ABSTRACT
OBJECTIVES: the objective this study was evaluating the prevalence of maternal colonization by Group B beta-hemolytic Streptococcus (GBS) in pregnant women who delivered preterm and its relationship with adverse maternal/perinatal outcomes.
METHODS: we carried out a retrospective cohort study with singleton pregnancies with or without a culture for GBS (vaginal-rectum) who delivered spontaneously <37 weeks of gestation.
RESULTS: the study included 190 pregnant women, 53.1% (101/190) did not undergo culture for GBS and 46.8% (89/101) have done. Among the patients who had a culture, 13.5% (12/89) had positive culture for GBS and 86.5% (77/89) had a negative culture. Pregnant women without GBS culture had higher prevalence of preterm birth (74.3 vs. 59.6%, p=0.031) and lower prevalence of antibiotic prophylaxis (27.7 vs. 56.2%, p<0.001) than pregnant women with GBS culture. Higher prevalence of crystalline penicillin G use was observed in pregnant women with positive culture compared to pregnant women with negative culture for GBS (100 vs. 39%, p<0.0001). There was no significant association between pregnant women with or without a culture for GBS or positive and negative GBS cultures and adverse maternal/perinatal outcomes.
CONCLUSION: No significant association was found between GBS culture or not, GBS positive or negative culture, adequate or inadequate GBS prophylaxis, and the prevalence of adverse maternal/perinatal outcomes.
Keywords:
Group B beta-hemolytic Streptococcus, Screening, Preterm delivery, Antibiotic prophylaxis, Adverse maternal/perinatal outcomes
IntroductionGroup B beta-hemolytic
Streptococcus (GBS or
Streptococcus agalactie) is a bacterium that commonly colonizes the lower genital tract of pregnant women and can cause infection and sepsis in neonates and infants <90 days of age.
1 Perinatal infection occurs by vertical transmission when GBS passes from the vagina into the amniotic fluid after the onset of labor or premature rupture of ovular membranes (PROM).
2 Approximately 50 to 75% of neonates exposed to vaginal GBS become colonized, and 1 to 2% develop early-onset invasive disease.
3 Early-onset neonatal sepsis is the most common manifestation and is characterized by infection manifesting by the 6
th day of life with symptoms including respiratory distress, pneumonia, and meningitis.
4Cultures for screening GBS infection in pregnant women should be obtained by swab of the anal and vaginal areas between 35 and 37 weeks of gestation. The negative predictive value of GBS cultures obtained less than five weeks after delivery is 95 to 98%. Screening and administration of intravenous antibiotic prophylaxis have been associated with a greater than 50% reduction in early-onset neonatal infection. Prophylaxis for GBS with intravenous antibiotics should be given to all pregnant women with a positive vaginal and/or rectal culture for GBS or, if the culture was not obtained in antepartum, with any of the following risk factors: intrapartum fever (>38ºC), preterm birth, PROM for more than 18 hours, previous delivery with neonatal GBS infection, or GBS bacteriuria in the current pregnancy.
5Intrapartum antibiotic prophylaxis is indicated on admission to the hospital for labor or PROM and is continued every four hours until delivery or negative culture is obtained. The antibiotic of choice is crystalline penicillin at a dose of 5,000.000 IU as a loading dose, followed by 2,500.000 IU maintenance intravenously every four hours until delivery. Patients admitted for preterm birth should have a culture for GBS obtained on admission if this was not done during prenatal care.
Pregnant women who undergo successful inhibition of labor should have prophylaxis discontinued and the culture result checked. If the culture is negative, there is no need to restart prophylaxis if labor occurs within the next five weeks. If the time between the last culture and actual labor is more than five weeks, a new culture should be obtained, and prophylaxis discontinued.
6The prevalence of maternal GBS colonization is influenced by several factors, including the gestational age at which the sample was collected, the culture methods used, race, age (the older the woman, the greater the risk of colonization), parity (the lower the parity, the greater the risk of colonization), and socioeconomic status. These variables explain the variable colonization rate of five to 41% described in the literature.
