ABSTRACT
OBJECTIVES: to develop an instrument designed to assess pregnant women's expectations regarding labor and birth.
METHODS: a cross-sectional study was conducted, utilizing two focus groups for the questionnaire's construction: one comprising eight obstetrics professionals and another with six pregnant women.
RESULTS: based on the focus group discussions, a preliminary 22-item questionnaire was developed. Its psychometric properties were tested in a pilot sample of 67 pregnant women. The results were descriptively analyzed and submitted to the validation process, where reliability measures and the validity of content, criterion and construction values were evaluated. The final instrument was composed of 10 items. Factorial analysis indicated three dimensions of the instrument: safety (four questions), feelings (four questions) and concerns (three questions). Its reliability was assessed using Cronbach's Alpha and Spearman Brown statistical tests, yielding values of 0.6727 and 0.7658, respectively.
CONCLUSIONS: the Questionnaire (QEDB) demonstrated adequate psychometric properties to measure pregnant women's expectations, particularly when examining the responses of women in the third trimester. Due to its ease of administration, the instrument can serve as a valuable tool in clinical obstetrics practice and for future research.
Keywords:
Birth expectations, Childbirth, Measurement instruments, Psychometric properties, Questionnaire
IntroductionEvery woman who is about to give birth has preconceptions regarding various environmental and social factors, and these factors can influence the choice of the type of birth, the fear of pain, and even her own experience and satisfaction with childbirth. Expectations reflect a state of anticipation, uncertainty and hope in something yet to be known.
1-4When pregnant women's expectations are met, understood, or validated, the probability of having a positive experience of childbirth increases.
5,6 Providing a positive birth experience is important because satisfaction is linked to self-esteem, which can in turn foster the mother-baby relationship postpartum. Conversely, feelings of frustration, postpartum depression and distress can affect the pregnant woman.
2,6By understanding the expectations of pregnant women, health professionals can help them align their desires with a realistic perspective. It is crucial to promote women's preparation for the difficulties they often encounter by addressing the feelings and emotions that may arise at this time and helping them to have a more satisfying, safer and less fearful experience.
7The level or degree of expectation cannot be measured directly because it lacks a unique understanding or conceptualization, being composed of a variety of feelings and emotions, including the level of anxiety in the face of something new or even unknown. Moreover, such feelings can be shaped by previous experiences or of acquaintances.
2-6Consequently, since it is considered a latent trait, as it cannot be measured directly, the measurement of the degree of expectation should involve the use of a measurement instrument composed of items that are observable facets of this trait. By obtaining a score, one can then gauge how positive or optimistic the pregnant woman is about the period of labor and birth.
8-14 According to the systematic review on the subject,
15 currently, there is no adequate instrument to measure pregnant women's expectations about delivery and birth.
Therefore, the objective of this study was to develop an instrument with appropriate psychometric properties to measure pregnant women's expectations of labor and birth and apply it to a pilot sample (preliminary validation).
MethodsA cross-sectional study was conducted, utilizing focus group interviews to construct the Questionnaire on Expectations of Pregnant Women regarding Delivery and Birth (QEDB). The study was carried out from March 18 to March 19, 2019 at the University of Southern Santa Catarina and the city of Tubarão.
For the first focus group, we aimed to incorporate the different perspectives of obstetrics professionals, inviting obstetricians, nurses, doulas, psychologists from hospitals and outpatient clinics in the city. The first group, which lasted approximately 90 minutes, was composed of eight professionals working in obstetrics: three doctors, four nurses, and one doula. The objective was to ensure representation of all possible members of the delivery and birth team. Participants were invited to share aspects of their experience and professional experience regarding delivery and birth. As an inclusion criterion, health professionals working with pregnant women were invited to represent all possible members of the delivery and birth team. Professionals who, despite their academic training, did not have experience working in the area with pregnant women were excluded.
For the second focus group, we invited pregnant women who were receiving prenatal care at the university's teaching clinic or municipal health units. We included, for convenience, those who agreed to participate. Women who were unable to read at the time of the survey were excluded from this study. The second focus group included six pregnant women and lasted approximately 60 minutes. Pregnant women were invited to discuss aspects related to their expectations, experiences and feelings about delivery and birth. Both groups were conducted in private rooms located at a university in southern Brazil.
