ABSTRACT
OBJECTIVES: to verify the adequacy of recommendations on food and nutrition for infants available on popular websites in relation to the “Twelve Steps for a Healthy Diet” from the Dietary guidelines for Brazilian children under 2 years of age.
METHODS: popular websites were searched via the Google platform to collect data about food recommendations for children under 2 years of age. The data was categorized according to criteria developed with the Guide: totally agree, partially agree, disagree, contradictory and absent. The websites were described according to the frequency of each step and the distribution in the categories.
RESULTS: 82 websites were included. Most frequent steps: 1 (84.1%), 2 (82.9%) and 4 (63.4%); least present: 8 (23.2%), 10 (19.5%), 11 (3.7%) and 12 (1.2%). The highest percentages of adequacy in relation to the Guide were steps 1 and 4 with 46.4% and 53.8%, respectively. Steps 3 (37.9%) and 7 (75.0%) had the highest percentages of disagreement or contradiction.
CONCLUSIONS: there is proper information on the internet, however, these are mixed with missing, in disagreement, partially in agreement or contradictory information, which reinforces the importance of disseminating the recommendations of the Guide
Keywords:
Internet, Breastfeeding, Complementary feeding, Dietary guidelines, Health communication
RESUMO
OBJETIVOS: analisar a adequação das recomendações sobre alimentação e nutrição de lactentes disponíveis em websites populares em relação aos “Doze passos para uma alimentação saudável” descritos no Guia alimentar para crianças brasileiras menores de dois anos.
MÉTODOS: websites populares foram buscados via plataforma Google para coleta de dados relativos às recomendações sobre alimentação de lactentes. As informações foram categorizadas segundo critérios desenvolvidos em relação à consonância com o Guia em: totalmente de acordo, parcialmente de acordo, em desacordo, contraditórias e ausentes. Os websites foram descritos e apresentados segundo frequência de cada passo e a distribuição segundo as categorias.
RESULTADOS: foram incluídos 82 websites. Passos mais presentes: 1 (84,1%), 2 (82,9%) e 4 (63,4%); passos menos presentes: 8 (23,2%), 10 (19,5%), 11 (3,7%) e 12 (1,2%). Os maiores percentuais de adequação em relação ao Guia foram os passos 1 e 4 com 46,4% e 53,8%, respectivamente. Os passos 3 (37,9%) e 7 (75,0%) apresentaram os maiores percentuais de desacordo ou contradição.
CONCLUSÕES: identificou-se a presença de informações adequadas na internet, entretanto, estas se misturam com informações ausentes, em desacordo, parcialmente de acordo ou contraditórias, reforçando a importância da disseminação das recomendações do Guia.
Palavras-chave:
Internet, Aleitamento materno, Alimentação complementar, Guias alimentares, Comunicação em saúde
IntroductionThe first two years of a child’s life is a period of intense growth and development in which food and nutrition are important elements as they influence not only physical, but also cognitive, language and socio-emotional development.
1,2 These dimensions are inextricably linked with the repercussions until adulthood.
2It is common for caregivers of babies to have several doubts about how to act and what decisions to make regarding the children’s health and feeding. The main difficulties found regarding the feeding of children up to two years of age are related to breastfeeding (BF), such as myths about breast milk and inadequate latch. Another common difficulty is related to food introduction, when there is the offering of other foods in addition to breast milk and infant formulas for infants, including barriers in preparing meals and, also, taboos about which food the child can or cannot eat and what their ideal consistency.
3,4The difficulties and doubts presented can be alleviated through the search for information, either by popular knowledge, by consulting health professionals or even using the internet. The latter has grown across the country. In 2019, 71% of Brazilian households already had accessed the internet, with the topic “health” accounting for 47% of virtual surveys.
5 The topic “children” appeared among the 10 most searched health-related topics, according to Google Trends
.6 Thus, it is observed that the internet is an important source of information on child’s health and health, therefore, it is desirable that it contains reliable information.
In Brazil, the current edition of the
Dietary Guidelines for Brazilian children under 2 years of age, hereinafter referred to as the Guide, was published in 2019.
7 It calls children up to two years of age as infants, a term used from now on. The publication of this edition represents a paradigm shift in relation to the previous version, from 2002, by adopting a classification of food based on the extent and purpose of processing, also used in the
Dietary Guidelines for the Brazilian population (2014),
8 in dialogue with the most up-to-date evidence on the relationship between diet and health.
