ABSTRACT
OBJECTIVES: to construct and validate educational videos as part of the LISA Down Program - Literacy and Innovation in Health for Adolescents with Down Syndrome.
METHODS: this is a methodological study of construction and validation of educational videos based on health literacy designed for adolescents with Down syndrome, assisted by an Associação de Pais e Amigos dos Excepcionais (APAE) (Association of Parents and Friends of the Exceptional) located in the Northeast of Brazil. The stages of construction and validation of the vídeos were: pre-production, production and post-production. The storyboards were prepared according to the fundamentals of health literacy and validated by seven expert judges. Subsequently, the storyboards were transformed into videos (production) and these were evaluated by 13 adolescents with Down Syndrome (post-production).
RESULTS: the storyboards totaled 248 scenes, ranging from 39 to 67 scenes each, were approved by the judges with percentages of agreement ranging from 94% to 100%. The vídeos recorded were approved by adolescentes with Down syndrome, in agreement of percentages ranging from 79.17% to 83.33%.
CONCLUSION: the educational vídeos were validated and well evaluated and, therefore, can be used among adolescents in social spaces in which the focus of attention is adolescentes with Down syndrome.
Keywords:
Down Syndrome, Adolescent, Educational video
RESUMO
OBJETIVOS: construir e validar vídeos educativos como parte do Programa LISA Down- Letramento e Inovação em Saúde para Adolescentes com Síndrome de Down.
MÉTODOS: trata-se de estudo metodológico de construção e validação de vídeos educativos fundamentados no letramento em saúde arquitetados para adolescentes com síndrome de Down, atendidos por uma Associação de Pais e Amigos dos Excepcionais (APAE), localizada no Nordeste brasileiro. As etapas da construção e validação dos vídeos foram: pré-produção, produção e pós-produção. Os storyboards foram elaborados de acordo com os fundamentos do letramento em saúde e validados por sete juízes especialistas. Na sequência os storyboards foram transformados em vídeos (produção) e estes foram avaliados por 13 adolescentes com Síndrome de Down (pós-produção).
RESULTADOS: os storyboards totalizaram 248 cenas, variando de 39 a 67 cenas cada um, foram aprovados pelos juízes com percentuais de concordância que variaram de 94% a 100%. Os vídeos gravados foram aprovados pelos adolescentes com síndrome de Down, com percentuais de concordância que variaram de 79,17% a 83,33%.
CONCLUSÃO: os vídeos educativos foram validados e bem avaliados e, portanto, podem ser utilizados entre adolescentes em espaços sociais nos quais o foco da atenção sejam os adolescentes com síndrome de Down.
Palavras-chave:
Síndrome de Down, Adolescente, Vídeo educativo
IntroductionAccording to the
Instituto Brasileiro de Geografia Estatística-(IBGE)(Brazilian Institute of Statistical Geography), in Brazil in 2018 there were about 45 million people with some physical disability and Down Syndrome (DS) was found in one in every 700 births, totaling approximately
This syndrome is characterized by a genetic alteration in chromosome 21, also known as "Trisomy 21". People with this syndrome are more likely to develop chronic health problems, such as heart, visual, and hearing problems, in addition to presenting obesity, respiratory alteration, apnea, and altered thyroid function. Moreover, due to the developmental delays caused by the syndrome, people with DS need educational and support actions to promote self-care, teaching procedures, such as dressing, performing daily personal hygiene activities, and issues related to education, leisure, and health.
2According to the
Constituição da República Federativa do Brasil de 1988 (1988 Constitution of the Federative Republic of Brazil), health is a right of everyone and a duty of the State, which establishes the universal and equal access to actions and services to promote, protect and recover.
3 In this conception, the importance of the Health Literacy (HL) fundamentals should be emphasized in the processes of promoting, protecting and recoverying health, contributing to the development of the individuals and the community's.autonomy
HL refers to the individuals'ability to access, understand, evaluate, and apply health information to make decisions that promote health, prevent and control diseases, and improve the quality of life of these individuals and, consequently, of the collectivity.
