ABSTRACT
OBJECTIVES: to estimate the prevalence of complementary feeding indicators and investigate its determinants.
METHODS: cross-sectional study with 12-month-old children from Vitória da Conquista, Bahia. The indicators minimum diet diversity, minimum meal frequency and minimally acceptable diet were constructed and adapted to the current recommendations of the food guide for Brazilian children under two years of age. Poisson regression analysis was used, with hierarchical entry of variables in the multivariate model.
RESULTS: the prevalence of minimum diet diversity was 38.8%, minimum meal frequency 47.9% and minimally acceptable diet 18.5%. Family income greater than one minimum wage was associated with minimal diet diversity (PR= 1.49; CI95%= 1.39-2.26); receiving guidance on complementary feeding was associated with a minimum meal frequency (PR= 1.37; CI95%= 1.05-1.78); and children who received exclusive breastfeeding for up to 6 months had significantly higher prevalences of all indicators compared to those who did not.
CONCLUSIONS: low prevalence of complementary feeding indicators was observed. The variables family income, receiving guidance on complementary feeding and offering exclusive breastfeeding for six months were associated with the highest prevalence of the studied indicators.
Keywords:
Infant nutritional physiological phenomena, Infant's nutrition, Healthy diet
RESUMO
OBJETIVOS: estimar as prevalências de indicadores da alimentação complementar e investigar seus determinantes.
MÉTODOS: estudo transversal com crianças aos 12 meses de idade do município de Vitória da Conquista, Bahia. Os indicadores diversidade mínima da dieta, frequência mínima de refeição e dieta minimamente aceitável foram construídos e adaptados às atuais recomendações do Guia alimentar para crianças brasileiras menores de dois anos. Utilizou-se análise de regressão de Poisson, com entrada hierarquizada das variáveis no modelo multivariado.
RESULTADOS: a prevalência de diversidade mínima da dieta foi de 38,8%, de frequência mínima de refeição 47,9% e de dieta minimamente aceitável 18,5%. A renda familiar maior que um salário-mínimo foi associada a diversidade mínima da dieta (RP= 1,49; IC95%= 1,39-2,26); o recebimento de orientações sobre alimentação complementar associou-se a frequência mínima de refeição (RP= 1,37; IC95%= 1,05-1,78); e as crianças que receberam aleitamento materno exclusivo até 6 meses apresentaram prevalências significativamente maiores de todos os indicadores comparadas às que não receberam.
CONCLUSÕES: foram observadas baixas prevalências dos indicadores da alimentação complementar. As variáveis renda familiar, recebimento de orientações sobre alimentação complementar e a oferta de aleitamento materno exclusivo por seis meses foram associadas as maiores prevalências dos indicadores estudados.
Palavras-chave:
Fenômenos fisiológicos da nutrição do lactente, Nutrição do lactente, Dieta saudável
IntroductionIn addition to being fundamental for children's growth and development, food plays an essential role in promoting and protecting health, especially in the first two years of life.
1 Especially in this phase, the insufficient quantity and low quality of complementary food, together with other unhealthy practices, represent a risk to children's health and nutrition.
2,3Indicators for evaluating feeding practices at childhood are central markers for the complementary feeding analysis.
4 Minimum diet diversity (MDD), minimum meal frequency (MMF) and minimally acceptable diet (MAD) are three of the nine complementary feeding indicators proposed by the World Health Organization (WHO) that permit monitoring the aspects related to infant feeding.
1On the national scene, the Ministry of Health (MH) also proposes indicators for evaluating complementary feeding practices, two of which deal with MAD and MMF. These indicators are used as markers of food consumption, serving as care and management tools at various health care levels.
5A data analysis from more than 80 low- and middle-income countries found that only one in four children under the age of two met the criteria for MAD, one in two consumed the recommended daily MMF and only one in six children had a MAD.
2 In Brazil, the
Estudo Nacional de Alimentação e Nutrição Infantil (ENANI-2019)(National Child Feeding and Nutrition Study) reported a MDD prevalence of 57.1% in children aged six to 23 months and a MMF of 39.2% in those aged six to eight months, revealing very sub-optimal feeding practices.
6Some national studies have already evaluated complementary feeding using the indicators proposed by WHO and MH, as well as indicators adapted to previous national recommendations.
