ABSTRACT
INTRODUCTION: central pontine myelinolysis (CPM) is characterized by the destruction of the myelin sheath from oligodendrocytes due to a rapid increase in plasma osmolarity and consequent passage of components through the blood-brain barrier.
DESCRIPTION: a woman at six weeks of pregnancy, presenting previous uninvestigated generalized tonic-clonic seizures, type 1 diabetes mellitus since childhood, and using both licit and illicit drugs, was admitted to the hospital with CPM diagnosed after dysglycemia. She presented an unfavorable obstetric outcome with a neurological rehabilitation prognosis.
DISCUSSION: the rapid correction of hyponatremia is considered the main cause of CPM among its different etiologies described in the literature, such as relevant dysglycemia, nutritional deficiencies, and drug abuse. This study reported differential diagnoses of CPM in an atypical context (i.e., pregnancy), emphasizing the importance of knowing this multifactorial condition in intensive and obstetric care for appropriate multi-professional clinical management.
Keywords:
Central pontine myelinolysis, Differential diagnosis, Osmolar concentration, Pregnancy
RESUMO
INTRODUÇÃO: a mielinólise pontina central (CMP) é caracterizada pela destruição da bainha de mielina das células oligodendríticas devido a uma elevação rápida da osmolaridade plasmática, com consequente passagem de componentes pela barreira hematoencefálica (prováveis alterações osmóticas abruptas).
DESCRIÇÃO: gestante na sexta semana de idade gestacional, com quadro convulsivo tônico-clônico generalizado prévio nunca investigado, diabetes mellitus tipo I desde a infância e uso de drogas lícitas e ilícitas, foi admitida com diagnóstico de MP após quadro de desregulações glicêmicas, a qual evoluiu com desfecho obstétrico desfavorável, porém, prognóstico neurológico em reabilitação.
DISCUSSÃO: dentre as várias etiologias de MP, a correção brusca da hiponatremia é considerada como principal causa. A literatura, entretanto, descreve causas como alterações glicêmicas importantes, deficiência nutricional e abuso de substâncias. Este relato vem no escopo dos diagnósticos diferenciais, em um contexto atípico - a gestação - evidenciando uma condição multicausal e corroborando com a importância do conhecimento de tal condição na terapia intensiva e obstétrica para adequado manejo clínico multiprofissional.
Palavras-chave:
Mielinólise central pontina, Diagnóstico diferencial, Concentração osmolar, Gravidez
IntroductionCentral pontine myelinolysis (CPM) was first described by Adams
et al.
1 after cases of pseudobulbar palsy and tetraplegia. Subsequent studies established this condition as the osmotic demyelination syndrome (ODS), which affects the white matter of the pons at different levels.
2 Thus, CPM is characterized by the destruction of the myelin sheath from oligodendrocytes due to a rapid increase in plasma osmolarity and passage of compounds (e.g., inositol, betaine, and glutamine) through the blood-brain barrier.
1,2CPM prevalence is still unknown. Indian researchers conducted a retrospective study, describing a 2.5% prevalence of ODS in intensive care units (ICU).
3 Extrapontine myelinolysis occurred in approximately 10% of cases, affecting the midbrain, thalamus, basal nuclei, and cerebellum.
4 Furthermore, CPM presents a high mortality rate, ranging from 40% to 50%.
4Although the mechanisms causing CPM are not well understood, electrolyte imbalance is one of the main causes, particularly during the rapid correction of hyponatremia. Other causes, such as hyperemesis gravidarum, hyperglycemia, malnutrition, liver failure, alcoholism, malignant diseases, hemodialysis, and severe burns, may also lead to fluid and electrolyte imbalance and osmotic change.
5Considering the lack of studies addressing pregnant women with CPM,
6 this study aimed to discuss the possible differential diagnoses and review the case of a pregnant woman with type 1 diabetes mellitus (DM), history of uninvestigated seizures, and using licit and illicit drugs. She presented CPM after episodes of sudden variations in capillary blood glucose, evolving to survival and mid-term partial recovery of neurological activities.
DescriptionFemale patient, 29 years old, multigravida (seven previous pregnancies, including the current one), three live births and three previous abortions, currently in the sixth week of pregnancy. Regarding clinical history, the companion reported that the patient had type 1 DM since she was six years old, was treated for congenital syphilis in childhood, and presented self-limiting seizures since adolescence, which were uninvestigated. Family members also reported that she has used licit and illicit drugs (e.g., alcohol and cannabis) since adolescence, including during pregnancy. The patient denied any other illnesses and had not started prenatal care.