4In order to promote HL, health professionals should develop strategies as materials for digital,written and oral communication, such as videos, podcasts, Instagram profiles, among others, that consider the principles and fundamentals of HL, as well as the target audience for which the communication strategies and materials were developed. By promoting lifelong educational actions that consider these issues, we intend to empower individuals and collectivity to improve the quality of life for everyone.
5However, the development of adequate strategies and materials based on HL for people with DS can be a great challenge. From this perspective, LISA, an acronym for
Letramento e Inovação em Saúde (Literacy and Innovation in Health), a trademark registered in
the Instituto Nacional de Propriedade Industrial (INPI)(National Institute of Industrial Property), from the Nutrition and Chronic-Degenerative Diseases research group of the
Universidade Estadual do Ceara (State University of Ceará), aimed to construct and validate educational videos based on HL for adolescents with DS, as part of the LISA Down Program -Adolescents'Literacy and Innovation in Health for everyone as wellDS.
MethodsThis is a methodological study todevelop technical production, specifically the development of didactic material,
6 that is, the construction and validation of educational videos based on HL or adolescents with DS, assisted by an
Associação de Pais e Amigos dos Excepcionais (APAE) (Association of Parents and Friends of Exceptional Children), located in Northeast Brazil.
This presente study is part of a project since 2017 and has not yet been completed, which includes the development of website, applications to use on cell phones, educational videos and podcasts by using via Internet or closed circuit, which will focus on healthy lifestyles in promoting health and in the prevention and control of chronic non-communicable diseases, based on health literacy to use complementary educational actions carried out in the
Sistema Único de Saúde (SUS), (Public Health System). This project is the "
Plano ConectaSaúde: (Plan to Connect Health) allying technological innovation and health literacy to fight against chronic non-communicable diseases".
7The LISA Down Program, in turn, part of the
Plano Conecta Saúde includes three themes that addresses healthy eating for the DS public: obesity prevention and control strategies, hygiene care with food, and personal hygiene care when handling food. In this way, the themes are related to basic activities of daily living.
8The video development process includes three stages: pre-production (synopsis, script, storyboard); production (recording); and post-production (editing).
9In the pre-production stage, the content and its subdivisions, the sequence of the content, and the combined sequence of texts and images for each video were defined:
At the end of this phase, we obtained five storyboards for five interdependent videos that should be watched in the sequence in which they were proposed, referring to the three themes mentioned:
1) Healthy weight protects me from diseases (46 scenes - 5'56"'): what is a healthy weight; how do I know if my weight is healthy; what diseases I can have if I weigh too much?.
2) How to eat healthy (38 scenes - 6'09"'): what is healthy eating; knowing and selecting food to eat; what kind of food is good for your health; what kind of food is bad for your health; how much eatting is important; how can I put together my daily meals.
3) Hygiene care with food - how to buy (67 scenes - 8'42"): selecting safe food to eat; meat, poultry and fish: how to know if they are good; vegetables and fruit: how to choose them; milk, yogurt, cheese and eggs: how to choose them; processed food: looking at the packaging and expiration date.
4) Hygiene care with food - what I should do at home (58 scenes - 7'27"): where to store each type of food; how to store each type of food; how to choose the food to eat first; caring about food before preparing and eating it.
5) My hygiene care before eating (39 scenes - 4'26"): care with my hands; care with the plates, glasses, and cutlery I will use to eat; caring for where I will eat.
The contents of the topics described were based on the guidelines of the
Guia Alimentar para a População Brasileira10 (Food Guide for the Brazilian Population), on the
Diretrizes Brasileiras de Obesidade11 (Brazilian Guidelines on Obesity), and recommendations on food hygiene.
12The written part and the selection of images followed the HL fundamentals contained in a compilation carried out in a previous study.
13 The storyboards were developed in the free version of the Canva® application. The images were extracted from this application or from other platforms with copyright-free images, or relevant photographs were taken.
