ABSTRACT
OBJECTIVES: to evaluate the influence of perception of care and maternal protection on breastfeeding practices on the infants' third month of life.
METHODS: longitudinal study with mother-infant pairs distributed in five groupsof gestational clinical conditions. The recruitment occurred in the period 2011 to 2016 at three hospitals in the public health systems in Porto Alegre, Brazil. The Parental Bonding Instrument and the Edinburgh Postpartum Depression Scale were assessed. Exclusive and prolonged breastfeeding were analyzed by questionnaires. Data were analyzed by one-way ANOVA with Tukey's post-hoc test, Kruskal-Wallis with Dunn's post-hoc test, or Pearson's chi-squared test. The significance was set at 5%.
RESULTS: 209 mother-infant pairs were investigated. Among those who did not practice breastfeeding, a lower perception of care, a higher perception of maternal protection, and a higher score of postpartum depression were observed (p=0.022, p=0.038, and p<0.001, respectively), when compared to peers who practiced. The control group had a significantly higher perception of care when compared to thediabetes mellitus group (p=0.006), and the perception of maternal protection and postpartum depression had no differences between the intrauterine groups (p>0.05).
CONCLUSIONS: the perception of care and maternalprotection and the postpartum depressive symptomatology influenced breastfeeding at three months. It is possible to assume a transgenerational effect on breastfeeding, suggesting the existence of a complex model related to mental health in a sample of women who had different backgrounds of gestational clinical conditions
Keywords:
en_v23e20200278.pdf
RESUMO
OBJETIVOS: avaliar a influência da percepção do cuidado e da proteção materna sobre as práticas de aleitamento materno em lactentes no terceiro mês de vida.
MÉTODOS: estudo longitudinal, com pares mães-lactentes distribuídos em cinco grupos de diferentes condições clínicas gestacionais. O recrutamento ocorreu no período de 2011 a 2016 em três hospitais da rede pública de saúde de Porto Alegre, Brasil. Foram utilizados o Parental Bonding Instrument e o Edinburgh Postpartun Depression Scale. O aleitamento materno exclusivo e continuado foi analisado por questionários. Na análise de dados foram utilizados os testes de ANOVA com post-hoc de Tukey, Kruskal-Wallis com post-hoc de Dunn e Qui-quadrado.
RESULTADOS: foram investigados 209 pares mães-lactentes. Entre aqueles que não praticaram o aleitamento materno foi observadouma menor percepção de cuidado materno, uma maior percepção de proteção materna e ummaior escore de depressão pós-parto (p=0,022, p=0,038 e p<0,001, respectivamente) quandocomparados aos pares mães-lactentes que praticaram. O grupo controle teve significativamente maior percepção do cuidado materno quando comparado ao grupo com diabetes mellitus (p=0,006) enquanto a percepção de proteção materna e a depressão pós-parto não apresentaram diferenças entre os cinco grupos intrauterinos (p>0,05).
CONCLUSÕES: a percepção de cuidado e proteção materna e asintomatologia depressiva pós-parto influenciaram o aleitamento materno aos três meses. É possível assumir um efeito transgeracional no aleitamento materno, sugerindo a existência de um modelo complexo relacionado à saúde mental numa amostra de mulheres que tinham diferentes antecedentes de condições clínicas gestacionais.
Palavras-chave:
Comportamento materno, Aleitamento materno, Estudo longitudinal, Depressão
IntroductionThe World Health Organization (WHO) recommended exclusive breastfeeding (EBF) practices for six months of age with continued breastfeeding (BF) up to two years of age or beyond.
1 Meanwhile, in Brazil, even considering this strong recommendation, it is known that the of EBF in children aged zero to six months was around 41% in all capital cities, while the prevalence of BF in children aged nine to 12 months was 58.7%.
2 BF is the first feeding practice to be encouraged to promote positive short- and long-term effects on the child's health, nutrition, and development and women's health and human capital.
1Evidence showedthat the initiation and maintenance of BF practices areassociated with multiple factors, emphasizing the contextual elements and those related to maternal sociodemographic characteristics, maternal smoking, maternal conditions during pregnancy, and dyad separation, among several aspects interacting with each other.
