ABSTRACT
OBJECTIVES: to estimate neonatal near miss rates and investigate sociodemographic, obstetric, childbirth, and neonate factors residing in a Midwest capital city.
METHODS: observational cohort study of live births from Cuiabá in the period of 2015 to 2018, with data from the Sistemas de Informações sobre Mortalidade e sobre Nascidos Vivos (Mortality and Live Birth Information Systems). The neonatal near miss rate was calculated according to sociodemographic, obstetric, childbirth, and neonate variables. Logistic regression model was adjusted to analyze the factors associated with neonatal near miss.
RESULTS: the neonatal near miss rate was 22.8 per thousand live births and the variables showed an association with the outcome were: maternal age 35 years or older (OR=1.53; CI95%=1.17-2.00), having fewer than six prenatal consultations (OR=2.43; CI95%=2.08-2.86), non-cephalic fetal presentation (OR=3.09; CI95%=2.44-3.92), multiple pregnancy (OR=3.30; CI95%=2.57- 4.23), no live birth (OR=1.62; CI95%=1.34-1.96) or one live birth (OR=1.22; CI95%=1.00-1.48), delivery in public/university hospital (OR=2.16; CI95%=1.73-2.71) and philanthropic hospital (OR=1.51; CI95%=1.19-1.91) and non-induced labor (OR=1.50; CI95%=1.25-1.80).
CONCLUSION: the neonatal near miss rate was 3.04 cases for each death, and neonatal near miss was influenced by maternal characteristics, obstetric history, type of birth hospital, and delivery care organization.
Keywords:
Vital statistics, Near miss, Information system, Morbidity, Newborn
RESUMO
OBJETIVOS: estimar as taxas de near miss neonatal e investigar os fatores sociodemográficos, obstétricos, do parto e dos neonatos residentes em uma capital do Centro-Oeste.
MÉTODOS: estudo observacional de coorte de nascidos vivos de Cuiabá no período de 2015 a 2018, com dados dos Sistemas de Informações sobre Mortalidade e sobre Nascidos Vivos. Foi calculada a taxa de near miss neonatal conforme as variáveis sociodemográficas, obstétricas, do parto e dos neonatos. Modelo de regressão logística foi ajustado para analisar os fatores associados ao near miss neonatal.
RESULTADOS: a taxa de near miss neonatal foi 22,8 por mil nascidos vivos e as variáveis que apresentaram associação com o desfecho foram: idade materna de 35 anos ou mais (OR=1,53; IC95%=1,17-2,00), realizar menos de seis consultas de pré-natal (OR=2,43; IC95%=2,08-2,86), apresentação fetal não cefálica (OR=3,09; IC95%=2,44-3,92), gravidez múltipla (OR=3,30; IC95%=2,57-4,23), nenhum filho nascido vivo (OR=1,62; IC=1,34-1,96) ouum filho nascido vivo (OR=1,22; IC95%=1,00-1,48), parto em hospital público/universitário (OR=2,16; IC95%=1,73-2,71) e filantrópico (OR=1,51; IC95%=1,19-1,91)e trabalho de parto não induzido (OR=1,50; IC95%=1,25-1,80).
CONCLUSÃO: a taxa de near miss neonatal foi de 3,04 casos para cada óbito, sendo que o near miss neonatal foi influenciado pelas características maternas, histórico obstétrico, tipo do hospital do nascimento e organização da assistência ao parto.
Palavras-chave:
Estatísticas vitais, Near miss, Sistema de informação, Morbidade, Recém-nascido
IntroductionIn 2017, neonatal deaths accounted for 2.5 million worldwide and 18 deaths/1,000 live births. It is estimated that 56 million children under the age of five will die between 2018 and 2023, with half of these deaths occurring in the neonatal period.
1 Brazil also follows this global trend. Between 2010 and 2017, the Infant Mortality Rate (IMR) reduced to 3.9%, reaching 13.4 deaths/1,000 live births in 2017, with the early neonatal component contributing to most of this total, with 7.2 deaths/1,000 live births.
2The reduction of neonatal mortality is closely related to the quality of care provided during pregnancy, childbirth and birth. From this perspective, the neonatal near miss (NNM) event can be used in the evaluation of maternal and child healthcare, since it broadens the basis of mortality analysis by using morbidity data and its conformation in the care context, investigating the factors interconnected with the threat to life at birth.