7,8The objective of this study was to evaluate the prevalence of maternal colonization by GBS in pregnant women who delivered preterm and its association with adverse maternal/perinatal outcomes.
MethodsA retrospective cohort study was carried out at
Mário Palmério Hospital Universitário –
Universidade de Uberaba (UNIUBE), Uberaba, Minas Gerais State, Brazil, by analyzing medical records from March 2016 to March 2023. The inclusion criteria were the following: 1) singleton pregnancies followed at the antenatal clinic admitted to the obstetrics unit, with or without a culture for GBS and whose delivery occurred spontaneously <37 weeks of gestation; 2) absence of chromosomal abnormalities or congenital anomalies diagnosed by prenatal ultrasound or in the postnatal period.
The GBS culture was carried out after vaginal and perianal swabs were routinely taken from all the pregnant women at the antenatal clinic between 35 and 37 weeks of gestation. To collect the swab, pregnant women are asked not to have bathed, douched or used any vaginal topical medication on the day of the test and have not had sexual intercourse in the last 24 hours. To collect the swab, the patients are placed in the lithotomy position using two sterile swabs (Biocon
®- Belo Horizonte, Brazil), after consenting. To collect the vaginal sample, the swab is introduced into the introitus, about 2.0 cm, making rotating movements so that it reaches the entire circumference of the vaginal wall. Subsequently, an anal sample was collected by introducing the swab at a distance of 0.5 cm from the anal sphincter, making rotating movements to reach the entire circumference of the region. Immediately after collection, each swab was individually inserted into a tube containing a transport medium called stuart, stored at room temperature until it was sent to the laboratory within a maximum of three days. In the laboratory, the material was inoculated into a specific enrichment medium (Todd Hewitt) that provides essential nutrients for the development of the target microorganism while partially inhibiting other microorganisms in the flora. After 24 hours in this enrichment medium at a temperature of 35 to 37ºC, a manual reading was made to identify and enumerate the growth of GBS.
In the service searched, prophylactic antibiotics are indicated for all pregnant women with a positive culture for GBS who are admitted for induction or management of labor, except those undergoing cesarean section with intact membranes (prophylactic antibiotics are given before skin incision). According to institutional protocol, prophylactic antibiotics are given to all pregnant women with a negative culture ≥five weeks, in labor with PROM for >18 hours. The antibiotic of choice for prophylaxis is crystalline penicillin G at a dose of 5,000.000 IU IV as a starting dose, followed by 2,500.000 IU IV every four hours until delivery. If crystalline penicillin G is unavailable, ampicillin 2.0 grams (IV) is given as a starting dose, followed by 1.0 gram IV every six hours until delivery. In cases of penicillin allergy, clindamycin 900 mg IV is given every eight hours until delivery. In patients undergoing cesarean delivery, cefazolin 2.0 grams IV may also be given as a starting dose, followed by 1.0 gram IV every six hours until delivery. Administration of two doses of any antibiotic within four hours of delivery is considered adequate prophylaxis.
9High-risk pregnancy was considered the following conditions: gestational arterial hypertension, gestational diabetes mellitus, collagen diseases, heart disease, decompensated lung disease, epilepsy, hereditary thrombophilia, antiphospholipid antibody syndrome, chronic kidney disease, thyroid disease, moderate/severe anemia, infection during pregnancy (toxoplasmosis, syphilis, cytomegalovirus, parvovirus, HIV), fetal growth restriction, oligohydramnios, fetal malformations, and chromosomal abnormalities.
To characterize the study population, the following variables were assessed: maternal age, ethnicity, number of pregnancies, number of previous deliveries, weight, height, body mass index (BMI), smoking, pre-existing diseases, gestational age at time of GBS culture, GBS culture result, gestational age at time of hospital admission, preterm birth, PROM, time of PROM, antibiotic prophylaxis for GBS, number of doses of antibiotic prophylaxis for GBS, adequate treatment, type of delivery, gestational age at delivery, birth weight, sex of newborn, APGAR score at the 1
st and 5
th minute.
