ABSTRACT
OBJECTIVES: to evaluate the association of pre-pregnancy and current body mass index and the density of dietary macronutrients on underreporting of energy intake at pregnancy.
METHODS: cross-sectional analysis of 327 postpartum women from the city of Mesquita, in Rio de Janeiro. A food frequency questionnaire was administered at maternity ward having the last six months of the pregnancy as the time frame. Energy balance was considered as the outcome, and it was calculated as the division of energy intake by basal metabolic rate (underreport <1.35). Multivariate logistic regression was applied to test the associations between body mass index (pre-gestational and postpartum) on energy balance (underreport or not). Dietary density of protein (4th quartile), carbohydrate (1st quartile) and fat intake (1st quartile) were tested.
RESULTS: mean energy intake was 2,894 kcal and near of 25% of the women were considered as underreported during pregnancy. Obese women had higher chance (OR=1.90; CI95%=1.09-3.33) of being underreported at pregnancy. Underreported women presented greater chance of report dietary intake with higher contents of protein (OR=2.37; CI95%=1.37-4.09) and lower density of fat (OR= .81; CI95%=1.04-3.15).
CONCLUSION: underreported pregnant womenhad higher chance of report great and lower amounts of protein and fat dietary densities.
Keywords:
Pregnancy, Body mass index, Underreporting, Obesity, Energy intake
RESUMO
OBJETIVOS: avaliar a associação entre o índice de massa corporal pré-gestacional e pós-parto e a densidade de macronutrientes da dieta com o sub-relato de energia da dieta na gestação.
MÉTODOS: análise transversal com 327 puérperas da cidade de Mesquita, no Rio de Janeiro. Aplicou-se o questionário de frequência alimentar na primeira semana após o parto tendo como base o consumo dos dois últimos trimestres gestacionais. O balanço energético foi calculado a partir da divisão da ingestão de energia pela taxa metabólica basal (sub-relato<1,35). Adotou-se a regressão logística multivariada para analisar as associações entre os índices de massa corporal e a densidade dos macronutrientes da dieta (proteína, carboidratos e lipídios) com o balanço energético (sub-relato ou não).
RESULTADOS: a ingestão média de energia foi de 2.894 kcal e 25% das mulheres foram classificadas com sub-relato. Mulheres obesas no pós-parto tiveram maiores chances (OR=1,90; IC95%=1,09-3,33) de sub-relato de energia na gravidez e gestantes com balanço energético <1,35 apresentaram dieta com maior densidade de proteína (OR=2,37; IC95%=1,37-4,09) e menor densidade de gordura (OR=1,81; IC95%=1,04-3,15).
CONCLUSÃO: a obesidade no pós-parto foi associada ao sub-relato de energia na gravidez e o balanço energético associou-se a densidade dos macronutrientes da dieta
Palavras-chave:
Gravidez, Índice de massa corporal, Sub-relato, Obesidade, Ingestão de energia
IntroductionUnderreporting of dietary intake is common in nutritional epidemiological studies, even when different methods such as food frequency questionnaires, 24-hour recalls, and food records are used to access the food consumption.
1-5 There is no the better method to assess dietary intake that is most accurate as it is dependent on the aim of your assessment, foods, nutrients, dietary patterns among others aims.
Although the food record is considered the most accurate method to estimate usual dietary intake, all of them have methodological limitations that could bias or misclassify the reporters and confound the direction of the associations.
1-3 Memory bias, random and systematic dietary intake variation, seasonal variation, the perception of the food size portion and food items list are some of issues that must be considered.
2-5 Body mass index (BMI) has been reported as the main predictor of underreporting. Most of the studies on this topic have been conducted with adults and verified that the relation of BMI with underreport may be stronger in women than men.
1-3Few studies have been conducted during the gestational period and have described the association between BMI and dietary intake underreporting among pregnant women.