The group discussions were led by a psychologist, who moderated the discussion and asked probing questions to explore the opinions in greater detail. The discussions were audio-recorded, and the verbatim transcripts of the speeches were subsequently produced.
After the focus groups were transcribed, all identifying information was removed, and codes were assigned to the participants, ensuring confidentiality and non-identification.
Following the transcription of the focus group discussion, content analysis was employed. This technique is characterized as a study of the researched content that seeks meaning and intentions of words and phrases, as well as comparing and evaluating their meanings.
16 The content analysis resulted in five distinct themes: Influences on the choice of delivery; The choice for cesarean section; The fear of delivery; The present day delivery; and The performance of the professional. The analysis of the content of the pregnant women's group allowed the identification of topics according to the categorization created in the group of professionals. This analysis resulted in 22 items/questions, which constituted the first version of QEDB.
The initial pilot test of the instrument was conducted with women selected in courses for pregnant women offered by regional hospitals and clinics or in doulas circles. All the women present were invited to participate. Since it was self-administered, those who could not read or failed to answer all the questions were excluded.
In addition to the 22 items of the instrument, sociodemographic and gestational variables of the women who participated in the pilot test were assessed, including age, number of children, weeks of gestation, choice of type of delivery and desired birthplace. Women pregnant for the first time were classified as primigravidae, while those who had previously given birth to a viable infant were classified as multiparous. The age of the participants was grouped dichotomously as 18 to 29 years old and ≥30 years old.
The pregnancy trimester was initially grouped in 10 to 15 weeks (1
st trimester), 16 to 27 weeks (2
nd trimester), and 28 to 40 weeks (3
rd trimester). It was subsequently dichotomized to highlight women in the third gestational trimester. For women who reported having a prior choice regarding the type of delivery, the option was categorized as either vaginal delivery or cesarean section.
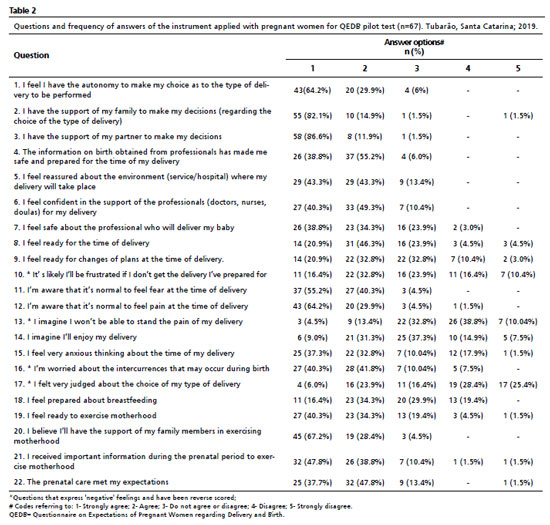
Categorical variables were described as frequencies and percentages, and quantitative variables as the mean and standard deviation or median and interquartile range. The response options for the instrument's items followed a 5-point Likert scale, ranging from "Strongly agree" to "Strongly disagree". A higher response category of the item indicated greater disagreement with the information contained within it. Five questions that expressed feelings considered negative had their scores reversed.
From the sum of the answers, the total score obtained by pregnant women was calculated, serving as the estimate of the latent trait of interest. A low score indicates a more optimistic or positive view/expectation of the pregnant woman, while a high score indicates a more negative expectation regarding the moment of labor and birth.
For the preliminary validation process, reliability measures were used, as well as the content validity, criterion validity (concurrent) and construct validity.
15 As reliability measures, Cronbach's Alpha (which evaluates internal consistency) and a measure obtained by split-half method using the Spearman-Brown formula were used.
17 These measurements range from zero to one, where a score closer to one indicates higher reliability.
The validity of a measuring instrument begins at the moment of its conceptualization and persists throughout the process of elaboration, application, correction and interpretation of results.
