ABSTRACT
OBJECTIVES: to analyze the impact of the covid-19 pandemic on screening, diagnosis and treatment of breast cancer in Pernambuco, Northeastern Brazil.
METHOD: cross-sectional study, based on secondary data from consultations with a mastologist, ultrasound, mammogram, biopsies, new cases, chemotherapy, radiotherapy and surgery, carried out in women for the screening, diagnosis and treatment of breast cancer, from January to December of the years 2019 to 2021.
RESULTS: the covid-19 pandemic reduced consultations with mastology (46.3%), ultrasounds (34.8%), mammogram (41.5%), biopsy (49.6%), new cases 45.7 % and Surgery 34.6% in 2020 compared to 2019. On the other hand, with the exception of consultations with a mastologist and surgeries, all services where a significant reduction was observed in 2020, increased significantly in 2021 and returned to the same level of production in the pre-pandemic period. The pandemic did not negatively affect the supply of chemotherapy and radiotherapy.
CONCLUSIONS: the findings of this study indicate negative impacts on breast cancer care, due to covid-19, during the first year of the pandemic, especially in consultations with a mastologist and surgery, which continued with low production in 2021. It is reasonable to assume that the reduction observed in procedures may reflect an increase in late diagnoses and a higher mortality rate in the coming years
Keywords:
Breast cancer, Screening, Treatment, Covid-19, Oncology service hospital
RESUMO
OBJETIVOS: analisar o impacto da pandemia da covid-19 nos atendimentos para rastreamento, diagnóstico e tratamento do câncer de mama em Pernambuco, Nordeste do Brasil.
MÉTODOS: estudo transversal, com base em dados secundários de consultas com mastologista, ultrassonografia, mamografia, biópsias, casos novos, quimioterapia, radioterapia e cirurgia, realizadas em mulheres para o rastreamento, diagnóstico e tratamento do câncer de mama, de janeiro a dezembro dos anos 2019 a 2021.
RESULTADOS: a pandemia da covid-19 reduziu as consultas com a mastologia (46,3%), ultrassonografias (34,8%), mamografia (41,5%), biópsia (49,6%), casos novos 45,7% e cirurgia 34,6% no ano de 2020 em relação ao ano de 2019. Por outro lado, com exceção das consultas com mastologista e cirurgias, todos os serviços onde se observou redução significativa em 2020, aumentaram significativamente em 2021 e voltaram ao patamar de produção do período pré-pandemia. A pandemia não afetou negativamente a oferta de quimioterapia e radioterapia.
CONCLUSÕES: os achados deste estudo apontam impactos negativos na atenção ao câncer de mama, em decorrência da covid-19, durante o primeiro ano da pandemia, sobretudo nas consultas com mastologista e cirurgia, que continuaram com baixa produção em 2021. É razoável supor que a redução constatada nos procedimentos poderá refletir em um aumento de diagnósticos tardios e maior taxa de mortalidades nos próximos anos.
Palavras-chave:
Câncer de mama, Rastreamento, Tratamento, Covid-19, Serviço hospitalar de oncologia
IntroductionBreast malignant neoplasm is considered a health problem worldwide due to its high incidence and mortality. In 2020, Brazil was the country with the highest incidence of cancer among 159 countries, with approximately 2,3 million new cases.
1 Brazil ranks first in deaths by cancer within the female population, and has the highest number of neoplasms in the female gender in all regions of the country, except the North region, which ranks the second place.
2The scenario of facing malignant neoplasms in the country and worldwide was already considered a great challenge for health services even before the outbreak of COVID-19 pandemic, this challenge is even higher for countries with public health systems, such as the Unified Health System (SUS - Portuguese acronym) in Brazil, which advocates among its rights, the assurance of integral assistance.
Without considering the context of Covid-19 pandemic, the estimate for breast cancer in Brazil was 74,000 new cases for each year of the 2003-2005 triennial. In 2019, 18,068 women died due to breast cancer in the country.
2The Coronavirus Disease 2019, or Covid-19 is a highly transmissible infectious disease caused by the novel coronavirus Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). In Brazil, the first confirmed case of Covid-19 occurred in February 2020, and in March, the first case of the disease was confirmed in Pernambuco, in June 2020, the state already had 184 (98.9%) municipalities with confirmed cases of Covid-19.