6-9 Obese pregnant women tend to misinterpret the dietary intake, and most of the times omitting or underreporting higher portions sizes when compared to lower BMI, and, depression, and diet behavior could be considered as independent predictors.
6,7Studies have shown a wide variation in the prevalence of energy underreporting during pregnancy.
6-9 Also, the increasing prevalence of underreporting of energy intake over pregnancy is not a consensus.
6,7,9 McGowan and McAuliffe
8 evaluated 248 healthy Irish pregnant women and verified that 44% were potential underreporters, while 10.9% were classified as definite under reporters. Winkvist
et al.
9 conducted a longitudinal study with pregnant women from Indonesia and showed prevalence of 29.7%, 16.2% and 17.6% of underreporting in the first, second and third trimesters, respectively. According to Moran
et al.
6 38.0% and 59.7% of pregnant women were classified as under-reporters of energy intake at study entry and at 36 gestational weeks, respectively.
Dietary intake during pregnancy should be evaluated with attention because insufficient or high energy and inadequate nutrient intakes may have deleterious effect on maternal weight gain and consequently on gestational outcome.
10-12 Additionally, underreporting pregnant women seem to be less compliant with maternal dietary recommendations
8 what can be harmful to the adequate gestational development. Literature has shown that specific macronutrients as protein and fat, and other nutrients as calcium or food items are often underreported.
1,8,12 It was observed that adult underreported tend to report lower intake of fat
8,13 and sweets
13 and higher consumption of protein
8. A better understanding of the proportion of underreporting of "healthy food", as fruits and vegetables, and the diet density of the nutrients is required.
Considering that few studies were conducted during pregnancy and the importance of the adequate nutrition assessment during this period to achieve desirable maternal and fetal outcomes, it is important to investigate the maternal characteristics, as well as the dietary factors, that are possibly associated with nutritional underreporting among pregnant women. This way may allow better screening for underreporting women, and it may be possible to minimize bias in future studies adjusting by confounders co-variables. Thus, the aim of the present study was to evaluate the association of pre-pregnancy BMI and the macronutrients dietary densities on underreport of energy intake.
MethodsThis is a cross-sectional study with 327 mothers who gave birth to their children in the maternity ward of Leonel de Moura Brizola Municipal Hospital (HMLMB) in Mesquita, that is a county in the State of Rio de Janeiro. This study is part of a larger project entitled 'Effect of nutritional, socio-demographic and reproductive determinants in postpartum weight variation and comorbidities development'. Women who gave birth between February 2009 and February 2011 were invited to participate according to the following eligibility criteria: being aged between 18 and 45 years, presenting single pregnancy and without pre-existing chronic diseases, except for obesity. Of the 338 recruited women, 334 (98.8%) accepted to participate and 7 (2.1%) were excluded from the analysis because their reported energy intake was above 6,000 kcal, which was considered implausible.
14,15Structured questionnaires were administered in the maternity ward in the first week after delivery in order to obtain information on sociodemographic conditions. Trained nutritionists were responsible for data collection and the anthropometric measurements, which were conducted in accordance to the Lohman protocol.
16 Information on the following socio-demographic variables was collected: age (years), schooling (years), family income (US$), skin color (black and brown or white and other), married or stable union (yes or no) and parity (number of births).
The outcome of the present study was energy balance (EB). This variable was calculated dividing energy intake (EI) by basal metabolic rate (BMR). The BMR calculation was based on the Harris-Benedict equation that considers weight (kg), height (cm) and age (years).
17 Values of EB lower than 1.35 were used to classify dietary underreporting among population.
18Dietary intake was obtained through the application of a Food Frequency Questionnaire (FFQ) with 81 food items in the maternity ward, having the last six months as time frame of pregnancy. The FFQ was previously validated by Sichieri and Everhart.
19 The FFQ had portions described as household measures according to Pinheiro
et al.