3Maternal mental health has a positive relation with some types of care behaviors,
4 which may have consequences on mother-infant interactions, infant temper, sleep, mental development and health, and internalizing behavior, for example.
5Specifically, maternal's poor mental well-being, like postpartum depression, was a risk factor for early and partial EBF interruption and reduction in breastfeeding duration and early infant formula introduction, implying a greater risk to the child's health.
6 There is evidence of intergenerational transmission of parenting behavior, with reported parenting of grandmothers associated with observed parenting in mothers,
7 interacting with fetal growth, and affecting the grandchildren's care skills at 18 months of age.
8In addition, other studies have concluded that the parental care style exercised during childhood interferes negatively in the lives of their children, reflecting prenatal and postnatal symptoms of depression and anxiety.
9 More recently, due to the covid-19 pandemic, individuals with high and low care control suffered more from confinement and with that, there was an increase in anxiety and depression levels.
10Despite extensive research into the aforementioned factors, the relationship between perception of care and maternal protection, as well as postpartum maternal depression with BF, was little investigated. In this context, this study aimed to investigate the influence of the perception of care and maternal protection and postpartum depression on BF practices in the third month in a sample of postpartum women from different backgrounds of gestational clinical conditions.
MethodsThis longitudinal observational study is a part of a research project titled "Impact of Perinatal Environmental Variations in the First Six Months of Life" - the IVAPSA Birth cohort, which aimed to assess the influence of adverse intrauterine environments, resulting from different gestational clinical conditions on childhood growth, behavior, and neurodevelopment. The study protocol has been published, as well as some baseline results.
11The participants' recruitment occurred in the period 2011 to 2016 at three public hospitals, references for prenatal and perinatal care of high-risk pregnancies by the public health system in Porto Alegre, the state capital in the extreme south of Brazil. The socioeconomic characteristics of the pregnant women seen in these hospitals are very similar.
The sample was divided into adverse intrauterine environment groups, according to the clinical conditions during pregnancy, considering the following criteria:
1) smoking group: mothers who reported smoking during pregnancy, regardless of the duration of exposure or the number of cigarettes smoked. Cigarette consumption after pregnancy has not been investigated.
2) diabetes mellitus (DM) group: mothers who reported a diagnosis of DM (gestational, type 1 and 2). The information was confirmed in hospital records.
3) small for gestational age (SGA) group newborns: full-term infants who were below the fifth percentile of the reference curve, because of intrauterine growth restriction (IUGR).
4) control group: mothers without characteristics previously mentioned and whose newborns were not SGA.
For this study, participants in each group had the defined condition alone. All mothers were residents of Porto Alegre. The sample did not include HIV-positive mothers, with premature birth (gestational age < 37 weeks), multiple pregnancies, or newborns with congenital malformations or who required early hospitalization
The initial recruitment and interview were carried out within 24 to 48 hours after childbirth, during rooming-in. After that, four evaluations occurred: on the 7
th and 15
th day and in the 1
st and 3
rd month after birth. Three of these interviews were home visits (7
th and 15
th, 3
rd month), while the one-month visit was scheduled at the Clinical Research Center (CRC). At all interviews, mothers were reminded about the next interview appointment and asked to return to CRC or receive the interviewers at home, as appropriate. Before data collection, clinical supervisors and interviewers (undergraduate and graduate students of biomedicine, medicine, nursing, nutrition, and physiotherapy) were trained and certified by the study coordinators to ensure standardized data collection.
For this study, the maternal variables evaluated were age (years), ethnicity (white or no white), schooling (years), marital status (married and lives with a companion or no single partner or separated), desired pregnancy (yes or no) and pregestational body mass index (BMI, Kg/m²). The gestational assistance variables used were a type of delivery (cesarean or vaginal) and prenatal consultations (number). Newborn variables included birth weight (g), length at birth (cm), cephalic perimeter (cm), and sex (male or female).
Exclusive and prolonged BF were analyzed from birth to three months by structured questionnaires applied postpartum and during the interviews occurred in: seven days, 15-day, one month, and three months postpartum. The period of food given to the child was recorded using a 24-h diet recall.