3In the beginning of the viral dissemination, the scarcity of scientific evidence regarding SARs-Cov-2, brought the concerning about the risks the disease would represent for oncologic patients, and what restrictive strategies should be adopted in order to decrease the risk of transmission for oncologic patients.
4In Pernambuco, several nurseries were implemented for patients with SARs-Cov-2, one of the reference services for the treatment of people with Covid-19 was the High Oncological Complexity Center (Cacon - Portuguese acronym). In order to decrease the risk of transmission, it was recommended the suspension of several procedures considered elective. In the oncology area, several studies reported suspensions of consultations, screening exams, diagnosis and cancer treatment.
5-9 Around 90% of countries reported one or more interruptions in essential health services.
9 In Pernambuco, the suspension of elective procedures endured 89 days.
10,11Scientific evidence emerged and indicated higher severity and mortality in the infection by SARS-CoV-2 in oncologic patients, leading health services and patients to avoid exposure due to concerns about contamination, resulting in delays or interruption of activities in oncological services.
12-14 There is direct influence in the mortality indexes related to late cancer diagnosis, which may aggravate if there are delays in exams due to the pandemic, as was observed in England.
15The absence of studies about the impacts of Covid-19 pandemic in relation to diagnosis and treatment for women with breast cancer, in the state of Pernambuco, justifies the conduction of this study, whose contributions will be important for the management, health professionals and the vulnerable population. Since authors intend to identify factors that indicate the magnitude of delays in the care of people with breast cancer, and, therefore, the demands that are currently restricted.
This research aims to analyze the impacts that Covid-19 caused in relation to consultations, screening, diagnosis and breast cancer treatment by means of the review of medical records and other registries available in the High Complexity Oncology Center, in the state of Pernambuco, Northeast of Brazil.
MethodsCross-sectional descriptive study, with quantitative approach, executed with secondary data, from the registry of the number of consultations, screening, diagnosis and treatment of women assisted at the High Complexity Oncological Center of the Institute of Integrative Medicine Professor Fernando Figueira (Cacon IMIP - Portuguese acronym) in Pernambuco.
Data from procedures executed from January to December in the years 2019 (pre-pandemic), 2020 (first year of pandemic and 2021(second year of pandemic).
The used variables about screening were consultations with mastologist, breast ultrasound exams and mammogram. The information used about diagnosis were: executed biopsies and new breast cancer cases. The information on treatment were: oncological breast surgeries, chemotherapy and radiotherapy for breast cancer treatment.
Information about consultations with mastologist, breast ultrasound, mammogram, biopsies and new cases were collected at the "Annual Statistical Report", an internal document of the studied service, and those related to surgeries, chemotherapies and radiotherapies were collected from information sent through Excel software spreadsheets, by Cacon's department of statistics.
In relation to information on radiotherapy for breast cancer treatment at Cacon, they were analyzed at the periods from June to December 2019 and June to December 2020, due to the lack of standardization in the registry of High Complexity Authorization (APAC - Portuguese acronym) for radiotherapy. The procedure of APAC's authorization for radiotherapy became unique, with fix and maximum validity of 3 (three) months, regardless of the number of sessions or duration of radiotherapy, as established by Ordinance number 263, from February 22, 2019.
In the months between January and May, 2019, at Cacon, the radiotherapy procedure was still authorized and registered by each session performed, so that each radiotherapy procedure that the patient did would generate one APAC. After June 2019, the registry of radiotherapy came to be considered a unique APAC, with 3 months validity for the patient, regardless of the quantity of sessions performed. For comparison purposes, we opted to consider the months that had the same way of registration, and thus, it was only possible to execute a comparative analysis in the year 2020 in relation to the same period of the previous year, after June.
A descriptive analysis was performed in order to expose the obtained results. In order to test the supposition of normality of variables involved in the study, the Kolmogorov-Smirnov test was applied, to assess the variation between months, the Friedman nonparametric test was applied, with its respective multiple comparison tests. For comparative analysis of the means between the years (2019-21) the Analysis of Variance (ANOVA) test was used. In order to test multiple comparisons, the Levene test was applied in order to verify the supposition of homogeneity of variances, thus, when it was verified, we used the Minimal Important Difference test (DMS - Portuguese acronym) and when not, the Tamhane test was applied. All conclusions were taken according to the 5% significance level.
Analyses were executed to compare the years 2019 with 2020 with the purpose of analyzing whether there was a decrease in any of the services in the first year of pandemic. From 2019 to 2021, to verify if the numbers returned to the level of the pre-pandemic year. And from2020 to 2021, to identify if there was constancy, decrease or increase in the services offered between the first and second year of Covid-19 pandemic.
