booklet.
The outcome in study was early weaning (yes or no). Was considered as early weaning the interruption of exclusive breastfeeding before 6 months of life of the children. The independent variables were, maternal age, lives with partner, maternal schooling, beneficiary of welfare program, income, home with piped water, sanitary sewage, mother was breastfed when child, primiparous, in what service attended prenatal care, number of prenatal care consultations, planned pregnancy, desired pregnancy, received guidance about breastfeeding at prenatal care, participated in educational groups for pregnant women, type of delivery, received guidance about breastfeeding in maternity, postpartum clinical intercurrence, difficulty in breastfeeding in maternity, difficulty in breastfeeding in the first week of life, received domiciliary visits in the first week after delivery, had support of someone to breastfeed, received guidance about EBF at neonatal nursing, smoker, alcoholic beverages consumption, physical activities, distance between residence and BHU. Variables related to children were also used: use of pacifier, use of nursing bottle, gestational age, birth weight, breastfed at the first hour of life, where was breastfed for the first time, use of artificial milk at maternity, after birth was discharged from hospital receiving what kind of milk. Data were typed in an Excel
® spreadsheet, using double validation in order to trace inconsistencies. Posteriorly, data were exported to software Statistical Package for the Social Sciences (SPSS) version 23, for statistical analysis.
In univariate analysis, data were exposed by means of absolute (n) and relative frequency distribution; and mean values, standard deviation, median and maximum and minimum values for quantitative variables. The association between early weaning and independent variables were assessed by means of bivariate analysis, using chi square test or Fisher exact test. Variables that presented p values under 0.25 in the bivariate analysis were introduced in the multiple logistic regression model using the Enter method. In the final regression model, variables with a significance level under 0.05 remained. The multicolinearity test, according to Tolerance and VIF (Variance Inflation Factors) parameters, with tolerance under 10, was performed previously to the multivariate analysis and confirmed the absence of multicolinearity between the independent variables. The quality of logistic regression adjustment was assessed by
Hosmer-Lemeshow test and Nagelkerke R test.
2The adequacy of the final model was assessed by means of the area under ROC curve.
The spatial analysis of the standard of distribution of breastfeeding in the study territory started with the geocoding of addresses of participating mothers that are attended in the health unit. This stage was executed by means of the MMQGIS plugin for QGis software, with Latlong/WGS84 projection. In complement, for registries that are not located at the cartographic database, Find latitude and longitude tool was used, which makes possible the geocoding via Google Earth access. The final archive of geocoded addresses followed the Universal Transverse Mercator (UTM) and datum Geodetic Reference System for the Americas (SIRGAS - Portuguese acronym) 2000.
The digital mesh of the municipality was obtained in the Institute of Geography and Statistics (IBGE – Portuguese acronym). In order to product the digital map of the location, data related to territorial area of adscription and manual sketches for territorialization of the unit were obtained at the BHU. All limits were punctuated, with the digital outlining of the location. After treatment, lines and polygons were imported to QGis software (version 2.18).
Analysis of point density of early weaning cases was performed, applying Kernel density estimation, a technique from geostatistics used for analysis of behavior of standards of points, indicating, by means of non-parametric exploratory interpolation, the intensity of event agglomerationin the study area. In order to demonstrate the geographic access of mothers to the health unit and displacement of residences for the service, flow maps of displacement were built. The flow maps represent the movement of people in space, demonstrating the way and magnitude of the studied movement by means of vectors traced over the travelled itinerary.
9 Simultaneously, buffer analysis was performed, or the area of influence of the health unit, considering a radius of 500 meters, distance considered ideal afoot displacement
10 similar to that used in point density analysis. In another layer, under area of influence, points that represent residences of breastfeeding and early weaning cases were distributed. The thematic maps of spatial analysis, according to addresses, were generated in QGis software version 2.18.
