ABSTRACT
OBJECTIVES: to evaluate coverage and identify factors associated with adequate prenatal care for adolescent mothers in Rio Grande, Southern Brazil, in a period of 13 years.
METHODS: over the years 2007, 2010, 2013, 2016 and 2019, a single standardized questionnaire was applied to all mothers at hospital level in this municipality. The outcome consisted of the proportion of puerperae women who started prenatal care in the first trimester and performed 6+ medical visits, completed 2+ HIV, syphilis, and urine tests. Chi-square test was used for proportions, Poisson regression in the multivariate analysis and the prevalence ratio (PR) as measure of effect.
RESULTS: among the 12,645 identified mothers, 2,184 (17.3%) were adolescents. Of this total, 35.2% (CI95%= 33.2%-37.2%) had received adequate prenatal care, ranging from 13.8% (10.8%-16.7%) in 2007 to 52,5% (46.8%-58.1%) in 2019. The adjusted analysis showed a higher PR for adequate prenatal care among those of older age and better schooling level, white/brown skin color, with a partner, never had an abortion, were primiparous and non-smokers.
CONCLUSION: there was substantial improvement in coverage of adequate prenatal care over the period studied, but there is still a long way to go. The increase in this coverage depends on reaching adolescents who are younger, less educated, black skin color, living without a partner, multiparous and smokers.
Keywords:
Prenatal care, Adolescents, Risk factors, Health services research
RESUMO
OBJETIVOS: estimar a realização de pré-natal adequado entre adolescentes no extremo sul do Brasil e identificar fatores associados à sua ocorrência ao longo de 13 anos.
MÉTODOS: em 2007, 2010, 2013, 2016 e 2019, entrevistadoras previamente treinadas aplicaram na maternidade questionário único, padronizado à todas as parturientes residentes no município de Rio Grande, RS. Considerou-se como tendo realizado pré-natal adequado a puérpera que iniciou consultas no primeiro trimestre da gravidez, realizou 6+ consultas e 2+ exames para HIV, sífilis e qualitativo de urina. Utilizou-se teste qui-quadrado para comparar proporções, regressão de Poisson na análise multivariável e razão de prevalências (RP) como medida de efeito.
RESULTADOS: dentre as 12.645 parturientes identificadas, 2.184 (17,3%) eram adolescentes. Destas, 35,2% (IC95%=33,2%-37,2%) realizaram pré-natal considerado adequado, variando de 13,8% (10,8%-16,7%) em 2007 a 52,5% (46,8%-58,1%) em 2019. A análise ajustada mostrou maior RP à realização de pré-natal adequado entre aquelas de maior idade (18-19 anos), de cor da pele branca e parda, vivendo com companheiro, com 9+ anos de escolaridade, que sofreram aborto, primíparas e não fumantes.
CONCLUSÕES: houve substancial melhora na cobertura de pré-natal adequado no período estudado, mas ainda muito aquém do desejado. A melhoria destes índices depende de alcançar adolescentes de menor idade, pior escolaridade, cor da pele preta, vivendo sem companheiro, multíparas e fumantes.
Palavras-chave:
Pré-natal, Adolescentes, Fatores de risco, Avaliação dos serviços de saúde
IntroductionPrenatal care is essential for maternal and child well-being from pregnancy to the first years of life.
1 Guidance and care received during this period curb morbimortality in these population groups and contribute to the children's full growth and development.
1,2Maternal age is an important factor to be considered when performing prenatal care.
3 Adolescent mothers (<20 years old) are at greater risk for eclampsia, puerperal endometritis, and systemic infections than other mothers.
3,4 Moreover, low birth weight, prematurity, and severe neonatal conditions are much more frequent in their children.
3,4 Commonly, adolescents who become pregnant have a worse socioeconomic level.
3-6Most studies evaluating prenatal care place all adolescents in a single category and compare them to other ages. Generally, their indicators are always the worst, especially against those aged 20-29.