7-11 However, at the presente moment, few studies have been published considering the definition of such indicators based on the most recent recommendations presented in the food guide for Brazilian children under two years of age, in addition to the relevance of identifying the factors that influence children's feeding practices, which makes this approach suitable for obtaining new evidence.
6,12In view of this, the aim of this study was to estimate the prevalence of complementary feeding indicators in children at 12 months of age and to investigate their determinants.
MethodsThis is a cross-sectional study, with data from a prospective cohort study entitled "
Acompanhamento das práticas de aleitamento materno e alimentação complementar em crianças menores de dois anos residentes no município de Vitória da Conquista - Bahia", (Follow-up of breastfeeding and complementary feeding practices in children under two years of age living in the city of Vitória da Conquista - Bahia), carried out between February 2017 and October 2019.
13,14 Vitória da Conquista is located in the Southwest region of the State, it is the third largest city in the State of Bahia, with a land area of 3,254.186 km
2, an estimated 343,643 inhabitants in 2021 and a population density of 91.41hab/km.
15 The city has four maternity hospitals, one of which is run exclusively by the
Sistema Único de Saúde (SUS), (Public Health System), another only a private hospital and two others which are assist both SUS and private services.
The cohort that led to this study included puerperal women and their babies who were hospitalized at the time of childbirth in all the maternity hospitals in Vitória da Conquista between March and October 2017. Children whose mothers lived in Vitória da Conquista, with a gestational age of 37 weeks or more, born healthy and not twins were considered eligible for the study. Children born to mothers who were carriers of a human immunodeficiency virus, who had a malformation that impaired breastfeeding, and those who lived in rural areas of the city were excluded.
The sample calculation for the cohort considered the incidence of exclusive breastfeeding (EBF) of 59.3% of children at the end of the first month,
16 relative risk of 1.2, power of 80% and confidence level of 95%. The minimum number of participants was 252, to which 30% was added for possible losses, resulting in a minimum sample of 328 mother-baby pairs. For this study, the sample power was calculated considering a 95% confidence interval and the prevalence of adequacy of each of the indicators investigated (MDD 38.8%, MMF 47.9% and MAD 18.5%), resulting in a power that ranged from 96.3% to 100%.
Participants in the cohort were assessed at birth (baseline) and followed up through home visits at 30 days, six, 12 and 24 months. At the baseline of the cohort from which this study originated, 388 mother/baby pairs were assessed. Over the course of the study, 26.7% of the participants (n=97) were lost due to changes in telephone contact, address or giving up. For this study, the sample consisted of the follow-up at 12 months (n=286).
Data collection at baseline was carried out in the maternity by trained interviewers who collected the information available in the medical records and administered the questionnaire to the puerperal women 24 hours after childbirth. The variables collected at baseline and used in this study were: family income (≤1; >1 minimum wage); maternal schooling (≤8; >8 years of schooling); maternal age (<20; 20-34; ≥ 35 years); parity (primiparous; multiparous); maternal race/skin color (white/yellow; black/mixed); newborn's sex (female; male); birth weight (<2,500g; ≥2,500g). At six and 12 months of age, home visits were made and questionnaires were administered to the children's mothers. From the questionnaire administered at six months, the variable EBF until six months of age was extracted (no; yes), based on the mother's answer to the question: "Until when (days) was the child exclusively breastfed?". Among the data collected at 12-month follow-up, the following variables were used in this study: current maternal work (no; yes); maternal marital status (without a partner; with a partner); receiving guidance on complementary feeding at childcare appointments (no; yes); person responsible for feeding the child (mother and/or father; grandmother/other).
To analyze the complementary feeding indicators, questions were used regarding the receipt of other types of milk besides breastmilk; consistency and frequency of food intake; and food groups consumed the previous day, collected at the 12-month follow-up. To avoid memory bias, the questionnaires were structured to obtain detailed information on food consumption and the respondents were encouraged to describe reliably the food offered to the children the previous day. From this information, we obtained the number of children who met the food consumption criteria, considering the definitions of the complementary feeding indicators, adapted to the recommendations of the food guide for Brazilian children under two years of age.