The study was approved by Research Ethics Committee of Federal University of Pernambuco, under opinion Nº 3.734.274
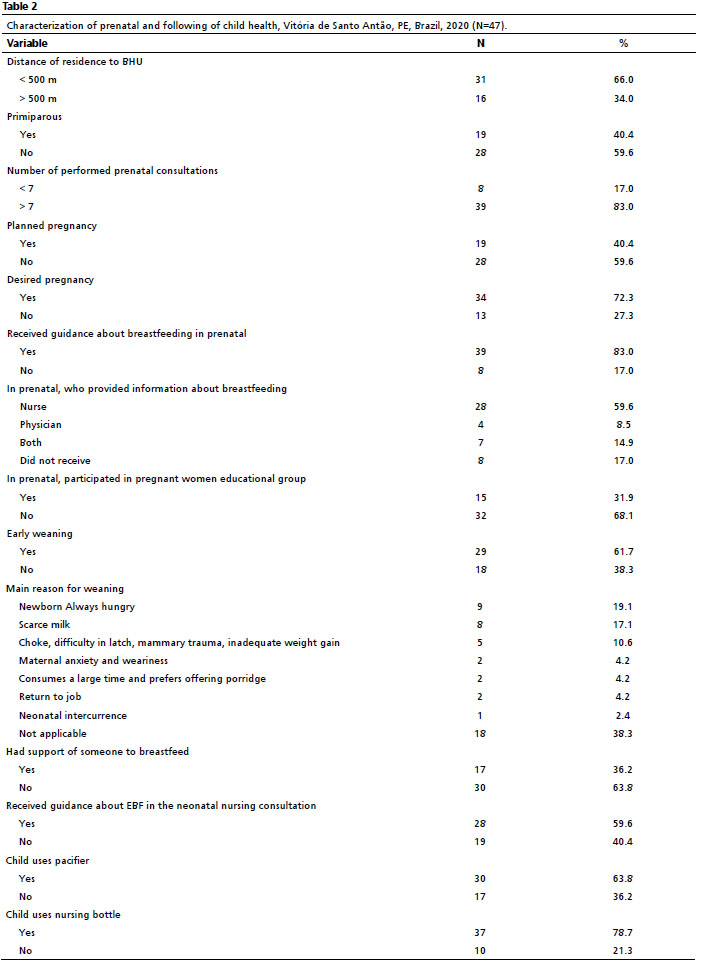
Results47 mothers participated in the study, according to sociodemographic profile available in Table 1. The prevalence of early weaning identified was 61.7% (CI95%= 47.8-75.6). Most interviewed mothers resided at a distance inferior to 500 meters to the BHU and were multiparous. Although non-planned pregnancy had predominated, higher prevalence of adequate number of prenatal consultations was observed, as well as desired pregnancy and perception of guidance about breastfeeding at the prenatal period, mainly from the nurse (Table 2).
In the bivariate analysis, according to established criterion (
p<0.25) were pre-selected the variables orientations about EBF in neonatal nursing consultation ((
p = 0.045), use of pacifier (
p = 0.029), use of nursing bottle (
p = 0.030), distance of residence to health unit (
p = 0.001), benefit from welfare program (
p = 0.074), house with piped water (
p = 0.225), sanitary sewage (
p = 0.225), primiparous ((
p = 0.242), participated in educational group for pregnant women at prenatal period (
p = 0.147), clinical postpartum intercurrence (
p = 0.185) and breastfed at the first hour of life (
p = 0.124).
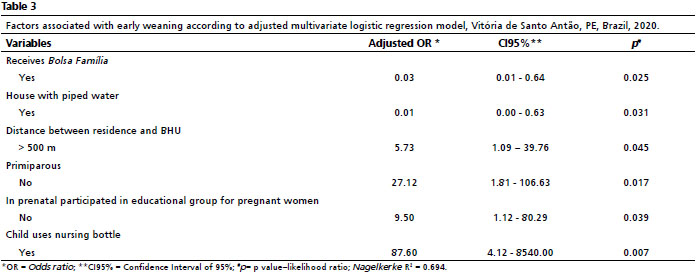
After multivariate analysis (Table 3), remained in the adjusted model associated with early weaning the following variables: distance of residence to BHU over 500 meters, showing almost 6 times more chance for the event of outcome, compared to mothers residing around BHU. In the same way, not being primiparous, in this study, showed a 27 times higher chance for the exclusive breastfeeding interruption outcome, as well as the non-participation in the group of pregnant women during prenatal period and use of nursing bottle. We highlight that being beneficiary of social welfare program and residing in a house with piped water were variables of protection against early weaning.