6-8Despite this and the fact that they account for almost 20% of births in Brazil,
8 it is rare to find a study evaluating prenatal care only among adolescents.
3,9,10 Generally, it does not matter if they are 12 or 19 years old as they end up being treated as if they were equal.
6-8Furthermore, the criteria used
11-13 to assess prenatal care adequacy must be simplified as they hindered health professionals' use at the primary health care (PHC) level. For this reason, an easy-to-apply criterion was created from the gestational age at the start of appointments, the number of appointments, and laboratory tests performed.
This article aims to estimate adequate prenatal care among adolescents in the extreme south of Brazil and identify factors associated with its occurrence over 13 years.
MethodsThis article is nested in the regular surveys called Perinatal Studies in Rio Grande, RS, Brazil, conducted in this municipality every three years to monitor the pregnancy and childbirth care services offered there.
7 The first was conducted in 2007, followed by 2010, 2013, 2016, and, more recently, 2019.
Rio Grande is a coastal municipality located in the extreme south of Rio Grande do Sul, 300 km off Porto Alegre and 250 km from the border with Uruguay. Its population increased from 195 thousand to 211 thousand over these 13 years. Agribusiness and port activity continue to be the basis of its economy. However, it experienced a certain "economic boom" with the assembly of oil platforms in the 2008-13 period, an activity discontinued in 2016. The public health network comprises two hospitals, one completely public, four medical specialty outpatient clinics, and 36 primary health care (PHC) units.
The puerperae should reside in an urban or rural area of the municipality, have given birth between January 1 and December 31 of the years in which the surveys were conducted, and their child should have weighed at least 500 grams at birth, or 20 weeks of gestational age to be part of the perinatal studies. It is, therefore, a census study. When still in the hospital and within 48 hours after delivery, these puerperae answered a single questionnaire, divided into blocks, including everything from pregnancy planning to the immediate postpartum period.
These questionnaires were always applied by four previously trained interviewers in the month before data collection. This application occurred through daily visits to maternity and nursing wards every day of the week, including weekends and holidays.
A physical questionnaire was used in the surveys from 2007 to 2013. On these occasions, the interviewers coded, revised, and delivered them to the study headquarters. The open-ended questions were coded, revised, and entered twice by different professionals in reverse order. This step was performed using Epi Data 3.1.
14 The comparison of databases and subsequent corrections were made using Epi Info.
15In the 2016 and 2019 surveys, data were entered simultaneously during the interview using tablets and the REDCap (Research Electronic Data Capture) application.
16 The questionnaires were downloaded to the central server and revised at each working day's end. Data were analyzed using the statistical package Stata version 12.
17This study's outcome consisted of adequate prenatal care, which included starting appointments in the first trimester of pregnancy, having six or more appointments, and undergoing at least two tests for HIV, syphilis, and qualitative urine. This information was retrieved from data provided by the mother or the Pregnant Woman's Card. Although most variables are self-explanatory, we should clarify that household income refers to the sum of amounts received by all its residents in the month immediately preceding the interview. These amounts were obtained in Brazilian reais and later, during the analysis, were converted into minimum wages. The interviewer classified skin color. According to the instruction manual, anyone who was not black or white was classified as brown. Schooling refers to the number of years of study completed.
Multivariate analysis was performed using Poisson regression, with robust variance adjustment
18 and following a previously established hierarchical model (Table 1).
19 The measure of effect adopted was the prevalence ratio (PR) with its respective confidence interval of 95 % (CI95%). The adjusted analysis included all variables in the model with a p-value of up to 0.20 associated with the outcome. Thus, all variables with up to this p-value were kept in the model to adjust the next (higher) levels. Wald tests for heterogeneity or linear trend were used for ordinal exposures.
