ABSTRACT
OBJECTIVES: to evaluate the repercussions of motherhood on patients deprived of their liberty.
METHODS: integrative review based on research in electronic databases: Medline (PubMed), LILACS, SciELO and Nursing Database (BDENF), using the following search strategy: ("Prisons" [Majr] AND "Pregnancy" [ Mesh]), as of 2016.
RESULTS: the research ended with 33 bibliographic references, being the highest level of evidence from cohort studies, which demonstrate the precariousness of health care offered to these pregnant women. Three main groups of results were identified: low quality prenatal care, negative maternal and neonatal health indicators in relation to the general population and the emotional issues involved in prison reality during the period of pregnancy and puerperium.
CONCLUSIONS: prenatal care has flaws that influence, in some way, the maternal and neonatal health indicators. In addition, the precarious structure of prison system directly interferes with the emotional health of these women.
Keywords:
Women's health, Prisons, Public health, Pregnancy, Stress psychological
RESUMO
OBJETIVOS: avaliar as repercussões da maternidade em pacientes privadas da liberdade.
MÉTODOS: revisão integrativa a partir de pesquisa nas bases de dados eletrônicas: Medline (PubMed), LILACS, SciELO e Base de Dados de Enfermagem (BDENF), sendo usada como estratégia de busca: ("Prisons"[Majr] AND "Pregnancy"[Mesh]), a partir de 2016.
RESULTADOS: a pesquisa finalizou com 33 referências bibliográficas, sendo o maior nível de evidência de estudos de coorte, que demonstram a precarização na assistência de saúde ofertada a essas gestantes. Foram identificados três grupos principais de RESULTADOS: pré-natal de baixa qualidade, indicadores de saúde maternos e neonatais negativos e as questões emocionais envolvidas na realidade carcerária durante o período de gestação e puerpério.
CONCLUSÕES: a assistência pré-natal apresenta falhas que influenciam nos indicadores de saúde maternos e neonatais. Além disso, a estrutura precária do sistema prisional interfere diretamente na saúde emocional dessas mulheres
Palavras-chave:
Saúde da mulher, Prisões, Saúde pública, Gravidez, Estresse psicológico
IntroductionBrazil has the fourth largest prison population worldwide, with 3.72 thousand incarcerated women, which corresponds to 4.9% of the entire country's prison population, according to the last survey from the statistical information system of Brazilian Prison System (Infopen - Portuguese acronym), published in December 2019. Of these, 38.3% are prisoners in closed conditions and 50.94% are sentenced for drug trafficking.
1 These women mostly portray delimited profile, being young (aged 18 to 29 years old), 63.6% black or brown, 58.4% single and 44.4% with incomplete elementary education.
2,3 According to information from National Prison Department, in April 2020 there was a total of 208 pregnant women and 44 puerperal women in all 27 federative units. In relation to temporary prisoners, 77 pregnant women and 20 puerperal women.
4Pregnancy is an important period in women's life, characterized by physical, psychological and social changes.
5 For those that experience this moment in a situation of privation of liberty, some feelings linked to pregnancy become even more intense.
6Every women should be assisted and receive adequate prenatal care from the healthcare team since they are aware of being pregnant, with requisition of necessary laboratory exams, immunizations, guidance and the perform of at least six prenatal consultations and two puerperal consultations, with the distribution of these prenatal consultations occurring, preferably, one at the first trimester of pregnancy, two at the second and three at the third.
7,8 The puerperal consultations should, ideally, occur in the first week after delivery and between the 30
th and 42
nd week after delivery.
8 Despite the pregnancies of incarcerated women are considered high risk due the vulnerability of the reality in which they live,
5 with overpopulated prisons, unhealthy structural conditions and inadequate food, prenatal care for this population falls short,
9 which ends up favoring negative outcomes in the main health maternal and neonatal indicators.
10The Ministries of Health and Justice defined guidelines related to prevention and healthcare for people deprived of liberty, offered by Unified Health System (SUS - Portuguese acronym) through the National Health Plan in Prison System (PNSSP - Portuguese acronym), replaced by the National Policy of Integrative Healthcare to People Deprived of Liberty in Prison System of 2014.
11 However the PNSSP is considered an improvement to healthcare, the approach concerning issues related to pregnant women healthcare is still precarious.