3Therefore, the concept of NNM considers the newborn that presented a severe life-threatening morbidity
4 but survived the first 28 days of life.
3-6 For some researchers, knowing the characteristics of NNM is the first step to reduce neonatal mortality and long-term sequelae.
3-5 However, data on this event are scarce because the construction of this concept is recent, a little more than a decade, and a research on the subject is being developed in embryonic form and we still have few literature reviews on the topic.
7-8Although Brazil leads in studies on this topic in Latin America, it is necessary to deepen and broaden the debate on its use in care practice, so that its application in the context of health services is feasible.
9 Therefore, this study aimed to estimate neonatal near miss rates and investigate socio-demographic, obstetric, delivery and neonate factors in a Midwest capital.
MethodsThis is a cohort of live births from 2015 to 2018. The study population consisted of 40,741 live newborns and children of mothers residing in Cuiabá-MT-Brazil. Data were collected from the
Sistema de Informações sobre Nascidos Vivos (SINASC) (Live Births Information System) and
Sistema de Informações sobre Mortalidade (SIM) (Mortality Information System), provided by the
Secretaria Municipal de Saúde (SMS) (City Health Secretary) in Cuiabá-MT-Brazil, with authorization to be used in this study. The choice for using secondary data from the information systems was due to accessibility, comprehensiveness, and multiplicity of data regarding vital events and morbidity.
Cases of NNM were defined based on criteria adapted from Silva
et al., (2014; 2017):
10,11 birth weight <1.500g, gestational age (GA) less than 32 weeks, Apgar<7 at the fifth minute, and presence of congenital malformation. These criteria have been validated
10,11 and have 97% sensitivity, 92.6% specificity
9,10 and 97% accuracy,
10,12 as well as presenting the most appropriate cohort points based on the perinatal literature.
12From the definitions of NNM pragmatic criteria in the literature, this study tested the validity of the following criteria in the neonatal period (0 to 27 days): birth weight <1. 500g, presence of congenital anomaly, gestational age (GA) less than 32 weeks, and Apgar <7 at the fifth minute, identifying specificity of 97.70% [CI95%=97.55-97.84], sensitivity of 80.07% [CI95%=75.20-84.17], and an accuracy of 97.57% [CI95%=97.41-97.71], presenting a high sensitivity and specificity, as in previous studies. This validation process used neonatal deaths as the gold standard.
12All live newborns from hospital births whose mothers resided in the city of Cuiabá and who survived until the 27th day of life after birth were included in the study. Those who had missing data in the information systems and those who were duplicates were excluded from the sample. To identify the deaths, a linkage
13 was performed between the SIM and SINASC, using the number of the
Declaração de Nascido Vivo (DNV) (Birth Statement) as a common field in both systems. SIM information was used to calculate mortality rates.
The variables in this study were obtained from SINASC: 1)
Maternal socioeconomic and demographic age range (ten to 19 years; 20 to 34 years and 35 years or older), marital status (married and stable union were recoded as "with partner" and being single, widowed and legally separated/divorced to "without partner"), schooling (zero to eight years of study; nine to 11 years of study and 12 years or more), race/skin color (white, mixed, black, and yellow were grouped with indigenous), maternal occupation (the categories students, housewives, unemployed, retired, and pensioners were classified as "does not work" and the other occupations received the denomination "works"); 2)
obstetric: parity (nulliparous, primiparous, secundipara, multipara), type of current pregnancy (single, double or more), obstetric history (number of previous normal and cesarean childbirths and number of live and dead children); 3)
prenatal care: trimester of prenatal initiation (first; second; third) and number of consultations attended (less than six or six or more); 4)
regarding to childbirth: type of facility (philanthropic, private, private contracted to the
Sistema Único de Saúde (SUS) (Public Health System) and, the university that was linked with the "public", as being contracted to SUS), type of childbirths (cesarean or vaginal), professional who attended the delivery (medical and non-medical), fetal presentation (cephalic and non-cephalic in which the podalic, pelvic and transversal positions were included), induced labor (yes or no) and; 5)
regarding newborns: sex.