12The definition of the MDD and MMF indicators proposed by WHO in 2021,
1 as well as by the Ministry of Health in 2015
2 present minimum requirements to be met in the child's diet. However, the current national recommendations presented in the food guide for Brazilian children under the age of two provide guidelines that constitute ideal adequacy targets.
12 Therefore, in this study, these indicators were adapted to characterize local dietary practices using the ideal criteria recommended nationally as a parameter, rather than the minimum established in the original version of the indicators, as described below:
a) MAD: Consumption of food from six food groups on the previous day (breast milk or milk other than breast milk; fruit; vegetables; meat and eggs; beans; cereals and root vegetables);
b) MMF: Daily consumption of five meals with adequate consistency for breastfed children: breakfast, two main meals (lunch and dinner) and two snacks between the main meals; or six meals with adequate consistency for non-breastfed children: breakfast, two main meals (lunch and dinner), two snacks between the main meals and a milk meal (supper);
c) MAD: Combination of MDD and MMF indicators.
Statistical analyses were carried out using Stata software version 14.0 (Stata Corp, College Station, Texas, USA). Descriptive statistics were used to characterize the sample and estimate the prevalence of the complementary feeding indicators assessed, with the qualitative variables expressed as absolute and relative frequencies.
Poisson regression analysis with robust variances was used to assess the associated factors with complementary feeding indicators.Initially, a bivariate analysis was carried out between each outcome and the independent variables, estimating crude prevalence ratios and respective confidence intervals. Next, the variables that showed statistical significance at a level of 20% (
p<0.20) in the bivariate analysis were selected for inclusion in the multivariate model.In the multivariate analysis, the variables were entered hierarchically in blocks, in the following order:Block 1 - Socioeconomic and maternal characteristics; Block 2 - Child's characteristics; Block 3 - Characteristics of feeding practices, according to the hierarchical conceptual model shown in Figure 1, which was constructed based on a previously proposed theoretical model.
17 The variables in the more distal blocks remained as adjustment factors for those in the hierarchically lower block. The statistically significant association (
p<0.05) between a given study factor and each of the complementary feeding indicators, after adjusting for the factors in the same block and in the higher hierarchical blocks, indicated the existence of an independent effect of that factor. The Akaike Information Criterion (AIC) was used to test the quality of the adjustment of the model.
The research project of which this paper is a part of was submitted to and approved by the Research Ethics Committee of the
Universidade Federal da Bahia on December 12, 2016 (CAAE no. 62807516.2.0000.5556 and protocol no. 1.861.163).
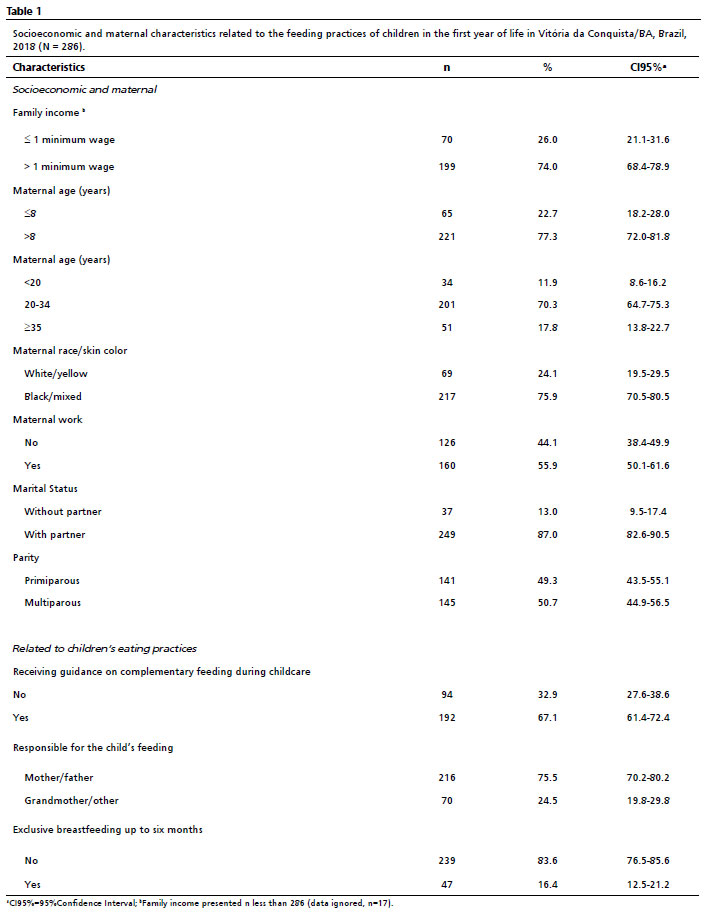
ResultsIn relation to sociodemographic and maternal characteristics, most mothers had a family income of over one minimum wage, more than eight years of schooling, were between 20 and 34 years old and were multiparous. As for the children's feeding practices, 67.1% of the mothers reported having received guidance on complementary feeding from health professionals and 16.4% kept EBF until the child was six months old (Table 1).