12It is perceived, thus, that being a woman deprived of liberty is a complex condition that intensifies the situation of vulnerability of this female portion of society, mainly in regard of puerperal and pregnant women, since they are women easily affected by the inadequacy of structure of prison facilities and the difficulty of access to quality healthcare service.
Given the above, this integrative review mainly aims to build information on repercussions of maternity in patients deprived of liberty, analyzing prenatal care, describing the main maternal and neonatal health indicators and assessing emotional repercussions of imprisonment in pregnancy and puerperal period.
MethodsIn order to produce this review, we conducted a broad survey in literature using the databases: Medline (PubMed), LILACS, SciELO and Nursing Database (BDENF - Portuguese acronym), being used the following search strategy: ("Prisons"[Majr] AND "Pregnancy"[Mesh]). The research was concluded in April 2021 and included articles published from 2016. Articles that aimed the process of being pregnant inside a prison unit were selected, concerning prenatal, birth and puerperium, besides articles that described emotional feminine issues involved in this reality. Were used as exclusion criteria non-original articles (point of view or debate articles) and those that were not in the selected languages (Portuguese, English, Spanish and French).
In the reading process of each complete article identified for inclusion in the review, as a part of data extraction process, quality assessment tools were applied for each selected study. Since the issues related to repercussions of motherhood in women deprived of liberty do not involve comparison of treatments, the higher level of evidence was constituted by prospective cohort studies, followed by retrospective cohort studies, case series and cross-sectional studies.
13The parameters for assessing studies were the study design, the sampling size and the verification of the predictive effect of variables by means of multivariate analysis.
ResultsIn Pubmed, 18 articles were found, and in the other databases more 82 articles, totaling 100 articles. After removal of 22 duplicates and reading of titles and abstracts, 40 articles with full text that were read and analyzed remained, excluding more 26 articles according to the informed criteria. The survey concluded with 14 original articles selected from database search.
The synthesis of original articles was described in Table 1, being observed the repercussions of pregnancy in women deprived from liberty, mainly in relation to the female psychic field, besides analyzing maternal and neonatal health indicators affected by imprisonment.
Among the included articles, two were retrospective cohort studies, nine were qualitative studies, two were cross-sectional and one was a case series.
The results of the selected studies converge to the demonstration of precariousness of healthcare provided to pregnant women deprived from liberty. Three main result groups were identified: low quality prenatal care, negative maternal and neonatal health indicators compared to general population and emotional issues involved in prison reality during pregnancy and puerperium.
Variables observed in the various studies were: maternal and neonatal outcomes, type of delivery, birth weight, preterm birth, Apgar, neonatal abstinence syndrome, practices of care to the newborn, separation of mother and child, perceptions of healthcare and environment.
Studies with low sample power (<80%) or without indication of power were considered as having low evidence level. In this way, the study of Ramirez
et al.
15 was the one of higher evidence level for being a retrospective cohort with good statistical power and with analysis of predictor effect of variables. The studies of Sufrin
et al. 20,21 also presented good sample power, although the cross-sectional design and the absence of multivariate analysis diminish their evidence level.
The quality of prenatal care in prison systemIn relation to prenatal care quality, Santana
et al. 25 developed a qualitative study at the Female Prison Facility of the Mata Escura Penitentiary Complex, in the city of Salvador, with participation of 10 pregnant women in situation of deprivation of liberty. It was observed, by means of interviews, that all women shared the opinion that the quality of prenatal care offered were unsatisfactory, with reports of highly technical consultations, focused solely on clinical-obstetric issues, which also weakened the care provided during pregnancy. Matos
et al.
22 and Leal
et al.
27 also added that, besides the insufficient number of consultations and the exams and procedures executed had weaknesses, for the lack of structure in prison units or denial of the system itself in supplying the particular gestational needs.
Maternal and neonatal health indicators in prison realityIn regard to the main maternal and neonatal health indicators, there are type of delivery, birth weight, prematurity, abortion, admission in neonatal ICU and Apgar index. Ramirez
et al.
15 and Sufrin
et al. 20,21 demonstrated that these indexes, when analyzed in female prisoners, are negative compared to the general population, being possible that this fact is partially related to low quality prenatal care, inadequate food and shelter. Besides, we observed a lower number of cesarean-section surgeries in this group of pregnant women deprived of liberty.