20 and nine frequencies of consumption that ranged from: never or almost never; one to three times per month; once a week; two to four times a week; five or six times a week; once a day; two or three times a day; more than three times a day. Afterwards, the information was converted to daily frequenciesusing a program developed by Sichieri
21 in the statistical package Statistical Analysis System version 9.3. The Brazilian Food Composition Table
22 was used as the main nutritional composition database for the conversion of food into macronutrients (protein, fat and carbohydrate and energy. The density of the dietary intake (grams/energy) was calculated for each macronutrient and, then, a binary variable was created considering the quartile of the intake: density of protein (4
thquartile versus others); density of carbohydrate (1
stquartile versus others); and density of fat (1
st quartile versus others).
Pre-pregnancy weight (PPW), pre-pregnancy body mass index (PPBMI), current body mass index (BMI) at immediate postpartum and gestational weight gain (GWG) were the anthropometric variables assessed. The information of PPW was obtained from the prenatal card, if measured before the 13
th gestational week. If not available, it was self-reported. Postpartum weight (kg) and height (m) were measured at the maternity ward in the first week after the delivery using a Tanita
® digital scale (Tanita Inner Scan, Tanita Corporation of America, Inc., Illinois, USA and Altura Exata
® portable stadiometer, respectively. For the anthropometric measurements, the participants used light clothing and had their shoes removed. PPBMI and current BMI were calculated by the formula: BMI= weight (kg)/height (m
2). BMI ≥ 25 kg/m
2 and BMI ≥ 30 kg/m
2 were adopted as the cutoff points for classifying overweight and obesity in the pre-pregnancy period.
23 The current BMI considered the cutoff point just to classify as obese women (or no).
Initially, nutritional status (PPBMI, BMI, PPW and GWG), energy intake (kcal), macronutrients dietary densities (protein, carbohydrate and fat, and socio-demographic characteristics [maternal age (years), parity (n), schooling (years), family income (us dollar), civil status (married and stable union or single and others) and skin color (Black and Brown or White and others) of the 327 postpartum women were compared according to EB status (≥1.35 or <1.35) using Student's t-Test to compare means or chi squared test for proportions. Secondly, all the variables were stratified according PPBMI (≥25 kg/m
2) or not and BE (≥ or <1.35 status).
Multiple logistic regression model was used to estimate the effect of PPBMI [obese (1) or no obese (0); overweight (1) or no overweight (0)] on EB [≥1.35 (1) or <1.35 (0)]. The adjustment of the model considered the background available in the scientific literature and the covariates that were represented as confounders (ancestor of the outcome and exposure by the DAGitty methodology (version 3.0). The multiple models for each predictor were adjusted for maternal age and skin color. All analyzes were conducted in SAS.
The present study was approved by the Research Ethics Committees of the Institute of Social Medicine of UERJ (Protocol number: CAAE - 0178.0.314.000-10). The context, procedures and objectives of the study were explained to the pregnant women and the ones who accepted to voluntarily participate gave their informed consent after all clarifications were made. Methodology was compliant with STROBE guidelines.
24ResultsPregnant women assessed at postpartum presented mean (SD) PPBMI of 23.6 kg/m
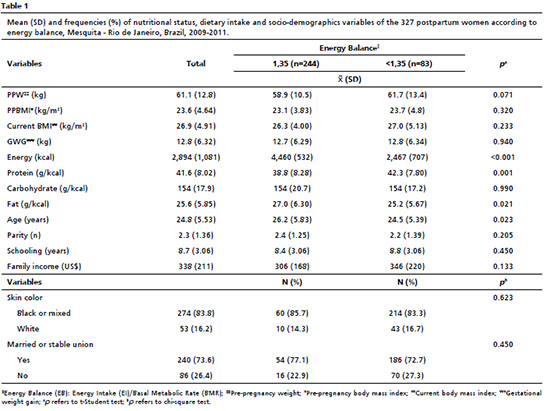
2 (4.64) and maternal age of 24.8 (5.53) years old. Of the 327 women assessed, 83 (25.4%) were classified as underreported, and these women reported greater amounts (Figure 1) of protein dietary density [42.3 g/kcal (7.80)
versus 38.8 g/kcal (8.28);
p=0.001] and lower contents of fat density [25.2g/kcal (5.67)
versus 27.0g/kcal (6.30);
p=0.021] than pregnant who did not underreport (Table 1).