Once developed, the storyboards were submitted to validate by expertize judges. The selection of the judges was based on their experience and qualification in the area of interest, knowledge about the elaboration of educational material, knowledge about the assumptions of health literacies and about the elaboration of digital materials. The areas of interest were: Health literacy and/or health educational videos and/or health education for adolescents with DS. The ideal number of judges is not consensual, so we followed a recommendation that suggests six to twenty experts,
14 and here, seven judges were included.
Their inclusion criteria were having a master's or doctoral degree and having at least one scientific production on the subject in the last three years. Scientific production included: authorship of a dissertation or thesis on the topic; supervision of a dissertation or thesis on the topic; authorship or co-authorship of books or chapters ofbook on the topic; authorship or co-authorship of an article on the topic; responsibility for a post-graduate course (master's or doctorate) on the topic.
The judges were located by searching the
Plataforma Lattes do Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (Lattes Platform of the National Council for Scientific and Technological Development). The contact took place via e-mail, with a link to access Google Forms, where the following were made available: an invitation letter, the Informed Consent Form, and the storyboards, with the respective evaluation instrument.
We used the
Plataforma Lattes do Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (Lattes Platform of the National Council for Scientific and Technological Development) developed by Leite et al.
15 This instrument has the domains: objective (purpose, goals, purposes); structure/presentation (organization, structure, coherence, and sufficiency); and relevance (significance, impact, motivation, and interest). Each domain has statements that should be scored as follows by the raters: 0 I disagree; 1 I partially agree; and 2 I totally agree. The Content Validity Index (CVI) was calculated considering the responses with a value of 1 and 2 in relation to the total responses, and the instrument was considered approved if the CVI reached 0-80.
6After validating the storyboards, the videos were produced using the Wondershare Filmora
® application. These videos were recorded at home, using an Apple
® cell phone camera, model Iphone 11, with IOS operational system and 128GB capacity.
Each recording began with the speaker (in this case the researcher), who explained the objective of the program and the content of the video, besides introducing the characters who would conduct the content, in this case José (playing the role of nutritionist) and Maria (representing the teenager with DS). The finalization was done by the same speaker, who summarized the approach of the video and announced the content of the next one. In the opening and ending, a background music was made available in the application itself was used.
Regarding the length of the videos, there is no single guideline as to ideal length of time for health literacy educational videos. One study states that there is a greater acceptance by the public when the videos do not exceed five minutes.
16 However, given the lack of consensus on this aspect, we tried to keep the videos short, but at the same time taking care is not the segment of theexcessive content, which could make understanding difficult. Thus, the time obtained varied from four minutes and 26 seconds to eight minutes and 46 seconds, depending on the video.
The strategy used to validate the videos produced by the target audience followed the proposal of the Centers for Medicare & Medicaid Services,
17 being carried out through individual interviews with the 13 adolescents with DS who agreed to participate in the study. It is noteworthy that, during the research, 17 were in follow-up, but four refused to participate in the study.
The adolescents and their guardians came to APAE, on a previously scheduled day, and watched the videos in a room reserved for this purpose. The videos were evaluated by means of an assistive technology assessment tool,
18 which had 14 questions, distributed in the following domains: interactivity; objectives; relevance and effectiveness; and clarity. Each topic could be scored 0 (inadequate), 1 (partially adequate) or 2 (adequate). Immediately after watching, each video was evaluated by the teenagers. For approval, the material should receive a score at least 1 in all topics evaluated by at least 70% of the adolescents.
19The study was approved by the Ethics Committee on Human Research of the academic institution coordinating the study, under the number 4,537,603 and CAAE 69459317.0.0000.5534.
ResultsThe expert judges who participated in the analysis were all female, worked in Collective Health or Public Health, and most had a degree in Nutrition and a post-doctoral degree, according to the data in Table 1.