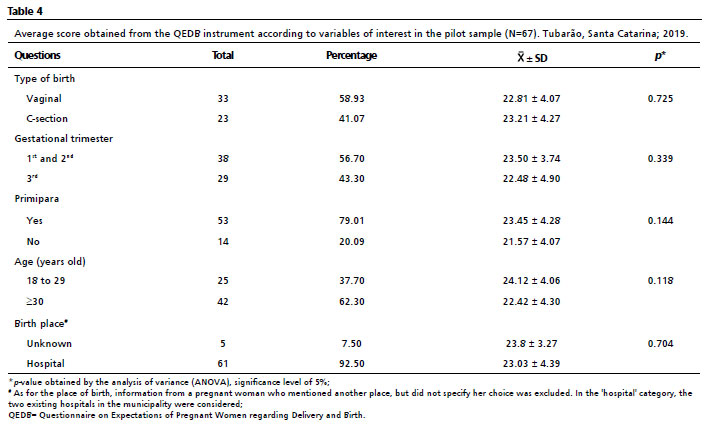
10 Content validity has been described in detail in the procedure section. Criterion validity was assessed by checking the existence of an association (direct or inverse) between the total score (degree of positive/negative expectation of the pregnant woman) and the variables that, theoretically, could be related to high (negative expectation) or low (more positive expectation) values. For categorical variables (age ≥30 years old, primigravida or multiparous status, gestational trimester, choice of delivery type and location, choice of vaginal delivery or cesarean section), analysis of variance was performed to compare the mean scores obtained across the different groups.
Construct validity was assessed through exploratory factor analysis, which verified the latent factor structure of the instrument.
16 The exploratory factor analysis utilized Promax's oblique rotation and Kaiser's measure of the sampling adequacy.
17-19The data obtained were inserted into a structured data base in Microsoft Excel, and analyzed by Statistical Package for Social Sciences (SPSS), version 21.0 (IBM) and Statistical Analysis System (SAS), version 9.4. The level of significance considered was 5%.
This research was approved by the Research Ethics Committee and registered under the following opinion 3.204.605 and CAAE: 04117018.4.0000.5369, in accordance with national regulations and the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to data collection.
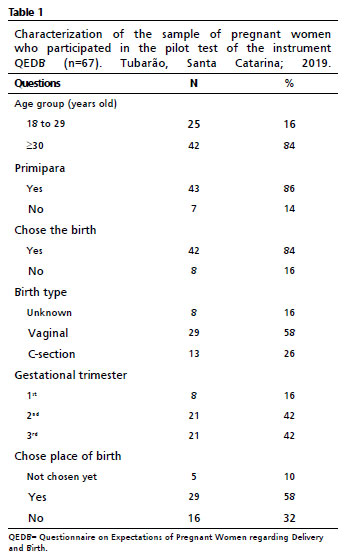
ResultsIn this study, 67 pregnant women answered the instrument, in its 22-item version. The average age of the participants was 30.4 years old (± 4.9), with a minimum age of 20 years old and a maximum age of 42 years old. The average gestational age was 25.13 weeks (± 8.05), ranging from 6 to 38 weeks. Among the participants of the survey, 86% were primiparous.
Table 1 displays the characteristics of the pregnant women who completed the proposed instrument in its first version.
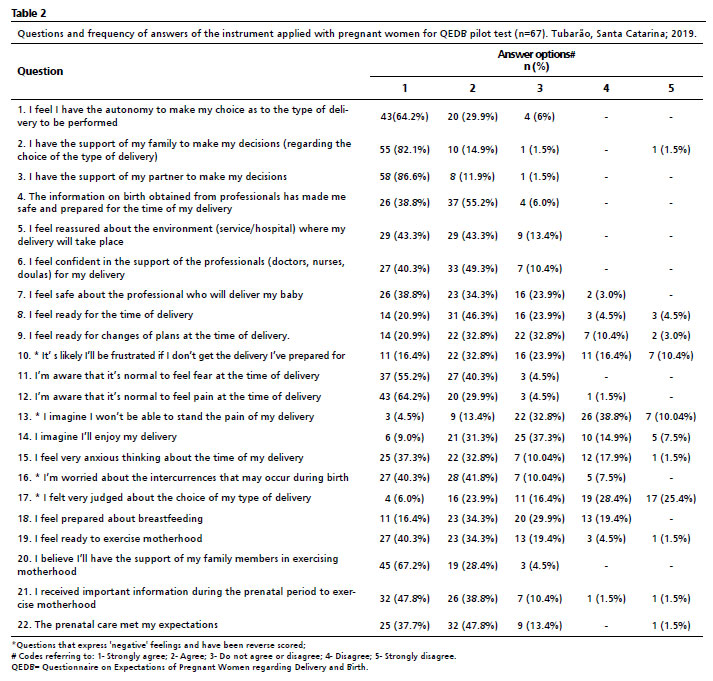
Table 2 describes the frequencies of responses to the questions of the proposed instrument in its complete version used in the pilot test. Questions concerning the choice of type of delivery and family support (1, 2, 3 and 20) were those with the highest frequency of affirmative answers.