The following variables were considered adverse maternal/perinatal outcomes: early-onset neonatal sepsis, maternal admission to the intensive care unit (ICU), chorioamnionitis, admission to the neonatal ICU, APGAR score at the 7
th minute <7, early neonatal death (up to 48 hours of life). Early-onset neonatal sepsis was considered to be the presence of laboratory changes such as leukocytes <5,000 or >25,000 cells/mm
3 at birth or >30,000 cells/mm
3 at 12-24 hours of life or ≥21,000 cells/mm
3 within two days of life, increased immature neutrophils, platelets <150,000/mm
3, ratio of immature neutrophils to total neutrophils >0.3, and the presence of signs such as lethargy, irritability, thin pulse, cyanotic extremities, and tachypnea.
10The GPower 3.1 program was used for sample calculation. To assess the association between a positive GBS culture and the presence of early-onset neonatal sepsis and adverse perinatal outcomes, considering an effect size of 0.2, a test power of 80% and a probability of error α=0.05, a total number of 197 patients will be needed.
The data was transferred to an Excel 2010 spreadsheet (Microsoft Corp., Redmond, WA, USA) and then analyzed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA) and Prisma GraphPad 7.0 (GraphPad Software, San Diego, CA, USA). The quantitative variables were initially subjected to the normality test (D'Agostino Pearson). Variables with a normal distribution were presented as means and standard deviations (SD). Variables with a non-normal distribution were presented as median, minimum and maximum values. Categorical variables were described using absolute and percentage frequencies and represented in tables. The Chi-square test was used to study the difference between categorical variables and their proportions. The Mann-Whitney and Student's t-tests were used to study the effect of the group studied on the continuous variables. Binary logistic regression was used to calculate the odds ratio (OR) for the adverse maternal/perinatal outcomes. The significance level for all tests was α=0.05.
The study was approved by the Research Ethics Committee at UNIUBE (CAAE: 52299421.7.0000.5145).
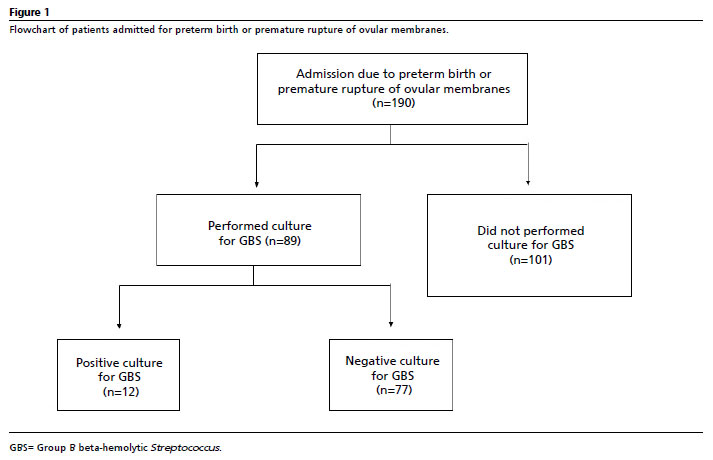
ResultsThe study included 190 pregnant women admitted to the service due to spontaneous preterm birth and/or PROM who delivered at up to 36 weeks and six days of gestation. Among the patients included, 53.1% (101/190) did not undergo culture for GBS and 46.8% (89/101) have done. Among the patients who had a culture, 13.5% (12/89) had positive culture for GBS and 86.5% (77/89) had negative culture (Figure 1).