20 All research protocols were approved by the Health Research Ethics Committee (CEPAS) of the Federal University of Rio Grande, linked to the National Research Ethics Committee (CONEP), under the following numbers: 2007 (Opinion 05369/2006); 2010 (Opinion 06258/2009); 2013 (Opinion 02623/2012); 2016 (Opinion 0030-2015); and 2019 (Opinion 278/2018).
ResultsTable 2 shows that more than half of the adolescents were between 18 and 19, about two-thirds lived with a partner, were white, and had seven or more years of schooling. One in every seven had a household income of less than the monthly minimum wage (MMW) and engaged in paid work during pregnancy. At least three-quarters of them did not plan the pregnancy, were having a child for the first time, and received prenatal care in the public sector, and 15% (328) were classified as smokers. Approximately 20% (492) mentioned being treated for systemic arterial hypertension, diabetes mellitus, or depression, resulting or not from pregnancy, while the mean adequate prenatal care over these 13 years was 35.3% (770) (CI95%= 33.2%-37.2%), ranging from 13.8% (71) (10.8%-16.7%) in 2007 to 52.5% (159) (46.8%-58.1%) in 2019.

Table 3 shows that the prevalence of adequate prenatal care ranged from 19.7% (13) for those aged between 11 and 15 years to 41.6% (286) among those with nine years of schooling and over. In the adjusted analysis following a previously defined hierarchical model, variables maternal age, skin color, living with a partner, maternal education, previous abortion, parity, and smoking during pregnancy were significantly associated with the outcome. The PR for adequate prenatal care among adolescents aged 18-19 and white compared to those aged 11-15 and Black was 1.78 (1.02-3.10) and 1.45 (1.13-1.85), respectively. Living with a partner and having nine years of schooling and over showed PR=1.32 (1.12-1.55) and 1.73 (1.22-2.46) compared to those without a partner and with up to four schooling years. The PR for adequate prenatal care among those who had an abortion reached 1.49 (1.15-1.95); on the other hand, it reached 1.72 (1.41-2.11) among primiparous women. The PR for adequate prenatal care was 1.36 (1.11-1.67) among non-smoking pregnant women against smokers.

Coverage of adequate prenatal care among adolescents increased approximately fourfold over these 13 years, from 13.8% in 2007 to 52.5% in 2019. However, almost half of them do not receive adequate prenatal care. The highest prevalence ratios for adequate prenatal care were observed among those of older age, white/brown, living with a partner, with a higher level of education, who had an abortion, primiparous, and non-smokers.
Prenatal care has improved in Brazil, especially in the last two decades.
21 While its beginning is practically universal, the proportion of those who perform adequate prenatal care, regardless of the criteria used, has increased in different locations and regions.
6,8,21 This better outlook can be attributed, above all, to the expanded Family Health Strategy (ESF).
8 It has not been different in Rio Grande. In these 13 years, the number of ESF teams hiked from 10 to 26, and its implementation occurred mainly in rural areas and the city's suburbs, which certainly increased prenatal care coverage, including among adolescents.
In this study, the younger the age of the adolescent, the greater the probability of her not having adequate prenatal care. This is particularly serious in Rio Grande because births among those up to 15 years of age increased by 26% (from 9.7% to 12.2%) in this same period.
7 This situation favors the emergence of different intercurrences throughout pregnancy, delivery complications, low birth weight, prematurity, and hospitalizations in the immediate postpartum period.
4,6,22,23White and brown adolescents had a PR of approximately 40% greater adequate prenatal care than Black ones. The worst coverage observed among Black puerperae has been denounced for a long time.
24,25 Generally, Black pregnant women start prenatal care later and have fewer appointments, clinical procedures, and laboratory tests. This situation holds even after adjusting for demographic, socioeconomic, reproductive, behavioral, and nutritional characteristics.
6,8,26,27 Public policy managers need to tackle this problem more effectively, from program design to training those who deliver care to the client.
25The proportion of Rio Grande do Sul puerperae living with a partner is very similar to that observed in several other locations in Brazil, around 75%-80%.