The research was approved by the Research and Ethics Committee of Institute of Integrative Medicine Professor Fernando Figueira - IMIP, CAEE 48515121.4.0000.5201, under the opinion: 4.832.181, in July 7, 2021.
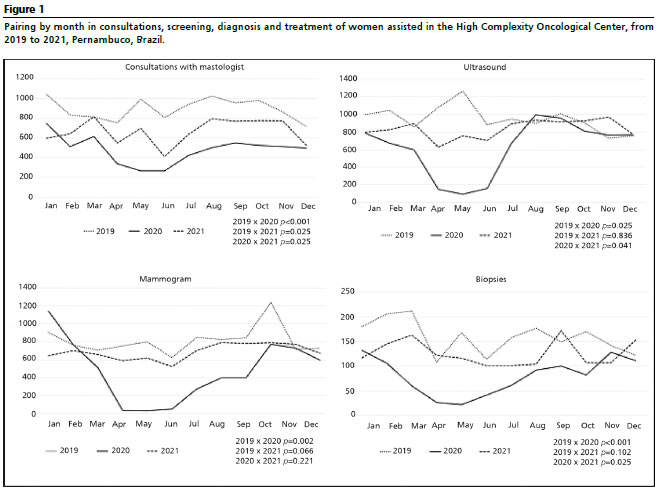
ResultsIn 2019, anaverage of 893.8 consultations with mastology were performed monthly. In 2020, the consultations had an expressive reduction of 46.3% in relation to the year 2019, with a monthly mean of 479.9 consultations. The months of May and June were the most critical in this service in relation to the same period in 2019, with a reduction of 73.1% and 67% of consultations performed, respectively. Statistically significant differences were observed in consultations with mastology in all analyzed periods (Table 1).
In 2021, there was an increase of 38.8% in consultations with mastology in relation to 2020. When analyzing 2019-2021, the consultations in 2021 stood 25.5% lower in relation to the year 2019. Despite the increase in 2021, the service did not return to its production at a pre-pandemic level.
In 2019, a monthly average of 947.2 ultrasound breast exams were performed (USG - Portuguese acronym), observing a decrease of 34.8% in 2020, with a monthly average of 617.5, with a statistically significant difference in relation to the year 2019 (
p=0.014). The months of April, May and June 2020 were those that presented the highest decreases in ultrasound exams in relation to the same period of 2019, with a reduction of 92.9% in May (Figure 1). There was no statistically significant difference in the comparison of the years 2019-2021 (
p=0.122) and 2020-2021 (
p=0.118).
In 2021, an average of 834.3 breast USG were performed monthly. The increase of 35.1% in ultrasounds in the year 2021 in relation to the year 2020 demonstrated that this procedure was able to return to the level of the pre-pandemic period (Figure1) (Table1).
In relation to the main screening test for breast cancer, the mammogram, in 2019 a monthly average of 813.8 exams was performed. There was a statistically significant difference in relation to the period of 2019=2020 (p=0.023). In 2020, there was a reduction of 41.5% of mammogram exams in relation to the year 2019, with an average of 476.3 exams per month. The months of April, May and June 2020 presented a higher reduction compared to the same period of 2019, with a reduction of 96.2% in May (Figure1).
In 2021, there was an increase of 44.5% in the number of mammograms, with a monthly average of 688.1 exams in relation to the year 2020. There was no statistically significant differences between 2019 and 2021 (
p=0.074), and the number of mammograms returned to the level of the pre-pandemic period (Figure 1) (Table 1).
With regard to the biopsies, significant differences were verified in all analyzed periods. In 2020, there was a reduction of 49.6% in the number of biopsies for breast cancer diagnosis, in relation to the previous year (
p<0.001).
In 2019, a monthly average of 158.8 biopsies were performed, and in 2020 the monthly average was of 80.1 biopsies. The most critical months in 2020 were March, April, May and June, with a reduction of 86.9% in May (Figure 1). In 2021, the number of biopsies increased 56.9%, in relation to the year 2020, with a mean of 125.7 per month, a higher number than the year 2020, and lower than the pre-pandemic period, with a statistically significant difference (p<0.001). (Table 1).