Emotional issues of motherhood in prison systemThere is a large emotional appeal in studies that survey feelings of pregnant and puerperal women in deprivation from liberty, mainly for the more concerning situation of these women that need to live maternity in a hostile reality. Several reports bring the speech of fear and feeling of powerlessness, of the search of isolation as an attempt of protection, of the denial of pregnancy due to fear of having a child in prison environment and the absence of a pregnant prisoner status, which, theoretically, would assure not only rights of both mother and children, but also higher safety during the pregnancy process, as well described by Abbott
et al.
18 and Fochi
et al.
23 Besides, the complaint about lack of support network, with distancing from family, is also frequent during interviews.
23DiscussionThe results found allow analyzing important aspects of maternal life in prison reality, mainly in regard to prenatal care, health indicators and emotional health.
The offer of quality prenatal care, with well-trained and qualified health professionals, has as its main objective the prevention of complications during pregnancy and delivery, which is in line with the National Health Plan of the Prison System. The detainee pregnant women should be referred to a prison unit that has a professional team and structure that allows the adequate follow-up of pregnancy. The delivery, in turn, should occur at the hospital unit of the prison facility or in the public health network.
28 Silva
et al. 17 highlight that female prisoners have difficulties in access to pregnancy tests, being the positive result prerequisite for being transferred to special cells destined to pregnant and puerperal women and newborns. The delay in the execution of tests and diagnosis ends up impairing adequate prenatal care.
In the analyzed studies, most detainees shared the opinion that prenatal care in prison is unsatisfactory, with few available exams, inadequate administration of drugs for treatment of specificities during pregnancy cycle and low humanized posture of the health team. Besides, several participants in the surveys reported not having contact with nursery during consultations nor received guidance about pregnancy, being prenatal care executed only by physicians.
22,25,27 Ferreira
et al. ,
26 in the other hand, demonstrated that besides the active participation of nursery in prenatal care practice (with laboratory exams, vaccines and timely consultations), the attendance itself was still insufficient in regard of humanity, due to, mainly, the issue of mechanization of procedures by both nurses and physicians, leading women to a feeling of helplessness.
Among the studies that assessed the maternal and neonatal health indicators of women in prison situation, Ramirez
et al.
15 observed that the chances of prematurity, low birth weight, and small for gestational age were two times higher in detainees, regardless if these women were in prison during pregnancy or not, compared to general population. Besides, the percentage of admission and length of stay in neonatal ICU were higher in newborns of detainees.
On the other hand, two studies in which were analyzed penitentiary data from United States between 2016 and 2017 observed that prematurity rate in units assessed was lower than the percentage of the country's population,
20,21 which can be partially explained due to prenatal care, nutrition, shelter and limited access to illicit drugs, conditions that may be different to non-prisoner women,
14.21 however, this hypothesis should be considered with caution, due to the variability of quality in prenatal care in different prisons.
20 Some states, singly, presented higher prematurity rate in relation to the national average, which suggests that the prison context and life conditions before incarceration play an important and defining role in the neonatal and maternal health indicators.
19,20 In contrast, Shlafer
et al.
14 demonstrated rare adverse neonatal and maternal outcomes, observing also that women that received specialized prenatal support, including follow-up of doulas during delivery, obtained outcomes similar to those of the control group of pregnant women that followed standard prenatal care and that the adverse birth outcomes in study sample were lower than national and state averages of women that did not have privation of liberty.
In relation to type of delivery within prison reality, studies were unanimous in demonstrating that vaginal delivery presented higher rates of occurrence.
14,19,20,29 Besides, Ramirez
et al. 15 demonstrated that there is no significant difference in cesarean delivery rates in prison groups compared to the general population.
Another important factor verified in studies is the emotional issue of pregnant women in deprivation of liberty. Silva
et al.
17 observed the feeling of abandonment reported by women, mainly at the birth moment, once, in most cases, the family is not contacted, preventing them from being present at the moment and so offering adequate support to both women and newborns. The institutional abandonment by obstetric professionals is also cited as a negative factor in the emotional field of these pregnant women. Many detainees affirm that the familiarity within pregnant and puerperal women is fundamental for them to feel supported and safer, demonstrating, with it, the importance of special cells for these women in the prison system.