The patient was admitted to the emergency Maternity hospital (Cabo, Pernambuco, Brazil), where she remained for approximately 10h, with psychomotor agitation, nausea and vomiting, and generalized tonic-clonic seizure of unknown duration and spontaneous resolution. Initially, she had no focal neurological signs, but the sensory level was decreased and associated with hyperglycemia during the treatment (capillary blood glucose monitoring: 344 mg/dl). Orotracheal intubation (to preserve the airway), volume expansion, and treatment of dysglycemia were performed, and she was transferred to the ICU of the Professor Fernando Figueira Institute of Integrative Medicine (IMIP – Portuguese acronym; Recife, Pernambuco, Brazil).
The patient presented stable hemodynamic parameters without vasoactive medication, normal pupillary light reflex, sinus rhythm, deep sedation (Richmond Agitation and Sedation Scale: -5) and was afebrile at ICU admission. No acute hemorrhagic or ischemic event was detected in non-contrast head computed tomography. The arterial blood gas test showed marked metabolic acidosis but without evidence of diabetic ketoacidosis nor hyperglycemic hyperosmolar state (pH:7.38; pCO
2:22.9mmHg; pO
2:115.2mmHg; lactate:5.7mmol/l; bicarbonate:13.5mmol/l; base excess: -10.8mmol/l; glycemia:245mg/dl; sodium:138.3mmol/l; potassium:3.62mmol/l; ionized calcium:0.374 mmol/l; oxygen saturation:100%; oxygenation index:548). The serum sodium level at ICU admission corroborated those from the arterial blood gas test (138mmol/l), discarding sensory decrease due to hyponatremia. Also, electrolyte levels were evaluated throughout the ICU stay as routine for critical patients, and sodium levels were maintained in the normal range.
A chest X-ray performed at admission showed diffuse pulmonary infiltrates, pleural effusion at the base of the left hemithorax, and findings compatible with consolidation in the right hemithorax, suggesting community-acquired pneumonia (Figure 1A). An empirical antibiotic regimen started with 2g/day of ceftriaxone (intravenous) and 500mg/day of azithromycin (nasoenteral tube), and 300mg/day of phenytoin (intravenous) was started due to the history of several uninvestigated self-limiting seizures and negative findings for acute events.
The patient was extubated two days after ICU admission and presented minimal cognitive function (only responding to pain stimuli in the four limbs) and spastic tetraparesis. She also presented preserved deep tendon reflexes, eye scanning movements, normal pupillary light reflexes, and no involuntary body movements.
In the following days, the patient was submitted to a magnetic resonance imaging (MRI) and magnetic resonance angiography of the brain, indicating hypersignal in the fluid-attenuated inversion recovery (FLAIR) sequence in the central pons with a sequela aspect, possibly related to osmotic demyelination (Figure 1B). Hypersignal was also detected in the white matter of the left temporal lobe, possibly related to a previous injury (Figure 1C).
The patient presented a slow pattern of cognitive and motor recovery in subsequent neurological assessments, recovering strength in the trunk and upper limbs and swallowing but maintaining relevant dysphasia and agitation. Approximately 20 days after ICU admission with this condition, a state of minimal consciousness was suggested due to chronic multifactorial damage of the brainstem (i.e., dysglycemia, drug abuse, possible sequela of hypoxia from the seizure that brought her to the emergency unit, and nutritional deficiency).
The treatment continued with vitamin B complex supplementation, 750mg/day of valproic acid, and management of
delirium (pharmacological approach using diazepam, levomepromazine, dexmedetomidine, haloperidol, and risperidone and non-pharmacological approach through contact with family members and therapeutic outings). The acquired nosocomial infections (i.e., urinary tract and bloodstream infections) were treated with antibiotic therapy using piperacillin-tazobactam, meropenem, metronidazole, and vancomycin, according to the results of the culture with antibiogram.
The patient was discharged from the ICU to the high-risk pregnancy ward at 21 weeks of pregnancy for obstetric follow-up after general improvement of neurological sequelae and no clinical or laboratory changes. She underwent an obstetric ultrasound, which found no fetal changes. The patient presented premature labor on the 22
nd week of pregnancy and had no intercurrences in the delivery. However, the fetus weighed 340 g (i.e., small for gestational age) and died after 20 minutes of life.
During the delivery, the patient was diagnosed with endometritis by a gynecological examination considering the warm vagina and a fetid odor associated with fever. She was treated with 900 mg of clindamycin (every eight hours) and 240 mg/day of gentamicin for three days. Also, the patient was referred to the ICU due to the potential for clinical worsening, being discharged to the pathological postnatal ward at the end of treatment for adequate control of the type 1 DM and functional rehabilitation with physical and speech therapy.