There was a statistically significant reduction in the number of new breast cancer cases between the years 2019 and 2020 (
p<0.001). In 2020, the monthly average for new cases was 45.5% lower in relation to the year 2019, being the average of new breast cancer cases, in 2020, of 14.8 cases per month. The months of April, May, June and September demonstrated the lowest registries of new cases, reducing the incidence in 73.1% in May (Figure 1). In 2021, there was an average increase of 71.1% on the number of new cases in relation to the previous year. There was no statistically significant difference between the years 2019 and 2021 (p=0.530), where the average of new cases returned to the level of the pre-pandemic period (Table1).
The number of breast surgeries was statistically significant between 2019 and 2020 (
p<0.001) and 2019 and 2021 (
p<0.001), with a reduction of 34.6% and 39.5% of performed surgeries, respectively. In 2019, an average of 57.8 surgeries were performed monthly, and, in 2020 and 2021, 37.8 and 35.1 surgeries were performed monthly, respectively. In 2020, the months that demonstrated expressive reduction in surgeries were May, June, July, with a reduction of 75.7% in July. The surgery did not return to the pre-pandemic level, observing a reduction of 7.3% of surgeries in 2021, in relation to 2020 (Figure 1) (Table 1).
In relation to the number of chemotherapies performed for breast cancer treatment, it was verified that in 2019 a monthly average of 1264.3 chemotherapies were performed, in 2020, in average, 1324 chemotherapies were performed monthly, and in 2020, there was an increase of 4.5% in relation to the year 2019, with statistically significant difference (
p=0.010). In 2021, the number of chemotherapies was equivalent to that of 2020 (Figure 1) (Table 1).
Impacts with statistically significant differences were not observed in the number of radiotherapies for breast cancer treatment in any of the analyzed periods. (Figure 1) (Table 1).
DiscussionThe results demonstrated statistically significant reductions in the first year of pandemic in consultations with mastology, ultrasound, mammogram, biopsies, new cases and surgeries in relation to the year 2019.
In the comparison of assistances and services provided to oncological care for breast cancer in the first two years of Covid-19 pandemic (2020 and 2021) in relation to the same period pre-pandemic (2019), in High Complexity Oncological Center, it was observed a significant reduction in all procedures focused on the screening and diagnosis of breast cancer, and in the surgery for treatment in the first year of pandemic. In 2021, the procedures returned to the pre-pandemic level, with exception to the consultations with mastologist and surgeries for breast cancer.
As expected, the reduction of procedures started in the first months of 2020, probably related to the suspensions of elective procedures recommended by sanitary authorities.
10-11 With exception to chemotherapy and radiotherapy, the months from April to June 2020 were those most critical for several services of oncological assistance. Of the eight types of procedures analyzed in this study, five presented higher reduction in May 2020. For the Pan-American Health Organization (PAHO), the restrictive measures of displacement and the suspension of procedures lead to an expressive reduction for patients assisted in outpatient clinics and units of oncological reference due to the risk of contamination in health services.
14The suspension of services of oncological care due to Covid-19 pandemic, assessed in this research, was also identified in other countries, such as Holland, which presented a reduction of approximately 40% of cancer incidence generally, and a reduction of 51.3% in breast cancer incidence. In the United States, there was a reduction of 56.9% of cancer cases in general, diagnosed in April 2020, compared to the same month in 2019. And the United Kingdom had significant reductions in referrals for diagnosis of suspect cancer cases, due to the implementation of restrictions due to Covid-19.
4,16-18The suspension of activities recommended by sanitary authorities implied in the reduction of the offer of services, affecting differently the diverse types of cancer. Some kinds of neoplasms were more affected than others during pandemic, among them, the breast cancer, with a 47.7% reduction in the diagnosis.
16 These findings may indicate severe consequences, considering the annual increase of breast cancer incidence, the low coverage of the screening, the high number of cases with advanced staging, growing mortality and low offer of diagnosis services.
18The lower number of new cases demonstrated in the study does not mean a decrease in the incidence of the disease, but a consequence of the non-execution of screening and diagnosis procedures, severely affected in the first year of pandemic. These interruptions in healthcare related to pandemic lead to delays in breast cancer diagnosis, with substantially less cases of detected breast cancer.
19The early diagnosis and treatment of patients with cancer should not be affected during a pandemic.
20 The delay imposed late diagnosis to patients, increasing the risk of a diagnosis in advanced cancer staging, which may compromise the patient's survival.