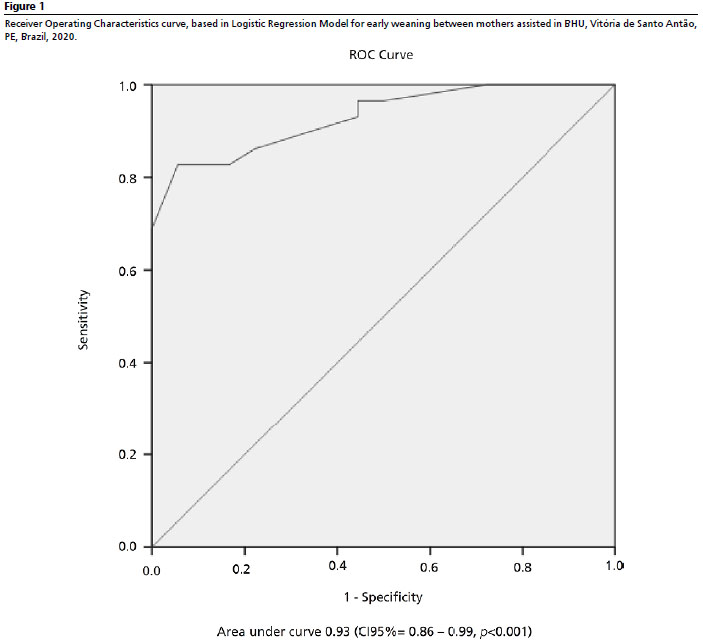
We observed that the model was capable to explain around 69.4% of variations registered in the dependent variable (
Nagelkerke R
2 = 0.694). It presented excellent capability of discrimination of findings and relevant difference of random estimation, as can be verified by the area under ROC curve (c=0.93;
p<0.001), indicated in Figure 1.
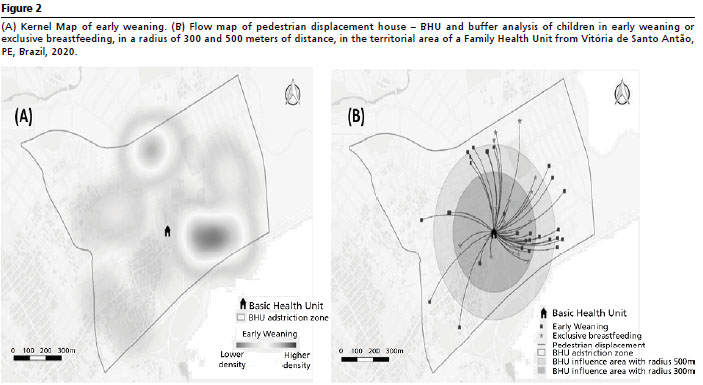
The map generated with Kernel technique (Figure 2A) shows locations with higher density of early weaning cases in the BHU ascription area, shown in darker shades. We observed the building of two clusters, concentrated mainly at North and Southeast zones of the ascription territory, with predominance of early weaning cases in locations that were further from the BHU, as shown in Figure 2B. There was centralization of children in exclusive breastfeeding residing at a closer distance of the service, considering a radius of 300 meters.
DiscussionData evidenced high prevalence of early weaning. A research conducted in the referred municipality between 2014 and 2015 found lower results (41.7%).
11 We infer, thus, that although the constant awareness of professionals and public health sectors regarding duration and exclusivity of breastfeeding, the resolution for this demand isyet to beaccomplished.
In regard of maternal characteristics, it was observed that more than half of women affirmed to live with a partner. Some authors suggest that the presence of a partner, supporting women with the care of the neonate, collaborates on EBF continuity.
12-14 Nevertheless, in spite of the living with a partner, most women affirmed not having received any kind of familiar support during the process of breastfeeding. It is known that the decision of the woman in breastfeeding is collective and involves social, familiar, employment and media aspects. In regard of the influence of the familiar nucleus (partner, mother, mother in law, aunts, grandmothers, among others), when it is favorable to the continuity of breastfeeding, it may resound in a positive stimulation for the mother with regard of caring and keeping the lactating child in EBF for a longer period.