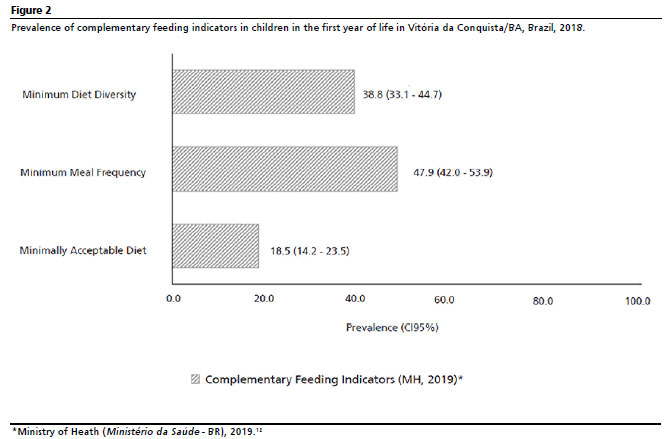
The prevalence of compliance with complementary feeding indicators at 12 months among the studied children was 38.8% (n=111) for MDD, 47.9% (n=137) for MMF and 18.5% (n=53) for MAD (Figure 2).
Based on the bivariate analysis (Table 2), considering
p<0.20, the following variables were included in the multivariate model for the MDD indicator: maternal age, family income, maternal work, receiving guidance on complementary feeding at childcare appointments and EBF up to six months. As for MMF, the following variables were included in the multivariate model: maternal age, maternal work, birth weight, receiving guidance on complementary feeding at childcare appointments and EBF up to six months. Regarding to MAD, the following variables were included in the multiple model: maternal schooling, family income, receiving guidance on complementary feeding at childcare appointments and EBF up to six months.
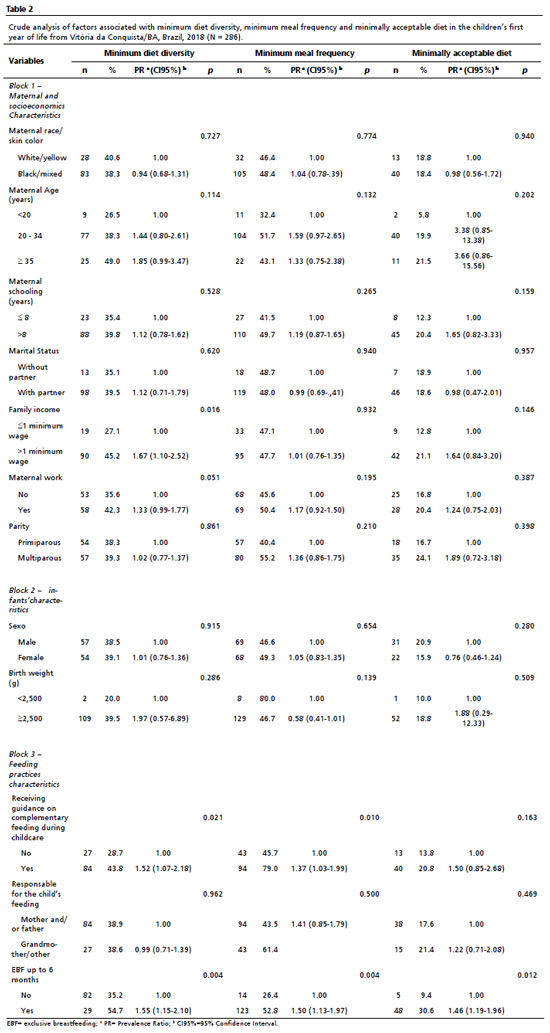
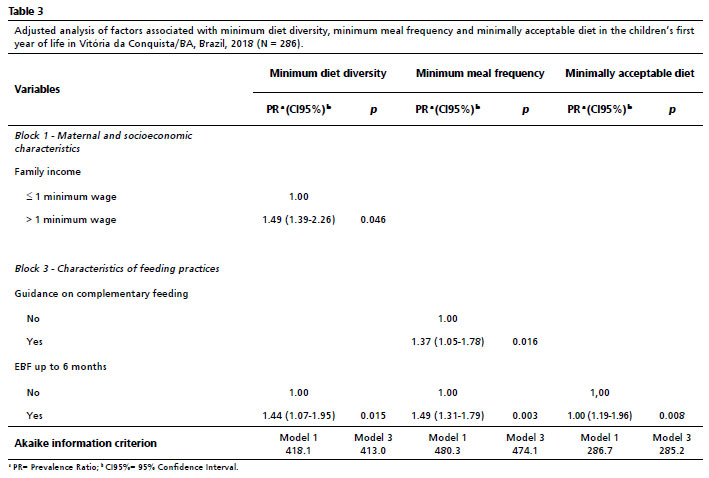
The multivariate analysis showed that the prevalence of MDD was 49% higher among children with a family income of more than one minimum wage (PR=1.49; CI95%=1.39-2.26). Children whose mothers received guidance on complementary feeding during childcare visits (PR=1.37; CI95%=1.05-1.78) had a higher prevalence of adequacy in the MMF indicator. Receiving EBF for six months positively influenced all the indicators. Thus, the prevalence of MDD was 44% higher among children who received EBF up to six months (PR=1.44; CI95%=1.07-1.95), 49% higher for MMF (PR=1.49; CI95%=1.31-1.79) and 46% for MAD (PR=1.46; CI95%=1.19-1.96) compared to children who did not receive EBF (Table 3).
DiscussionAnalysis of the estimates of complementary feeding indicators adapted to current national recommendations, in children at 12 months of age, shows that complementary feeding practices are far from the ideal recommendations in the sample studied. Just over a third of the children received a diet with minimal diversity, less than half consumed the minimum number of meals a day and only approximately one in five children achieved MAD. In addition, higher family income, EBF up to the sixth month of life and receiving guidance on complementary feeding had a positive impact on the prevalence of adequacy of the indicators.