21 The increase of the risk of Covid-19 infection demanded the temporary suspension of some activities, however, a balance between risk and benefit should had been proposed, demanding an evaluation of each case, observing the urgency of the execution of these procedures.
20The reduction of surgical procedures and significant increase of chemotherapy during pandemic indicate that the approaches of treatment should be quickly adapted into the situation. In a study with women with breast cancer included at the Cancer Registry of Holland and diagnosed during four periods in the weeks, and the authors verified that there was a clear change in the approach of the initial treatment received by patients with breast cancer diagnosed during the pandemic period, with less patients submitted to surgeries and more patients receiving primary hormonal treatment.
22The modifications in the guidelines of oncological treatment during pandemic and the variables associated to patients may also be related to the increase of chemotherapy.
4 There are situationsin which the use of neoadjuvant therapies allow the delay of a surgery without compromising the life of a patient, however, it is necessary to evaluate the condition of the patient with the probability that the disease evolves in the next weeks and recognize the situation of the hospital to execute the procedure.
6A delay of four weeks in cancer treatment is associated with the increase of mortality due to delays in surgery, systemic treatments and indications for radiotherapy for seven types of cancer, breast cancer among them.
23 When considered the three main varieties of treatment (surgery, systemic treatment and radiotherapy), it was verified that a 4 weeks delay in treatment is associated with increased death risk.
In the first year of the pandemic it was already noticed a statistically significant reduction in oncological breast surgeries in the studied service, which prevailed in 2021. The American College of Surgeons recommended surgery restricted to patients with probability of having their survival compromised if the surgery is not performed in up to three months.
6A study carried out in the United States surveyed the relationship between the period since diagnosis until breast cancer surgery in 94,544 patients, and indicated that the specific mortality due to breast cancer evidenced that for surgery there is an increase of 6-8% in the risk of death for each 4 weeks of delay.
23 Before suspending the elective surgery for breast cancer treatment, it is necessary to consider several scenarios facing the pandemic context.
6The effect of cancer progression caused by delay in diagnosis and treatment may increase the number of deaths by oncological disease, whichwould be cured, if properly diagnosed and treated. In this context, the oncological services need to quickly absorb the accumulated delays and mitigate the aggravation and avoidable deaths by cancer.
13,14,21In order not to interrupt assistance, Covid-19 pandemic provoked a digital transformation in healthcare itself, with the dissemination and consolidation of guidelines for the use of telehealth, during the crisis caused by the novel coronavirus.
The use of digital tools in a regulated way provided higher safety to health professionals and the populations, bringing positive impacts when ensuring higher agility and opportune care in face of the crisis. Aiming to avoid contamination and dissemination of the disease, the use of telehealth in oncological patients was reported for remote management of chemotherapy, management of symptoms, general care supervision, palliative care and clinical trials.
25It is essential that the health team perform permanent communication (via phone, SMS, teleconsultation or e-mail) with oncological patients in order to inform about decisions concerning their case and conduct the follow up.
14Telehealth came to be one effective strategy for cancer care in both private and public services. It is implied that the remote assistance to oncological patients should continue after the end of pandemic, since it is a strategy that allows favoring all sectors of society, which still lacks quantity and quality in the population historically excluded, mainly with regard to advances and innovative products.
In the cases in which the public service cannot afford a necessary demand, it is expected that the offer is ensured by the Unified Health System by means of contracts or agreements with the complementary network, with the proper prioritization to oncological patients by means of the readjustment of health services.
23 One of the possible solutions for the increase in agreements with pathology laboratories, is represented by the adequate review of the SUS Table of procedures, which payment of procedures should be compatible with the complexity of the requested services, since the values offered by SUS do not meet the operational cost of the exams.
The results of the study indicate impacts the pandemic brought for breast cancer treatment and this can be extended to other neoplasms that are highly prevalent in the country.
Data reinforce the challenge and the need for health services to restructure the assistance towards the demand that became restricted during the pandemic without compromising the current demand, with no delay for the new cases, since the structure of oncological care network is incipient.
26It is necessary to strengthen the system of assistance regulation, since it makes it possible to follow the scheduling of consultations with mastologists, scheduling and execution of mammograms, ultrasounds and biopsies, and the follow-up to the treatment the patient needs from the schedule to the finalization, without harms to the right to integral assistance, equitable and suitable.
Since the pandemic scenario is still present, the states and municipalities will need to reinforce the strategies of control of the disease, once the access to timely diagnosis and treatment are rights prescribed by law.
