ABSTRACT
OBJECTIVES: to assess ovarian reserve in women with endometriosis according to the presence of antithyroid antibodies.
METHODS: retrospective cross-sectional study conducted in assisted reproduction clinics in Recife, Brazil, from February 2017 to August 2021. Women aged 18-49 years with endometriosis and recorded measurements of anti-TPO and/or anti-Tg, anti-Müllerian hormone (AMH), and antral follicle count (AFC) were included. Women with other causes of diminished ovarian reserve were excluded. Numerical variables were compared using the Mann-Whitney test, with p<0.05 considered significant.
RESULTS: of 83 eligible women, 48 were analyzed: 14 (29.2%) antibody-positive and 34 (70.8%) negative. Age and body mass index were similar between groups. No significant differences were found in TSH or free T4 levels. Median AMH was 0.66 ng/mL in the positive group and 1.37 ng/mL in the negative group (p=0.09), and AFC was 7.5 vs. 10.0, respectively (p=0.41).
CONCLUSIONS: among women with endometriosis, a high prevalence of thyroid autoantibodies was observed. There were no statistically significant differences in ovarian reserve markers between groups, although a trend toward lower AMH values was seen among antibody-positive participants. Future studies with larger samples may confirm or modify these findings.
Keywords:
Hashimoto disease, Autoimmune thyroiditis, Ovarian reserve, Fertility, Endometriosis, Autoimmunity
RESUMO
OBJETIVOS: avaliar a reserva ovariana de mulheres com endometriose em idade reprodutiva, com e sem anticorpos antitireoidianos positivos.
MÉTODOS: estudo transversal retrospectivo realizado em clínicas de reprodução assistida em Recife, Pernambuco, entre fevereiro de 2017 a agosto de 2021. Foram incluídas mulheres de 18 a 49 anos, com diagnóstico de endometriose e dosagem registrada de anticorpos antitireoidianos (anticorpos anti-tireoperoxidase – anti-TPO e antitireoglobulina – anti-Tg), hormônio anti-mulleriano (HAM) e contagem de folículos antrais (CFA). Foram excluídas outras causas de baixa reserva ovariana. As variáveis numéricas foram comparadas pelo teste de Mann-Whitney (grupos com e sem anticorpos), considerando p<0,05. Resultados: foram analisados 48 prontuários de mulheres elegíveis com prevalência de 29,2% de mulheres com anticorpos antitireoidianos positivos e 70,8% negativos. A mediana do HAM foi de 0,66 ng/mL no grupo positivo e 1,37 ng/mL no grupo negativo (p=0,09), e a CFA foi de 7,5 e 10,0, respectivamente (p=0,41).
CONCLUSÃO: observou-se uma alta prevalência de anticorpos antitireoidianos positivos em mulheres com endometriose, sem diferença estatisticamente significativa nos marcadores de reserva ovariana, embora com tendência a menores valores de HAM entre as soropositivas. Estudos futuros com amostras ampliadas poderão confirmar ou modificar estes achados.
Palavras-chave:
Tireoidite autoimune, Doença de Hashimoto, Reserva ovariana, Fertilidade, Endometriose, Autoimunidade
IntroductionEndometriosis is a chronic, estrogen-dependent inflammatory disease that affects approximately 10% of women of childbearing age, and is associated with infertility, pelvic pain and impaired quality of life.
1,2 In addition to local mechanisms, there is increasing evidence that systemic immunological and inflammatory alterations participate in the disease's pathophysiology.
3,4Highlighted among these alterations is the potential relationship between endometriosis and autoimmune disorders, particularly those of the thyroid.
5,6 The presence of anti-thyroid antibodies [anti-thyroid peroxidase (anti-TPO) and anti-thyroglobulin (anti-Tg)] is common in women with endometriosis, potentially representing a subclinical autoimmune condition that affects ovarian functions.
7,8 However, the literature reveals conflicting results regarding the impact of thyroid autoimmunity on ovarian reserve, which is estimated by markers such as the Anti-Müllerian Hormone (AMH), and the Antral Follicle Count (AFC).
9,10Given these uncertainties, this study aimed to evaluate the ovarian reserve of women with endometriosis, based on the positivity of anti-thyroid antibodies.
MethodsThis was a retrospective cross-sectional study conducted at assisted reproduction clinics in the f Recife, Pernambuco, Brazil, between February 2017 and August 2021. Women aged 18 to 49 years with endometriosis diagnosis, confirmed by ultrasound or laparoscopy, and laboratory records of AMH, AFC and anti-TPO and/or anti-Tg were included.
Participants with a history of ovarian surgery, chemotherapy, pelvic radiotherapy, recent utilization of hormonal contraceptives, early menopause or acknowledged endocrine diseases that could interfere with ovarian reserve were excluded. Clinical variables included age, body mass index (BMI), serum levels of thyroid-stimulating hormone (TSH) and free thyroxine (FT4).