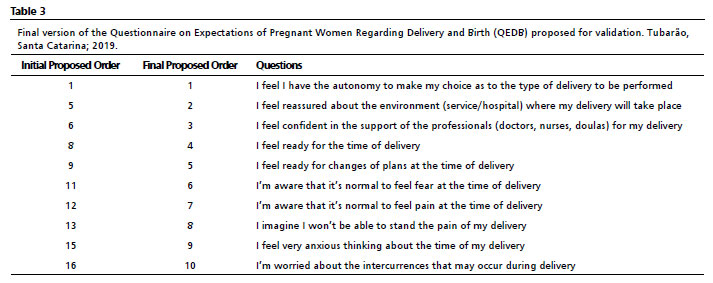
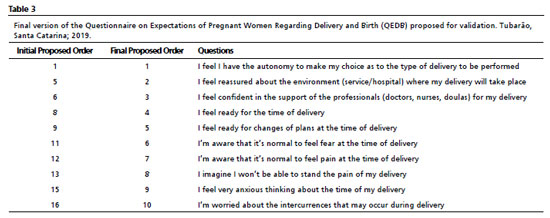
Analysis of the 22 items comprising the questionnaire in the pilot test showed that: 1) Some items were not observable aspects of the latent trait of interest, as they involved questions related to maternity and not only to delivery (questions 18 to 22); 2) Some items were expressing a reality already experienced with more focus than an expectation in itself, as in questions 2, 3 and 17; 3) Some items were overlapping, as they intended to measure the same characteristic through different questions, as in questions 4 and 8; 6 and 7; 9 and 10, with the most comprehensive question chosen in each case. These issues were discussed by the research team and, along with the instrument's reliability analysis, led to the removal of several questions from the final version of the questionnaire, resulting in a proposed final instrument composed of 10 items (Table 3).
The estimate of the degree of expectancy of pregnant women for labor and birth is obtained by the total score (the sum of the answers of each pregnant woman to the 10 items of the proposed instrument) which ranges from 10 (when the pregnant woman answers category 1 for all items) to 50 (when the pregnant woman answers category 5 for the 10 items of the instrument). Therefore, a total score of 10 is considered low, indicating a "good" or optimistic expectation, and a total score of 50 is considered high, indicating a "bad" or more negative expectation.
The instrument's reliability was assessed through Cronbach's Alpha and the measure produced by the split-half method with the Spearman Brown formula, obtaining the values of 0.6727 and 0.7658, respectively. For the 29 pregnant women in the third quarter, Cronbach's Alpha value was 0.7593.
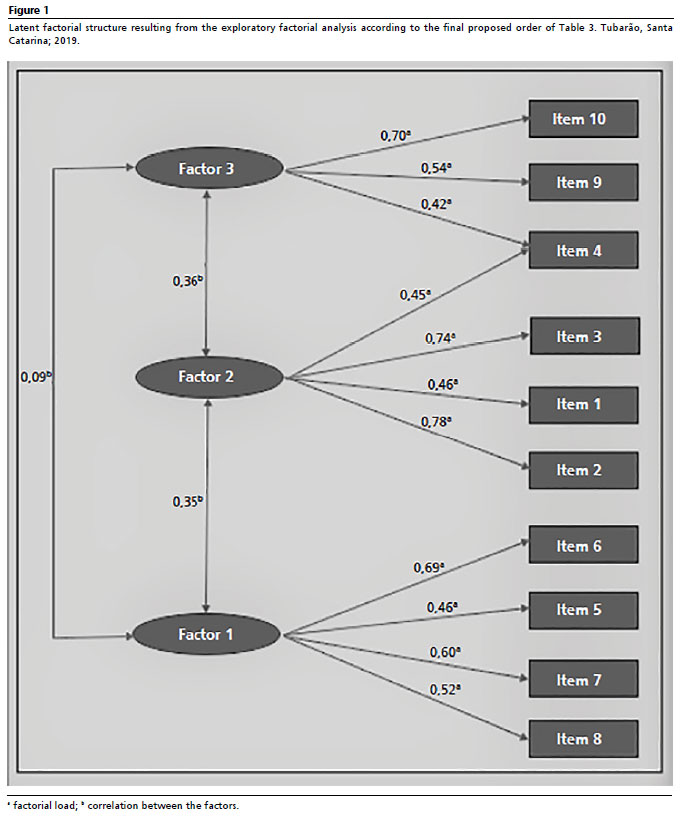
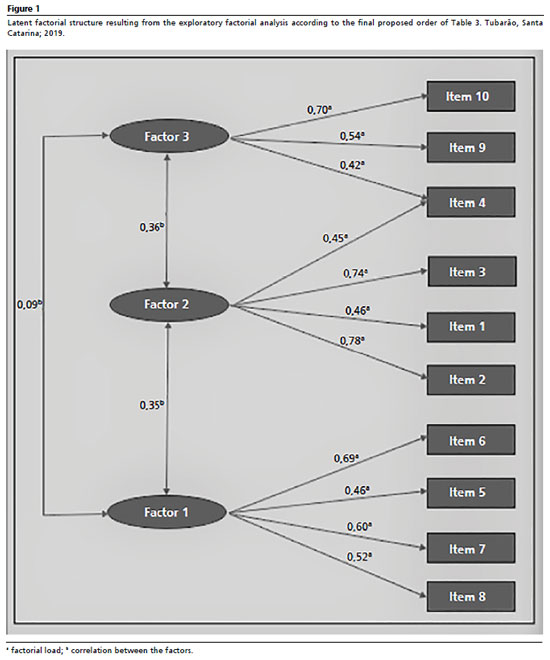
The exploratory factorial analysis identified a latent factorial structure showing that the instrument can be divided into three dimensions (factors), as follows: 1) "Safety", covering questions: 1, 5, 6 and 8, which are related to the feeling of security of the pregnant woman in relation to the care by health professionals, to the environment where she will have her delivery, and in her preparation for the delivery time; 2)"Feelings", covering questions: 9, 11, 12 and 13, which talk about the pregnant woman's feelings when thinking about the moment of birth, such as fear, anxiety and pain; and 3)"Concerns", covering questions 15, 16 and 8, which address the pregnant woman's fears about pain, obstetric interventions and loss of control. The correlation between the factors is presented in Figure 1.