13,14Mothers reported having received information from health professionals related to breastfeeding, including its benefits and techniques. The applicability with effectiveness of this information and clearness of language used by health professionals positively reverberates in the high prevalence of early weaning highlighted within the group of mothers participating in the survey. Studies show that mothers that were not well informed about breastfeeding plan to breastfeed for a shorter time, emphasizing the importance of good communication between the subjects for the success of breastfeeding.
14-16As to the factors that influenced early weaning, the belief in the fact that the breast milk would be weak or insufficient for the baby was highlighted as the most frequent answer. This occurs due to the clear aspect of breast milk and the frequent association of the children’s cry with hunger, cultural factors and the lack of knowledge of the mother concerning physiological and nutritional aspects of human milk, as well as the way it is produced.
6In face of this, the mother is lead to complementary feeding with infant formulas, teas and other foods, interfering with the alimentary satisfaction of the child, besides propitiating problems such as: insufficient suction, mammary engorgement, nipple lesions and in the end, early weaning.
12,17,18Other justifications for early weaning reported by mothers were: choking, difficulty in latch and nipple trauma. This is directly related to the position of the neonate in relation to the breast in the moment of breastfeeding, and could be corrected by means of practical and instructional support from health professionals, mainly nurses, in the prevention, stimulation to maternal self-confidence, early identification and handling of mammary intercurrences at the period of lactation, attempting to contribute to the expanding of EBF.
5,17,19,20From the findings of multivariate and spatial analyses, it could be evidenced that living further away from the BHU was associated with early weaning, which is an unprecedented finding in the literature, once there is a gap in the scientific knowledge about how geographic accessibility to health services can impact neonatal indicators and outcomes. An integrative review found that higher distances to be roamed increase the probability of women not seeking for health services. The mobility between home and health services is impaired by distance, even when there is possibility of having a vehicle. Furthermore, the time of travel, the public transport precariousness, locations or residence socioeconomically underprivileged and lower schooling of women are factors that hinder displacement from home to health services.
21The access to health services is a multidimensional theme, involving political, economic, social, organizing and geographic aspects in the establishment of paths taken by people seeking for care. In Family Health Strategy quotidian, access difficulties, high spontaneous demand and lack of professionals exacerbate the health care accesibilty.
22 We infer, accordingly, that beyond good communication, the building of a link with the ascribed population makes possible the longitudinality and completeness of care. The strengthening of the link health unit - community can promote confidence and building of autonomy for the user’s perspective, contributing to the adhesion of healthcare actions proposed by health professionals.
Concerning parity, the early interruption of EBF was associated with mothers that had more than one child. Such finding differs from previous studies that affirm that early weaning is more prevalent in primiparous mothers due to low experience and immaturity with the care and breastfeeding.Multiparous mothers need constantly to be focused in the care of other children, dividing their time with them, as well as job and housework, which can possibly lead to breastfeeding interruption. Such aspect can be reinforced by lack of familiar support for breastfeeding and non-participation in educational health groups for pregnant women, reported by most women.
5,13,17The use of nursing bottles showed a higher chance of early weaning compared to mothers who did not use it. A cohort prospective research conducted in Porto Alegre with 150 mothers and children in rooming-in also demonstrated that children that did not use nursing bottles and pacifiers showed a 23.08 times higher chance of maintaining EBF.
23 The non-offering of these devices to children that are being breastfed is referred to as one of the Ten Steps for Successful Breastfeeding.
24 It is worth highlighting that this offer is directly associated with a media and sociocultural issue that strongly affects the breastfeeding mother.
25-27It is known that the introduction of substitutive foods for breast milk with usage of nursing bottles brings impairments to the development of the oral motor system of the child. Besides, the use of nursing bottles and pacifiers lead to an increase of the gaps between each breastfeeding, incoordination of the suction process, partial breast emptying, greater risk of breast engorgement, nipple lesions and reduction in milk production.