This study was approved by the research ethics committee of the IMIP. The patient caregiver signed the informed consent form.
DiscussionThis study presented the case of a pregnant woman with type 1 DM, history of uninvestigated seizures, and using both licit and illicit drugs, who was admitted to the emergency unit with emetic episodes and generalized tonic-clonic seizure. She developed CPM, mainly caused by inadequate and difficult glycemic control.
In 1949, Victor and Adams
7 described the case of a patient with tetraplegia, facial weakness, mutism, and bilateral Babinski's sign. They hypothesized that a lesion at the basis pontis would be compromising the cortico-spinal and cortico-bulbar tracts, which was confirmed after necropsy.
7Researchers suggested that CPM could be caused by the rapid correction of hyponatremia based on experimental data in animal models. Later, Sterns
et al.
8 reported neurological complications in 25% of patients whose severe hyponatremia was corrected rapidly, which could be avoided with slow correction.
4,5 The blood-brain barrier is responsible for regulating the passage of substances between the blood and central nervous system. In this sense, brain endothelial cells and astrocytes play a protective role in maintaining iso-osmolarity, preventing tissue damage from possible systemic deregulation. However, cells have a short time to adapt to acute hyponatremia and may induce cerebral edema.
4Previous studies suggested other etiologies for CPM cases without hyponatremia, such as malnutrition, dysglycemia, use of diuretics, end-stage liver disease, liver transplant, and alcohol abuse.
4 Also, patients with alcohol use disorders present suppressed antidiuretic hormone levels characterized by hypovolemia and chronic hyponatremia, further increasing demyelination due to inadequate sodium and water regulation.
4Hyperglycemia and diabetic ketoacidosis are rare causes of CPM with unclear physiopathology, which may involve sudden contraction of brain cells and demyelination due to the rapid increase in plasma osmolarity. Currently, two hypotheses may explain the contraction and myelinolysis of oligodendrocytes: (I) local inflammatory demyelination due to blood-brain barrier damage and (II) apoptosis of oligodendrocytes due to hypertonic stress from osmotic changes, which occur rapidly to allow alterations in specific molecules. Also, dysglycemia due to inadequate DM control may induce an unstable osmotic environment and irregular cell compensation, favoring the onset of CPM.
9Chronic alcohol abuse may be a risk factor for CPM since patients with chronic alcoholism may have few or no symptoms compared with those who developed CPM after rapid correction of hyponatremia.
10 The proposed mechanisms are similar to those previously described, including osmotic damage to brain endothelial cells, which may induce the release of toxic factors for the myelin sheath, vasogenic edema, and brain dehydration. Patients with chronic alcoholism may be unable to maintain protection mechanisms against osmotic stress in the brain and are directly affected by alcohol toxicity. Also, the excessive production of free radicals and the metabolic effects of nitric oxide in these patients may favor the apoptosis of neurons.
10,11Considering that the patient had type 1 DM, presented hyperglycemia at admission to the emergency unit, and is a chronic alcohol user, we hypothesized that dysglycemia combined with chronic alcohol abuse and incipient pregnancy might have led to complications, such as CPM. Similar to the present case, a previous study (2016) reported a patient with type 1 DM, CPM, and regular sodium levels who developed dysarthria, dysphagia, and nasal regurgitation, progressing with partial improvement.
12 In contrast, another study (2017) reported a patient with type 2 DM who developed gait imbalance, dysarthria, and inappropriate laughter, improving significantly after few weeks. The differences between both reports suggested a mixed nature of prognosis in patients with hyperglycemia.
11,13 Thus, dysglycemia from an inadequate treatment may cause osmotic deregulation in the extracellular environment, hindering adequate cellular compensation and leading to CPM, especially if this deregulation occurs during pregnancy.
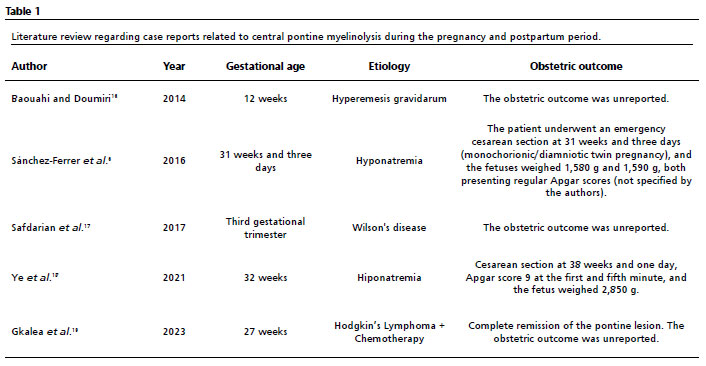
14In 2015, a case similar to the present study described a 42-year-old woman at 14 weeks of a dichorionic-diamniotic twin pregnancy admitted to the emergency unit with hyperemesis gravidarum and malnutrition, who improved after correction of the electrolyte imbalance.