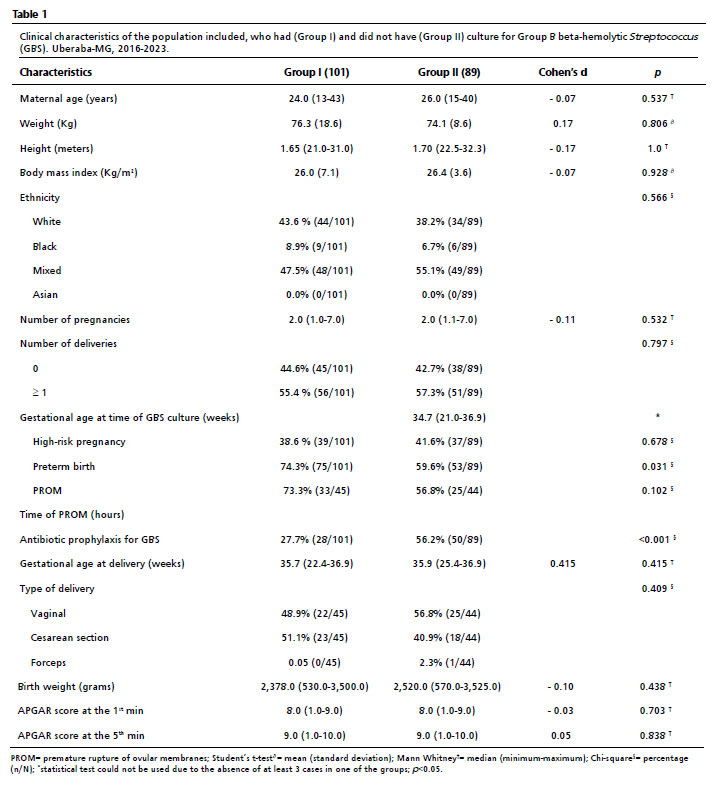
Pregnant women who did not have a GBS culture (Group I) had a higher prevalence of preterm birth (74.3
vs. 59.6%,
p=0.031) and a lower prevalence of antibiotic prophylaxis (27.7
vs 56.2%,
p<0.001) than pregnant women who had a GBS culture (Group II). There was no significant effect or association between the groups and the other variables analyzed (Table 1).
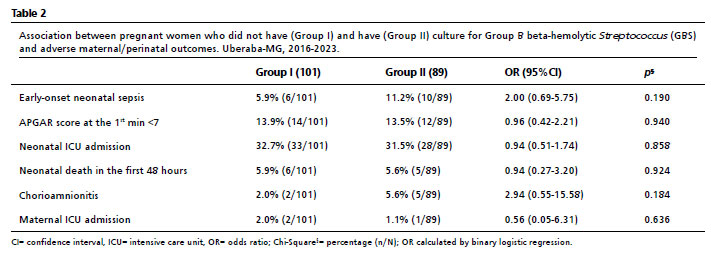
There was no significant association between pregnant women with or without a culture for GBS and the presence of early-onset neonatal sepsis (
p=0.190), APGAR score at the 1
st minute <7 (
p=0.940), neonatal ICU admission (
p=0.856), neonatal death in the first 48 hours (
p=0.924), chorioamnionitis (
p=0.184) and maternal ICU admission (
p=0.636) (Table 2).
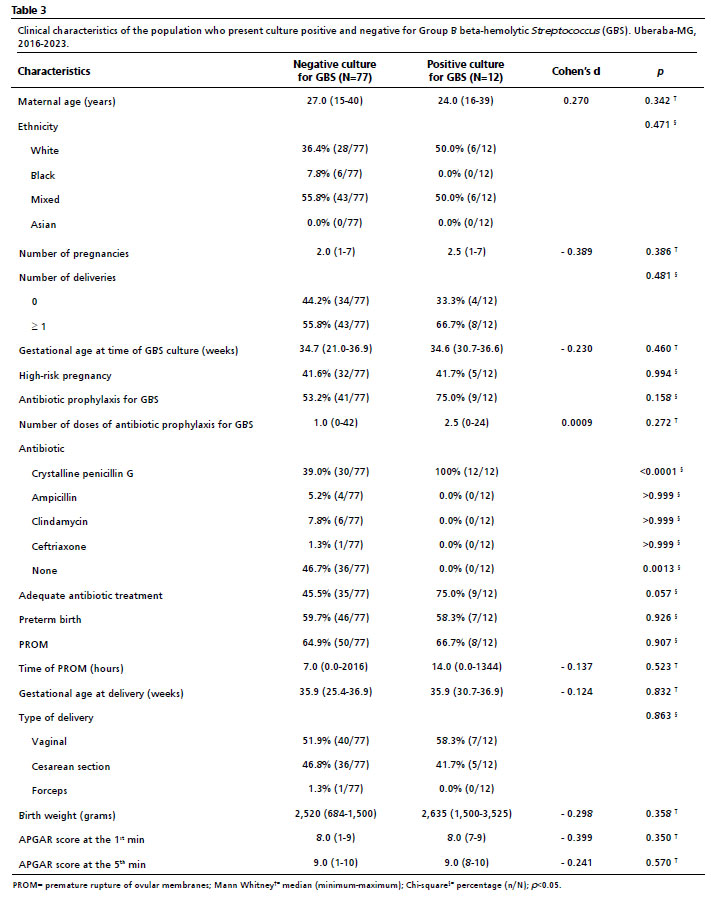
There was no significant association between the presence of positive or negative cultures for GBS and antibiotic prophylaxis (
p=0.272). However, a higher prevalence of crystalline penicillin G use was observed in pregnant women with a positive culture for GBS compared to pregnant women with a negative culture (100
vs 39%,
p<0.0001). There was no significant association or effect between a positive or negative culture for GBS and the other variables (Table 3).
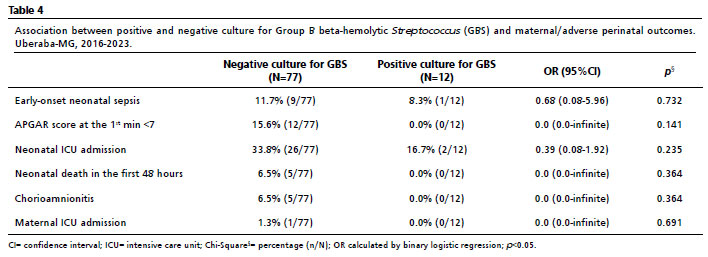
There was no significant association between the presence of positive and negative GBS cultures and the presence of early-onset neonatal sepsis (
p=0.732), APGAR score at the 1
st minute <7 (
p=0.141), neonatal ICU admission (
p=0.235), neonatal death in the first 48 hours (
p=0.364), chorioamnionitis (
p=0.364) and maternal ICU admission (
p=0.691) (Table 4).