16,17 Reports about hierarchy between detainees, in which those with higher income pay other detainees to care for their children in cells, outsourcing the process of care, evidence the reproduction of market relationships present outside prisons.
16The growing feeling of fear and insecurity is reported with a certain constancy by detainees, mainly after delivery, when the concern comes to be not only with themselves, but also with the wellbeing and safety of their children. Rebellions, conflicts with security agents and distrust about other detainees are among the main yearnings, unleashing a constant defense-surveillance response. Reports concerning the desire of receiving the special status of pregnant detainee is common, for protection of their lives, since in most cases cells are populated by pregnant and non-pregnant women.
17,23 Overcrowding of cells impairs sleep, resting and privacy, leading to irritability, discomfort and feelings of sadness and isolation.
23 Besides, incarceration results in the building of mother and baby link stressed by the anxiety of separation, due to the knowledge of the need of mandatory separation after some months, or the threat of separation at any time due to disciplinary problems. The established role of what a good mother is also lead these women to the feeling of guilty and powerlessness, for not being able to execute, in prison, the role that they believe to be adequate to children, and also, for understanding that their mistakes end up affecting the child, that stays the first months of life within prison reality.
19,23,24Pregnant women deprived of liberty, in general, are transferred from prison units near their residences to capitals, leading to increasing costs and impairment to relatives in their visitations, hindering the existence of an adequate support network. Given the above, women end up being dependent on penitentiary management, where the professionals of units perform this role themselves, however in a fragile and inadequate way, which triggers feelings of uncertainty and insecurity, besides physical and emotional exhaustion. Therefore, although the support network is fundamental to both puerperal women and newborns, the prison reality results in limitation of interactions.
16,24Brazilian jurisdiction has a legal precept that, in prison units, should exist the inclusion of nursery and possibility of crèche/section for pregnant and parturient women, as preconized by Lawnumber 11.942/09.
30,31 Therefore, women in deprivation of liberty that give birth inside prison system should be referred to Mother and Child Unit, remaining in this sector until a minimum period of six months of baby's life, ensuring exclusive breastfeeding until the ideal preconized period. After this period, the mother is separated from her child and returns to her original sector.
30,32 There is no consensual time interval between female prison units in regard of permanence of the detainee mother with her child, but the maximum period is of 1 year and 6 months, according to resolution number 4, July 15, 2009, of the National Council of Criminal and Prison Policy (CNPCP - Portuguese acronym).
33 Breastfeeding, a right assured by Brazilian legislation, is not always assured in prison system, since units with adequate nursery are rare. In exclusively female prisons, 34% have cells or dormitories for pregnant women, 32% have nurseries and 5%, crèches. In mixed prisons, these rates fall to 6%, 3% and 0%, respectively.
2It is understood that the availability of nursery and crèche in prison system are necessary structural resources to assure basic rights necessary not only to children, but also to mothers, however they have been used as a reason for denying home detentions, under justification that the prison environment would provide better life conditions to these women that, mostly, live in precarious conditions outside prison.
34 On the other hand, the care to the child occurs in an integral manner, generating a kind of hyper-motherhood experienced by these incarcerated women, which results in isolation and feeling of loneliness, besides physical and psychological exhaustion.
35The main limitation of the study was the option of using studies that are methodologically heterogeneous, which could compromise the validity of results. However, since data did not show opposite outcomes, this was not significant. Besides, the exclusion of articles could lead to publication bias. Accordingly, more prospective studies should be executed in order to validate findings.
The complexity of management of pregnancy, delivery and puerperium within the prison system and the flaws in prenatal care influence, in a certain way, maternal and neonatal health indicators. Besides, prison structures, mostly conceived aiming a male population, with overcrowding and mostly unhealthy environments, do not meet the needs of pregnant and puerperal women. All of these factors directly influence the emotional health of women that experience this reality, in which fear, insecurity and sadness prevails. It is necessary to think about women rights in this reality in a more humanized manner, in order to assure adequate maternal care with whole rights of access to quality public health.