6,8 In Rio Grande, living with a partner favored adequate prenatal care. The presence of a partner was beneficial for adequate prenatal care and reducing the incidence of low birth weight
6, greater supplementation with folic acid
28 and ferrous sulfate.
29 Thus, regarding prenatal care, having a partner benefits maternal and child health.
No important maternal and child health outcome is exempt from the influence of maternal schooling.
30 Generally, the higher the mother's schooling level, the better her health indicators and those of her offspring.
7,29,30 Although the effect of schooling on the adequacy of prenatal care is more evident when it includes older mothers, therefore with higher education, the results obtained here show that this is already found in adolescence, even with few study years.
Adolescents who suffered an abortion showed a greater PR for adequate prenatal care. We did not find, even for pregnant women of any age, a single study evaluating the possible effect of previous (spontaneous or induced) abortions on performing adequate prenatal care (or not), not even outside Brazil. Almost all studies that evaluate prenatal care only control for demographic, socioeconomic, lifestyle, and behavior characteristics and type of service (public or private) and include only parity when showing reproductive ones.
31-33 It is quite possible that because these women have suffered a traumatic situation, including a potential risk of death, when pregnant again, they take more and better care of themselves, which ends up resulting in better quality prenatal care.
The PR for adequate prenatal care among primiparous women was substantially higher than the others. This result can be attributed to the first delivery's clinical condition, which is a risk situation, but also due to the concern, anxiety, and novelty of the parturient and family members. After this moment, one would assume that subsequent pregnancies, especially if the first one was successful, which occurs in most cases, demand less concern and, thus, multiparous women have a lower PR for adequate prenatal care.
Non-smoking adolescents showed a higher PR for adequate prenatal care. A similar result was observed in Aracaju (SE), where the PR of not performing adequate prenatal care among smokers reached 2.25 (CI95% = 1.69-2.99) compared to non-smoking mothers.
33 This result suggests that some risk behaviors are important factors associated with inadequate use of health services, in this case, prenatal care.
Like so many other studies addressing the subject, at least one limitation needs to be mentioned about how to retrieve the information. Most information derives from the mother's report, not medical or hospital records. Data from the Pregnant Woman's Card were copied, but only half were in possession. Even so, they needed to be more complete, mainly regarding procedures and laboratory tests performed. Some forgetfulness or inaccuracy for one or another referred value may have occurred. If, on the one hand, this does not provide exact information, it at least ensures comparability with other studies, especially population-based ones, invariably affected by this problem.
This study shows that adequate prenatal care among adolescents has improved considerably in the municipality. However, there is still much to be done for their benefit since half of them have not yet reached this condition. It also showed that the factors that most contributed to achieving this condition are not the same as those observed regarding older pregnant women and that, even among adolescents, the magnitude of the effect varies because they are different. Thus, treating them as if they were equal does not seem reasonable because it diminishes the potential impact of interventions and perpetuates inequalities. We need to prioritize the most vulnerable, or we will continue living with high levels of maternal and child morbimortality in an economically thriving country with a universal health system but unequal access.
References1. World Health Organization. WHO Recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO; 2016. [access in 2022 Mai 2]. Available from:
https://www.who.int/publications/i/item/97892415499122. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Atenção ao pré-natal de baixo risco. Brasília (DF): Ministério da Saúde; 2012. [access in 2022 Mar 5]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/cadernos_atencao_basica_32_prenatal.pdf3. Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, Bommarito K, Madden T, Olsen MA,
et al. Maternal age and risk of labor and delivery complications. Matern Child Health J. 2015 Jun; 19 (6): 1202-11.
4. Ganchimeg T, Ota E, Morisaki N, Laopaiboon M, Lumbiganon P, Zhang J,
et al; WHO Multicountry Survey on Maternal Newborn Health Research Network. Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multicountry study. BJOG. 2014 Mar; 121 (Suppl. 1): 40-8.