Considering all the cases included in the study, 33.7% (64/190) underwent adequate prophylaxis for GBS. No significant association was observed between adequate prophylaxis, inadequate prophylaxis and the prevalence of early-onset neonatal sepsis [12.5 (8/64)
vs 6.3% (8/126),
p=0.171, respectively].
DiscussionIn the present study, there was no significant association between pregnant women with or without a culture for GBS or positive and negative GBS cultures and adverse maternal/perinatal outcomes.
In a systematic review and meta-analysis including 45 studies, the estimated risk ratio for preterm birth with maternal GBS colonization was 1.21 in cohort and cross-sectional studies, and the odds ratio (OR) was 1.85 in case-control studies.
11 In a meta-analysis published in 2022 with 9,778 pregnant Indian women, Ashary
et al.
12 found that the risk of preterm birth was higher (OR=7.9) in women with a positive culture for GBS compared with those without GBS.
In this study, the prevalence of pregnant women who perform culture for GBS between 35 and 37 weeks of gestation was 53.1%. In an Italian study of 2022 that analyzed the regional birth certificate register of the Piedmont Department of Health Policy from 2006 to 2018, following specific recommendations for compliance with international guidelines, the mean proportion of women tested for GBS vaginal-rectal swabs during pregnancy increased from 83.5% in 2006 to 90.7% in 2018, with the largest increase in 2010.
13The rate of positive culture for GBS (vaginal-rectal) in our population was 13.5% (12/89). The positivity of GBS culture varies among different populations and countries. In a study conducted in two cities in Ghana, Africa, the positive culture for GBS varied from 25.5% (51/200) to 28.0% (56/200).