References1. Ministério da Justiça e Segurança Pública (BR). Departamento Penitenciário Nacional. Levantamento Nacional de Informações Penitenciárias (Infopen). Brasília (DF): Ministério da Justiça e Segurança Pública; 2019. [access in 2021 mar 15]. Available from:
https://dados.mj.gov.br/dataset/infopen-levantamento-nacional-de-informacoes-penitenciarias/resource/225de757-416a-46ab-addf-2d6beff4479b2. Ministério da Saúde (BR). Secretaria de Atenção em Saúde, Departamento de Ações Programáticas Estratégicas. Legislação em saúde no sistema penitenciário. Brasília (DF): Ministério da Saúde; 2010. [access in 2021 mar 15]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/legislacao_saude_sistema_penitenciario.pdf3. Ministério da Justiça e Segurança Pública (BR). Departamento Penitenciário Nacional. Relatório temático sobre mulheres privadas de liberdade. Brasília DF): Ministério da Justiça e Segurança Pública; 2017. [access in 2021 mar 15]. Available from:
https://carceraria.org.br/mulher-encarcerada/depen-divulga-infopen-mulheres-de-junho-de-20174. Conselho Nacional de Justiça (CNJ). Mulheres presas e adolescentes em regime de internação que estejam grávidas e/ ou que sejam mães de crianças até 6 anos de idade: sumário executivo. Brasília (DF): Conselho Nacional de Justiça; 2022. [access in 2021 mar 15]. Available from:
https://www.cnj.jus.br/wp-content/uploads/2022/04/eixo1-primeira-infancia-sumario-executivo-final.pdf5. Fochi MCS, Silva ARC, Lopes MHBM. Prenatal care in a primary healthcare center for imprisoned pregnant women. Rev RENE. 2014; 15 (2): 371-7.
6. Shah S, Plugge EH, Douglas N. Ethnic differences in the health of women prisoners. Public Health. 2011; 125 (6): 349-56.
7. Ministério da Saúde (BR). Secretaria de Atenção à Saúde, Departamento de Ações Programáticas Estratégicas. Pré-natal e Puerpério: atenção qualificada e humanizada: manual técnico. Brasília (DF): Ministério da Saúde; 2006. [access in 2021 mar 15]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_pre_natal_puerperio_3ed.pdf8. Trajano AJB, Monteiro DLM, Jesús NR. Rotinas hospitalares/Hospital Universitário Pedro Ernesto; vol. 1. 2ª ed. Rio de Janeiro: EdUERJ; 2017.
9. Silva EF, Luz AMH, Cecchetto FH. Maternidade atrás das grades. Enferm Foco. 2011; 2: 33-7.
10. Ministério da Justiça (BR). Secretaria Especial de Política para Mulheres da Presidência da República, Grupo de Trabalho Interministerial. Reorganização e reformulação do sistema prisional feminino: relatório final. Brasília (BR): Ministério da Justiça; 2007. [access in 2021 mar 15]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/relatorio_final_reorganizacao_prisional_feminino.pdf11. Ministério da Saúde (BR). Portaria interministerial Nº 1, de 2 de janeiro de 2014. Institui a Política Nacional de Atenção Integral à Saúde das Pessoas Privadas de Liberdade no Sistema Prisional (PNAISP) no âmbito do Sistema Único de Saúde (SUS). Brasília (DF): DOU; 2014. [access in 2021 mar 15]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2014/pri0001_02_01_2014.html12. Diuana V, Ventura M, Simas L, Larouzé B, Correa M. Direitos reprodutivos das mulheres no sistema penitenciário: tensões e desafios na transformação da realidade. Ciên Saúde Colet. 2016; 21 (7): 2041-50.
13. Burns PB, Rohrich RJ, Chung KC. The levels of evidenceand their role in evidence-based medicine. Plast Reconstr Surg. 2011 Jul; 128 (1): 305-10.
14. Shlafer R, Saunders JB, Boraas CM, Kozhimannil KB, Mazumder N, Freese R. Maternal and neonatal outcomes among incarcerated women who gave birth in custody. Birth. 2021 Mar; 48 (1): 122-31.
15. Ramirez AC, Liauw J, Costescu D, Holder L, Lu H, Kouyoumdjian FG. Infant and Maternal Outcomes for Women Who Experience Imprisonment in Ontario, Canada: A Retrospective Cohort Study. J Obstet Gynaecol Can. 2020 Apr; 42 (4): 462-72.