27,28 The screening and diagnosis exams returned to the pre-pandemic level, but the treatment by surgery was still reduced in 2020 and 2021, compared to 2019. In order to execute a breast cancer surgery, the risks should be balanced and re-evaluated individually, since they depend on the clinical status of each patient.
29With the availability and development of the Covid-19 vaccine in 2021, studies evidenced that patients with breast cancer tolerate the Covid-19 vaccine during systemic cancer therapy without any additional side effects besides those reported by the general population.
30The reality of oncological care and the impacts brought by Covid-19 evidence the need for reinforcing the effective implementation of care sectors in the healthcare network in its different levels of complexity, with agreement of flows between services in order to quicken the access to integral assistance, according to what is preconized by public policies.
27,28For this, it is necessary the monitoring of health managers, in order to maintain and expand the inclusion of telehealth use in the services continuously, mainly in countries such as Brazil, which possesses several geographical barriers in the access to health services. However, advanced although complex technologies need to be implemented to offer the ideal care.
25 Making it possible the execution of inter-consultations between specialist professionals that the municipality does not possess, strengthening the Permanent Health Education for qualification, updating and standardization of procedures, and allowing the management of therapeutic conduct remotely.
The advances with the telehealth are important and need to continue, although it is essential to prioritize the improvement of the structure of the available diagnosis network, in a proper way, in order to meet the restricted demand of new cancer cases, and the implementation of new public services, which were precarious before the onset of Covid-19 pandemic.
The Unified Health System demands more investments, in the primary level, also specialized and tertiary hospital levels. The demand for services in all levels has been increasing, and the investments have been insufficient in the public sector. The post-pandemic period demands planning and funding to promote the reduction of harms that arouse from the delay in diagnosis and treatment of the restricted demand, in an overloaded and disaggregated system.
18This studied presented some limitations for the comprehension of the impact of the pandemic in the treatment of radiotherapy for breast cancer, due to the change of the APAC registry, when the procedure came to be authorized by a single APAC authorization, with a three months validity, and not by the number of sessions performed anymore. Such change did not allow analyzing statistically the comparison of twelve months in 2020 and 2021 with the same period in 2019.
New studies are necessary to the identification of other impacts of the pandemic in oncology, in order to guide the decision-making process of managers. Using breast cancer as a tracing condition, since it is one of the most prevalent neoplasms in the world, can be favorable to the generalization of possible impacts occasioned by the pandemic in other neoplasms.
In face of the aforementioned scenario, it is necessary a rearrangement of health services to make it possible the return of patients, in conformity with the necessary safety protocols, and to establish the best therapeutic procedure, considering the capability of the service, the situation of Covid-19 pandemic in the place, measures of control of SARS-CoV-2 infection in the health service and the flow of patients with and without Covid-19 in the health unit.
References1. Intenational Agency for Research on Cancer; Word Health Organization. Latest global cancer data: Cancer burden rises to 19.3 million new cases and 10.0 million cancer deaths in 2020. [
Internet]. Lyon (FR): IARC-WHO; 2020. [acesso em 2021 jul 25]. Disponível em:
https://www.iarc.who.int/wp-content/uploads/2020/12/pr292_E.pdf2. Instituto Nacional de Câncer (INCA). Estimativa 2023 - Incidência de Câncer no Brasil. [Internet]. Rio de Janeiro (RJ): INCA; 2019. [acesso em 2021 Jul 26]. Disponível em:
https://www.gov.br/inca/pt-br/assuntos/noticias/2022/inca-estima-704-mil-casos-de-cancer-por-ano-no-brasil-ate-20253. Silva RR, Guilhermino GMS, Oliveira Neto, BL, Lira Neto JB. A Interiorização da covid-19 nos municípios do Estado de Pernambuco, Nordeste do Brasil. Rev Bras Saúde Matern Infant. 2021; 21 (1): 109-20.
4. Araujo SEA, Leal A, Centrone AFY, Teich VD, Malheiro DT, Cypriano AS,
et al. Impact of covid-19 pandemic on care of oncological patients: experience of a cancer center in a Latin American pandemic epicenter. Einstein. 2020; 19: eAO6282.