The following indicators were calculated: 1) neonatal near miss rate (NNMR), defined as the number of neonatal near miss cases divided by total live births multiplied by one thousand; 2) severe neonatal outcome rate (SNOR), defined by the number of neonatal near miss cases plus neonatal deaths divided by total live births multiplied by one thousand; 3) infant mortality rate (IMR): number of deaths in children under one year of age divided by total live births multiplied by thousand; 4) Neonatal mortality rate (NMR): number of neonatal deaths divided by total live births multiplied by thousand; 5) Early neonatal mortality rate (ENMR): number of early neonatal deaths (zero to sixth day) divided by total live births multiplied by thousand; 6) Late neonatal mortality rate (LNMR): number of late neonatal deaths (seventh to 27th day) divided by total live births multiplied by thousand.
Descriptive analysis was performed using absolute and relative frequencies by STATA
@ version 12 software. In bivariate analysis, Pearson's chi-square test was used to assess the association between NNMR and maternal, obstetric, childbirth and newborn sociodemographic variables. Variables with
p<0.20 in the bivariate analysis were included in the initial multivariate logistic regression model, the backward selection method was considered. Variables with
p<0.05 remained in the final model. For these, the odds ratio (OR) and 95% confidence interval (CI95%) were estimated.The adequacy of the multiple model was verified by the Hosmer-Lemeshow test (
p=11.82).The research project was evaluated and approved by the Research Ethics Committee, with opinion no. 3.734.141, CAAE 25558619.0.0000.5541 on November 28, 2019.
ResultsIn the period from 2015 to 2018, 40.741 live births were born in Cuiabá, of this total, 427 came to death during the first year of life and 306 in the neonatal period (zero to the 27th day of life), representing 71.7% of total infant deaths. Of the neonatal deaths, 66% occurred in the early neonatal period (zero to six days), of which 47.02% occurred in the first 24 hours of life; and 34% in the late neonatal period (zero to 27 days) (Table 1).
It was identified in the analyzed period that 931 (2.28%) live births presented at least one pragmatic criterion; and of these, 42.96% were born with gestational age less than 32 weeks; 40.71% had birth weight less than 1.500g; 27.93% presented Apgar index<7 in the fifth minute and; 20.08% manifested at least one congenital malformation at birth. The NNMR was 22.8/1,000 live births and the NMR was 7.5/1,000 live births, with 3.04 cases of neonatal near miss for each neonatal death (Table 1).
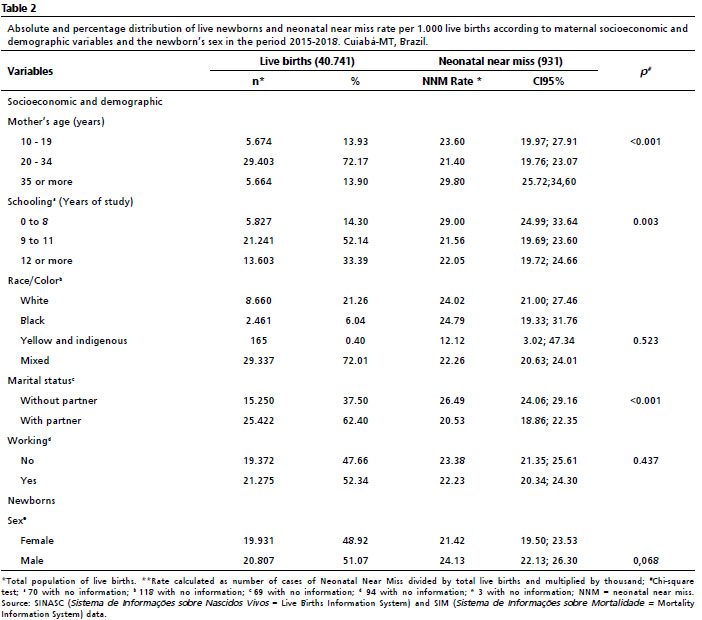
Of all live births, most mothers were between 20 and 34 years old (72.17%) and were mixed skin color (72.01%). More than half had schooling between nine and 11 years (52.14%), were working (52.34%), had a male child (51.07%), and had a partner (62.40%). The proportion of teenage mothers and those aged 35 years or older was low (6.22% and 13.90%, respectively). The NNMR was higher among mothers aged 35 years or older, with up to eight years of schooling, and without a partner. (Table 2).