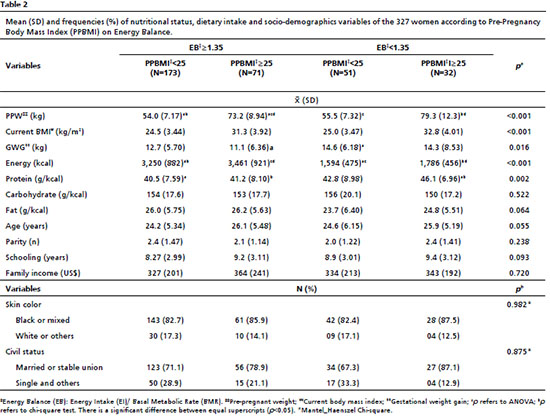
Furthermore, underreported overweight women reported higher contents of protein intake (
p=0.002) than women without excess of weight and with EB≥1.35 (Table 2).
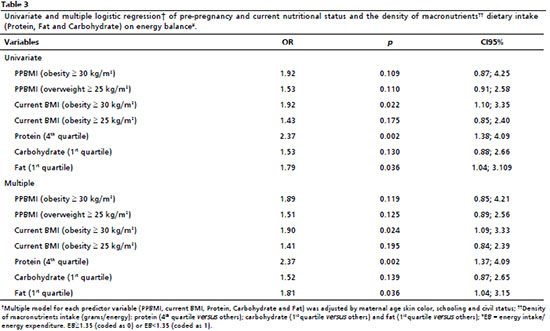
According to the multiple logistic models, current obese (BMI≥30 kg/m
2) women (OR=1.90; CI95%=1.09-3.33;
p=0.024) had higher chance of being classified as underreported. It was shown in the Table 3, that underreported women presented greater risk of report higher density of protein (OR=2.37; CI95%=1.37-4.09;
p=0.002) and lower density of fat intake (OR=1.81; CI95%=1.04-3.15;
p=0.036).
DiscussionThe main finding of the current study is that underreported pregnant women tend to report greater and lower density of protein and fat, respectively. Also, current obese women had higher chance of being classified as underreported women when compared to normal weight counterparts. Approximately twenty-five percent of the study subjects were classified as under-reporters and among then, more than one third was classified with excess of weight.
According to the scientific literature, the BMI seems to be the most consistent predictor of underreported intake,
25,26 although actual age, income and schooling
26 are also commonly cited as important ones. In a sample of 248 pregnant women studied by McGowan & McAuliffe,
8 the total prevalence of underreporting was up to 45%. This study results shows a higher prevalence of underreporting with increasing BMI, in line with our results. Winkvist
et al.
9 assessed dietary intake of pregnant women performing six repeated 24-hour diet recalls in each gestational trimester and authors found a decreasing prevalence of underreporting from the first to the third gestational trimesters. However, the authors did not stratify their analysis according to BMI. The differences in the proportions of underreporting in studies with pregnant women may be due to the different cut-off points used to definethis outcomethat has been frequently used in literature.
Previous studies have described associations between nutritional status and underreporting of dietary intake. Energy underreporting varies as a function of pre-pregnancy BMI and among obese pregnant women.
6,7 According Ravelli and Schoeller,
27 obese people are more likely to underreporting energy intake by 7% more than those with adequate BMI. Authors mentioned the association of underreporting and individual's concerned weight.