5. Assis TSC, Martinelli KG, Gama SGN, Santos-Neto ET. Gravidez na adolescência no Brasil: fatores associados à idade materna. Rev Bras Saúde Mater Infant. 2021; 21 (4): 1065-74.
6. Viellas EF, Domingues RMSM, Dias MAB, Gama SGN, Theme Filha MM, Costa JV,
et al. Prenatal care in Brazil. Cad Saúde Pública. 2014;30 (Supl. ): S85-100.
7. Cesar JA, Mendoza-Sassi RA, Marmitt LP. Evolution of care during pregnancy and childbirth in the extreme south of Brazil. Rev Saúde Pública. 2021 Aug; 55: 50.
8. Tomasi E, Fernandes PAA, Fischer T, Siqueira FCV, Silveira DS, Thumé E,
et al. Qualidade da atenção pré-natal na rede básica de saúde do Brasil: indicadores e desigualdades sociais. Cad Saúde Pública. 2017; 33 (3): e00195815.
9. Vaz RF, Monteiro DLM, Rodrigues NCP. Trends of teenage pregnancy in Brazil, 2000-2011. RevAssoc Med Bras. 2016; 62 (4): 330-5.
10. Gama SGN, Szwarcwald CL, Sabroza AR, Branco VC, Leal MC. Fatores associados à assistência pré-natal precária em uma amostra de puérperas adolescentes em maternidades do Município do Rio de Janeiro, 1999-2000. Cad Saúde Pública 2004; 20 (Suppl. 1): S101-11.
11. Kotelchuck M. An evaluation of the Kessner Adequacy of Prenatal Care Index and a proposed Adequacy of Prenatal Care Utilization Index. Am J Public Health. 1994; 84:1414-20.
12. Ministério da Saúde (BR). Portaria nº 569 de 01 de junho de 2000. Institui o Programa de Humanização no Pré-Natal e Nascimento, no Âmbito do Sistema Único de Saúde. Brasília (DF): DOU de 8 de junho de 2000. Seção 1, p. 4-6. [access in 2022 Mar 5]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2000/prt0569_01_06_2000_rep.html13. Coimbra LC, Silva AAM, Mochel EG, Alves MTSSB, Ribeiro VS, Aragão VMF,
et al. Fatores associados à inadequação do uso da assistência pré-natal. Rev Saúde Pública. 2003;37:456-62.
14. Lauritsen JM, editor. EpiData data entry, data management and basic Statistical Analysis System. Odense (DK): EpiDataAssociation; 2000-2008 [acesso em 2017 Oct 20]. Disponível em:
http://www.epidata.dk15. Dean A, Arner T, Sunki G, Friedman R, Lantinga M, Sangam S,
et al. Epi Info
TM, a database and statistics program for public health professionals. Atlanta (USA): CDC; 2011.
16. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research Electronic data capture (REDCap): a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009 Apr; 42 (2): 377-81.
17. Stata Corp. Stata statistical software: release 11.2. College Station (TX): Stata Corporation; 2011.
18. Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003 Oct;3:21.
19. Victora CG, Huttly SH, Fuchs SC, Olinto MT. The role of conceptual frameworks in Epidemiological analysis: a hierarchical approach. Int J Epidem. 1997; 26(1): 224-7.
20. Kirkwood BR, Sterne JAC. Essentials of medical statistics. 2
nd ed. Londres: Blackwell Scientific Publications; 2003.
21. França GV, Restrepo-Mendez MC, Maia MF,Victora CG, Barros AJD. Coverage and equity in reproductive and maternal health interventions in Brazil: impressive progress following the implementation of the Unified Health System. Int J Equity Health. 2016; 15: 149.
22. GBDCM 2015 Child Mortality Collaborators. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016 Oct; 388 (10053): 1725-74.
23. Molina-García L, Hidalgo-Ruiz M, Arredon- do-López B, Colomino-Ceprián S, Delgado-Rodríguez M, Martínez-Galiano JM. Maternal age and pregnancy, childbirth and the puerperium: obstetric results. J Clin Med. 2019 May; 8 (5): 672.