The AMH and AFC values were compared between the groups with or without antibody positivity. Statistical analysis was conducted using SPPS software, version 20.0, employing Mann-Whitney test for numeric variables and the chi-square test for categoric variables, with
p<0.05 considered statistically significant.
The study was approved by the Research and Ethics Committee of the institution, under CAAE N
o. 66226122.5.0000.5201 and opinion N
o. 5.971.732, on March 29, 2023.
ResultsOf the 83 women initially eligible, 48 met the inclusion criteria, as described in the selection flowchart (Figure 1). Of these, 14 (29.2%) tested positive for antithyroid antibodies and 34 (70.8%) tested negative.
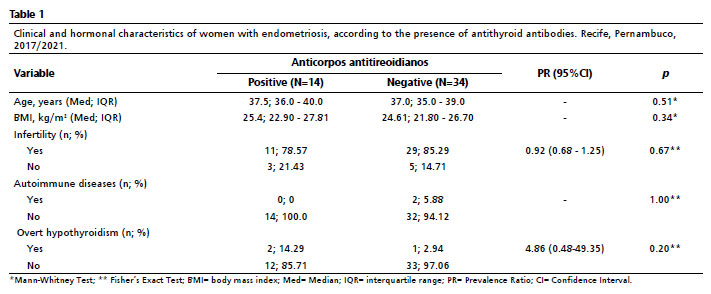
The general clinical and hormonal characteristics are presented in Table 1. The mean ages were 34.7±5.8 and 35.2±6.1 years, respectively, with no significant difference between the groups (
p=0.72). Body Mass Index (BMI) was also similar (23.4 ± 2.7 vs. 23.1 ± 3.0 kg/m²;
p=0.68).
No significant differences were observed in serum TSH levels (2.1±0.7 vs. 2.3±0.9 µIU/mL;
p=0.54) and FT4 (1.1±0.2 vs. 1.2±0.3 ng/dL;
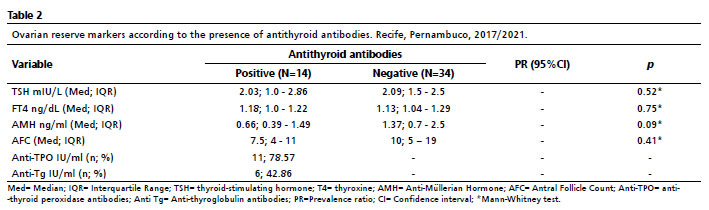
p=0.41). Ovarian reserve markers showed median AMH levels of 0.66 ng/mL in the autoantibody-positive group and 1.37 ng/mL in the negative group (
p=0.09). The median AFC levels of 7.5 and 10.0, respectively (
p=0.41), as shown in Table 2.
A trend towards lower AMH values was observed among women with thyroid autoimmunity, although it did not reach statistical significance. No relevant correlation was found between TSH and AMH levels (r= -0.11;
p=0.39).
DiscussionThe association between endometriosis and autoimmune disorders, particularly thyroid disorders, has been reported by different studies, suggesting that systemic inflammatory processes and immune alterations may be involved with both conditions.
1-4 The presence of anti-thyroid antibodies, such as anti-TPO and anti-Tg, reflects autoimmune activity that may interfere with steroidogenesis and folliculogenesis, thereby indirectly affecting the ovarian reserve.
5,6In this sample of women with endometriosis, the prevalence of thyroid autoimmunity was high (29.2%); however, no significant differences in AMH and AFC were observed between the positive and negative groups. These findings are consistent with those reported by Osuka
et al.
7 and Notaro
et al.,
8 who also found no statistically significant association between thyroid antibodies and diminished ovarian reserve.
Studies with larger samples, however, indicate that subtly lower AMH levels may occur in women with antibody positivity, suggesting a potential follicular damage mediated by inflammation or cytokine-inducted apoptosis.
9-11 Such differences may depend on the stage of the disease, reproductive age and laboratory criteria utilized to define positivity.
The main limitations of this study include the retrospective design, the small sample size, and the lack of control for potential confounders, such as the duration of endometriosis and prior use of hormone therapy. Nevertheless, the consistency of findings with the literature reinforces the notion that isolated thyroid autoimmunity may not exert a clinically relevant impact on the ovarian reserve in women with endometriosis.
12-14The coexistence of endometriosis and thyroid autoimmunity reinforces the complexity of the interface among inflammation, immunity and female fertility. Although no statistically significant difference was observed in the ovarian reserve makers, the trend towards lower AMH levels in seropositive women suggests a potential subclinical influence of autoimmunity over ovarian function. Prospective studies, with greater statistical power and standardization of diagnostic and laboratory criteria will be essential to clarify the role of thyroid autoimmunity on reproductive pathophysiology and the clinical management of endometriosis.
AcknowledgementsWe thank the Professor Fernando Figueira Institute of Integrative Medicine (IMIP), the Institutional Scientific Initiation Scholarship Program (PIBIC), and the National Council for Scientific and Technological Development (CNPq) for the financial support.