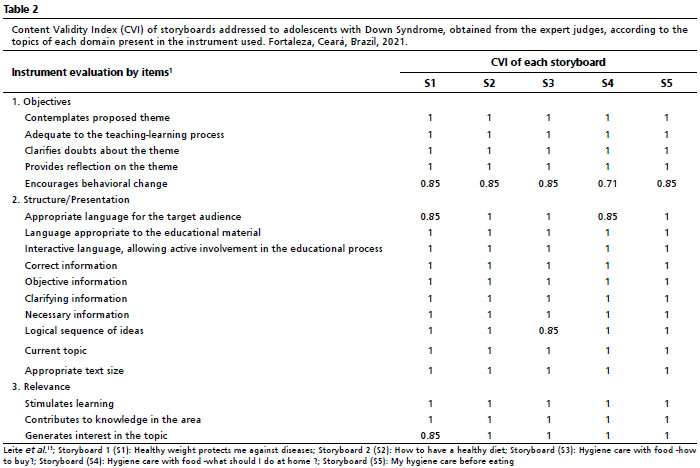
From the analysis of the storyboards by the judges, the CVI of each storyboard, according to the topics of each domain present in the instrument used, was composed of high values, indicating approval of the storyboards built in all criteria evaluated, according to Table 2. It is worth mentioning that Figure 1 presents a cutout of the storyboard 05 as an example of the materials developed.
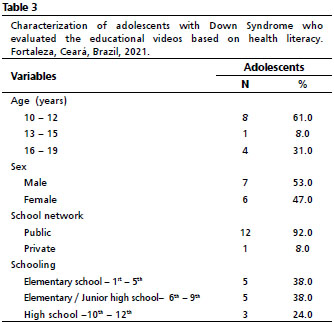
In relation to the target audience, it can be observed, according to Table 3, a majority aged 10-12 years old, students from public schools, mainly enrolled from 1st to 9th grade, and with similar distribution considering the sex.
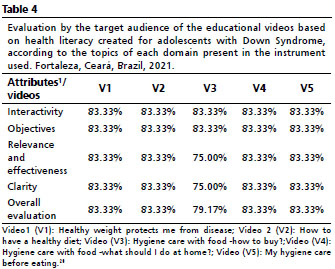
Regarding to the evaluation of the videos by this audience, all the videos were approved, according to data expressed in Table 4. However, regarding to video 3, which addresses the topic "Hygiene care when buying food", the approval percentages were close to the minimum of approval by cut-off point on the relevant and effectiveness and clarifiedtopics.
DiscussionThis study was set out to elaborate and validate videos based on the fundamentals of HL as an educational tool for adolescents with DS. All the developed videos were evaluated by experienced judges in the field and by the adolescents themselves and were approved by both,
In recent years, there has been greater concern with the use of assistive technology as a strategy to disseminate information for some specific audiences, such as the elderly and people with disabilities.
18 Videos, in turn, as an educational tool, allow to have access to information, arousing the curiosity of individuals and facilitating the perception of the developed content, helping in health promotion.
20In the validation process of these educational materials, the judges' analysis step is essential, because they contribute to the enrichment of the final product and to the improvement of its applicability through the reformulation of information, replacement of terms, and review of illustrations. In the study by Moura
et al. ,
21 who also worked with adolescents, but not with DS, the judges were divided into three categories: judges ofcontent (researchers/teachers in the field of adolescent health, educational technologies, and/or instrument validation), six technical judges (professionals with experience in the field of adolescent health); and seven judges with professional experience in design.
In the present study, no such categorization occurred, so the judges needed to evaluate several aspects. However, since all of them had a background in health care, especially nutrition, and all are experienced in HL aspects, there was no prejudice in the evaluation either the content or the technique.
The validation made by the expert judges was done by analyzing the storyboards, not the videos itself. They were approved, considering objectives, structure/presentation, and relevance. It is worth mentioning that the fact that the storyboards have a script and image selection based on HL principles also contributes to a better understanding and facilitates the approval of the material, which is also confirmed by the absence of suggestions for changes. This process of video validation through the storyboards was also used by Lima
et al.