The MDD reflects on the variety of food included in a child's diet that can meet their nutritional necessity for adequate growth and development.
1 When considering the daily consumption of six food groups, a small number of children met the MDD indicator.
Other local studies, carried out between 2006 and 2017 in Brazilian cities with children aged between six and 23 months, corroborate these findings by identifying MDD in only 24% to 35.5% of the children assessed.
8,10,18,19 According to data from ENANI-2019
6, the prevalence for the MDD indicator in the Northeast was 48.5%, a result higher than identified in this analysis, but much lower than the ideal. In this sense, the low prevalence of this indicator is a concern, since a poorly diversified diet can result in a lower intake of micronutrients and, consequently, damage physical and cognitive health, as well as leading to delays in growth in children under two years of age.
20,21In relation to MMF, the results also showed a low prevalence of this indicator, noting that most children did not receive the minimum number of meals recommended by the current national guidelines.
12 These data are similar to the national panorama, confirmed by data from ENANI-2019
6 which found a MMF prevalence in Brazil of only 39.2% among children aged six to eight months, varying from 23.8% to 52% between the five regions of the country. In the Northeast, only 34.6% of the children met the MMF parameters.
6WHO emphasizes that eating less frequently than the ideal, compromises the total daily intake of energy and micronutrients, which can also lead to delayed growth, dwarfism and nutritional deficiencies that can increase the risk of morbidity and mortality at childhood.
1MAD also had a low prevalence in the studied children, which was to be expected since this indicator results from the combination of MDD and MMF indicators. Similarly, a study carried out in 2008 with 76 cities in the State of São Paulo showed a low prevalence of MAD, observed in only 28.9% of the children aged between six and 12 months.
19 Other analyses showed a variation in prevalence of between 20.3% and 46%, which could be attributed to the form this indicator was constructed.