Of the live birth cohort, most mothers started prenatal care in the first trimester of gestation (80.34%), had six or more visits (83.92%), had no dead children (81.22%), had labor with cephalic presentation (96.74%), not induced (75.55%), by single gestation (97.57%), attended by a physician (99.10%), in a private hospital linked to SUS (53.36%), and by cesarean delivery (55.71%) (Table 3).
The NNM rate was higher among mothers who had fewer than six prenatal visits, who had no previous cesarean delivery, who had no living children, who had two or more dead children, who experienced their childbirths in a public/university hospital, who had non-cephalic fetal presentation, with a double pregnancy or more, and with non-induced labor (Table 3).
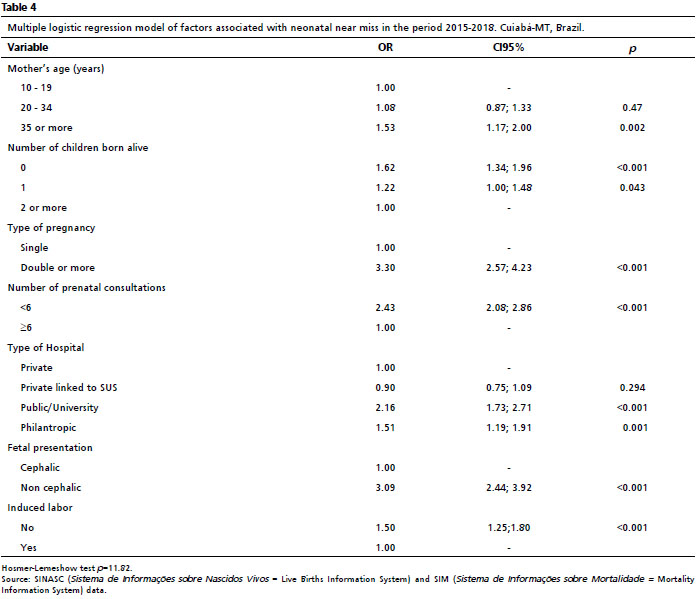
In multiple analysis, the factors that maintained statistically significant association were a mother, 35 years of age or older (OR=1.53; CI95%=1.17-2.00), having an obstetric history none (OR=1.22; CI95%=1.00-1.48) or one live-born child (OR=1.62; CI95%=1.34-1.96), multiple pregnancy (OR=3.30; CI95%=2.57-4.23), less than six prenatal visits (OR=2.43; CI95%=2.08-2.86), delivery in public/university hospital (OR=2.16; CI95%=1.73-2.71) and philanthropic (OR=1.51; CI95%=1.19-1.91), non-cephalic presentation (OR=3.09; CI95%=2.44-3.92) and who did not have labor induced (OR=1.50; CI95%=1.25-1.80) (Table 4).
DiscussionIn the period studied, in Cuiabá-MT-Brazil a NMR of 7.5/1.000 NB and a NNMR of 22.8/1,000 NB, resulting in 3.04 cases of NNM for each neonatal death, resulting in data similar to those of a study developed in a Fortaleza-CE maternity hospital, which identified 2.2 cases of NNM for each death.
14 A study carried out in the cities of São Paulo (SP), Rio de Janeiro (RJ) and Niterói (RJ), using almost the same pragmatic criteria of this research, excluding congenital anomaly and mechanical ventilation, found an NNMR of 17.2/1.000 NB.
4On the other hand, a research developed in 191 Brazilian cities
10 and another carried out in Joinville-SC,
11 which used the same criteria of NNM in this study, with the addition of mechanical ventilation, obtained respectively the NNMR of 39.2/1.000 live births and a NMR of 11.1/1.000 live births, resulting in 3.5 cases of NNM for each death
10 and NNMR of 33/1.000 live births and a NMR of 4.5/1.000 live births, so for each 7.3 cases of NNM there was one death.
11 It is likely that such variations in the results are justified by the inclusion or not of mechanical ventilation and congenital malformation to classify cases of NNM. The previous could not be included in this study because this information was not available in the SIM and SINASC.