14 However, the patient returned two weeks after discharge, presenting hyperemesis associated with psychomotor retardation, tremors, fluctuation in mental state, urinary incontinence for two days, and sepsis, and CPM was diagnosed by MRI.
15 The neurological condition improved when the hypernatremia was corrected, and she subsequently underwent termination of pregnancy, with improved signs and MRI findings after two months.
15Regarding imaging tests for proper diagnosis of CPM, the sensitivity of the computed tomography in early stages is lower than a conventional MRI, which is considered gold standard to identify lesions. However, clinical-radiological dissociation is plausible, and regular findings in the first days do not exclude CPM diagnosis since changes suggesting demyelination may not appear at this moment, highlighting the importance of follow-up tests between 10 and 14 days in case of suspicious events.
5,6MRI images show a hypointense signal in T1-weighted sequences without contrast, whereas a hyperintense signal is observed in T2-weighted sequences with different shapes according to the slices (i.e., triangular in axial, oval in sagittal, and bat-wing-shaped in coronal).
6 Although lesion severity is not directly related to the symptoms, it tends to reduce in the image with symptoms regression, as shown in the T2 and FLAIR signal.
12 However, the patient was not submitted to a prior imaging examination.
After a literature review using the descriptor "central pontine myelinolysis", 319 articles were found in the PubMed/Medline database in the last ten years; only five were related to pregnancy and postpartum period (Table 1).
In this context, the present study described a pregnant woman diagnosed with an unusual multifactorial condition, excluding the classic etiology (i.e., rapid change in sodium levels) as the cause of CPM. She evolved with an unfavorable obstetric outcome and partial neurological recovery. Thus, this study contributed to future discussions regarding the main etiologies of CPM.
References1. Adams RD, Victor M, Mancall EL. Central pontine myelinolysis: a hitherto undescribed disease occurring in alcoholic and malnourished patients. AMA Arch Neurol Psychiatry. 1959 Feb; 81 (2): 154-72.
2. Danyalian A, Heller D. Central Pontine Myelinolysis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 Jan. [access in 2024 August 20]. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK551697/3. Rao PB, Azim A, Singh N, Baronia AK, Kumar A, Poddar B. Osmotic demyelination syndrome in Intensive Care Unit. Indian J Crit Care Med. 2015; 19 (3): 166-9.
4. Tiwari R, Kumari A. Central Pontine Myelinolysis: a case report. Indian J Crit Care Med. 2022 Sep; 26 (9): 1049-51.
5. Lambeck J, Hieber M, Dreßing A, Niesen WD. Central pontine myelinosis and osmotic demyelination syndrome. Dtsch Arztebl Int. 2019; 116: 600-6.
6. Sánchez-Ferrer ML, Prieto-Sánchez MT, Orozco-Fernández R, Machado-Linde F, Nieto-Diaz A. Central pontine myelinolysis during pregnancy: pathogenesis, diagnosis and management. J Obstet Gynaecol. 2017; 37 (3): 273-9.
7. Victor M, Adams RD. Lesions of the brain stem. Arch Neurol Psychiatry. 1949; 61 (4): 577-92.
8. Sterns RH, Riggs JE, Schochet SS Jr. Osmotic demyelination syndrome following correction of hyponatremia. N Engl J Med 1986; 314: 1535-42.
9. Guerrero WR, Dababneh H, Nadeau SE. Hemiparesis, encephalopathy, and extrapontine osmotic myelinolysis in the setting of hyperosmolar hyperglycemia. J Clin Neurosci. 2013 Jun; 20 (6): 894-6.
10. Yoon B, Shim YS, Chung SW. Central Pontine and Extrapontine Myelinolysis After Alcohol Withdrawal. Alcohol Alcohol. 2008; 43 (6): 647-9.
11. Mir WAY, Shrestha DB, Aryal BB, Reddy VK, Yadullahi MAA. Central Pontine Myelinolysis Secondary to Hyperglycemia in a Young Patient. Cureus. 2021 Oct; 13 (10): e18495.