14 In a study of 379 Korean pregnant women, the rate of GBS colonization (vaginal-rectal) was 19.8%.
15 The rate of vaginal colonization by GBS in 200 Pakistani women was 8.5%.
16The prevalence of GBS colonization in 9,778 pregnant women from data of 36 studies (1981 – 2019) was 7.8%.
12 A prevalence of positive culture for GBS (vaginal and/or rectum) in different Brazilian regions ranged from 4.2 to 28.4% between 2008 and 2018.
17 Uberaba is located in the Southwest region of Brazil, has a population of approximately 330,000 inhabitants , and a Municipal Human Development Index (HDI) of 0.772 in 2010, above Brazilian HDI which was 0.699.
18 Even though, the prevalence of positive culture for GBS in our population was higher than the prevalence of positive culture of GBS in other less developed countries as Pakistan and lower than higher developed countries as South Korea. Thus, we believe that not only the human development index is related to the prevalence of positive culture for GBS, but other factors should be evaluated to better understand the GBS colonization of the population in each region.
The present study observed a higher prevalence of crystalline penicillin G use in pregnant women with a positive culture for GBS. The antibiotic of choice for prophylaxis in our service is crystalline penicillin G. If crystalline penicillin G is unavailable, ampicillin and clindamycin are the second and third options, respectively. According to the guidelines of the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists, penicillin, ampicillin, or cefazolin are recommended for prophylaxis of GBS, with clindamycin and vancomycin reserved for cases of significant maternal penicillin allergy.
19 A European consensus conference in Florence, Italy, attended by 16 experts from different countries representing all major scientific societies, established crystalline penicillin G as the first-line agent for antibiotic prophylaxis of GBS colonization.
20 ACOG Committee Opinion recommends that intravenous penicillin should be the preferred agent for intrapartum prophylaxis, with intravenous ampicillin being an acceptable alternative. First-generation cephalosporins are recommended for women who report a penicillin allergy that indicates a low risk of anaphylaxis or is of uncertain severity.
21In this research, the presence of a positive culture for GBS was not associated with early-onset neonatal sepsis and other maternal/adverse perinatal outcomes. In a Malaysian retrospective cohort study between 2015 and 2020, which included 991 neonates from 44 neonatal intensive care units, the incidence of early-onset neonatal sepsis increased from 0.46 to 0.49/1000 live births during this period. GBS was the most common pathogen (388, 39.2%). Multiple logistic regression analysis showed that Indian ethnicity, chorioamnionitis, gestational age ≥37 weeks, female, spontaneous vaginal delivery, instrumental delivery, and surfactant therapy were significantly associated with increased risk of early-onset neonatal sepsis due to GBS.
22 In a Chinese study of 617 pregnant women between 35 and 37 weeks' gestation, the GBS-positive group (560) had a higher incidence of intrauterine infection, postpartum hemorrhage, and fetal distress than the GBS-negative group (57), but similar incidence of PROM, preterm delivery, and meconium-stained amniotic fluid.
23 Gad
et al.,
24 in a retrospective cohort study, evaluated the association between peripartum maternal bacteremia and early neonatal sepsis. Among the 536 maternal blood cultures analyzed, 102 (19.0%) were positive. The most prevalent organisms were GBS (39.2%), followed by
Escherichia coli (14.7%) and anaerobes (10.8%). Maternal GBS infection was associates with increased risk of early neonatal sepsis [OR 6.33 (3.02 to 13.25)].
24 We believe that the lack of statistical differences between the groups is a consequence of the small sample size in the positive culture for GBS.
In the present study, 33.7% of pregnant women with a positive culture for GBS received adequate prophylaxis, but there were no significant statistical differences between adequate and inadequate prophylaxis and the prevalence of early-onset neonatal sepsis. Zhu
et al.
25 prospectively evaluated 16,384 pregnant women and 16,634 neonates between May 1, 2019 and April 30, 2020. They observed that adequate intrapartum antibiotic prophylaxis was a protective factor in neonates of pregnant women with GBS colonization. In a retrospective cohort study conducted at 2016, Bianco
et al.