16. Nunes LRC, Deslandes SF, Jannotti CB. Narrativas sobre as práticas de maternagem na prisão: a encruzilhada da ordem discursiva prisional e da ordem discursiva do cuidado. Cad Saúde Pública. 2020; 36 (12): e00215719.
17. Silva JB, Moraes MN, Brandão BMLS, Freitas WMF, Souto RQ, Dias MD. Mulheres em privação de liberdade: narrativas de des(assistência) obstétrica. REME - Rev Min Enferm. 2020; 24: e-1346.
18. Abbott L, Scott T, Thomas H, Weston K. Pregnancy and childbirth in English prisons: institutional ignominy and the pains of imprisonment. Sociol Health Illn. 2020 Mar; 42 (3): 660-75.
19. Chaves LH, Araújo ICA. Gestação e maternidade em cárcere: cuidados de saúde a partir do olhar das mulheres presas em uma unidade materno-infantil. Physis (Rio J. ). 2020; 30 (1): e300112.
20. Sufrin C, Jones RK, Mosher WD, Beal L. Pregnancy Prevalence and Outcomes in U.S. Jails. Obstet Gynecol. 2020 May; 135 (5): 1177-83.
21. Sufrin C, Beal L, Clarke J, Jones R, Mosher WD. Pregnancy Outcomes in US Prisons, 2016-2017. Am J Public Health. 2019 May; 109 (5): 799-805.
22. Matos KKC, Silva SPC, Lima JKS. Representações de mulheres encarceradas sobre gestar na prisão. Rev. enferm. UFPE. 2018; 12(11): 3069-77.
23. Fochi MCS, Higa R, Camisão AR, Turato ER, Lopes MHBM. Vivências de gestantes sem situação de prisão. Rev Eletr Enf. 2017; 19: a57.
24. Diuana V, Corrêa MCDV, Ventura M. Mulheres nas prisões brasileiras: tensões entre a ordem disciplinar punitiva e as prescrições da maternidade. Physis (Rio J. ). 2017; 27 (3): 727-47.
25. Santana AT, Oliveira GRSA, Bispo, TCF. Mães do cárcere: vivências de gestantes frente à assistência no pré-natal. Rev Baiana Saúde Pública. 2017; 40 (1): 38-54.
26. Ferreira LS, Moreira WC, Nascimento MVF, Sousa GN, Sertão MAL, Lago EC, et al. Percepção de presidiárias sobre a assistência à saúde materna em uma penitenciária feminina. Rev Cuba Enferm. 2017; 33 (4): 776-92.
27. Leal MC, Ayres BVS, Esteves-Pereira AP, Sánchez AR, Larouzé B. Nascer na prisão: gestação e parto atrás das grades no Brasil. Ciênc Saúde Colet. 2016; 21 (7): 2061-70.
28. Ministério da Saúde (BR). Plano Nacional de Saúde no Sistema Penitenciário. Portaria Interministerial Nº 1.777, de 9 de novembro de 2003. Aprova o Plano Nacional de Saúde no Sistema Penitenciário, constante do ANEXO I da Portaria, destinado a prover a atenção integral à saúde da população prisional confinada em unidades masculinas e femininas, bem como nas psiquiátricas. Brasília (DF): Ministério da Saúde; 2004. [access in 2021 mar 15]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2003/pri1777_09_09_2003.html29. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010 Sep; 25 (9): 603-5.
30. Brasil. Lei nº 11.942, de 28 de maio de 2009. Dá nova redação aos arts. 14, 83 e 89 da Lei n. 7.210, de 11 de julho de 1984 - Lei de Execução Penal, para assegurar às mães presas e aos recém-nascidos condições mínimas de assistência. Brasília (DF): DOU de 29 de maio de 2009. Seção 1, p.1. [access in 2021 mar 15]. Available from:
http://www.planalto.gov.br/ccivil_03/_ato2007-2010/2009/lei/l11942.htm31. Ministério da Justiça (BR). Diretoria de Políticas Penitenciárias. Departamento Penitenciário Nacional. Mulheres Presas - Dados Gerais. Projeto Mulheres/ DEPEN. Brasília (DF): Ministério da Justiça; 2011. [access in 2021 mar 15]. Available from:
http://fileserver.idpc.net/library/Mulheres-presas-dados-gerais.pdf32. Amaral MF, Bispo TCF. Mães e filhos atrás das grades: um olhar sobre o drama do cuidar de filhos na prisão. Rev Enferm Contemporânea. 2016; 5 (1): 51-8.