The EBF classification excluded all other solids or liquids besides human milk, except for vitamin and mineral supplements, oral rehydration salts, or medicines in oral solution or syrup form. Thus, children who received only breast milk were considered EBF. The prolonged breastfed group included children who received, besides breast milk, water, water-based drinks, teas, infusions, sugar water, fruit juice, and/or any other solid-liquid food.
12The evaluation of the perception of care and and maternal protection was conducted during the three-month home-visit interview, using the Parental Bonding Instrument (PBI),
13 cross-cultural adaptation to Portuguese.
14Internal consistency coefficients for the assessment of maternal bonding were 0.91 (care) and 0.87 (protection).
15 This 25-item self-reported questionnaire examines retrospectively maternal rearing style during their first 16 years of life, from the subject's viewpoint, on a 4-point Likert scale of 0 to 3. The 12 items on the care subscale allow for a maximum score of 36, indicating parental affection, understanding, closeness, and emotional support, and a minimum score of 0, indicating parental coldness, indifference, and emotional rejection. The cutoff point forthe care subscale used was 27. On the protection subscale, a maximum score of 39 is indicative of parental intrusiveness, control, and prevention of independent behavior, while a minimum score of 0 suggests encouragement of autonomy and independence. The cutoff point for the protection subscale used was 13.5.
The presence of depressive symptoms in the postnatal period was investigated by the validated Edinburgh Postpartum Depression Scale (EPDS),
16 a 10-item self-report questionnaire, administered also during the three-month home-visit interview. Mothers were asked to describe their mood during the preceding seven days on a scale from 0 to 3, with higher scores indicating postpartum depressive symptoms. For the Brazilian population, a Portuguese version validated used the cutoff point considered positive for depressive symptomatology was a value equal to or superior to 10, with 82.6% sensitivity and 65.4% specificity.
17The initial sample was based on the effect size of 0.5 standard deviations (SD) of difference between the average z-score of weight, level of significance of 5%, and test power of 80%. It was calculated that 72 mother-child pairs per group and 144 pairs in the control group, summing up a total of 432 pairs. Estimating a loss of follow-up of 20%, the size of the final sample consisted of 521 mother-child pairs.
11 For this study, it was estimated a sample number of 200 mother-child pairs, considering an effect size of 0.25 and atest power of 80%. This calculation was performed in the G Power
® program version 3.1.9.
Continuous variables were represented by mean ± (SD) or median and interquartile range (IR) (median
25, p
75]), as appropriate. The categorical variables were presented as the absolute (n) and relative (%) frequency. Continuous parametric data were analyzed by one-way analysis of variance (ANOVA) with Tukey's post hoc test, while continuous nonparametric data were analyzed by the Kruskal-Wallis test with Dunn's post-hoc test, and the Pearson's chi-squared test was used to categorical variables. The final analyses were adjusted for infant's sex, birth weight, and postpartum depressive symptoms, variables related to the outcomes of the behavior. The significance level was set at 5% (
p<0.05) for all tests. The significance level w as set at 5% (
p<0.05) for all tests. Statistical analyses were conducted at the individual level in the IBM SPSS (PASW)
® version 18.0.
ResultsA total of 209 mother-infant pairs were included in this study.The median maternal age was 25.00 [20.00-31.00] years and 54.5% (n=114) of the neonates were female. Three months after childbirth, 139 mothers (66.5%) were BF non-exclusively, 41 (19.6%) were BF exclusively, and 29 (13.9%) no longer offered breast milk. Considering the intrauterine environments, the control group presented the lowest frequency of weaned infants (11.5%; n=26), while the SGA group had the highest (19.0%; n=7). Indeed, there were no differences between adverse intrauterine environments (
p>0.05) (data not shown).
Table 1 shows maternal sociodemographic and perinatal characteristics of the different adverse intrauterine environments according to the gestational clinical conditions. Mothers from the SGA group had significantly the lowest median age when compared to the DM group (
p=0.035); and the lowest prepregnancy BMI, when compared to the smoking and DM group (
p<0.001). While the smoking group had significantly the lowest prenatal consultations, when compared to the DM group (
p<0.001), had more women with no single partner or separated, when compared to all groups (
p<0.001), and had more women with no desired pregnancy, when compared to DM and control group (
p=0.019). As expected, newborns from the SGA group had significantly lower birth weights, smaller lengths, and lower cephalic perimeters than other groups (
p<0.001). In all groups, the mean perception of care (±SD) was 25.58±7.75, and was observed that the control group had a significantly higher score when compared to the DM group (
p=0.006). The mean perceived maternal protection score was 17.50±7.66 and the median maternal EPDS score was 4 [2-8], both variables without differences among the intrauterine environment groups (
p=0.201 and
p=0.230, respectively). In all samples, 14.3% (n=30) of mothers had EPDS equal or superior to 10 scores.