9 Unlike the previous version, the recommendations are presented in text format and illustrations in an accessible language for the general population – and not just for health professionals, which, added to the fact that it is the main official federal document on food for infants, justifies its use in this work as a reference for the evaluation of the information present on the websites. At the end of the document, the central aspects are summarized in the “Twelve Steps for a Healthy Diet”, in order to facilitate and summarize the reading.
Not only the complete
Guide, but also an abridged version the Twelve Steps can be found on the internet for download in digital format for reading and consultation. In both dietary guidelines currently in force in the country (for children under two and for the general population), the search for reliable information on the internet is recognized as a contemporary challenge.
7,8 A previous study carried out a similar analysis in relation to the “Ten Steps for a Healthy Eating”, present in the previous edition of the guide,
10 but no similar study was found that considered the recommendations of the current document.
The present work proposes to analyze the adequacy of recommendations on food and nutrition for infants available on popular
websites in relation to the “Twelve Steps for a Healthy Diet”, described in the
Guide.
MethodsDescriptive study based on the collection and analysis of information about infant feeding available on popular
websites. The search tool used was
Google. The search terms included were those identified as usual in searches on the topic of feeding children from zero to two years old, according to
Google Trends.
6They are (search perfomed in Portuguese): “aleitamento materno” (breastfeeding), “leite materno” (breast milk), “comida bebê” (baby food), “comer bebê” (baby eat), “alimentação bebê” (baby feeding), “introdução alimentar” (food introduction) and “alimentação complementar” (complementary feeding).
The list of websites was obtained in March 2020, on a scheduled day and time, using personal computers with a browser in an anonymous window, so that personal searches would not influence Google’s search algorithm. The websites found on the first two pages of the search were included in the study in order to capture the information most likely to be accessed by the infants’ parents and caregivers .
11Links that directed to documents from official bodies (for example: Ministry of Health (MH), World Health Organization (WHO) and Sociedade Brasileira de Pediatria (SBP) (Brazilian Pediatrics Society ); academic searches; sales and advertising
websites; images were excluded from the study; videos; definition of terms;
websites that talk exclusively about breastfeeding techniques and whose purpose was not to explain content about infant feeding; websites that only had links and no content; and unavailable
websites. In addition,
websites that appeared as a search result for more than one term were considered only once. The search followed the same order as the terms presented above.
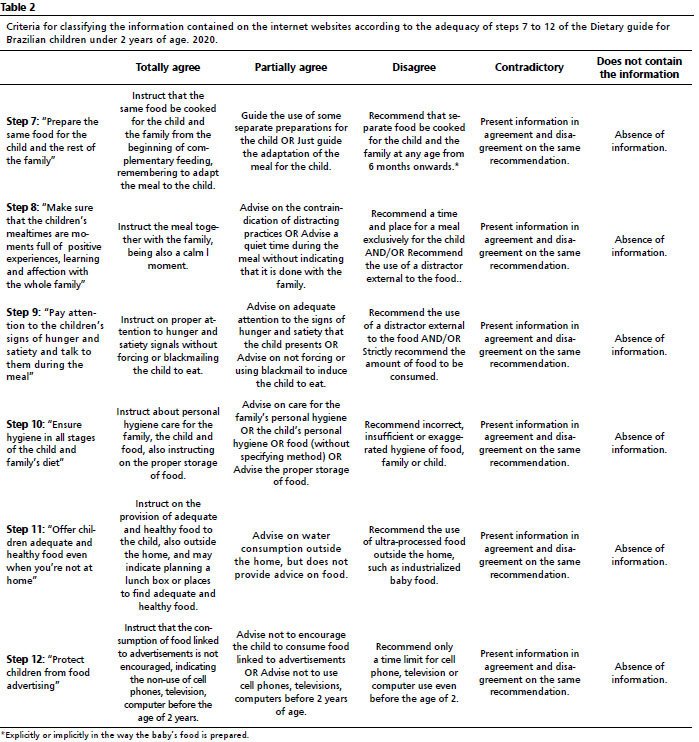
The construction of the database was done through the collection of information from the selected
websites, according to metrics, prepared by the researchers, from the “Twelve Steps for a Healthy Diet”, available in the
Guide and presented in Tables 1 and 2.