References1. Tal R, Seifer DB. Ovarian reserve testing: a user's guide. Am J Obstet Gynecol. 2017 Aug; 217 (2): 129-40.
2. Meskhi A, Seif MW. Premature ovarian failure. Curr Opin Obstet Gynecol. 2006 Aug; 18 (4): 418–26.
3. Jirge PR. Ovarian reserve tests. J Hum Reprod Sci. 2011 Sep; 4 (3): 108-13.
4. Ferraretti AP, la Marca A, Fauser BCJM, Tarlatzis B, Nargund G, Gianaroli L. ESHRE consensus on the definition of "poor response" to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum Reprod. 2011 Jul; 26 (7): 1616-24.
5. Grynberg M, Sermondade N. Fertility preservation: should we reconsider the terminology?. Hum Reprod. 2019 Oct; 34 (10): 1855-7.
6. Martinez F, Andersen CY, Barri PN, Brannigan R, Cobo A, Donnez J,
et al. Update on fertility preservation from the Barcelona International Society for Fertility Preservation–ESHRE–ASRM 2015 expert meeting: indications, results and future perspectives. Fertility Sterility. 2017 Sep; 108 (3): 407-15.e11.
7. Kirshenbaum M, Orvieto R. Premature ovarian insufficiency (POI) and autoimmunity-an update appraisal. J Assist Reprod Genet. 2019 Nov; 36 (11): 2207-15.
8. Seyhan A, Ata B, Uncu G. The impact of endometriosis and its treatment on ovarian reserve. Sem Reprod Med. 2015 Nov; 33 (6): 422-8.
9. Coelho Neto M, Martins W, Luz C, Jianini B, Ferriani R, Navarro P. Endometriosis, ovarian reserve and live birth rate following in vitro fertilization/intracytoplasmic sperm injection. Rev Bras Ginecol Obstetr. 2016 May; 38 (5): 218-24.
10. Shah DK. Diminished ovarian reserve and endometriosis: insult upon injury. Sem Reprod Med. 2013 Feb; 31 (2): 144-9.
11. Sousa Barbosa DA, Oliveira AM. Endometriose e seu impacto na fertilidade feminina. Saúde Ciênc Ação. 2015 Fev; 1 (1): 43-56.
12. Orgiazzi J. Thyroid autoimmunity. La Presse Médicale. 2012 Dec; 41 (12): e611-25.
13. Notaro ALG, Lira Neto FT, Bedoschi GM, Silva MJ, Nunes MC, Lira CCPM,
et al. Evaluation of ovarian reserve in women with thyroid autoimmunity. JBRA Assist Reprod. 2024 Jun; 28 (3): 442–9.
14. Osuka S, Iwase A, Goto M, Takikawa S, Nakamura T, Murase T,
et al. Thyroid Autoantibodies do not Impair the Ovarian Reserve in Euthyroid Infertile Women: A Cross-Sectional Study. Horm Metab Res. 2018 Jul; 50 (7): 537-42.
Authors' contributionSouza ASR and Notaro LGR: conceptualization and study design, data collection and analysis, manuscript writing and review. Ferreira MER, Gomes RC, Rios SV, Chacon VO and Viana MAB: data collection and interpretation and drafting and critical review of the manuscript. All authors approved the final version of the article and declared no conflicts of interest.
Data AvailabilityAll datasets supporting the study are included in the article.
Received on October 19, 2024
Final version presented on October 9, 2025
Approved on October 10, 2025
Associated Editor: Leila Katz


 ; Maria Eduarda Rodrigues Ferreira2
; Maria Eduarda Rodrigues Ferreira2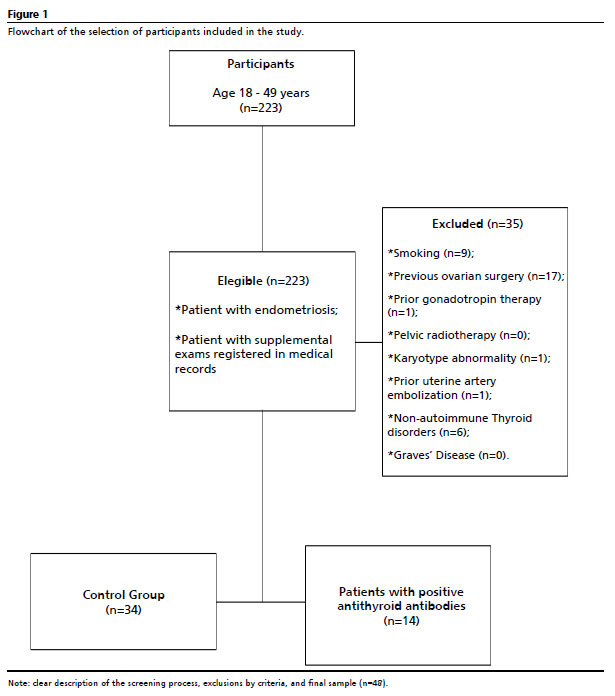






 Ler em português
Ler em português