9,11Regarding to the determinants of complementary feeding indicators, higher family income was positively associated with MDD, corroborating other international studies.
22,23 Children from families with higher monthly incomes, they have more financial resources and, have greater access to diversified food than children from low-income families.
24In line with the present study, results from ENANI-2019
6 showed a higher prevalence of MDD and MMF in children whose families had a higher income, but no significant difference. These findings suggest that financial inequality is reflected in the quality of children's diets, with Brazil being one of the nations with the highest income inequality in the world.
25This study also showed that children who received EBF up to six months of age had a higher prevalence of adequacy in all the indicators assessed. A study on Brazilian children aged 6 to 24 months showed that breastfed children who did not have contact with non-human milk are more likely to have a diversified and healthy diet, and are 19% less likely to consume unhealthy food rich in sugar, salt and fat.
26One factor that can influence the acceptance and diversity of food is contact with the flavors of food ingested by mothers through breast milk.
27 Evidence also suggests that women who breastfeed exclusively for six months also try to follow other recommendations about their children eating healthy.
28This study showed that children whose mothers had received guidance on complementary feeding during childcare visits were more likely to be fed by the recommended MMF. In this sense, childcare professionals are essential for promoting healthy complementary feeding.
29Studies show that mothers who have received guidance on feeding their children are more likely to feed their children appropriate food, confirming that healthy eating habits at childhood are influenced by mothers' greater knowledge of appropriate nutrition.
24,30Thus, the results of this study reinforce the importance of health professionals disseminating recommendations on infant feeding, encouraging the adoption of healthy habits at childhood.In this sense, the food guide for Brazilian children under the age of two is an important tool to be used to guide family members on complementary feeding.
12This study has some limitations. Firstly, the use of information on food consumed on a single day, which may not reflect the child's usual diet, although this is the recommended form to assess the diet.
1,5 Another aspect concerns the fact that data collection took place before the publication of the current recommendations in the food guide for Brazilian children under two years of age; however, the previous recommendations do not differ in terms of the number of meals and the presence of all the food groups on a daily basis.
On the other hand, the strength of this study is the use of indicators constructed in accordance with current national guidelines, thus contributing to updating scientific evidence on complementary feeding in the country.
In conclusion, this study showed low prevalence rates for the three complementary feeding indicators in the first year of life. The factors that contributed to the better prevalence of the indicators studied were higher family income, breastfeeding for up to six months and parental guidance on complementary feeding during childcare. This finding reinforces the importance of monitoring these feeding practices in children under two years old to guide the implementation of public actions and policies aiming at healthy complementary feeding, with a view to intensify strategies in improving this reality.
References1. World Health Organization (WHO), United Nations Children's Fund (UNICEF). Indicators for assessing infant and young child feeding practices: definitions and measurement methods. Geneva: WHO/UNICEF; 2021. [access in 2022 Nov 10]. Available from:
https://apps.who.int/iris/bitstream/handle/10665/340706/9789240018389-eng.pdf?sequence=1&isAllowed=y2. Danaei G, Andrews KG, Sudfeld CR, Fink G, McCoy DC, Peet E,
et al. Risk Factors for Childhood Stunting in 137 Developing Countries: A Comparative Risk Assessment Analysis at Global, Regional, and Country Levels. PLoS Med. 2016 Nov; 13 (11): e1002164.
3. Mistry SK, Hossain MB, Irfan NM, Saha M, Saberin S, Shamim AA,
et al. Trends in Complementary Feeding Indicators and Intake from Specific Food Groups among Children Aged 6-23 Months in Bangladesh. Int J Environ Res Public Health. 2022 Jan; 19 (1): 550.
4. Gatica-Domínguez G, Neves PAR, Barros AJD, Victoria CG. Complementary Feeding Practices in 80 Low- and Middle-Income Countries: Prevalence of and Socioeconomic Inequalities in Dietary Diversity, Meal Frequency, and Dietary Adequacy. J Nutr. 2021; 151 (7): 1956-64.
5. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Orientações para avaliação de marcadores de consumo alimentar na atenção básica. Brasília (DF): Ministério da Saúde; 2015. [access in 2022 Nov 10]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/marcadores_consumo_alimentar_atencao_basica.pdf6. Universidade Federal do Rio de Janeiro (UFRJ). Alimentação Infantil I: Prevalência de indicadores de alimentação de crianças menores de 5 anos: ENANI 2019. Rio de Janeiro (RJ): UFRJ; 2021. [access in 2022 Nov 10]. Available from:
https://enani. nutricao.ufrj.br/index.php/relatorios/7. Oliveira DA de, Castro IRR de, Jaime PC. Complementary feeding patterns in the first year of life in the city of Rio de Janeiro, Brazil: time trends from 1998 to 2008. Cad Saúde Pública. 2014; 30 (8): 1755-64.
8. Oliveira MIC, Rigotti RR, Boccolini CS. Fatores associados à falta de diversidade alimentar no segundo semestre de vida. Cad Saúde Colet. 2017; 25 (1): 65-72.
9. Neves AM, Madruga SW. Alimentação complementar, consumo de alimentos industrializados e estado nutricional de crianças menores de 3 anos em Pelotas, Rio Grande do Sul, Brasil, 2016: um estudo descritivo. Epidemiol Serv Saúde. 2019; 28 (1): e2017507.
10. Ortelan N, Neri DA, Benicio MHD. Feeding practices of low birth weight Brazilian infants and associated factors. Rev Saúde Pública. 2020; 54: 14.
11. Leonez DGVR, Melhem ARF, Vieira DG, Mello DF, Saldan PC. Complementary feeding indicators for children aged 6 to 23 months according to breastfeeding status. Rev Paul Pediatr. 2021; 39: e2019408.
12. Ministério da Saúde (BR). Secretaria de atenção primária à saúde. Departamento de promoção da saúde. Guia alimentar para crianças brasileiras menores de 2 anos. Brasília (DF): Ministério da Saúde; 2019. [access in 2022 Nov 10]. Available from:
http://189.28.128.100/dab/docs/portaldab/publicacoes/guia_da_crianca_2019.pdf13. Cirqueira RP, Novaes TG, Gomes AT, Bezerra VM, Netto MP, Rocha DS. Prevalence and factors associated with tea consumption in the first month of life in a birth cohort in the Northeast Region of Brazil. Rev Bras Saúde Mater Infant. 2020; 20 (4): 945-53.
14. Porto JP, Bezerra VM, Netto M, Rocha DS. Introdução de alimentos ultraprocessados e fatores associados em crianças menores de seis meses no sudoeste da Bahia, Brasil. Ciênc Saúde Colet. 2022; 27 (5): 2087-98.
15. Instituto Brasileiro de Geografia e Estatística (IBGE). Cidades e Estados: Vitória da Conquista. [
Internet] 2021. [access in 2022 mai 10]. Available from:
https://www.ibge.gov.br/cidades-e-estados/ba/vitoria-da-conquista.html16. Vieira GO, Martins CC, Vieira TO, Oliveira NF, Silva LR. Fatores preditivos da interrupção do aleitamento materno exclusivo no primeiro mês de lactação. J Pediatr. 2010; 86 (5): 441-4.
17. Boccolini CS, Carvalho ML, Oliveira MIC. Factors associated with exclusive breastfeeding in the first six months of life in Brazil: a systematic review. Rev Saúde Pública. 2015; 49: 91.
18. Lacerda PS, Taques N, Vieira DG, Benneman GD, Brecailo MK, Saldan PC. Estado nutricional de crianças atendidas em centro de recuperação nutricional de Guarapuava-PR. Interagir: pensando a extensão. 2018; 25: 32-46.
19. Passanha A, Benício MHD, Venancio SI. Caracterização do consumo alimentar de lactentes paulistas com idade entre seis e doze meses. Ciênc Saúde Colet. 2020; 25 (1): 375-85.
20. Prado EL, Dewey KG. Nutrition and brain development in early life. Nutr Rev. 2014; 72: 267-84.
21. Tassew AA, Tekle DY, Belachew AB, Adhena BM. Factors affecting feeding 6-23 months age children according to minimum acceptable diet in Ethiopia: A multilevel analysis of the Ethiopian Demographic Health Survey. PLoS ONE. 2019; 14 (2): e0203098.