It is necessary to consider the use of the pragmatic criteria in isolation, since it does not contemplate to other associated problems. It is known that when the mechanical ventilation criterion is added, the probability of neonatal near miss morbidity is greater, since just being born with a low weight does not mean that you will present respiratory distress requiring mechanical ventilation.
10Although the NNM studies developed in the country have used different criteria indicative of newborn severity and different periods of neonatal survival, they have good accuracy and sensitivity to detect cases of neonatal near miss,
15 such as the present study.
As for the selection of criteria for the identification of cases of neonatal near miss adopted in this research, the main pragmatic entry criterion was gestational age <32 weeks, which was also identified by studies conducted in Maceió-AL
6 and in the South region of Ghana, Africa.
16 On the other hand, a research developed in Recife-PE,
17 identified low birth weight as the main isolated pragmatic entry criterion. It is noteworthy that both gestational age and low birth weight are factors associated with neonatal death.
18-21The most predictive elements of NNM observed in Ghana, Africa, were gestational age <33 weeks, neurological and respiratory dysfunction, and hemoglobin <10 gd/dl.
16 Whereas in Gujarat, India, the pragmatic criterion that most identified NNM cases was Apgar<7 at the fifth minute, followed by birth weight <1.500g and prematurity (GA <30 weeks).
22 These divergences between locations may be explained by differences in care and the inclusion or not of a certain criterion to classify NNM cases.
In this study, birth weight <1.500g was the second criterion that concentrated the highest number of NNM cases. The literature shows that an efficient and qualified action to restrict preterm and low birth weight births will decisively influence the reduction of neonatal mortality rates,
18 which applies not only to the Brazilian reality, but also to of other countries.
The results of this study also showed that the pragmatic criteria Apgar<7 in the fifth minute and congenital malformation at birth concentrated the third and fourth highest frequency of NNM cases, respectively, both proven to be associated with neonatal mortality in our country.
19-21Although the Apgar assessment is considered a specific and subjective method to report the vitality conditions of the newborn immediately after birth and the response to the necessity for resuscitation,
19,23 its use in care is relevant. The Apgar score <7 in the fifth minute of life increases the risk of death
10,21 and has been considered an indicator of neonatal near miss,
3,6,7 with a sensitivity of 82.6% and specificity of 97.9%.
10It is noteworthy that few studies up to now have used congenital malformation as a pragmatic criterion to identify NNM cases. However, it should be considered that newborns with this condition have a significantly higher chance of neonatal mortality,
19,21,24 making it relevant to include this criterion in future studies, although there are no precise boundaries for this inclusion,
6 since not all malformations are fatal and contribute to neonatal death.
7In this sense, we suggest including only those that cannot be prevented, even with quality and effective interventions, such as some severe central nervous system deformities and congenital heart diseases. However, this is still a challenge, since there is no consensus on which are the severe anomalies and those that can be treated early.
Regarding maternal age, NNMR was more prevalent among mothers aged 35 or older. In line with these findings, studies using data from the
Pesquisa Nascer no Brasil 2011-2012
25,26 (Birth in Brazil Survey) showed an association between maternal age above 35 years and NNM, which indicates a high risk of the event in this age group,
25 with 1.32 more chance of NNM when compared to the age group of 20 to 34 years old.
26 In addition, these women are subject to develop complications during the gestational period and consequently have adverse perinatal outcomes.
25,26Even though most of the women studied had more than six prenatal visits, there was a higher rate of NNMR among those with fewer than six visits, in agreement with the findings of other studies,
4,6,27 which reinforce that the insufficient number of prenatal visits during pregnancy can be harmful to the mother and the baby, such as prematurity,
4 and is associated with NNM.
22,26 Theoretically, the higher the number of prenatal visits, the greater the chances of detecting and intervening in changes, especially in high-risk pregnancies, which are associated with poor maternal and perinatal outcomes.
6,27Pelvic or podalic/transverse presentation was also associated with a high rate of NNM, as in a research conducted in Ghana, Africa, which found that poor presentation during childbirth causes complications for both mother and baby and can interfere with the NNM outcome.
27 However, there is a need for further research to understand this outcome, which may be related to the conduct of childbirth, care protocols and preparation of professionals who assist the mother.