24. Leal MC, Gama SG, Cunha CB. Desigualdades raciais, sociodemográficas e na assistência ao pré-natal e ao parto, 1999-2001. Rev Saúde Pública. 2005; 39: 100-7.
25. Victora CG, Matijasevich A, Silveira M, Santos I, Barros AJ, Barros FC. Socio-economic and ethnic group inequities in antenatal care quality in the public and private sector in Brazil. Health Policy Plan. 2010; 25 (4): 253-61.
26. Almeida AHV, Gama SGN, Costa MCO, Viellas EF, Martinelli KG, Leal MC. Economic and racial inequalities in the prenatal care of pregnant teenagers in Brazil, 2011-2012. Rev Bras Saúde Mater Infant. 2019; 19 (1): 43-52.
27. Holand BL, Fonseca SG, Drehmer M, Bosa VL. Adequacy of prenatal care considering nutritional assistance in Southern Brazil: Maternar Cohort Study. Cad Saúde Pública. 2021 Jul 5; 37 (6): e00130320.
28. Lunet N, Rodrigues T, Correia S, Barros H. Adequacy of prenatal care as a major determinant of folic acid, iron, and vitamin intake during pregnancy. Cad Saúde Pública. 2008; 24 (5): 1151-7.
29. Victora CG, Barros FC, Vaughan JP. The Epidemiology of Inequality: A Longitudinal Study of 6000 Brazilian Children. São Paulo, Brazil: CEBES-HUCITEC; 1988.
30. Farias-Antunez S, Simões VMF, Cardoso VC, Silveira MFD. Sociodemographic profile of primiparous mothers from nine birth cohorts in three Brazilian cities. Cad Saúde Pública. 2021 May 14; 37 (4): e00057520.
31. Silva EPD, Leite AFB, Lima RT, Osório MM. Prenatal evaluation in primary care in Northeast Brazil: factors associated with its adequacy. Rev Sa
úde P
ública. 2019; 53: 43.
32. Mario DN, Rigo L, Boclin KLS, Malvestio LMM, Anziliero D, Horta BL,
et al. Quality of Prenatal Care in Brazil: National Health Research 2013. Ciên Saúde Colet. 2019: 24: 1223-32.
33. Ribeiro ER, Guimarães AM, Bettiol H, Lima DD, Almeida ML, Souza L,
et al. Risk factors for inadequate prenatal care use in the metropolitan area of Aracaju, Northeast Brazil. BMC Pregnancy Childbirth. 2009 Jul; 22; 9: 31.
Received on July 14, 2022
Final version presented on May 16, 2023
Approved on May 17, 2023
Associated Editor: Gabriela Sette
Author's contribution: Cesar JA: study design, data analysis, drafting of the manuscript. Saavedra JS and Marmitt LP: assisted in data analysis and interpretation, drafting of the manuscript. Mendoza-Sassi RA: assisted in data interpretation, drafting of the manuscript. The authors approved the final version of the article and declare no conflict of interest.


 ; Janaína Salomão Saavedra2
; Janaína Salomão Saavedra2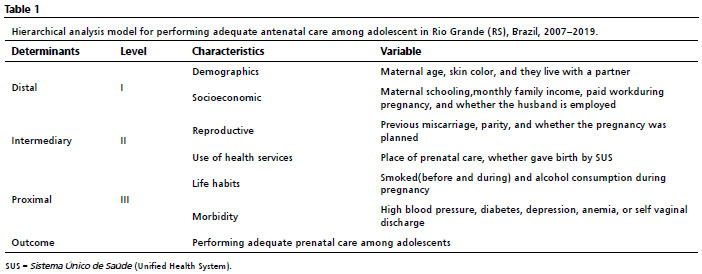








 Ler em português
Ler em português