27,28The predictors “receiving social welfare benefit” and “residing in a home with piped water” reflect the life conditions and social context in which mothers live, being considered protection variables to early weaning. Studies demonstrate that house conditions and sanitation are considered relevant social and sanitary indicators to health promotion, being directly linked to efficacy and safety in breastfeeding process, besides representing a constitutional right.
2 The Family Allowance program (
Bolsa Família - Portuguese), implemented in the BHU routine, present as educational measures the incentive to breastfeeding and promotion of adequate and healthy nutrition. Furthermore, it contributes to the regular following of children’s health in the services.
30A prospective observational study conducted in Italy in 2017 found that mothers with low schooling are prone to early interrupt breastfeeding. The higher level of schooling was considered as precursor of access to information and motivation towards the advantages of EBF, resulting in a higher duration.
12In the same way, mothers with lower income are prone to early abandon exclusive breastfeeding. Besides, they seek health services less frequently.
25,29In this perspective, it is evidenced that early weaning acts together with health social determinants, a construct associated with individual behaviors, to life and work conditions and to the sociocultural and economic macrostructure,
31 pointing to the need for intervening in these non-clinic elements with an expanded plan of care, ensuring, thus, the promotion of EBF support and the benefits of this practice to maternal-and-child and community health.
We identify as limitations of this study the impossibility of establishing a cause and effect relationship inherent to the cross-sectional design of the research, being important that prospective and multicentric studies can be conducted in order to argue against the results. The findings cannot be generalized for the total population of mothers due to the analysis sample size and the use of convenience sample, however it is capable to offer subsides for further studies. It is worth mentioning that the overestimation of variance in some confidence intervals may be related to a small sample size due to difficulties of reaching of population and the sample itself, previously calculated for the study, with adherence to the restriction of physical contact and access to health services imposed by the onset of COVID-19 pandemic. The memory bias of interviewees should also be considered in the analysis of study limits due to the obtaining of self - referral information.
This study allows for advances in aspects related to knowledge of determinants of early weaning molded in the social context in which mothers are inserted in territories assisted by Family Health Strategy, an aspect that is scarcely investigated in scientific publications and that needs to be largely propagated and discussed with health professionals.
We conclude that a higher distance between the residence to BHU, not being primiparous, the non-participation of the mother in the pregnant women group during prenatal period and use of nursing bottle were predictors of early weaning in the study population. The spatial analysis corroborated the predominance of children in EBF residing in a closer distance to the BHU located in the study territory. Being beneficiary of social welfare program and residing in a house with piped water stood out as protection variables. Strategies of incentive to breastfeeding with awareness to social determinants in healthcare, working in inter-sectorial partnerships and improving equity for each child since the beginning until the further life should be developed in a way that contributes to successful EBF and with the decrease of infant morbimortality, mainly in the Primary Attention sector.
References1. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. Departamento de Promoção da Saúde. Guia alimentar para crianças brasileiras menores de 2 anos. Brasília (DF): Ministério da Saúde; 2019. [acess in 2021 Fev 20]. Available from:
http://189.28.128.100/dab/docs/portaldab/publicacoes/guia_da_crianca_2019.pdf2. Victora CG, Barros AJD, França GVA, Bahl R, Rollins NC, Horton S,
et al. Amamentação no século 21: epidemiologia, mecanismos, e efeitos ao longo da vida. Epidemiol Serv Saúde. 2016; 25 (1): 1-24.
3. Miranda e Silva C, Pellegrinelli ALR, Pereira SCL, Passos IR, Santos LC. Práticas educativas segundo os “Dez passos para o sucesso do aleitamento materno” em um Banco de Leite Humano. Ciênc Saúde Colet. 2017; 22 (5): 1661-71.
4. Rollins NC, Bhandari N, Hajeebhoy N, Horton S, Lutter CK, Martines JC,
et al. Why invest, and what it will take to improve breastfeeding practices? Lancet. 2016; 387 (10017): 491-504.
5. Lima APC, Nascimento DS, Martins MMF. A prática do aleitamento materno e os fatores que levam ao desmame precoce: uma revisão integrativa. J. Health BiolSci. 2018; 6 (2): 189-96.