28Few researches have investigated the relationship between the type of pregnancy (single, double, triple or more) and the NNM
11,25-27 and revealed a higher risk of multiple pregnancy and the outcome (NNM), which was also observed in the findings of this study. It is also noteworthy that this variable is considered a risk factor for neonatal mortality
21,25 and the worst results for severe neonatal morbidity,
14 being important that prenatal care services monitor high-risk pregnancies, providing appropriate information to multiparous women about the consequences and risks of multiparity.
27As for the number of live children in previous pregnancies and their relationship with NNM,
14 there is still no scientific evidence, although this study identified an association of NNM with the mother having no or one live-born child in a previous pregnancy. Therefore, the insertion of this variable in future studies is questionable, since pregnancy history has been gaining relevance in the literature because it acts on neonatal outcomes and prognoses, with a greater chance of neonatal mortality in mothers who have a history of child death.
29The research identified an association between NNM and being born in a public/university and philanthropic hospital, besides presenting a higher NNMR among neonates born in public hospitals, as was identified in Joinville-SC.
11 Still about the place of birth and NNM, a study identified that maternity hospitals/hospitals located in the capitals
26 showed a greater association with near miss. This association, also observed in this research, may have been favored by the fact that maternity hospitals located in the capital of Mato Grosso State, especially public/university hospitals, have specialized and reference services to assist pregnant women and neonates at risk, providing care protocols, trained professionals and use of technologies.
Non-induced labor was associated with NNM, however, no studies with this variable were identified, signaling the need for investment in future research of this variable with NNM, given its relevance in conducting childbirths.
30As already mentioned, there are difficulties in comparing results among NNM research due to the lack of agreement on the concept and the criteria for its classification. Nevertheless, it is consensual that this new model of neonatal mortality analysis can be used in diversified contexts, guiding effective interventions that may improve the quality of neonatal care,
3,7 even if its applicability in services is still a great challenge.
The limitations of the study were due to the use of data from secondary sources, with a lack of relevant information for epidemiological studies on maternal and child health, besides the incompleteness of some variables analyzed, making inferences difficult. Another limitation of this study was the exclusive use of a single criterion, the pragmatic one, which resulted in a reduced number of NNM, but by covering the entire neonatal period it broadened the identification of cases and balanced the values found.
In this study, the NNMR was higher than the NMR, with 3.04 NNM cases for each death. The variables that showed association with NNM were the maternal age of 35 or more years old, less than six prenatal visits, non-cephalic fetal presentation, multiple pregnancy, having had no or one live-born child, being born in a public/university and philanthropic hospital, and non-induced labor. Still, these findings should be discussed with caution, in order to seek further evidence of the factors involved.
The results showed the relevance of determining NNM in the distribution of maternal characteristics, care and obstetric history, since they are factors that are amenable for intervention. In conclusion the investigation of NNM cases and associated factors has relevant implications for the health system, contributing to improve the quality of care and consequently reducing neonatal deaths.
References1. United Nations Inter-Agency Group for Child Mortality Estimation (UN IGME). Levels & trends in child mortality: Report 2018. Estimates Developed by the UN Inter-agency Group for Child Mortality Estimation. United Nations Children's Fund: New York; 2018. [access in 2021 mar 3]. Available from:
https://www.unicef.org/media/47626/file/UN-IGME-Child-Mortality-Report-2018.pdf2. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis. Saúde Brasil 2019 uma análise da situação de saúde com enfoque nas doenças imunopreveníveis e na imunização. Brasília (DF): Ministério da Saúde; 2019. [access in 2021 mar 3]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/saude_brasil_2019_analise_situacao.pdf3. Santos JP, Pileggi-Castro C, Júnior JSC, Silva AA, Duran P, Serruya SJ,
et al. Neonatal near miss: a systematic review. BMC Pregnancy and Childbirth. 2015; 15(320):1-10.
4. Kale PL, Mello- Jorge MHP, Silva KS, Fonseca SC. Neonatal near miss and mortality: factors associated with life-threatening conditions in newborns at six public maternity hospitals in Southeast Brazil. Cad Saúde Pública. 2017; 33 (4): 1-12.