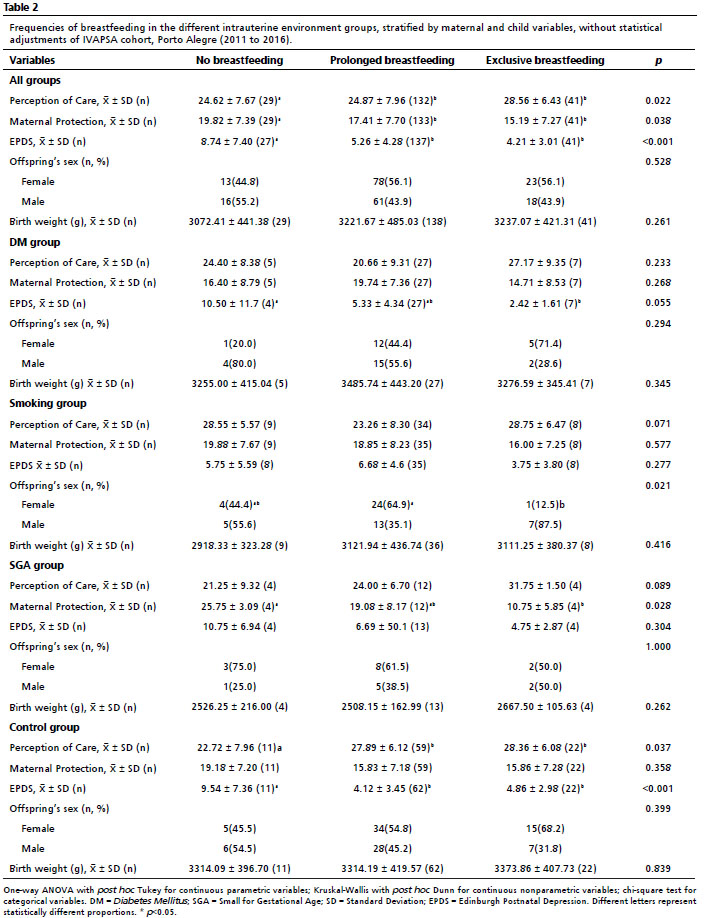
Table 2 shows an unadjusted analysis of the BF practices and maternal and child variables. In the overall sample, it was observed that the levels of perception of care, maternal protection, and EPDS scores were statistically different between BF practice groups. The pairs of mothers-infants presented in the non-breastfed group had the lowest perception of care and EPDS scores, when compared to breastfed group (exclusive or prolonged) (
p=0.022 and
p<0.001, respectively), conversely, in the non-breastfed group there were mothers who highest maternal protection, also when compared to breastfed groups (
p=0.038). Considering the intrauterine environment groups, in the smoking group, it was observed more females than males in prolonged BF, when compared to the EBF group (
p=0.021). In the SGA group, the non-breastfed group had significantly highest maternal protection scores, that compared to the EBF group (
p=0.028). The control group found significantly lowest perception of care and highest EPDS scores in the non-breastfed group when compared to BF groups (
p<0.001).