6. Ferreira TDM, Piccioni LD, Queiroz PHB, Silva EM, Do Vale IN. Influência das avós no aleitamento materno exclusivo: estudo descritivo transversal. Einstein. 2018; 16 (4): 1-7.
7. Ministério da Saúde (BR). Universidade Federal do Rio de Janeiro (UFRJ). Estudo Nacional de Alimentação e Nutrição Infantil – ENANI-2019: Resultados preliminares - Indicadores de aleitamento materno no Brasil. UFRJ: Rio de Janeiro; 2020. [access in 2021 Fev 20]. Available from:
https://enani.nutricao.ufrj.br/wpcontent/uploads/2020/08/Relatorio-preliminar-AM-Site.pdf8. Uchoa JLU. Autoeficácia das mulheres no ciclo gravídico-puerperal em amamentar [dissertação]. Fortaleza: Faculdade de Farmácia, Odontologia e Enfermagem da Universidade Federal do Ceará; 2012.
9. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Fundação Oswaldo Cruz. Abordagens espaciais na saúde pública. Brasília (DF): Ministério da Saúde; 2006. [access in 2021 Fev 20]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/serie_geoproc_vol_1.pdf10. Gonçalves PH, Fonseca TP, Cardoso CF. Entraves ao deslocamento pedonal em uma cidade de pequeno porte: os níveis de caminhabilidade na cidade de Goiás-GO. Mix Sustentável. 2017; 3 (2): 57-65.
11. Carvalho MF, Santos CR, SANTOS PTF. Primeira visita domiciliar puerperal: uma estratégia protetora do aleitamento materno exclusivo. Rev Paul Pediatr. 2018; 36 (1): 66-73.
12. Colombo L, Crippa BL, Consonni D, Bettinelli ME, Agosti V, Mangino G,
et al. Breastfeeding determinants in healthy term newborns. Nutrients. 2018 Jan; 10 (1): 48.
13. Margotti E, Margotti W. Fatores relacionados ao aleitamento materno exclusivo em bebês nascidos em hospital amigo da criança em uma capital do Norte brasileiro. Saúde Debate. 2017; 41 (114): 860-71.
14. Tewabe T, Mandesh A, Gualu T, Alem G, Mekuria G, Zeleke H. Exclusive breastfeeding practice and associated factors among mothers in Motta town, East Gojjam zone, Amhara Regional State, Ethiopia, 2015: a cross-sectional study. Int Breastfeeding J. 2017; 12 (1): 12.
15. Andrade HS, Pessoa RA, Donizete LCV. Fatores relacionados ao desmame precoce do aleitamento materno. Rev Bras Med Fam Comunidade. 2018; 13 (40): 1-11.
16. Silva KMS, Goetz ER, Santos MVJ. Aleitamento materno: conhecimento das gestantes sobre a importância da amamentação na Estratégia de Saúde da Família. RBCS. 2017; 21 (2): 111-8.
17. Alvarenga SC, Silveira CD, Leite FMC, Brandão MAG, Zandonade E, Primo CC. Fatores que influenciam o desmame precoce. Aquichan. 2017; 11 (17): 93-103.
18. Oliveira AKP, Melo RA, Maciel LP, Tavares AK, Amando AR, Sena CRS. Práticas e crenças populares associadas ao desmame precoce. Av Enferm. 2017; 35 (3): 303-12.
19. Alatalo D, Jiang L, Geddes D, Hassanipour F. Nipple deformation and peripheral pressure on the areola during breastfeeding. J Biomech Eng. 2020; 142 (1): 011004.
20. Degefa N, Tariku B, Bancha T, Amana G, Hajo A, Kusse Y,
et al. Breast feeding practice: positioning and attachment during breast feeding among lactating mothers visiting health facility in Areka Town, Southern Ethiopia. Int J Pediatrics. 2019; 1-6.
21. Rodrigues IR, Sales LBF, Oriá MOB, Gomes MLS, Moura NS. Impact on pregnant/parturient women’s health resulting from displacement between residence and health service. Rev Rene. 2021; 22: e61115.