5. Society of Breast Imaging (SBI). Society of Breast Imaging statement on screening in a time of social distancing. Reston (USA): SBI; 2020. [acesso em 2021 Abr 20]. Disponível em:
https://www.sbi-online. org/Portals/0/Position Statements/2020/SBI-statement-on-screening-in-a- time-of-social-distancing_March-17-2020.pdf6. American College of Surgeons (ACS). Covid-19: elective case triage guidelines for surgical care. Chicago: ACS; 2020. [acesso em 2021 Set 1]. Disponível em:
https://www.facs.org/covid-19/clinical-guidance/elective-case/breast-cancer7. Corrêa KM, Oliveira JDB, Taets GGCC. Impacto na Qualidade de Vida de Pacientes com Câncer em meio à Pandemia de covid-19: uma Reflexão a partir da Teoria das Necessidades Humanas Básicas de Abraham Maslow. Rev Bras Cancerol. 2020; 66 (Tema atual): e-1068.
8. Instituto Nacional do Câncer (INCA). Nota Técnica - DIDEPRE/CONPREV/INCA - 30/3/2020: Detecção precoce de câncer durante a pandemia de covid-19. [
Internet] Rio de Janeiro (RJ); INCA; 2020. [acesso em 2021 Jul 1]. Disponível em:
https://saude.rs.gov.br/upload/arquivos/202004/03141003-covid-19-nota-tecnica-deteccao-precoce.pdf9. World Health Organization (WHO). Covid-19 continues to disrupt essential health services in 90% of countries. Genebra: WHO; 2021. [acesso em 2021 Set 1]. Disponível em:
https://www.who.int/news/item/23-04-2021-covid-19-continues-to-disrupt-essential-health-services-in-90-of-countries.10. Pernambuco. Decreto Estadual nº 48.809, de 14 de março de 2020. Regulamenta, no Estado de Pernambuco, medidas temporárias para enfrentamento da emergência de saúde pública de importância internacional decorrente do coronavírus, conforme previsto na Lei Federal nº 13.979, de 6 de fevereiro de 2020. Pernambuco: Diário Oficial do Estado de 14 mar 2020. [acesso em 2021 Set 1]. Disponível em:
https://legis.alepe.pe.gov.br/texto.aspx?tiponorma=6&numero=48809&complemento=0&ano=2020&tipo=&url=11. Pernambuco. Decreto nº 49.055, de 31 de maio de 2020. Sistematiza as regras relativas às medidas temporárias para enfrentamento da emergência de saúde pública de importância internacional decorrente do novo coronavírus, conforme previsto na Lei Federal nº 13.979, de 6 de fevereiro de 2020. Pernambuco: Diário Oficial do Estado de 31 mai 2020. [acesso em 2021 Set 1]. Disponível em:
https://www.legisweb.com.br/legislacao/?id=39621712. Riera R, Bagattini AM, Pacheco RL, Pachito DV, Roitberg F, Ilbawi A. Delays and Disruptions in Cancer Health Care Due to covid-19 Pandemic: systematic review. JCO Glob Oncol. 2021 Feb; 7: 311-23.
13. Schutte HW, Heutink F, Wellenstein DJ, van den Broek GB, van den Hoogen FJA, Marres HAM,
et al. Impact of time to diagnosis and treatment in head and neck cancer: a systematic review. Otolaryngol Head Neck Surg. 2020; 162 (4): 446-57.
14. Panamerican Organization of Health (PAHO). Recommendations for the progressive reorganization and expansion of health services in response to the covid pandemic 19. Washington: PAHO; 2020. [acesso em 2021 Jul 1]. Disponível em:
https://iris.paho.org/bitstream/handle/10665.2/52214/OPSHSSHSCOVID- 19200018_spa.pdf?sequence=1&isAllowed=y.15. Maringe C, Spicer J, Morris M, Purushotham A, Nolte E, Sullivan R,
et al. The impact of the covid-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study. Lancet Oncol. 2020; 21 (8): 1023-34.
16. London JW, Fazio-Eynullayeva E, Palchuk MB, Sankey P, Mcnair C. Effects of the covid-19 Pandemic on Cancer-Related Patient Encounters. JCO Clin Cancer Inform. 2020 Jul; 4: 657-65.
17. Kaufman HW, Chen Z, Niles J, Fesko Y. Changes in the Number of US Patients With Newly Identified Cancer Before and During the Coronavirus Disease 2019 (COVID-19) Pandemic. JAMA Netw Open. 2020; 3 (8): e2017267.
18. Lôbo CC, Pinheiro LGP, Vasques PHD. Impact of the covid-19 pandemic on breast cancer diagnosis. Mastology. 2020; 30: 1-5.