5. Santos JP, Cecatti JG, Serruya SJ, Almeida PV, Duran P, De Mucio B,
et al. Neonatal Near Miss: the need for a standard definition and appropriate criteria and the rationale for a prospective surveillance system. Clinics. 2015; 70 (12): 820-6.
6. Lima THB, Katz L, Kassar SB, Amorim MM. Neonatal near miss determinants at a maternity hospital for high-risk pregnancy in Northeastern Brazil: a prospective study. BMC Pregnancy Childbirth. 2018; 18 (401): 1-8.
7. Surve S, Chauhan S, Kulkarni R. Neonatal near miss review: Tracking its conceptual evolution and way forward. Curr Pediatr Rev. 2017; 21 (2): 264-71.
8. Modes PSSA, Gaíva MAM. Near miss Neonatal: revisão integrativa. Res Soc Dev. 2020; 9 (11): 1-21.
9. França KEX, Vilela MBR, Frias PG, Gaspar GS, Sarinho SW. Near miss neonatal precoce identificado com base em sistemas de informação em saúde. Cad Saúde Pública. 2018; 34 (9): 1-10.
10. Silva AAM, Leite ÁJM, Lamy ZC, Moreira MEL, Gurgel RQ, Cunha AJLA,
et al. Morbidade neonatal near miss na pesquisa Nascer no Brasil. Cad Saúde Pública. 2014; Sup 30: S182-91.
11. Silva GA, Rosa KA, Saguier ESF, Henning E, Mucha F, Franco SC. Estudo de base populacional sobre a prevalência de
near miss neonatal em município do sul do Brasil: prevalência e fatores associados. Rev Bras. Saúde Matern Infant. 2017; 17 (1): 169-77.
12. Kale PL, Jorge MHPM, Laurenti R, Fonseca SC, Silva KS. Critérios pragmáticos da definição de
near miss neonatal: um estudo comparativo. Rev Saúde Pública. 2017; 51 (111): 1-11.
13. Brustulin R, Marson PG. Inclusão de etapa de pós-processamento determinístico para o aumento de performance do relacionamento (linkage) probabilístico. Cad Saúde Pública. 2018; 34 (6): 1-13.
14. Lopes FNB, Gouveia APM, Carvalho OMC, Viana Júnior AB, Leite AJM, Araujo Júnior E,
et al. Associated factors with neonatal near miss in twin pregnancies in a public referral maternity unit in Brazil. J Turk Ger Gynecol Assoc. 2021; 22: 12-21.
15. Brasil DRPA, Vilela MBR, França KEX, Sarinho SW. Neonatal morbidity near miss in tertiary hospitals in a capital of Northeast Brazil. Rev Paul Pediatr. 2019; 37 (3): 275-82.
16. Bakari A, Bell AJ, Oppong SA, Bockarie Y, Wobil P, Plange-Rhule G,
et al. Neonatal near-misses in Ghana: a prospective, observational, multi-center study. BMC Pediatr. 2019; 19 (509): 1-10.
17. França KEX, Vilela MBR, Frias PG, Sarinho SW.
Near miss neonatal precoce em hospital universitário: estudo transversal comparativo. Rev Paul Pediatr. 2021; 39: 1-7.
18. Bezerra NF, Rassy MEC, Alves BLA, Carvalho TCN, Bandeira FJS. Factors related to the neonatal mortality. J Nurs UFPE. 2016; 10 (11): 3951-59.
19. Garcia LP, Fernandes CM, Traeber J. Risk factors for neonatal death in the capital city with the lowest infant mortality rate in Brazil. J Pediatr (Rio J). 2019; 95 (2): 194-200.
20. Lima JC, Mingarelli AM, Segri NJ, Zavala AAZ, Takano OA. Estudo de base populacional sobre mortalidade infantil. Ciênc Saúde Colet. 2017; 22 (3): 931-9.
21. Demitto MO, Gravena AAF, Dell'Agnolo CM, Antunes MB, Pelloso SM. High risk pregnancies and factors associated with neonatal death. Rev Esc Enferm USP. 2017; 51: e03208.
22. Shroff BD, Ninama NH. A Call for Eminence Obstetrics Care by Way of ''Neonatal Near Miss'' Events (NNM): A Hospital-Based Case-Control Study. J Obstet Gynaecol Índia. 2019; 69 (1): 50-5.