33. Ministério da Justiça (BR). Conselho Nacional de Política Criminal e Penitenciária. Resolução nº 4, de 15 de julho de 2009. Dispõe sobre o direito à amamentação para mulheres encarceradas. Brasília (DF): DOU de 3 de novembro de 2009. [access in 2021 mar 15]. Available from:
https://www.gov.br/depen/pt-br/composicao/cnpcp/resolucoes/2009/resolucao-no-4-de-15-de-julho-de-2009-1.pdf/view34. Braga AGM. Entre a soberania da lei e o chão da prisão: a maternidade encarcerada. Rev Direito GV. 2015; 11: 523-46.
35. Braga AGM, Angotti B. Da hipermaternidade à hipomaternidade no cárcere feminino brasileiro. SUR Rev Int Direitos Humanos. 2015; 12 (22): 229-39.
Received on July 2, 2021
Final version presented on August 4, 2022
Approved on August 15, 2022
Associated Editor: Leila Katz
Authors' contribution: Moraes LF: conceptualization, survey, methodology, elaboration of draft and edition of article. Sorares LC: methodology, supervision, elaboration of draft and edition of article. Raupp RM: supervision, elaboration and edition of article. Monteiro DLM: conceptualization, formal analysis, methodology, supervision, elaboration of draft and edition of article.
All authors approved the final version of the article and declare no conflict of interest.


 ; Leila Cristina Soares2
; Leila Cristina Soares2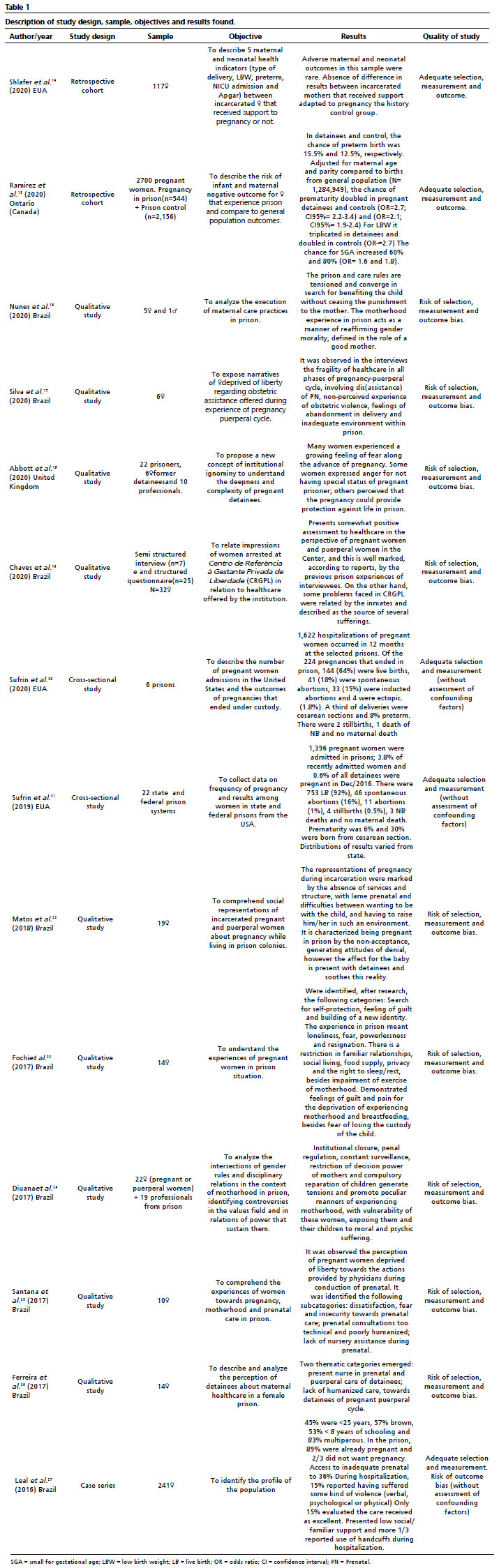






 Ler em português
Ler em português