22Specifically for the DS audience, there are few proposals for intervention using educational videos, which justifies the absence of comparative data in this discussion. It is possible to find interventions for adults that involve other themes such as physical exercise, but not on the topic of food. If we think of educational actions aimed at adolescents with DS that include educational videos based on the principles of health literacy, there will be a huge gap in the scientific field.
23Regarding the development of the videos, one of the concerns of the team was their duration. The lack of consensus on this issue, already mentioned, brought uncertainty about the extent to which they would not be too short or too long, which in the latter case could lead to dispersion of the adolescents' attention. However, the length of the videos was not commented by the adolescents. Although not directed to adolescents with DS, some authors developed an educational video on eye health for 5th grade students with a duration of 16 minutes and 14 seconds and managed to keep the audience attentive.
24For adolescents, the importance of service structuring and professional preparation of the health team on adherence to primary care actions is fundamental and is highlighted by Queiroz
et al. 25 As adolescents, they face a series of transformations and need autonomy to be built and strengthened, even more for DS carriers, health education actions face the challenge of monitoring the health team at school, following the whole process, from assessment, intervention, and evolution.
Therefore, it is important to build challenging pedagogical strategies that stimulate people with DS by learning to play and that facilitates the teaching-learning process, such as the use of playful games or technology that allow these people to associate the contents with their world.
26The use of technologies by children and adolescents in general has increased, and these technologies have helped educators to understand that learning does not occur simply through the transmission of information in a vertical way, but is the result of an internal construction process, from interaction processes with the environment, whether it is a physical, digital, virtual, and/or social link. The subject of learning is no longer considered a passive subject, a receiver of information, but an active subject, who acts, interacts, participates and experiments, appropriating knowledge.
27The choice of videos as an educational strategy is pertinent to the condition of the adolescent with DS, because it combines sound and image, motivating them more to concentrate on the contents. To approach health education with adolescents, it is necessary to use devices such as videos that enable the specific teaching and learning process, because they have characteristics inherent to the transition phase between childhood and adulthood.
28Finally, the preparation of videos based on health literacy combines guidelines to maximize understanding of the general population and also follows recommendations to arouse the interest of adolescents with DS, because the topics related to HL, such as language, clarity, use of active voice, short and objective sentences and selection of images appropriate to the content and easy to understand, also integrate the recommendations for this type of audience.
29Many adolescents with DS may have difficulty in learning that requires the use of conventional pencil and pen, due to somemotor limitations, and many may have difficulty in hearing and seeing, in addition to difficulty in understanding some content.
29 The use of health literacy videos allows adolescents to watch them as many times as necessary, at the appropriate volume for themselves, and eliminating the demand for notes.
However, it is necessary, to reflect more on the aspects associated with the evaluation of educational materials by this target audience. But, the number of articles with this object, theme and audience is scarce, so research is needed, since there is no way to be sure whether the appreciated material is fully useful. Moreover, it is unclear what points adolescents observe, beyond formal instruments, to like and/or understand an educational material or not. It is also not clear what kind of activities can be developed by the teacher, from the different educational videos constructed, to broaden the participation of this adolescent.
In conclusion, the videos developed by the LISA Down Program were approved by expert judges and by the target audience, and can be used as educational strategies in the routine and activities developed by APAEs that attends adolescents with DS. Their use can also be applied to other spaces that have adolescents with DS as a focus of attention. To facilitate the access and dissemination of these videos, they were made available on the Youtube platform, in the research group's channel.
30Therefore, this study highlights the need for further research involving the development of various educational materials aimed for adolescents with DS and the insertion of the field of health literacy in the context of successful communication.