The mean score obtained in the pilot test was 23.06 (±4.28), with a minimum score of 12 and a maximum score of 34. The average score was 24.13 ±4.23 for primigravidae women aged 18 to 29 years old, and 24.00 ±2.82 for multiparous women of the same age group. The primigravidae ≥30 had a score of 22.93 ±4.31, and the multiparous women of the same age group had a score of 21.16 ±4.19. There was no significant difference in the average total score between primigravidae and multiparous women. The total score was lower for women aged 30 years or older, and women who were in the third trimester had a lower score (more positive expectation with childbirth), but without statistically significant differences. The same trend was observed in the score of women who chose vaginal birth; they had a lower score (higher expectation) but there was no significant difference either (Table 4).
DiscussionThis study aimed to develop an instrument to more comprehensively measure women's expectations regarding labor and birth. When applied in a pilot study, the instrument—comprising 10 items in its final version—encompassed three dimensions: safety, emotions, and concerns. Its psychometric properties were satisfactory, especially among women who responded closer to the time of delivery.
Greater internal consistency was observed for pregnant women in the third gestational trimester, indicating more homogeneous responses within this group.
17 Women who are more mature or closer to the delivery date, being at the end of pregnancy, tend to report more positive expectations of delivery. It is plausible to assume that, throughout pregnancy, a woman will seek more information, thus demystifying many fears that arose at the outset,
17-25 leading her to feel better prepared. Most pregnant women who participate in pregnancy groups and courses are "first time mothers", as they seek more greater insight into the previously unknown world of the gravid-puerperal period, as well as how to develop and exercise motherhood, a trend also observed in previous studies.
20-22 In this study, differences in the achieved scores were not verified according to variables that, based on the theoretical framework, could influence expectations. This absence of significance may be attributable to the small sample size.
It was initially hypothesized that women aged 30 and over would exhibit positive expectations regarding delivery, potentially due to greater maturity or a more thorough search for information and pregnancy planning, which could generate greater security.