22. Senarath U, Godakandage SSP, Jayawickrama H, Siriwardena I, Dibley MJ. Determinants of inappropriate complementary feeding practices in young children in Sri Lanka: secondary data analysis of Demographic and Health Survey 2006-2007. Matern Child Nutr. 2012; 8: 60-77.
23. Solomon D, Aderaw Z, Tegegne TK. Minimum dietary diversity and associated factors among children aged 6-23 months in Addis Ababa, Ethiopia. Int J Equity Health. 2017; 16 (1): 181.
24. Ogbo FA, Ogeleka P, Awosemo AO. Trends and determinants of complementary feeding practices in Tanzania, 2004-2016. Trop Med Health. 2018; 46: 40.
25. Bezerra MS, Jacob MCM, Ferreira MAF, Vale D, Mirabal IRB, Lyra CO. Insegurança alimentar e nutricional no Brasil e sua correlação com indicadores de vulnerabilidade. Ciênc Saúde Colet. 2020; 25 (10): 3833-46.
26. Bortolini GA, Giugliani ERJ, Gubert MB, Santos LMP. Breastfeeding is associated with children's dietary diversity in Brazil. Ciênc Saúde Colet. 2019; 24 (11): 4345-54.
27. Maier AS, Chabanet C, Schaal B, Leathwood PD, Issanchou SN. Breastfeeding and experience with variety early in weaning increase infants' acceptance of new foods for up to two months. Clin Nutr. 2008; 27 (6): 849-57.
28. Nunes LM. Efeito de intervenção educativa pró-aleitamento materno e alimentação complementar saudável junto a mães adolescentes e avós maternas sobre a qualidade da alimentação no primeiro ano de vida. [tese]. Porto Alegre (RS): Faculdade de Medicina da Universidade Federal do Rio Grande do Sul; 2016.
29. Moura JWS, Vasconcelos EMR, Vasconcelos CMR, Silva AA, Medeiros KS, Lemos FS,
et al. Promoção da alimentação complementar saudável em menores de dois anos por enfermeiros: revisão integrativa. Rev Enferm Digit Cuid Prom Saúde. 2021; 6: 1-8.
30. Beyene M, Worku AG, Wassie MM. Dietary diversity, meal frequency and associated factors among infant and young children in Northwest Ethiopia: a cross- sectional study. BMC Public Health. 2015; 15 (3).
Received on May 26, 2023
Final version presented on September 4, 2023
Approved on September 26, 2023
Associated Editor: Ana Albuquerque
Acknowledgements: We would like to thank the
Fundação de Amparo à Pesquisa do Estado da Bahia (Fapesb) (Research Support Foundation in the State of Bahia) for the financial support given to the student: Clessiane de Brito Barbosa through a Master's scholarship: Scholarship Grant Term No. BOL0571/2020.
Authors' contribution: Barbosa CB contributed to the analysis, interpretation of data and writing of this article. Magalhães EIS aid to critically review the analysis and intellectual content of the article. Rocha DS contributed to the conception, design, coordination of the study, data collection and critical revision of the content of this article. All the authors have approved the final version of the article and declare no conflict of interest.


 ; Elma Izze da Silva Magalhães2
; Elma Izze da Silva Magalhães2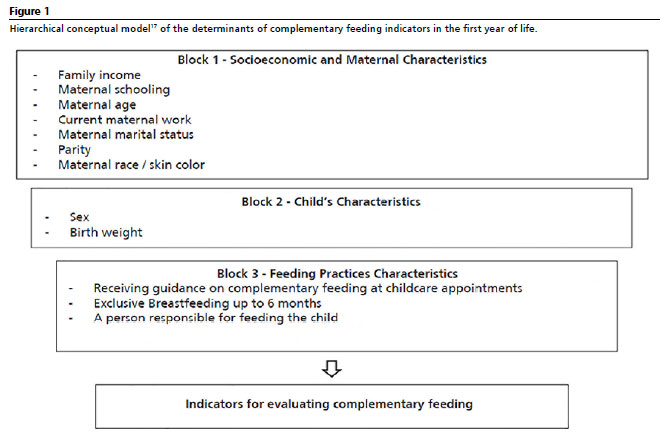







 Ler em português
Ler em português