19. Lowry KP, Bissell MCS, Miglioretti DL, Kerlikowske K, Alsheik N, Macarol T,
et al. Breast Biopsy Recommendations and Breast Cancers Diagnosed during the covid-19 Pandemic. Radiology. 2022; 303 (2): 287-94.
20. Corsi F, Caruso A, Albasini S, Bossi D, Polizzi A, Piccoti F,
et al. Management of breast cancer in an EUSOMA-accredited Breast Unit in Lombardy, Italy, during the covid-19 pandemic. Breast J. 2020; 26 (8): 1609-10.
21. Vrdoljak E, BALJA MP, Marułić Z, Avirović M, Blažičević V, Tomasović C,
et al. Covid ‐19 Pandemic Effects on Breast Cancer Diagnosis in Croatia: a population and registry based study. Oncologist. 2021 Jul; 26 (7): e1156-60.
22. Eijkelboom AH, Munck L, Peeters MTFDV, Broeders MJM, Strobbe LJA, Bos ME MM,
et al. Impact of the COVID-19 pandemic on diagnosis, stage, and initial treatment of breast cancer in the Netherlands: a population-based study. J Hematol Oncol. 2021; 14 (1): 1-12.
23. Hanna TP, King WD, Thibodeau S, Jalink M, Paulin G, Harvey-Jones E,
et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020; 371: 4087-98.
24. Bleicher RJ, Ruth K; Sigurdson ER, Beck JR, Ross E, Wong Y,
et al. Time to Surgery and Breast Cancer Survival in the United States. JAMA Oncol. 2016 Mar; 2 (3): 330-9.
25. Alshamrani M, AlHarbi A, Alkhudair N, AlNajjar F, Khan M, Obaid AB,
et al. Practical strategies to manage cancer patients during the covid-19 pandemic: saudi oncology pharmacy assembly experts recommendations. J Oncol Pharm Pract. 2020; 26 (6): 1429-40.
26. Tribunal de Contas da União (Brasil). Política Nacional de Atenção Oncológica. Relator Ministro José Jorge. Brasília (DF); 2011.
27. Brasil. Lei nº 12.732, de 22 de novembro de 2012. Dispõe sobre o primeiro tratamento de paciente com neoplasia maligna comprovada e estabelece prazo para seu início. Brasília (DF): DOU de 22 de nov 2012. [acesso em 2021 Jul 1]. Disponível em:
https://www.planalto.gov.br/ccivil_03/_ato2011-2014/2012/lei/l12732.htm28. Brasil. Lei nº 13.896, de 30 de outubro de 2019. Altera a Lei nº 12.732, de 22 de novembro de 2012, para que os exames relacionados ao diagnóstico de neoplasia maligna sejam realizados no prazo de 30 (trinta) dias, no caso em que especifica. . [acesso em 2021 Jul 1]. Disponível em: Brasília (DF): DOU de 30 out 2019.
https://www.planalto.gov.br/ccivil_03/_ato2019-2022/2019/lei/l13896.htm29. Ko G, Hota S, Cil TD. Covid-19 vaccination and breast cancer surgery timing. Breast Cancer Res Treat. 2021 Aug; 188 (3): 825-6.
30. Forster M, Wuerstlein R, Koenig A, Amann N, Beyer S, Kaltofen T,
et al. Covid-19 vaccination in patients with breast cancer and gynecological malignancies: a german perspective. Breast. 2021 Dec; 60: 214-22.
Received on September 12, 2022
Final version presented on January 19, 2023
Approved on March 28, 2023
Associated Editor: Aurélio Costa
Author's contribution: Silva RR: planning of survey, data survey and analysis, discussion of results, writing and final evaluation of the manuscript. Lyra TM: orientation of the project, review of the plan of research, data and contribution to the writing and final review of the manuscript. Luna CF: statistical analysis, presentation and discussion of results and final evaluation of the manuscript. Pedroza RM: contribution to the planning of the research, analysis and data and results discussion, as well as the writing and final review of the manuscript. Albuquerque EC: support in the analysis of statistical results and final review of the manuscript. BritoAM: contribution to the writing and final review of the manuscript.
All authors approved the final version of the article and declare no conflicts of interest.


 ; Tereza Maciel Lyra2
; Tereza Maciel Lyra2






 Ler em português
Ler em português