26-30 However, comparing them with younger yielded no significant differences.
The proposed instrument, in its reduced version, demonstrated satisfactory internal consistency.
17 The QESP instrument, developed in Portugal and validated by Costa
et al.
28 is composed of 108 questions which assess experience, satisfaction and pain in relation to delivery, labor and immediate postpartum, which reached a Cronbach's Alpha value of 0.9032. The "Wijma Delivery Expectancy Questionnaire (WDEQ)" instrument, created by Wijma
et al.
29 measures the feelings of pregnant women in relation to expectations and experiences before (version A) and after delivery (version B) using 33 questions. Its Cronbach's Alpha values ranged from 0.93 to 0.63, across different groups and versions of the same instrument.
29 Based on these comparisons and considering the sample size utilized in the pilot study, the developed instrument obtained an adequate internal consistency value, particularly for women in the third gestational trimester. The validation, involving the refinement of the questionnaire and its application on a larger scale, will be crucial for a more accurate evaluation of its reliability.
The limitations of this study include the small sample size and the difficulty in identifying instruments in the literature that measure the same phenomenon without restricting their focus exclusively to fear and pain during delivery, which would have facilitated a more robust interpretation of the obtained results.
The Questionnaire on Expectations of Pregnant Women Regarding Delivery and Birth (QEDB), in its reduced 10-item version, demonstrated adequate psychometric properties to evaluate pregnant women's expectations. It obtained good scores in its reliability and internal consistency analyses, presented three dimensions of related feelings dimensions, and proved to be easy to administer.
References1. Blomquist JL, Quiroz LH, Handa VL. Mothers' satisfaction with planned vaginal and planned cesarean birth. Am J Perinatol. 2011; 28 (5): 383-8.
2. Ledford CJW, Canzona MR, Womack JJ, Hodge JA. Influence of provider communication on women's delivery expectations and birth experience appraisal: A qualitative study. Fam Med. 2016; 48 (7): 523-31.
3. Moradabadi A, Alavi A, Yabandeh A, Eftekhaari T, Dadipoor S. Factors involved in selecting the birth type among primiparous women. J Educ Health Promot. 2018; 7 (1): 16.
4. Iravani M, Zarean E, Janghorbani M, Bahrami M. Women's needs and expectations during normal labor and delivery. J Educ Health Promot. 2015; 4 (1): 31-7.
5. World Health Organization (WHO). WHO recommendations: Intrapartum Care for a Positive Childbirth Experience. Geneva: WHO; 2018. [
Internet]. [access in 2025 Jan 20]. Available from: https://www.who.int/publications/i/item/9789241550215
6. Lopes RDCS, Donelli TS, Lima CM, Piccinini CA. O antes e o depois: expectativas e experiências de mães sobre o parto. Psicol Reflexão e Crítica. 2005; 18 (2): 247-54.
7. Pasquali L, Primi R. Fundamentos da Teoria da Resposta ao Item –TRI. Avaliação Psicológica. 2003; 2 (2): 99-110.
8. Raymundo PV. Construção e validação de instrumentos: um desafio para a psicolinguística. Let Hoje. 2009; 44 (3): 86-93.
9. Sawyer A, Ayers S, Abbott J, Gyte G, Rabe H, Duley L. Measures of satisfaction with care during labour and birth: A comparative review. BMC Pregnancy Childbirth. 2013; 13 (1): 1.
10. Nilvér H, Begley C, Berg M. Measuring women's childbirth experiences: A systematic review for identification and analysis of validated instruments. BMC Pregnancy Childbirth. 2017; 17 (1): 1-19.
11. Martins GA. Sobre confiabilidade e validade. Rev Bras Gest Negocios. 2006; 8 (20): 1- 12.
12. Korukcu O, Bulut O, Kukulu K. Psychometric Evaluation of the Wijma Delivery Expectancy/Experience Questionnaire Version B. Health Care Women Int. 2016; 37 (5): 550-67.
13. Marques GM, Nascimento DZ, Trevisol DJ, Iser BPM. Instruments measuring pregnant women's expectations of labor and childbirth: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2020 Mar; 246: 90-8.