26 evaluated 902 pregnant women to determine whether complete intrapartum antibiotic prophylaxis for GBS was administered according to the revised Centers for Disease Control and Prevention guidelines. Completely appropriate intrapartum antibiotic prophylaxis for GBS was given to 36.3% of pregnant women, inappropriate prophylaxis was given to 10.4%, and the remaining 45.3% of pregnant women received partially appropriate prophylaxis. Multivariate analysis showed that completely appropriate antibiotic prophylaxis for GBS was significantly more likely in pregnant women with a positive culture at antenatal GBS screening. In our study, we observed a similar rate of appropriate antibiotic prophylaxis for GBS as in the study by Bianco
et al.
26Limitations of our study include that it was a retrospective analysis and we were unable to reach the sample size of 197 patients. However, according to post hoc calculation, the power of our study to evaluate the association between a positive GBS culture and the presence of early-onset neonatal sepsis was 78.7%.
In summary, we did not find significant association between GBS culture or not, GBS positive or negative culture, and adequate or inadequate GBS prophylaxis and the prevalence of adverse maternal/perinatal outcomes in pregnant women who delivered preterm.
References1. Nandyal RR. Update on group B streptococcal infections: perinatal and neonatal periods. J Perinat Neonatal Nurs. 2008; 22 (3): 230-7.
2. Vornhagen J, Adams Waldorf KM, Rajagopal L. Perinatal Group B Streptococcal Infections: Virulence Factors, Immunity, and Prevention Strategies. Trends Microbiol. 2017; 25(11): 919-31.
3. Terry RR, Kelly FW, Gauzer C, Jeitler M. Risk factors for maternal colonization with group B beta-hemolytic streptococci. J Am Osteopath Assoc. 1999; 99 (11): 571-3.
4. Simonsen KA, Anderson-Berry AL, Delair SF, Davies HD. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014; 27 (1): 21-47.
5. Money D, Allen VM; Infectious Diseases Committee. The prevention of early-onset neonatal group B streptococcal disease. J Obstet Gynaecol Can. 2013; 35 (10): 939-48.
6. Apgar BS, Greenberg G, Yen G. Prevention of group B streptococcal disease in the newborn. Am Fam Physician. 2005; 71 (5): 903-10.
7. Jiao J, Wu W, Shen F, Liu Z, Zhou H, Fan G,
et al. Clinical Profile and Risk Factors of Group B Streptococcal Colonization in Mothers from the Eastern District of China. J Trop Med. 2022; 2022: 5236430.
8. Qadi M, AbuTaha A, Al-Shehab R, Sulaiman S, Hamayel A, Hussein A,
et al. Prevalence and Risk Factors of Group B Streptococcus Colonization in Pregnant Women: A Pilot Study in Palestine. Can J Infect Dis Med Microbiol. 2021; 2021: 8686550.
9. Verani JR, McGee L, Schrag SJ; Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC). Prevention of perinatal group B streptococcal disease--revised guidelines from CDC, 2010. MMWR Recomm Rep. 2010; 59 (RR-10): 1-36.
10. Goulart AP, Valle CF, Dal-Pizzol F, Cancelier ACL. Risk factors for early-onset neonatal sepsis in Brazilian public hospital short-title: early-onset neonatal sepsis. Rev Bras Ter Intensiva. 2006; 18(2): 148-53.
11. Bianchi-Jassir F, Seale AC, Kohli-Lynch M, Lawn JE, Baker CJ, Bartlett L,
et al. Preterm Birth Associated With Group B Streptococcus Maternal Colonization Worldwide: Systematic Review and Meta-analyses. Clin Infect Dis. 2017; 65 (Suppl. 2): S133-42.
12. Ashary N, Singh A, Chhabria K, Modi D. Meta-analysis on prevalence of vaginal group B streptococcus colonization and preterm births in India. J Matern Fetal Neonatal Med. 2022; 35(15): 2923-31.