7 The metrics were developed considering the main recommendations present in the respective step. Information that clearly aligned with the main recommendations of the twelve steps was considered to be fully in agreement; when the information on the
websites was not clear or complete, it was classified as partially in agreement; when the
websites presented incorrect information about the main content of the step, it was classified as in disagreement and, when presenting information either correct or incorrect, the
websites were classified as contradictory.
In addition to classifying the
websites according to metrics, the following information was also collected: link with company/food industry or products aimed at children, link with educational/research institution, presence of bibliographic references, citation of health professionals, date of last update, presence of advertisement and country of origin. Any relationship with partner institutions/companies or dependencies presented in the content of the
site was considered a link.
Websites in Portuguese were included, even if from countries other than Brazil, in order to encompass all information available to be accessed by the infants’ parents and caregivers
All data were collected twice, independently, by two researchers in order to improve the accuracy of the classification according to the metrics of adequacy of the recommendations. The discrepancies were resolved by a third evaluator.
As an indicator of the quality of the metrics, inter-rater agreement was calculated using the adjusted kappa statistic for prevalence and bias (PABAK) and 95% confidence interval, using the
STATA 14.0 software. The following cut-off points were considered: 0 = poor; 0.01-0.20 = light; 0.21-0.40 = weak; 0.41-0.60 = moderate, 0.61-0.80 = substantial, and 0.81-1 = almost perfect.
12 Except for one of the steps where agreement was moderate (step 7; PABAK = 0.6), all others had substantial or near perfect agreement, with PABAK ranging from 0.71 to 1.0.
Data were organized in
Excel and analyzed in
STATA 14.0. The
websites were described according to the presence and types of links, the presence of references and advertising, and the date of the last update. The date of the last update was categorized into: “until Nov. 2014”, “Dec. 2014 to Oct. 2019” and “from Nov. 2019” (the cutoff points adopted are based on the publication dates of the Dietary Guidelines for the Brazilian Population, published in November 2014, a document that introduced food processing into Brazilian public policies and which was one of the bases for the development of the Guide, published in October 2019.
7,8Then, the frequency with which each step was addressed on the
websites was presented, as well as the distribution of the classification according to the metrics. We chose to add the “contradictory” criterion to the “disagreeing” criterion due to the low occurrence of the first (12 times and in only five steps). Finally, the proportion of adequacy of
websites was analyzed according to descriptive variables for the three most frequently addressed steps (steps 1, 2 and 4).
Results209
websites were found. Of these, 127 were excluded, of which 35.4% were sales
websites, 22.0% were videos, 11.8% were duplicate
websites and 30.8% related to the other exclusion criteria. Eighty-two popular
websites were analyzed, including blogs, food and children’s products
websites, magazine
websites and others. The vast majority of websites analyzed were Brazilian, except for three Spanish and one Portuguese.
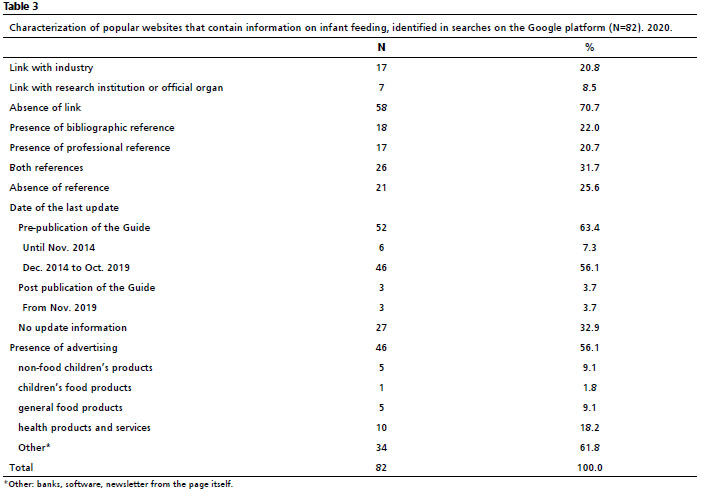
Table 3 presents the characteristics of the
websites studied. Regarding the link with institutions and companies, the majority (70.7%) did not present a such relationship. Among the
websites where there was a declaration of affiliation, most were with food or children’s products (20.7%). A large part presented some reference to the available content (74.4%), whether bibliographic or professional.