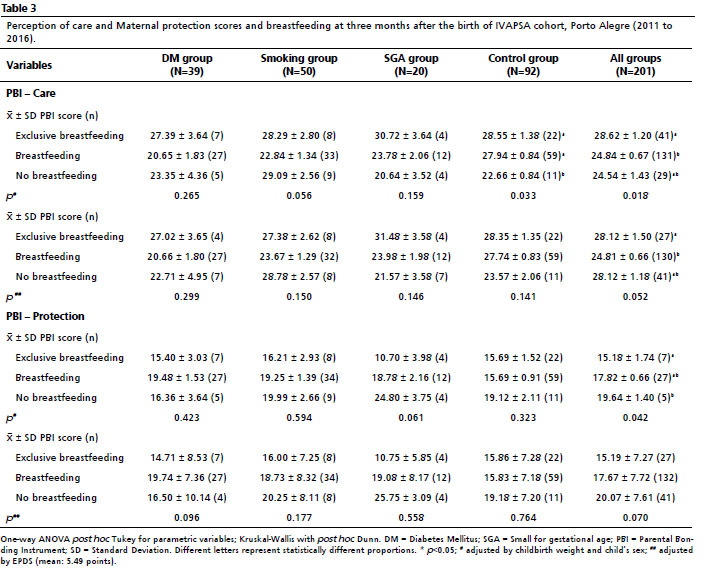
In the analysis adjusted by infant sex and birth weight, Table 3 shows the same trend confirmed in theresults of Table 2. In all groups, it was observed a significant role of perception of care and maternal protection on BF practices in general (
p=0.018 and
p=0.042, respectively). However, these effects were not significant after adjustment for the EPDS score, following the same trend as the results (
p=0.052 and
p=0.070, respectively). There were no differences in the adverse intrauterine environments (
p>0.05).
DiscussionThe perception of care and maternal protection showed an influence on BF practices three months after childbirth as well as maternal depressive symptoms. From these perceptions, it is possible to assume a transgenerational impact on the health and disease pattern through maternal behavior and the child's health. The results also showed that this association can be found in all groups, regardless of different adverse intrauterine exposures.
A lower continued EBF practice was identified in this study. Evidence shows that BF initiation, exclusivity, duration, and cessation depend on a wide range of maternal, child, social, and environmental factors.
3,18 Research about the same sample indicates delayed BF initiation, an additive interaction between maternal pre-pregnancy overweight/obesity and gestational diabetes mellitu.
4In this study, it was found that the mothers from the SGA group had lower age and pregestational BMI values, presumably to restriction mechanisms of their offspring, such as deficiencies in nutrients, a lack of expansion of plasma volume, infection, or other unidentified problems.
19 Besides that, as expected, the SGA infants had significantly lower birth weights, smaller lengths, and lower cephalic perimeters than other groups. In addition to these characteristics at birth, previous publications of this same research group found different patterns of hormone concentrations in breast milk from mothers of SGA newborns, which may be involved in the rapid weight gain of these newborns in the first month of life.
20 And also found that SGA newborns had a greater impact on the growth trajectory in the first six months of life.
21 Likewise, it was found that the mothers from the smoking group had a lower number of prenatal consultations, more women with no partner or separated, and more women with undesired pregnancy, demonstrating an environment of social vulnerability. Regarding the PBI scores, it was observed that the control group presented higher scores in perception of care when compared to the DM group. A cross-sectional study conducted with 71 mother-infant pairs found that maternal depressive symptoms (measured by EPDS) and perception of quality of paternal care (measured by PBI) explained that type of symptom in infants. Thus,good mothering perception can allow the formation of a quality bond between mother and infant,
22 which may then have a positive impact on the management of maternal diseases.
As previously reviewed in the literature, this was the first study to assess the relationship between perception of care and maternal protection on EBF practices at three months postpartum, allowing us to suppose a possible influence of these factors on infant feeding. The mothers who were non-breastfed group until the third month after childbirth had the lowest perception of care, highest EPDS scores, and highest maternal protection when compared to breastfed groups. Data collected from a cohort of 1,226 women who initiated EBF found that lower scores on the postpartum depression risk (measured by EPDS) were significantly associated with EBF practices, lasting 4 months or longer, with greater depression and depressive symptoms reducing both exclusive and non-EBF.
18With the increase in the levels of anxiety and depression in the current times,aggravated by the COVID-19 pandemic,
10 it is important to observe the reflex that it can have on the levels of breastfeeding. There is a wealth of evidence showing the significant influence of individual parenting experiences on behavior.
8 Also, there is evidence that some characteristics of maternal care can be transmitted persistently across generations
23 and influence offspring outcomes.
24 Likewise, it is well known that psychological factors can influence the maternal decision to breastfeed and continue BF,
25 while attitudes toward BF and postpartum depression can be associated with EBF practices.
18 The results of the present study added a new perspective to this issue by showing that perception on maternal behavior (care and protection) can be influenced by the previous generation in such a way as to modify BF practices.