References1. Instituto Brasileiro de Geografia e Estatística (IBGE). PNAD Contínua. Acesso à Internet e à televisão e posse de telephone móvel celular para uso pessoal. Rio de Janeiro; 2018. [access in 2022 fev 3]. Available from:
https://ftp.ibge.gov.br/Trabalho_e_Rendimento/Pesquisa_Nacional_por_Amostra_de_Domicilios_continua/Anual/Acesso_Internet_Televisao_e_Posse_Telefone_Movel_2018/Analise_dos_resultados_TIC_2018.pdf2. Ferreira M, Pereira CRR, Smeha LN, Patrícia Paraboni P, Weber AS. Repercussões do Diagnóstico de Síndrome de Down na Perspectiva Paterna. Psicol Ciênc Profissão. 2019; 39: 1-14.
3. Constituição da República Federativa do Brasil de 1988. Brasília (DF); 1988.
4. Parnell TA, Stichler JF, Barton AJ, Boyle DK. A concept analysis of health literacy. Nurs Forum. 2019; 54 (3): 315-27.
5. Perry MA, Devan H, Davies C, Hempel D, Ingham T, Jones B,
et al. iSelf-Help: a co-designed, culturally appropriate, online pain management programme in Aotearoa. Res Involv Engagem. 2022; 8 (1): 6.
6. Polit FD, Beck CT. Fundamentos de Pesquisa em enfermagem: avaliação de evidências para as práticas da enfermagem. 9
th ed. Porto Alegre: Artmed; 2019.
7. Galeno DS, Moreira TMM, Vergara CMAC, Sampaio HAC, Vasconcelos Filho JE. Design de uma tecnologia mHealth para escores de estratificação de risco cardiovascular apoiado no Letramento em Saúde. Saúde Debate. 2020; 44 (126): 656-65.
8. Giacomin KC, Duarte YAO, Camarano AA, Nunes DP, Fernandes D. Cuidado e limitações funcionais em atividades cotidianas-ELSI-Brasil. Rev Saúde Pública. 2018; 52 (Supl. 2): 9s.
9. Musburger RB, Kindem G. Introduction to media production: the path to digital media production. 4
th ed. Boston: Focal Press; 2013.
10. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Guia alimentar para a população brasileira. 2
a ed. 1
a reimpr. Brasília (DF): Ministério da Saúde; 2014. [access in 2022 fev 3]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2ed.pdf11. Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica. Diretrizes Brasileiras de Obesidade. 4
th ed. São Paulo: ABESO; 2016.
12. Morais AHA, Maia JKS, Damasceno KSFSC, Seabra KSFSC, Passos TS. Orientações nutricionais para o enfrentamento do COVID-19.Rio Grande do Norte: Universidade Federal do Rio Grande do Norte; 2020. [access in 2023 fev 18]. Available from:
https://www.asbran.org.br/storage/arquivos/CARTILHAUFRN.pdf13. Brito D, Lopes AS, Filipe B. Texto, imagem e som do interesse do paciente. In: Almeida CV, Moraes KL, Brasil VV. 50 Técnicas Literacia em Saúde na Prática - um guia para a saúde. Mauritius: Novas Edições Acadêmicas; 2020. p. 97-109.
14. Pasquali L. Instrumentação Psicológica: Fundamentos e práticas da enfermagem. Porto Alegre: Artmed; 2010.
15. Leite SS, Áfio ACE, Carvalho LV, Silva JMS, Almeida PC, Pagliuca LMF. Construção e validação de Instrumento de Validação de Conteúdo Educativo em Saúde. Rev Bras Enferm. 2018: 71 (4); 1635-41.
16. Haslam K, Doucette H, Hachey S, MacCallum T, Zwicker D, Smith-Brilliant M,
et al. YouTube videos as health decision aids for the public: an integrative review. Can J Dent Hyg. 2019: 53 (1); 53-66.
17. Centers for Medicare & Medicaid Services. Toolkit for making written material clear and effective. Baltimore: Department of Health & Human Services; 2010.
18. Guimarães FJ, Carvalho ALRF, Pagliuca LMF. Elaboração e validação de instrumento de avaliação de tecnologia assistiva. Rev Eletrôn Enferm. 2015: 17 (2); 302-11.
19. Teixeira E, Mota VMSS. Educação em Saúde: tecnologias educacionais em foco. São Caetano do Sul, SP: Difusão Editora; 2011.