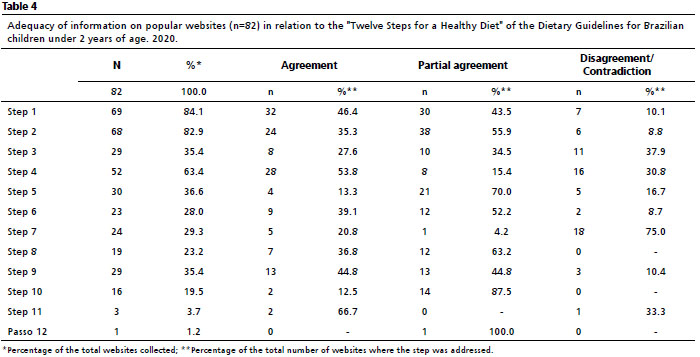
Table 4 shows the percentages of adequacy, partial adequacy and disagreement/contradiction for each of the “Twelve Steps for a Healthy Diet” of the
Guide, on the websites that contained information.
Steps 1, 2 and 4, mainly related to breastfeeding and the beginning of complementary feeding, were the most frequently addressed steps, being present in 84.1%, 82.9% and 63.4% of the
websites, respectively. Contrastingly, the least present were steps 8 (present in 23.2% of the
websites), which addresses the importance of positive experiences at mealtimes with the family; 10 (19.5%) about food hygiene during preparation and consumption; 11 (3.7%) about planning meals outside the home; and 12 (1.2%), which discusses the protection of children against child advertising.
While steps 1, with 46.4%, and 4, with 53.8%, were the ones with the highest percentages of total adequacy, steps 3, on the importance of prioritizing water over other beverages, and 7, that addresses the need to cook the same food for the child and the family, showed the highest percentages of disagreement/contradiction, with 37.9% and 75.0%, in that order.
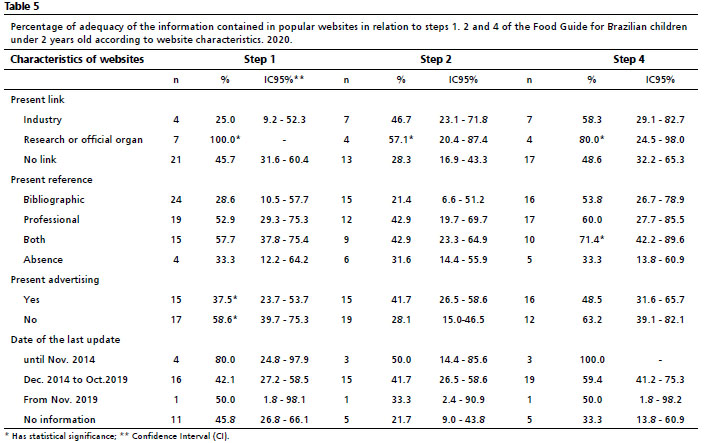
Table 5 presents the percentages of total adequacy of steps 1, 2 and 4 on the
websites included in the survey according to the descriptive variables. Regarding steps 1 (100.0%), 2 (57.1%) and 4 (80.0%), there was a higher percentage of adequacy on
websites that were linked to an organ and/or research institution when compared to not having any kind of bond. Although there was no statistical significance, the websites that were linked to the food industry or sales on children’s products showed less adequacy to the content of the
Guide.
7 In step 1, a greater proportion of adequacy was observed when the
websites did not present advertisements for any types; in step 4, the adequacy was greater when the websites had professional or bibliographic references in relation to the absence of such references.
12 DiscussionIn this study, it was found that steps 1, 2 and 4 were the most present in the analyzed sites, with 1 and 4 having the highest percentages of total adequacy. Steps 11 and 12 were the least discussed recommendations on the websites of this study. The recommendations of steps 7 and 3 were those with the highest percentage of inadequacy/contradiction in relation to the Guide.
7The high diffusion of step 1 can be interpreted in the light of the success of a set of actions to promote breastfeeding implemented in Brazil from the 1980s onwards.
13,14 Between 1986 and 2006, the prevalence of exclusive breastfeeding (EBF) increased from 2.9% to 37.1%, remaining stable in 2013.