Evidence showed that maternal depression can interact with perception of care in a complex manner to influence EBF practices in a transgenerational model, considering that inadequate maternal bonding is positively correlated with depressive symptoms.
25 Therefore, the style of parental care perceived during childhood can have an impact on offspring in the next generation, reflecting on the children's
8 behavioral outcomes and chronic illness in adulthood.
26Among mothers in the SGA group, those who did not breastfeed displayed lower care scores and higher EPDS scores in the third month postpartum. Poor care and overprotection during childhood and adolescence are associated with unfavorable outcomes in adulthood.
26 A nested cross-sectional study within a Canadian prenatal cohort found that children born SGA whose mothers reported low maternal care during their childhood showed scored lower scores in care set-shifting trait and attention construct at 18 months of age suggesting a complex transgenerational transmission.
8 A cohort study suggests that parental care promoted mental health in adults Born with normal weight and did not have the same protective effect in extremely low birth weight survivors.
27Regarding thequality of parental emotional care, a study suggests that higher maternal care (measured by PBI), represents a lower maternal depressive symptom rate, reducing the prevalence of maternal smoking and decreasing the risk of some diseases in adulthood.
28 Other studies also reported that higher maternal care results in less difficulty identifying and describing feelings
29 (measured by PBI),while greater perception on protection resulting in higher dependency and dysfunctional attitudes and a higher prevalence of chronic pain
30 (measured by general psychopathology tests).
Strengths of this study include its being the first to assess potential relationships between the perception of care and maternal protection of BF practices, characterizing these relationships as transgenerational behavior. Furthermore, all instruments used in the study have been validated for Brazilian Portuguese and have a history of use in several countries and cultures without significant changes in the measured construct, as well as good psychometric properties and stability over the years. In terms of outcome measurement by the PBI questionnaire, there was a wide range of results for perceived protection and care scores, depending mainly on the participants' age, sex, and social backgrounds. In this sense, all the participants in this study presented the same social characteristics, avoiding possible bias.
This study is limited by its sample size because some mothers were lost to follow-up at three months postpartum and could not be included in the final analysis. The sample size may have influenced the analysis of adverse intrauterine environments when comparing to the perception of care and maternal protection scores. Thus, upon filling in the PBI, we had the mothers' report regarding the perception of care of their mothers, although we were not able to obtain information reported from the grandparents themselves.
This research showed a possible transgenerational impact of the perception of care and maternal protection on BF practices at the third month of life, operating in a complex model with mental disorders along with postpartum maternal depressive symptoms. These results can lead to new insight into the prevention of weaning and be used to propose new interventions in terms of counseling and behavioral recommendations during antenatal care.
References1. Rollins NC, Bhandari N, Hajeebhoy N, Horton S, Lutter CK, Martines JC. Why invest, and what it will take to improve breastfeeding practices? Lancet. 2016 Jan; 387 (10017): 491-504.
2. Venancio SI, Escuder MML, Saldiva SRDM, Giugliani ERJ. Breastfeeding practice in the Brazilian capital cities and the Federal District: current status and advances. J Pediatr (Rio J). 2010; 86 (4): 317-24.
3. Cohen SS, Alexander DD, Krebs NF, Young BE, Cabana MD, Erdmann P,
et al. Factors Associated with Breastfeeding Initiation and Continuation: A Meta-Analysis. J Pediatr (Rio J). 2018 Dec; 203: 190-196.e21.
4. Basnet S, Frongillo EA, Nguyen PH, Moore S, Arabi M. Associations of maternal resources with care behaviours differ by resource and behaviour. Matern Child Nutr. 2020 Mar; 16 (3): e12977.
5. Field T. Postnatal anxiety prevalence, predictors and effects on development: A narrative review. Infant Behav Dev. 2018 May; 51: 24-32.
6. Sha T, Gao X, Chen C, Li L, Cheng G, Wu X,
et al. A prospective study of maternal postnatal depressive symptoms with infant-feeding practices in a Chinese birth cohort. BMC Pregnancy Childbirth. 2019 Oct; 19 (1): 388.