20. Oliveira LMR, Vergara CMAC, Sampaio HAC, Filho JEV. Tecnologia mHealth na prevenção e no controle de obesidade na perspectiva do letramento em saúde: Lisa Obesidade. Saúde Debate. 2018: 42 (118); 714-23.
21. Moura IH, Silva AFR, Rocha AESH, Lima LHO, Moreira TMM, Silva ARV. Construção e validação de material educativo para prevenção de síndrome metabólica em adolescents. Rev Lat Am Enferm. 2017; 25: e2934.
22. Lima MB, Rebouças CB, Castro RCMB, Cipriano MAB, Cardoso MVLML, Almeida PC. Construção e validação de vídeo educativo para orientação de pais de crianças em cateterismo intermitente limpo. Rev Esc Enferm USP. 2017; 51: e03273.
23. Ptomey LT, Szabo AN, Willis EA, Greene JL, Danon JC, Washburn RA,
et al. Remote Exercise for Adults with Down Syndrome. Transl J Am Coll Sport Med. 2018; 3 (8): 60-5.
24. Rodrigues Jr JC, Rebouças CBA, Castro RCMB, Oliveira PMP, Almeida PC, Pagliuca LMF. Construção de vídeo educativo para a promoção da saúde ocular em escolares. Texto Contexto Enferm. 2017: 26 (2); 26 (2): 1-11.
25. Queiroz RO, Moroskoski M, Shibukawa BMC, Uema RTB, Oliveira RR, Higarashi IH. Family and community guidance in adolescence: Assessment in the family health strategy. Rev Lat Am Enferm. 2021; 29: e3457.
26. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Diretrizes de atenção à pessoa com Síndrome de Down. 1a ed. 1a reimpr. Brasília (BR): Ministério da Saúde; 2013. [access in 2022 fev 3]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_atencao_pessoa_sindrome_down.pdf27. Santos MS, Pereira FM, Medeiros AM, Nascimento LS. Uso de tecnologia no desenvolvimento de jogos educativos eletrônicos para a promoção de saúde bucal e Educação Ambiental Rev Thema. 2021: 17 (4); 843-54.
28. Souza VP, Perrelli JG, Neto WB, Pereira MBFLO, Guedes TGG, Monteiro EMLM. Construção e validação de vídeo. Texto Context Enferm. 2022; 31 (e20210171): 1-16.
29. Farias MEL, Lopes Neto D, Llapa-Rodriguez EO. Special education of students with Down Syndrome for self-care. Esc Anna Nery. 2020; 24 (1): 1-7.
30. Nutrindo-Laboratório de Nutrição e Saúde Coletiva. Alimentação saudável para adolescentes com síndrome de Down. 2022. [access in 2022 fev 3]. Available from:
https://www.youtube.com/watch?v=0s1Sdys1clg&list=PLxn_WhZgp7NJHnruR0URDFZ-5Ssu_xd20Received on September 12, 2022
Final version presented on February 4, 2023
Approved on February 8, 2023
Associated Editor: Lygia Vanderlei
Authors' contribution: Silva MCA, Martins AMEBL, Galiza DDF, Melo NFR, Pinto MF: writing of the original manuscript.Cabral LA, Sampaio HAC: writing of the original manuscript, review and editing.
The authors approved the final version of the article and declare no conflict of interest.


 ; Lisidna Almeida Cabral2
; Lisidna Almeida Cabral2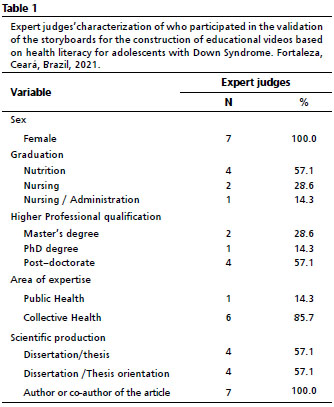







 Ler em português
Ler em português