14 In 2019, the
Estudo Nacional de Alimentação e Nutrição Infantil (ENANI)(National Child Food and Nutrition Study) revealed that the prevalence of EB among children under four months of age was 59.7% in Brazil and in children under six months of age it was 45.8% on the previous day to research. As for continued breastfeeding in the second year of life (among children aged 12 to 23 months), the prevalence was 43.6% in the country.
14 It is observed that the greater dissemination of correct information about breastfeeding can contribute to the increase in its prevalence.
9The second step was also quite frequent, presenting an important percentage of partial adequacy. The partial adequacy is due to the fact that, in more than half of the
websites, the indication of the food groups to be included in the diet was limited or absent. This incompleteness of the content can lead to the dissemination of erroneous information and increase the risk of offering food that is not very diverse and of low nutritional quality.
15 In ENANI-2019, it was observed a low prevalence of minimum food diversity for children aged between six and 11 months (46%),
16 which highlights the importance of encouraging food diversity in health materials and media.
Step 3 had a low presence on
websites and a high proportion of disagreement and contradiction. The first version of the Guide (2002)
17 recommended the offer of natural fruit juice at 12 months of age, which may partly explain this indication still present on the
websites. The prevalence of consumption of sweetened beverages by Brazilian children aged between six and 23 months on the day before the survey was 24.5%, with an increase to 37.8% in the age group of 18-23 months, which reiterates the importance of dissemination of this complete and correct information.
16Step 4 was quite present on the
websites, and more than half presented information fully adequate to the Guide
.7 The high adequacy can be explained by the fact that this information has been recommended by competent organs for almost 20 years, presented by the MS in the first version of the Guide (2002)
17 and by the Pan American Health Organization/WHO (PAHO/WHO), since 2001.
18 It is also observed in the ENANI-2019 study, that the prevalence of consumption of food with table salt in the proper consistency on the day prior to the interview was 67.8% in the country.
16The recommendations from step 5 were present in just over a third of the
websites. Some previous documents, such as the first edition of the Guide (2002)
17 and WHO guidelines,
19 only advise to avoid sugar consumption. It is possible that this dissonance between the recommendations may be related to the low frequency of this recommendation on the
websites and configures a concerning scenario, since the early supply of sugar makes it difficult to accept vegetables and increases the chance of being overweight, which may have repercussions until adult life.
7Step 6 is an unprecedented recommendation, which may explain, at least in part, its low presence on the
websites studied. The ENANI-2019 national survey revealed the need to disseminate this recommendation and public policies that guarantee a complementary diet based
on natural and minimally processed foods, since 80.5% of children between six and 23 months of age consumed at least an ultra-processed food the day before the survey.
16Regarding step 7, the high inadequacy of the information present on the
websites can be explained as it differs from the recommendations of both the previous edition of the Guide (2002) and the Brazilian Society of Pediatrics
20 which guides to separate the preparation of baby food and not adding salt to the child’s food. It is important to note that in order to share food with the child, the family must follow the recommendations for healthy eating presented in the
Dietary Guidelines for the Brazilian Population.7,8Step 8 was rarely present on the websites studied, which might be explained by being an innovative recommendation and not present in the first edition of the Guide (2002).
17 Regarding step 9, the previous edition of the Guide (2002) already contains instructions for the attention to the baby’s hunger signals, but also establishes strict amounts in closed menus for them, this may justify the distribution between total or partial adequacy in this recommendation. The recommendations of step 10, in turn, may have been infrequent because they are more embedded in common sense; but they must be reminded in order to guarantee the health and safety in the infant’s food.
Steps 11 and 12 were present on few websites, only three and one, respectively, which is concerning, since eating out is an opportune scenario for the influence of food advertising, from which children must be protected. Progress in the regulation of food advertising in favor of children and youth consumers took a long time to be achieved, as can be seen in the Law no. 11,265/2006,
21 directed to the commercialization of food and products aimed for children up to six years of age, known as NBCAL. This Law had been debated for a few years, but it was only regulated with the publication of Decree No. 9,579 in 2018.
22 Advertisements aimed children and can influence the food choices of both parents/caregivers and the children, thus being harmful to the health of these children, who become doubly susceptible.
23In addition to the above, steps 5, 6, 11 and 12 are the most potentially affected by the political-corporate strategies of the food industry, which may be reflected in the information available on the
websites. According to Mialon and Gomes,
24 most of the political-corporate strategies adopted by the ultra-processed industry are in the informational dimension, that is, they seek to modulate public opinion about its image and products. The effective control and mitigation of these practices can only be acquired through regulation with public policies based on scientific production without conflict of interests, with the objective of promoting the health and well-being of populations.