7. Madden V, Domoney J, Aumayer K, Sethna V, Lles J, Hubbard I,
et al. Intergenerational transmission of parenting: findings from a UK longitudinal study. Eur J Public Health. 2015 Dec; 25 (6): 1030-5.
8. Neuwald MF, Agranonik M, Portella AK, Fleming A, Wazzana A, Steiner M,
et al. Transgenerational effects of maternal care interact with fetal growth and influence attention skills at 18 months of age. Early Hum Dev. 2014 May; 90 (5): 241-6.
9. Choi H, Yamashita T, Wada Y, Kohigashi M, Mizuhara Y, Nagahara Y,
et al. Predictors for exacerbation/improvement of postpartum depression-A focus on anxiety, the mothers' experiences of being cared for by their parents in childhood and borderline personality: A perspective study in Japan. J Affect Disord. 2013 Sep; 150 (2): 507-12.
10. Bussone S, Pesca C, Tambelli R, Carola V. Psychological Health Issues Subsequent to SARS-Cov 2 Restrictive Measures: The Role of Parental Bonding and Attachment Style. Front Psychiatry. 2020 Nov; 4 (11): 589444.
11. Werlang ICR, Bernardi JR, Nunes M, Marcelino TB, Bosa VL, Michalowski MB,
et al. Impact of Perinatal Different Intrauterine Environments on Child Growth and Development: Planning and Baseline Data for a Cohort Study. JMIR Res Protoc. 2019 Nov; 8 (11): e12970.
12. WHO. Indicators for Assessing Infant and Young Child Feeding Practices. 2008. [access in 2020 fev 5]. Available from:
http://apps.who.int/iris/bitstream/handle/10665/43895/9789241596664_eng.pdf;jsessionid=1A- 5F25F517D247B597B43E89CDF3553C?sequence=113. Parker G. Parental characteristics in relation to depressive disorders. Br J Psychiatry. 1979 Feb; 134: 138-47.
14. Hauck S, Schestatsky S, Terra L, Knijnik L, Sanchez P, Ceitlin LHF. Adaptação transcultural para o português brasileiro do Parental Bonding Instrument (PBI). Rev Psiquiatr Rio Gd Sul. 2006; 28 (2): 162-8.
15. Teodoro MLM, Benetti SPC, Schwarts CB, Mônego BG. Propriedades psicométricas do parental bonding instrument e associação com funiconamento familiar. Aval Psicol. 2020 Abr; 9 (2): 243-51.
16. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987 Jun; 150: 782-6.
17. Santos IS, Matijasevich A, Tavares BF, Barros AJD, Botelho IP, Lapolli C,
et al. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in a sample of mothers from the 2004 Pelotas Birth Cohort Study. Cad Saúde Pública. 2007 Nov; 23 (11): 2577-88.
18. Pitonyak JS, Jessop AB, Pontiggia L, Crivelli-Kovach A. Life Course Factors Associated with Initiation and Continuation of Exclusive Breastfeeding. Matern Child Health J. 2016 Feb; 20 (2): 240-9.
19. Heude B, Thiébaugeorges O, Goua V, Forhan A, Kaminski M, Foliguet B,
et al. Pre-pregnancy body mass index and weight gain during pregnancy: relations with gestational diabetes and hypertension, and birth outcomes. Matern Child Health J. 2012 Feb; 16 (2): 355-63.
20. Nunes M, Silva CH, Bosa VL, Bernardi JR, Werlang IC, Goldani MZ. Could a remarkable decrease in leptin and insulin levels from colostrum to mature milk contribute to early growth catch-up of SGA infants? BMC Pregnancy Childbirth. 2017 Dec; 17 (1): 410.
21. Brito ML, Nunes M, Bernardi JR, Bosa VL, Goldani MZ, Silva CH. Somatic growth in the first six months of life of infants exposed to maternal smoking in pregnancy. BMC Pediatr. 2017 Mar; 17 (1): 67.
22. Maia GN, Frizzo GB, Levandowski DC. Psychofunctional symptoms in infants of young mothers: Association with maternal mental health and parental bonding. Early Hum Dev. 2020 Feb; 141: 104938.
23. Meaney MJ. Maternal care, gene expression, and the transmission of individual differences in stress reactivity across generations. Annu Rev Neurosci. 2001; 24: 1161-92.