More specifically, during pregnancy, a cohort study
8 evaluated 248 Irish women between 12 and 20 weeks of gestation and identified that the higher category of BMI (≥25 kg/m
2) was associated with higher odds of energy underreporting (OR=4.40; CI95%=2.48;7.67) compared to normal weight women (<25 kg/m
2). In the study of Winkvist
et al.,
9 early pregnancy BMI was significantly associated with higher risk of being an under-reporter in all pregnancy trimester. The results of these previous studies conducted with adult samples and with pregnant women are in line with our findings, that showed an inverse association between PPBMI and EB.
Another important question is the direction of the misreporting and the bias that uncontrolled systematic error could introduce among interpretations and leading to erroneous conclusions. Pregnant women may report their dietary intake in socially and health desirable way as observed by Scagliusi
et al.
28 among 38 healthy women. In our study, it was observed that pregnant women with higher BMI underreported dietary fat intake and overestimated protein intake. This unequal direction of the amounts of macronutrient intake was described later by Johansson
et al.
13 They observed that under-reporters reported a significantly higher protein density diet and lower intake of fat among 193 Swedish respondents. As well as our results, no difference was observed between under-reporters or normal reporters in relation to carbohydrate intake. According to Ravelli and Schoeller,
27 the protein intake is underreported in a lower percentage than carbohydrate and fat. McGowan and McAuliffe
8 observed that the mean percentage intake of protein (higher) and fat (lower) were significantly different across energy reporting groups.
The limitations of the present study are mostly related to the study design. Cross-sectional studies do not allow assumptions of temporality once both measures are assessed in a single moment in time. The impossibility of measuring the basal metabolic rate (BMR) or total energy expenditure using gold standard methods such as the double labeled water may also be considered a limitation. On the absence of the gold-standard method, researchers have used the ratio of EI/BMR proposed by Goldberg
et al.
29 and considering values lower than 1.35 to classify underreporting. During pregnancy it is necessary a steady rate between energy intake and expenditure, as lower rates values do not support body weight gain throughout pregnancy. In addition, the recall bias is inherent to retrospective assessment of dietary intake, but we could have minimized it using a validated FFQ.
Despite this drawback, inherent to cross-sectional studies, it is important to highlight that our hypothesis was carefully designed considering previous studies that have already described the temporal plausibility of our main hypothesis. We tried to evaluate social and demographic variables, which may also be potential confounders. Thus, we have selected the confounders based on the biological plausibility and based on DAG arrangement.
Our results were based on valid measures widely used in epidemiological studies, that are feasible to be collected for tracking subgroups in nutritional care. The instrument used to measure dietary intake has been previously validated
19 and other researchers have reported good validity and reproducibility of this method when used during gestational and postpartum periods.
15The choice of the cutoff point of EB considered the fact of FFQ has the last six months of pregnancy as a time frame. The insufficient EI among this period would be incompatible with GWG during pregnancy. Besides this, according toa review conducted by Livingstone and Black,
30 it was showed that the correlation of EI and energy expenditure measured by different dietary assessment could range from 0.76 and to 1.24 using accurate techniques such as doubly labeled water.
Finally, we relight that more studies should be conducted to understand the risk of being underreported at pregnancy. In our study was found that the probability of underreporting is higheras BMI increases andit increases the risk of report diets with high contents of protein and low densities of fat. Methods accounting for under and over self-reported EI with plausible energy requirements, as multiples of resting metabolic rate recommended by Goldberg
et al.,
29 increase the validity of the information excluding from the analyses misreporting people.
In summary, our data corroborate previous studies that evaluated the association between BMI and underreported dietary intake. We identified that this association also occurred when women in the immediate postpartum reported their food intake throughout pregnancy. Also, to be an obese-postpartum women was associated with underreported at pregnancy, pointing out that nutritional status should be considered to identify women that potentially sub-report their gestational food intake. Besides underreporting, it was showed that dietary macronutrients weren't reported in equal way too. To be classified as pregnant under-reporters increased the chance to relate a higher diet protein density.