12. Shah SO, Wang A, Mudambi L, Ghuznavi N, Fekete R. Asymptomatic central pontine myelinolysis: a case report. Case Rep Neurol. 2012 Sep; 4 (3): 167-72.
13. Donnelly H, Connor S, Quirk J. Central pontine myelinolysis secondary to hyperglycaemia. Pract Neurol. 2016 Dec; 16 (6): 493-5.
14. Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008; 358 (19): 1991–2002.
15. Janga KC, Khan T, Khorolsky C, Greenberg S, Persaud P. A rare case of central pontine myelinolysis in overcorrection of hyponatremia with total parenteral nutrition in pregnancy. Case Rep Nephrol. 2015; 2015: 940807.
16. Baouahi H, Doumiri M. Encéphalopathie de Wernicke compliquant l'hyperémèse gravidique et associée à une myélinolyse centropontique [Wernicke encephalopathy complicating hyperemesis gravidarum and associated with pontine myelinolysis]. Pan Afr Med J. 2014 Dec; 19: 340. [French].
17. Safdarian M, Munhoz RP, Aghaei M, Rohani M. Wilson's disease presenting as central pontine myelinolysis. Neurol Sci. 2017 Dec; 38 (12): 2223-5.
18. Ye W, Huang W, Chen L, Yao C, Sheng S, Liu Z,
et al. Pituitary tumor apoplexy associated with extrapontine myelinolysis during pregnancy: a case report. Medicine (Baltimore). 2021 Mar; 100 (10): e25075.
19. Gkalea V, Bachmeyer C, Petrou V, Xirokosta A, Sindos M, Velonakis G,
et al. Asymptomatic Central Pontine Myelinolysis in a Pregnant Woman with Hodgkin Lymphoma. Am J Med. 2023 Apr; 136 (4): e74-e75.
AcknowledgmentsThe present study was supported by the Coordination of Improvement of Higher Education Personnel (CAPES – Portuguese acronym) through the Academic Excellence Program (PROEX – Portuguese acronym).
Author's contributionUrquiza DM and Souza GFA: data analysis and writing and review of the manuscript. Souza ASR and Katz L: study conceptualization and supervision, and manuscript review. Tavares GM: study conceptualization, data collection and analysis, and writing and review of the manuscript. All authors have approved the final version of the article and declared no conflicts of interest.
Received on September 6, 2024
Final version presented on January 14, 2025
Approved on January 15, 2025
Associated Editor: Ricardo Cobucci


 ; Alex Sandro Rolland Souza1,2,3
; Alex Sandro Rolland Souza1,2,3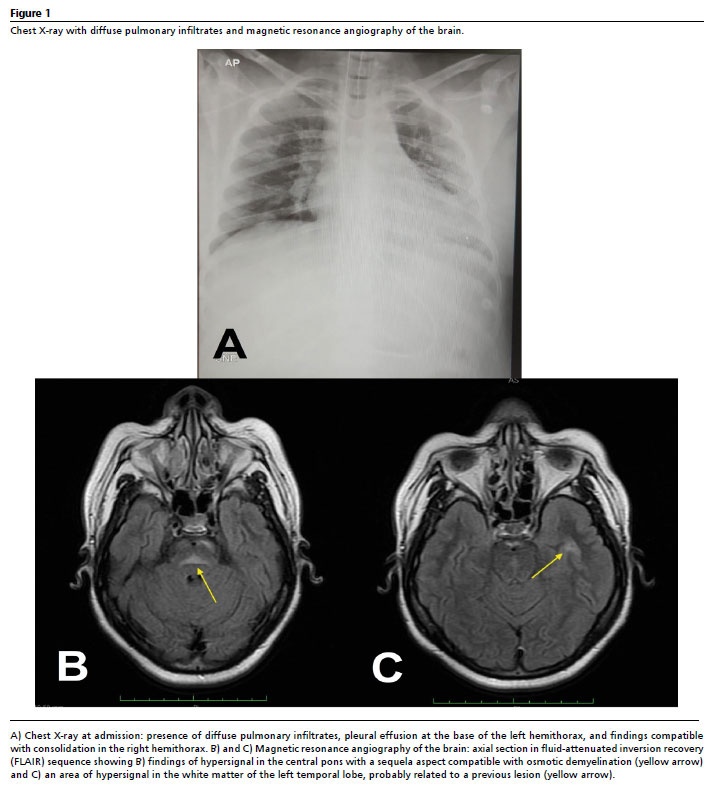






 Ler em português
Ler em português