22. Chávez GM, Viegas SMF, Roquini GR, Santos TR. Access, accessibility, and demand at the family health strategy. Esc Anna Nery. 2020; 24 (4): e20190331.
23. Gasparin VA, Strada JKR, Moraes BA, Betti T, Pitilin EB, Santo LCE. Fatores associados à manutenção do aleitamento materno exclusivo no pós-parto tardio. Rev Gaúcha Enferm. 2020; 41 (spe): e20190060.
24. World Health Organization (WHO). Implementation guidance - protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services: the revised Baby-Friendly Hospital Initiative 2018. Geneva: WHO; 2018. [access in 2021 Fev 20]. Available from:
https://www.who.int/publications/i/item/978924151380725. Santana GS, Giugliani ER, Vieira TO, Vieira GO. Factors associated with breastfeeding maintenance for 12 months or more: a systematic review. J Pediatr. 2018; 94 (2): 104-22.
26. Araújo AR, Nascimento ALV, Camargos JM, Silva FS, Faria NVMG. Fotobiomodulação como uma nova abordagem para o tratamento de traumas mamilares: um estudo piloto, randomizado e controlado. Fisioter Bras. 2018; 14 (1): 20-6.
27. Santos EM, Silva LS, Rodrigues BFS, Amorim TMAX, Silva CS, Borba JMC,
et al. Breastfeeding assessment in children up to 2 years of age assisted in primary health care of Recife in the state of Pernambuco, Brazil. Cienc Saúde Colet. 2019; 24 (3): 1211-22.
28. Salcan S, Topal I, Ates I. The frequency and effective factors of exclusive breastfeeding for the first six months in babies born in Erzincan Province in 2016. Eurasian J Med. 2019; 51 (2): 145-9.
29. Ministério da Saúde (BR). Bases para a discussão da Política Nacional de Promoção, Proteção e Apoio ao Aleitamento Materno. Brasília (DF): Ministério da Saúde; 2017. [access in 2021 Fev 20]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/bases_discussao_politica_aleitamento_materno.pdf30. Barbosa KIP, Conceiçao SIO. Factores sociodemográficos maternos asociadosconlalactancia materna exclusiva. Rev Cuid. 2020; 11 (1): e811.
31. Gadelha IP, Diniz FF, Aquino PS, Silva DM, Balsells MMD, Pinheiro AKB. Determinantes sociais da saúde de gestantes acompanhadas no pré-natal de alto risco. Rev Rene. 2020; 21: e42198.
Received on March 31, 2021
Final version presented on April 11, 2022
Approved on September 1, 2022
Author’s contribution: Holanda ER: conceptualization of work, production and analysis of results, data interpretation, writing and critic review of manuscript. Silva IL: conceptualization of work, data collection writing and critic review of the manuscript.
The authors approved the final version of the article and declare no conflict of interest.


 ; Isabela Lemos da Silva2
; Isabela Lemos da Silva2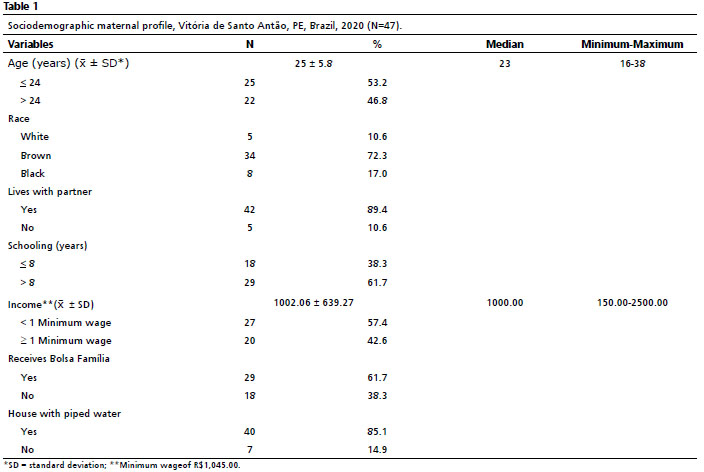






 Ler em português
Ler em português