24. Hipwell AE, Tung I, Northrup J, Keenan K. Transgenerational associations between maternal childhood stress exposure and profiles of infant emotional reactivity. Dev Psychopathol. 2019 Ago; 31 (3): 887-98.
25. Oyetunji A, Chandra P. Postpartum stress and infant outcome: A review of current literature. Psychiatry Res. 2020 Fev; 284: 112769.
26. Pinquart M. Do the parent-child relationship and parenting behaviors differ between families with a child with and without chronic illness? A meta-analysis. J Pediatr Psychol. 2013 Aug; 38 (7): 708-21.
27. Amani B, Schmidt LA, Saigal S, Lieshout RJV. Exposure to caring parenting and adult mental health in extremely low birthweight survivors. J Paediatrics and child health. 2019 Dez; 55 (12): 1481-6.
28. Almeida ND, Loucks EB, Kubzansky L, Pruessner J, Maselko J, Meaney MJ,
et al. Quality of parental emotional care and calculated risk for coronary heart disease. Psychosom Med. 2010 Feb; 72 (2): 148-55.
29. Thorberg FA, Young RM, Sullivan KA, Lyvers M. Parental bonding and alexithymia: a meta-analysis. Eur Psychiatry. 2011 Apr; 26 (3): 187-93.
30. Herraiz-Serrrano C, Rodríguez-Cano T, Beato-Fernández L, Latorre-Postigo JM, Rojo-Moreno L, Vaz-Leal FJ. Parental rearing and eating psychopathology. Actas Esp Psiquiatr. 2015; 43 (3): 91-8.
Received on July 10, 2020
Final version presented on October 25, 2022
Approved on February 16, 2023
Associated Editor: Aurélio Costa
Authors' contribution: Matos S,Bernardi JR and Werlang IC: Responsible for the data collection and drafted the manuscript.
Guimarães LSP: Responsible for the statistical analysis.
Homrich da Silva C: Responsible for the final conference.
Goldani MZ: Responsible for the study design, and coordinated the IVAPSA study.
All authors approved the final version of the article and declare no conflict of the interest.


 ; Juliana Rombaldi Bernardi2
; Juliana Rombaldi Bernardi2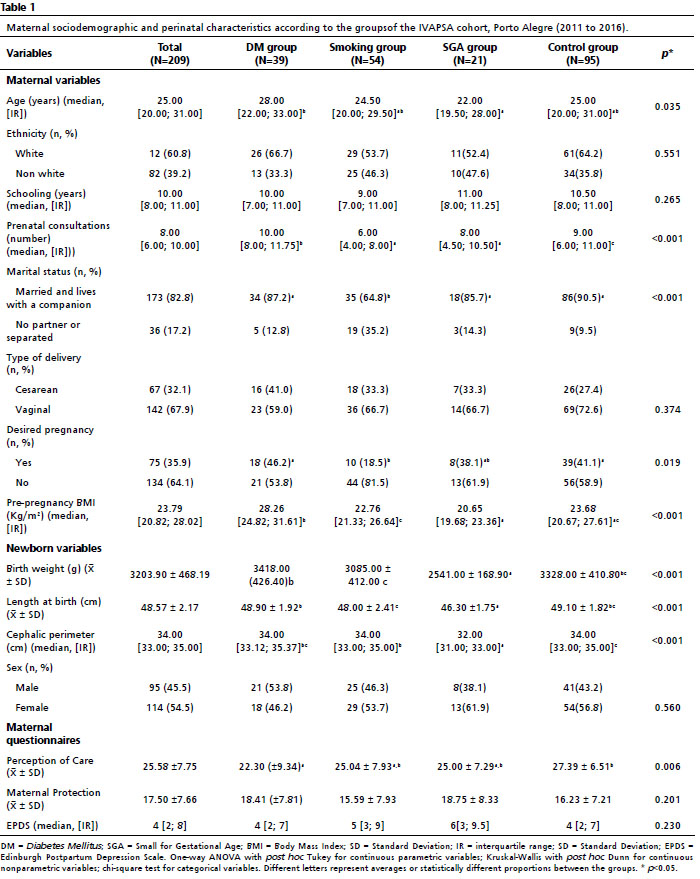






 Ler em português
Ler em português