23. American Academy of Pediatrics Committee on Fetus and Newborn; American College of Obstetricians and Gynecologists Committee on Obstetric Practice. The Apgar Score. Pediatrics. 2015; 136 (4): 819-24.
24. Veloso FCS, Kassar LML, Oliveira MJC, Lima THB, Bueno NB, Gurgel RQ,
et al. Analysis of neonatal mortality risk factors in Brazil: a systematic review and meta-analysis of observational studies. J Pediatr (Rio J).2019; 95 (5): 519-30.
25. Martinelli KG, Gama SGN, Almeida AHV, Pacheco VE, Santos Neto ET. Advanced maternal age and factors associated with neonatal near miss in nulliparous and multiparous women. Cad Saúde Pública. 2019; 35 (12): 1-13.
26. Pereira TG, Rocha DM, Fonseca VM, Moreira MEL, Gama SGN. Fatores associados ao near miss neonatal no Brasil. Rev Saúde Pública. 2020; 54 (123): 1-11.
27. MershaA, Bante A, Shibiru S. Factors associated with neonatal near-miss in selected hospitals of Gamo and Gofa zones, southern Ethiopia: nested case- control study. BMC Pregnancy Childbirth. 2019; 19 (516): 1-8.
28. Valente MP, Afonso MC, Clode N. O parto pélvico vaginal ainda é uma opção segura?. Rev Bras Ginecol Obstet. . 2020; 42(1): 712-16.
29. Sleutjes FCM, Parada CMGL, Carvalhaes MABL, Temer MJ. Risk factors for neonatal death in an inland region in the State of São Paulo Brazil. Ciênc Saúde Colet. 2018; 23 (8): 2713-20.
30. Alfirevic Z, Keeney E, Dowswell T, Welton NJ, Medley N, Dias S,
et al. Which method is best for the induction of labour? A systematic review, network meta-analysis and cost-effectiveness analysis. Health Technol Assess. 2016; 20 (65).
Received on June 18, 2021
Final version presented February 7, 2023
Approved on February 23, 2023
Associated Editor: Samir Kassar
Authors' contribution: Modes PSSA: research design and development, data collection and analysis, writing of the manuscript. Gaíva MAM: participated in all stages of the research. Acted in the corrections and writing of the manuscript.
Andrade ACS: statistician who helped in the construction of the project methodology, assisted in the analysis and interpretation of the data, software used in the analyses and corrections of the manuscript; Guimarães LV: assisted in the construction of the project, in conducting the research, in the interpretation of the data, and in the correction of the manuscript.
The authors approved the final version of the article and declare no conflict of interest.


 ; Maria Aparecida Munhoz Gaíva2
; Maria Aparecida Munhoz Gaíva2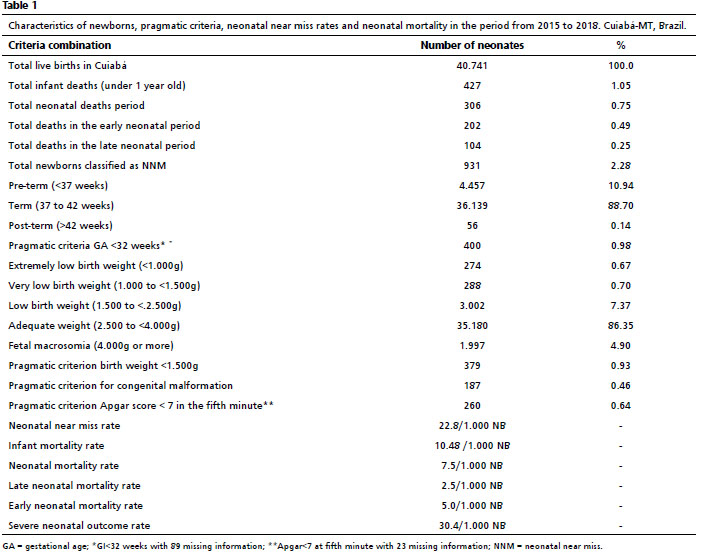







 Ler em português
Ler em português