13. Finale E, Spadea T, Mondo L, Arnulfo A, Capuano A, Ghiotti P,
et al. Streptococcus agalactiae in pregnancy and the impact of recommendations on adherence to guidelines: an Italian area-based study. J Matern Fetal Neonatal Med. 2022; 35 (25): 7826-30.
14. Slotved HC, Dayie NTKD, Banini JAN, Frimodt-Møller N. Carriage and serotype distribution of Streptococcus agalactiae in third trimester pregnancy in southern Ghana. BMC Pregnancy Childbirth. 2017; 17 (1): 238.
15. Choi SJ, Kang J, Uh Y. Recent Epidemiological Changes in Group B Streptococcus Among Pregnant Korean Women. Ann Lab Med. 2021; 41 (4): 380-5.
16. Chaudhry BY, Akhtar N, Balouch AH. Vaginal carriage rate of group B Streptococcus in pregnant women and its transmission to neonates. J Ayub Med Coll Abbottabad. 2010; 22 (4): 167-70.
17. Nascimento CS, Santos NFB, Ferreira RCC, Taddei CR. Streptococcus agalactiae in pregnant women in Brazil: prevalence, serotypes, and antibiotic resistance. Braz J Microbiol. 2019; 50 (4): 943-52.
18. United Nations Development Programme. [access in 2013 Jul 29]. Available from:
https://www.undp.org/pt/brazil/idhm-munic%C3%ADpios-201019. Dhudasia MB, Flannery DD, Pfeifer MR, Puopolo KM. Updated Guidance: Prevention and Management of Perinatal Group B Streptococcus Infection. Neoreviews. 2021; 22 (3): e177-88.
20. Di Renzo GC, Melin P, Berardi A, Blennow M, Carbonell-Estrany X, Donzelli GP,
et al. Intrapartum GBS screening and antibiotic prophylaxis: a European consensus conference. J Matern Fetal Neonatal Med. 2015; 28 (7): 766-82.
21. Prevention of Group B Streptococcal Early-Onset Disease in Newborns: ACOG Committee Opinion, Number 797. Obstet Gynecol. 2020; 135 (2): e51-72.
22. Boo NY, Ang EBK, Neoh SH, Ang EL, Chee SC. Early-onset sepsis in Malaysian neonatal intensive care units. Malays J Pathol. 2022; 44 (3): 443-59.
23. Shi CY, Qu SH, Yang L, Yang HX. Detection of maternal colonization of group B streptococcus in late pregnancy by real-time polymerase chain reaction and its effect on perinatal outcome. [Chinese] Zhonghua Fu Chan Ke Za Zhi. 2010; 45 (1): 12-6.
24. Gad A, Alkhdr M, Terkawi R, Alsharif H, Ibrahim M, Amin R, et al. Associations between maternal bacteremia during the peripartum period and early-onset neonatal sepsis: a retrospective cohort study. BMC Pediatr. 2024; 24 (1): 526.
25. Zhu Y, Gao L, Huang ZL, Wu JY, Ni Y, Wang YJ,
et al. Current status of group B Streptococcus infection in neonates: a multicenter prospective study. Zhongguo Dang Dai Er Ke Za Zhi. 2021; 23(9): 889-95.
26. Bianco A, Larosa E, Pileggi C, Pavia M; Collaborative Working Group. Appropriateness of Intrapartum Antibiotic Prophylaxis to Prevent Neonatal Group B Streptococcus Disease. PLoS One. 2016; 11 (11): e0166179.
Authors' contribution: Rezende MC: literature search and medical practices. Rodrigues TP: concept. Freitas APM: data collection or processing. Lopes KS: design. Araujo Júnior E: writing. Peixoto AB: analysis or interpretation. All authors approved the final version of the article and declare no conflicts of interest.
Received on July 8, 2024
Final version presented on October 7, 2024
Approved on October 9, 2024
Associated Editor: Alex Sandro Souza


 ; Thamirys Pereira Rodrigues1
; Thamirys Pereira Rodrigues1