25It was observed in this study that the level of adequacy in steps 1, 2 and 4 was higher when the
websites did not present advertising, had links with research institutions or official bodies or had some type of reference. This set of results support the hypothesis that food advertising influences the quality of available information. Incomplete or incorrect information about infant feeding can impair the hunger and satiety mechanism, malnutrition and overweight.
26Barriers are recognized for scientific evidence to reach the population.
7,8 In a previous study, an important discrepancy between the information present on popular
websites and the MH recommendations was also observed, which reiterates the challenges of communicating current official recommendations.
10 Health professionals and official information channels have the role of acting as a bridge between science and society, but there are inequalities in access to health services and reliable sources of information.
27The dissemination and implementation of the Guide are important for the access to quality information.
7 The implementation plan must include the production and distribution of educational materials, the inclusion of guidelines in public policies, use protocols for nutritional counseling in Primary Health Care (PHC) and also continuing education for health professionals.
28 In this sense, the Ministry of Health promotes an online course with the recommendations of the Guide entitled: “Breastfeed and feed Brazil: recommendations based on the Dietary guide for Brazilian children under 2 years of age”.
Thus, it can be seen: the urgency of expanding the regulation of content published
online, the importance of continuing education for health professionals, the need for adequate implementation of official recommendations for children under two years of age, and the expansion of scientific dissemination. Such actions have the potential to contribute so that the information disclosed on the internet is aligned with the current Guide
.7The present study has some limitations. First, social media (such as
Twitter, Facebook, Instagram and YouTube) were not evaluated, as the different types of language would require different analysis methods than those defined in this study. In addition, only the first two pages of
Google searches were evaluated, which restricted the volume of information evaluated. However, they were the most accessed pages.
11 It is important to highlight that only 3.7% of the websites collected were updated after the publication of the Guide.
7 It is noteworthy that the document was chosen as a theoretical reference to evaluate the information present online and not to verify the extent of its dissemination.
As highlights, we have the use of Google
Trends to certify that the search terms were appropriate for the purpose of the study and the fact that the duplicate data collection was carried out simultaneously and in a short period, avoiding updates on the
websites that compromised the quality of the collected data. In addition, the inter-rater agreement assessed by
kappa statistics showed that the adequacy criteria were appropriate to the objectives of this study.
It was identified that there is adequate information on popular internet websites regarding the Twelve Steps described in the Guide. However, these are mixed with missing, partially agreeing, disagreeing or contradictory information. Caregivers of infants should be careful when looking for information on the internet and, when possible, consult professionals and official channels to ensure access to reliable and quality information. The results of this work reinforce the importance of developing tools to disseminate the recommendations available in the
Dietary guide for Brazilian children under 2 years of age.References1. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: crescimento e desenvolvimento. Brasília (DF): Ministério da Saúde; 2012. [access in 2021 out 10]. Available from:
http://189.28.128.100/dab/docs/publicacoes/cadernos_ab/caderno_33.pdf2. Cunha AJ, Leite AJ, Almeida IS. The pediatrician’s role in the first thousand days of the child: the pursuit of healthy nutrition and development. J Pediatr (Rio J). 2015; 91: 44-51.
3. Santos CS. Principais problemas encontrados pelas mães de crianças entre cinco e oito meses relativos à transição alimentar atendidas em um Serviço de puericultura do Recife. [dissertação]. Recife (PE): Universidade Federal do Pernambuco; 2004.
4. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde da criança: aleitamento materno e alimentação complementar. 2ª ed. Brasília (DF): Ministério da Saúde; 2015. [access in 2021 out 10]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/saude_crianca_aleitamento_materno_cab23.pdf5. Comitê Gestor da Internet no Brasil. Núcleo de Informação e Coordenação do Ponto BR. TIC domicílios: Pesquisa sobre o uso das tecnologias de informação e comunicação nos domicílios brasileiros. São Paulo: Comitê Gestor da Internet no Brasil; 2019. [access in 2021 out 10]. Available from:
https://www.cetic.br/media/docs/publicacoes/2/12225320191028-tic_dom_2018_livro_eletronico.pdf6. Google [homepage on the Internet]. Google Trends [access in 2020 Mar 7]. Available from:
https://trends.google.com.br/7. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. Departamento de Promoção da Saúde. Guia alimentar para crianças brasileiras menores de 2 anos. Brasília (DF): Ministério da Saúde; 2019. [access in 2020 Mar 7]. Available from:
https://www.svb.org.br/images/guia_da_crianca_2019.pdf8. Ministério da Saúde (BR). Secretária de Atenção à Saúde. Departamento de Atenção Básica. Guia alimentar para a população brasileira. 2
nd ed. Brasília (DF): Ministério da Saúde; 2014. [access in 2020 Mar 7]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2ed.pdf9. Bortolini GA, Moura AL, Lima AM, Moreira H, Medeiros O, Diefenthaler IC,
et al. Food guides: a strategy to reduce the consumption of ultra-processed foods and prevent obesity. Rev Panam Salud Publica. 2019; 43:1-6.
10. Monteiro GS, Assis M, Leite M, Mendes L. Assessing the nutritional information for children younger than two years old available on popular websites. Rev Paul Pediatr. 2016; 34: 287-92.
11. Liu Z, Qiu F, Cho J. Analysis of user web traffic with a focus on search activities. Statistics (Ber). 2005; 103-8.
12. Sim J, Wright CC. The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Phys Ther. 2005; 85: 257-68.
13. Silva KB, Oliveira MI, Boccolini CS, Sally EO. Illegal commercial promotion of products competing with breastfeeding. Rev Saúde Pública. 2020; 54: 10.
14. Universidade Federal do Rio de Janeiro(UFRJ). (UFRJ). Aleitamento materno: Prevalência e práticas de aleitamento materno em crianças brasileiras menores de 2 anos 4: ENANI 2019. [Internet]. Rio de Janeiro (RJ): UFRJ; 2021. Coordenador geral, Gilberto Kac. [access in 2022 Fev 15]. Available from:
https://enani.nutricao.ufrj.br/wp-content/uploads/2021/11/Relatorio-4_ENANI-2019_Aleitamento-Materno.pdf15. Oliveira LP, Assis AM, Pinheiro SM, Prado MS, Barreto ML. Complementary feeding in the first two years of life. Rev Nutr. 2005; 18: 459-69.
16. Universidade Federal do Rio de Janeiro (UFRJ). Alimentação Infantil I: Prevalência de indicadores de alimentação de crianças menores de 5 anos: ENANI 2019. [Internet]. Rio de Janeiro (RJ): UFRJ; 2021. Coordenador geral, Gilberto Kac. [access in 2022 Fev 16]. Available from:
https://enani.nutricao.ufrj.br/wp-content/uploads/2021/12/Relatorio-5_ENANI-2019_Alimentacao-InfantiL.pdf17. Ministério da Saúde (BR). Organização Pan Americana da Saúde (PAHO). Guia alimentar para crianças menores de dois anos. Brasília (DF): Ministério da Saúde; 2002. [access in 2022 Fev 16]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/10_passos.pdf18. Organização Pan Americana da Saúde (PAHO). Guiding principles for complementary feeding of the breastfed child. Washington (DC); 2003. [access in 2022 Fev 16]. Available from:
https://iris.paho.org/handle/10665.2/75219. World Health Organization (WHO). Infant and young child feeding: model chapter for textbooks for medical students and allied health professionals. Geneva: WHO; 2009. [access in 2022 Fev 16]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/44117/9789241597494_eng.pdf?sequence=1&isAllowed=y20. Sociedade Brasileira de Pediatria (SBP). Posição da Sociedade Brasileira de Pediatria diante do Guia de Alimentação do Ministério da Saúde. Rio de Janeiro (RJ): SBP; 2019. [access in 2022 Fev 16]. Available from:
https://www.sbp.com.br/fileadmin/user_upload/ALIMENTACAO_COMPLEMENTAR_MS.pdf21. Presidência da República (BR). Casa Civil. Lei n
o 11.265, de 3 de janeiro de 2006. Regulamenta a comercialização de alimentos para lactentes e crianças de primeira infância e também a de produtos de puericultura correlatos. Brasília (DF): DOU de 4 de janeiro de 2006. [access in 2022 Fev 16]. Available from:
http://www.planalto.gov.br/ccivil_03/_ato2004-2006/2006/lei/l11265.htm22. Presidência da República (BR). Decreto n
o 9.579, de 22 de novembro de 2018. Consolida atos normativos editados pelo Poder Executivo federal que dispõem sobre a temática do lactente, da criança e do adolescente e do aprendiz, e sobre o Conselho Nacional dos Direitos da Criança e do Adolescente, o Fundo Nacional para a Criança e o Adolescente e os programas federais da criança e do adolescente, e dá outras providências. Brasília (DF): DOU de 23 de novembro de 2018. [access in 2022 Fev 16]. Available from:
http://www.planalto.gov.br/ccivil_03/_ato2015-2018/2018/decreto/D9579.htm23. Ueda MH, Porto RB, Vasconcelos LA. Food advertising and children’s food choices. Psicol Teor Pesq. 2014; 30: 53-61.