References1. Freedman LS, Commins JM, Moler JE, Arab L, Baer DJ, Kipnis V,
et al. Pooled results from 5 validation studies of dietary self-report instruments using recovery biomarkers for energy and protein intake. Am J Epidemiol. 2014; 180: 172-88.
2. Willett WC. Nutritional epidemiology. 2
nd ed. New York: Oxford University Press; 1998.
3. Nybacka S, Forslund HB, Wirfält E, Larsosn I, Ericson U, Warensjö E,
et al. Comparison of a web-based food record tool and a food frequency questionnaire and objective validation using the doubly labeled water technique in a Swedish middle-aged population. J Nutr Sci. 2016; 5: e39.
4. Bailey RL. Overview of Dietary Assessment Methods for Measuring Intakes of Foods, Beverages, and Dietary Supplements in Research Studies. Curr Opin Biotechnol. 2021; 70: 91-6.
5. Oliveira OS, Levy J, De Carli E, Bensenor IJM, Lotufo PA, Pereira RA,
et al. Estimation of underreporting of energy intake using different methods in a subsample of the Elsa-Brasil study. Cad Saúde Pública 2022; 38 (7): e00249821.
6. Moran LJ, McNaughton SA, Sui Z, Cramp C, Deussen AR, Grivell RM,
et al. The characterisation of overweight and obese women who are under reporting energy intake during pregnancy BMC Pregnancy Childbirth. 2018; 18: 204.
7. McNitt KM, Hohman EE, Rivera DE, Guo P, Pauley AM, Gernand AD,
et al. Underreporting of Energy Intake Increases over Pregnancy: An Intensive Longitudinal Study of Women with Overweight and Obesity. Nutrients. 2022; 14 (11): 2326.
8. McGowan CA, McAuliffe FM. Maternal nutrient intakes and levels of energy underreporting during early pregnancy. Eur J Clin Nutr. 2012; 66:906-913.
9. Winkvist A, Persson V, Hartini TNS. Underreporting of energy intake is less common among pregnant women in Indonesia. Public Health Nutr. 2002; 5: 523-9.
10. Marshall NE, Abrams B, Barbour LA, Catalano P, Christian P, Friedman JE,
et al. The importance of nutrition in pregnancy and lactation: lifelong consequences. Am J Obstet Gynecol. 2022; 226 (5): 607-32.
11. Kramer MS, Kakuma R. Energy and protein intake in pregnancy. Cochrane Database Syst Rev. 2003; 4: CD000032.
12. Castro-Quezada I, Ruano-Rodríguez C, Ribas-Barba, Serra-Majem L. Misreporting in nutritional surveys: methodological implications. Nutr Hosp. 2015; 31: S119-27.
13. Johansson G, Wikman A, Ahrén AM, Hallmans G, Johansson I. Underreporting of energy intake in repeated 24-hour recalls related to gender, age, weight status, day of interview, educational level, reported food intake, smoking habits and area of living. Public Health Nutr. 2001; 4: 919-27.
14. Colangelo LA, He K, Whooley MA, Daviglus ML, Liu K. Higher dietary intake of long-chain omega-3 polyunsaturated fatty acids is inversely associated with depressive symptoms in women. Nutrition. 2009; 25: 1011-9.
15. Pedersen M, Schoket B, Godschalk RW, Wright J, von Stedingk H, Törnqvist M,
et al. Bulky DNA adducts in cord blood, maternal fruit-and-vegetable consumption, and birth weight in a European mother-child study [New Generis]. Environ Health Perspect. 2013; 121: 1200-6.
16. Lohmann TG, Roche AF, Martorell R. Anthropometric Standardization Reference Manual. Human Kinetics Books, Champaign, Il; 1988.