14. Coluci MZO, Alexandre NMC, Milani D. Construção de instrumentos de medidana
área da saúde. Ciên Saúde Colet. 2015; 20 (3): 925-36.
15. Urbina S. Essentials of Psychological Testing. 4
th ed. Nova Jersey (EUA): Ed. Wiley; 2014.
16. Kaiser HF. A second generation little jiffy. Psychometrika. 1970; 35 (4): 401-15.
17. Kaiser HF, Rice J. Little Jiffy, Mark Iv. Educ Psychol Meas. 1974; 34 (1): 111-7.
18. Cerny BA, Kaiser HF. A study of a measure of sampling adequacy for factor analytic correlation matrices. Multivariate Behav Res. 1977; 12 (1): 43-7.
19. Souza NA, Queiroz LLC, Queiroz RCCS, Ribeiro TSF, Fonseca MSS. Perfil epidemiológico das gestantes atendidas na consulta de pré-natal de uma unidade básica de saúde em São Luís-MA. Rev Ciênc Saúde. 2013; 15 (1): 28-38.
20. Silva AGCB, Silva JL, Lisboa LL, Monteiro RA, Viana ESR. Perfil sociodemográfico e clínico das participantes de um curso para gestantes. Rev APS. 2014; 17 (3): 382-7.
21. Sanfelice C, Beatriz L, Karine R, Stumm E. Crenças e práticas do períodogestacional. Saúde (Santa Maria). 2013; 39 (2): 35-48.
22. Barretos APV, Oliveira ZM. O ser mãe: expectativas de primigestas. Rev Saúde Com. 2010; 6 (1): 9-23.
23. Mandarino NR, Chein MBDC, Monteiro Júnior FDC, Brito LMO, Lamy ZC, Silva Nina VJ,
et al. Aspectos relacionados à escolha do tipo de parto: um estudo comparativo entre uma maternidade pública e outra privada, em São Luís, Maranhão, Brasil. Cad Saúde Pública. 2009; 25 (7): 1587-96.
24. Piccinini CA, Levandowski DC, Gomes AG, Lindenmeyer D, Lopes RS. Expectativas e sentimentos de pais em relação ao bebê durante a gestação. Estud Psicol. 2009; 26 (3): 373-82.
25. CoşkunerPotur D, Mamuk R, Şahin NH, Demirci N, Hamlaci Y. Association between fear of childbirth and maternal acceptance of pregnancy. Int Nurs Rev. 2017; 64 (4): 576-83.
26. Alehagen SIW, Wijma B, Wijma K. Fear of childbirth before, during, and after childbirth. Acta Obstet Gynecol. 2006; 85: 56-62.
27. Bland JM, Altman DG. Cronbach's alpha. BMJ. 1997; 314 (22): 572.
28. Costa R, Figueiredo B, Pacheco A, Marques A, Pais A. Questionário de experiência e satisfação com o parto (QESP). Psicol Saúde Doenças. 2004; 5 (2): 159-87.
29. Wijma K, Wijma B, Zar M. Psychometric aspects of the W-DEQ; a new Questionnaire for the measurement of fear of childbirth. J Psychosom Obstet Gynecol. 1998; 19 (2): 84-97.
30. Fenaroli V, Saita E. Fear of chilbirth: A contribution to the validation of the Italian version of the Wijma delivery expectancy/experience questionnaire (WDEQ). TPM. 2013; 20 (2): 131-54.
AcknowledgementWe acknowledge financial support provided by the National Council for the Improvement of Higher Education (CAPES), Brazil, and the Foundation for Research and Innovation Support of the State of Santa Catarina (FAPESC).
Authors' contribution: Marques GM and Nascimento DZ: study design, data extraction and analysis, and writing and revision of the final manuscript. Souza RCF: contributed to quality assessment and critical review of the manuscript. Giugliani C and Iser BPM: contributed to study design, data analysis, quality assessment, writing, and critical review of the manuscript. Castro SMJ: contributed to data analysis and interpretation, quality assessment, writing and critical review of the manuscript. All authors approved the final version of the article and declared no conflict of the interest.
Data availability: All datasets supporting the result of this study are included in the article.
Received on March 15, 2025
Final version presented on November 26, 2025
Approved on November 28, 2025
Associated Editor: Alex Sandro Souza


 ; Diego Zapelini do Nascimento2
; Diego Zapelini do Nascimento2