24. Mialon M, Gomes F. Public health and the ultra-processed food and drink products industry: corporate political activity of major transnationals in Latin America and the Caribbean. Public Health Nutr. 2019; 22: 1898-908.
25. Moodie R, Stuckler D, Monteiro C, Sheron N, Neal B, Thamarangsi T,
et al. Profits and pandemics: prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet. 2013; 381: 670-9.
26. Pizzatto P, Dalabona CC, Correa ML, Neumann NA, César JA. The knowledge of mothers and guardians of children about breastfeeding and complementary feeding. Rev Bras Saúde Matern Infant. 2020; 20 (1): 181-91.
27. Barata RB. Como e por que as desigualdades sociais fazem mal à saúde. Rio de Janeiro (RJ): Editora Fiocruz; 2009.
28. Gabe KT, Tramontt CR, Jaime PC. Implementation of food-based dietary guidelines: conceptual framework and analysis of the Brazilian case. Public Health Nutr. 2021; 24 (18): 6521-33.s
Received on November 19, 2021
Final version presented on July 6, 2022
Approved on August 17, 2022
Authors’ contribution: Santos AA and Silva EO: discussion, planning, data collection and analysis, bibliographic research and article writing. Gabe KT and Leite MA: data analysis, discussion and critical review of the content. The authors approved the final version of the article and declare no conflict of interest.


 ; Evelyn Oliveira da Silva2
; Evelyn Oliveira da Silva2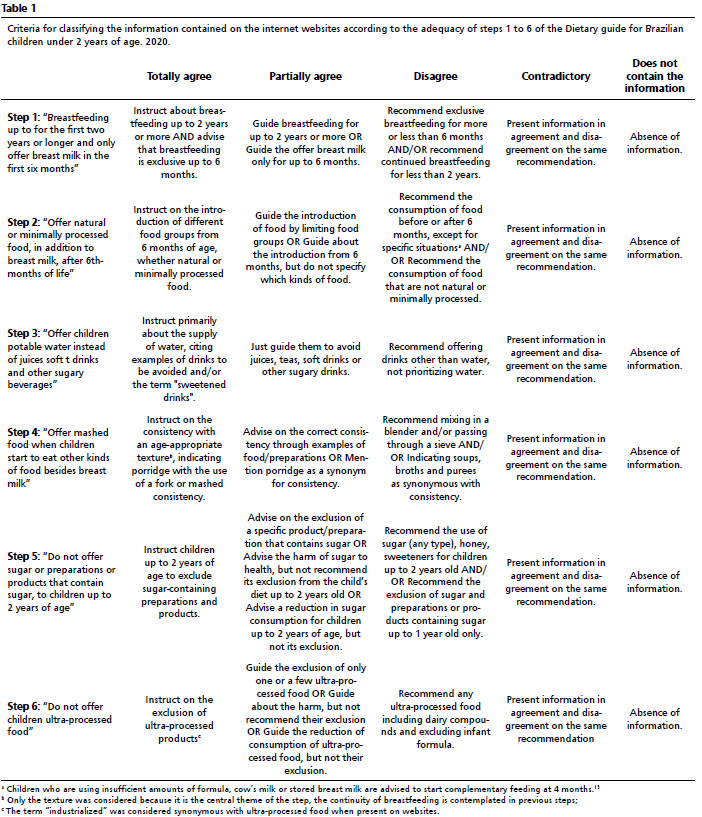






 Ler em português
Ler em português