17. FAO/WHO/UNU. Human energy requirements: report of a Joint FAO/WHO/UNU Expert Consultation. Rome: Food and Agricultural Organization of the United Nations; 2001. [access in 2021 jun 10]. Available from:
https://www.fao.org/3/y5686e/y5686e.pdf18. Black A, Cole TJ. Biased over or under-reporting is characteristic of individual whether over time or by different assessment methods. J Am Diet Assoc. 2001; 101: 70-80.
19. Sichieri R, Everhart JE. Validity of a Brazilian food frequency questionnaire against dietary recalls and estimated energy intake. Nutr Res. 1998; 18: 1649-59.
20. Pinheiro ABV. Tabela para avaliação de consumo alimentar em medidas caseiras. São Paulo: Atheneu; 2004.
21. Sichieri R. Epidemiologia da obesidade. Rio de Janeiro: EdUERJ; 1998.
22. NEPA. TACO. Tabela Brasileira de Composição de alimentos. 4
th ed. Campinas, SP: NEPA-UNICAMP; 2011.
23. IOM. Weight Gain During Pregnancy: Reexamining the Guidelines Rasmussen KM, Yaktine AL, editors. Washington (DC): National Academies Press. [access in 2021 jun 10]. Available from:
http://www.ncbi.nlm.nih.gov/books/NBK32813/24. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology [STROBE] statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008; 61: 344-9.
25. Orcholski L, Luke A, Plange-Rhule J, Bovet P, Forrester TE, Lambert EV,
et al. Under-reporting of dietary energy intake in five populations of the African diaspora. Br J Nutr. 2015; 113: 464-72.
26. Bothwell EKG, Ayala GX, Conway TL, Rock CL, Gallo LC, Elder JP. Underreporting of Food Intake among Mexican/Mexican-American Women: Rates and Correlates. J Am Diet Assoc. 2009; 109: 624-32.
27. Ravelli MN, Schoeller DA. Traditional self-reported dietary instruments are prone to inaccuracies and new approaches are needed. Front Nutr. 2020; 7: 90.
28. Scagliusi FB, Polacow VO, Artioli GG. Selective underreporting of energy intake in women: Magnitude, determinants, and effect of training. J Am Diet Assoc. 2003; 103: 1306-13.
29. Goldberg GR, Black AE, Jebb SA, Cole TJ, Murgatroyd PR, Coward WA,
et al. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur J Clin Nutr. 1991; 45: 569-81.
30. Livingstone MBE, Black AE. Markers of the validity of reported energy intake. J Nutr. 2003; 133: S895-920.
Received on August 13, 2021
Final version presented on November 22, 2022
Approved on Februar 7, 2023
Associated Editor: Sheila Morais
Authors' contribution: Castro MBT: conceptualized the study and collected the data, performed the statistical analysis and the interpretation of the data, draft and review the manuscript. Franco-Sena AB: performed the interpretation of the data, draft and review the manuscript. Freitas-Vilela AA, Pinto TJP, Rocha CMM, Benaim C and Eshriqui I: draft and review the manuscript and approved the final version. Kac G: review the manuscript. All authors have approved the final version of the article and declare no conflict of the interest.


 ; Camila Benaim2
; Camila Benaim2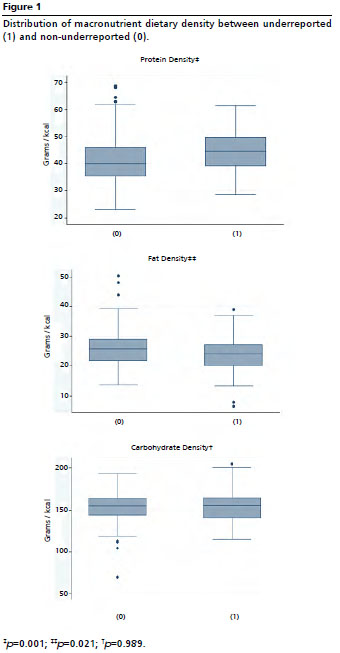






 Ler em português
Ler em português