ABSTRACT
OBJECTIVES: to analyze the evolution and inequalities in prenatal care consultations in Pernambuco, according to maternal education level.
METHODS: this is an ecological study of pregnant women who attended seven or more prenatal consultations and resided in Pernambuco between 2011 and 2020, stratified by maternal education level and year of birth. Data were obtained from the Live Birth Information System. Temporal trend analysis was performed using the joinpoint regression method, and patterns of inequality were assessed through absolute measures (difference, ratio), relative measures (concentration index - CIX), and Equiplot-type graphs.
RESULTS: a rising trend in access to seven or more prenatal consultations among women in Pernambuco was observed between 2011 and 2020 (+3.6; p<0.001). Among women with no formal education, prenatal coverage was 47.85%, while for those with more than 12 years of education, it reached 78.15%. The Concentration Index (CIX=0.0979; p<0.001) suggests that 9.79% of prenatal access is concentrated among women with higher education levels.
CONCLUSIONS: despite the expansion of prenatal care in Pernambuco, access remains unequal among women with different levels of education, highlighting maternal education as a marker of health inequities. Strategies need to be adopted to ensure greater equity in prenatal care for more vulnerable pregnant women.
Keywords:
Prenatal care, Educational status, Health inequality indicators, Health status disparities
RESUMO
OBJETIVOS: analisar a evolução e as desigualdades na realização das consultas de pré-natal em Pernambuco segundo escolaridade materna.
MÉTODOS: estudo ecológico das gestantes que realizaram sete e mais consultas de pré-natal residentes em Pernambuco entre 2011 e 2020 segundo as variáveis escolaridade materna e ano do nascimento. Os dados foram obtidos do Sistema de Informações sobre Nascidos Vivos. A análise de tendência temporal foi realizada por meio do método de joinpoint regression e para análise dos padrões de desigualdades foram utilizadas medidas absolutas (diferença, razão), relativa (índice de concentração - CIX) e gráficos do tipo Equiplot.
RESULTADOS: observou-se uma tendência crescente no acesso das mulheres a sete e mais consultas de pré-natal entre 2011 e 2020 em Pernambuco (+3,6; p<0,001). Nas gestantes sem escolaridade, a cobertura pré-natal foi de 47,85%, enquanto entre aquelas com mais de 12 anos de estudo, chegou a 78,15%. O Índice de Concentração (CIX=0,0979; p<0,001) sugere que 9,79% do acesso ao pré-natal concentra-se nas mulheres com maior escolaridade.
CONCLUSÕES: apesar da expansão do pré-natal em Pernambuco, o acesso é desigual entre mulheres com diferentes níveis de escolarização, evidenciando a escolaridade materna como um marcador de iniquidades em saúde. É preciso adotar estratégias para garantir maior equidade no atendimento às gestantes mais vulneráveis.
Palavras-chave:
Cuidado pré-natal, Escolaridade, Indicadores de desigualdade em saúde, Disparidades nos níveis de saúde
IntroductionThe health of women and children is characterized as an important subject in the Public Health area, demonstrating indicators that reflect the life conditions of the population. In this context, prenatal care is composed of actions and services focused on the admission and follow-up of pregnant women, contributing to the improvement of mother and child indicators and reducing the negative outcomes related to pregnancy and birth.
1,2In Brazil, between 2000 and 2015, there was a significant increase in the access of women to prenatal care, from 46.0% to 66.9%.
3 The Unified Health System (SUS – Portuguese acronym) has been prioritizing the development of strategies for the expansion and improvement of access to prenatal care, with emphasis on the implementation of the Stork Network and the Program of Humanization of Prenatal and Birth (PHPN – Portuguese acronym).
4 The Stork Network initiative, launched by the Ministry of Health in 2011, considers the execution of seven or more prenatal consultations as a parameter of quality.
5However, in spite of the improvements on the mother and child health area, there are inequalities in the access to prenatal care within Brazilian women. Historically, the national territory is marked by social inequities that influence the access of the population to healthcare services. With regard to prenatal care, geographic and socioeconomic conditions are related to the access and quality of prenatal.
3Concerning inequalities in the children's health area, the "inverse equity" principle is used to approach social inequities in healthcare. According to this principle, public policies favors initially more privileged socioeconomic groups, and posteriorly, those less privileged. Thus, healthcare inequalities are expanded and this generates impact on the indicators related to the coverage, morbidity and mortality.
6In this scenario, maternal schooling is considered an important marker to assess the life conditions of the female population. Pregnant women with less years of schooling demonstrate a higher concentration of risk factors and negative outcomes. Accordingly, maternal schooling may be used as a parameter to identify more vulnerable population groups, measuring healthcare inequalities.
7,8The analysis of the evolution of access of pregnant women to prenatal care is a strategy to the identification of social inequities, guiding the planning of public policies. The measurement of healthcare inequalities regarding pregnant women who had at least seven consultations, having schooling as a marker, may contribute to the development of policies focused on the reduction of mother and child mortality and the promotion of health equity.
9Therefore, the present study aimed to assess the temporal evolution and the inequalities in the execution of prenatal consultations in Pernambuco from 2011 and 2020, according to maternal schooling.
MethodsMixed ecological study (temporal series and inequalities) based on aggregated data of live births and pregnant women who had, at least, seven prenatal consultations, residing in the state of Pernambuco and registered in the Live Birth Information System (SINASC – Portuguese acronym) between 2011 and 2021.
The area of influence of the study was the state of Pernambuco, located in the Northeast Region of Brazil, with 98,067,877 km
2 of area and an estimated population of 9,674,793 inhabitants in 2021. Pernambuco is considered the seventh most populous state in the country, composed of 184 municipalities and a state district (Fernando de Noronha), with 12 Health Regions.
10The study adopted the following exploratory variables: I – dependent variable: Proportion of live births born to pregnant women who attended to seven or more prenatal consultations; II – independent variables: Maternal schooling (no schooling, one to three years of schooling, four to six, eight to 11 and 12 or more) and year of birth (2011 to 2020). As an exclusion criterion, we excluded data from mothers that performed less than seven prenatal consultations and those who did not inform the level of schooling.
We calculated the proportion of live births of pregnant women who performed seven and more prenatal consultations for each group of maternal schooling and year, considering, in the numerator, the number of live births of pregnant women who performed at least seven prenatal consultations in the year and in the denominator, the total number of live births per year, multiplied by 100.
Data were obtained with the online interface of the Department of Informatics of the SUS (DATASUS – Portuguese acronym), collecting information from the SINASC, which is based on the document Declaration of Live Births (DNV – Portuguese acronym), with compulsory fulfillment in the entire national territory.
11For the temporal trend analysis, we used the joinpoint regression method, which enables the analysis of both significant trends and inflection points, known as joinpoints; or, still, moments in which a significant alteration of the trends occurs over time. This method allows to test whether a temporal line, of multiple segments, is statistically adequate to perform the description of the temporal evolution of data, compared to a straight line or one with less segments.
12We estimated the APCs (Annual Percent Change) and the AAPC (Average Annual Percent Change) for the assessed period, with the respective 95% confidence intervals (CI) and the statistical significance (
p). The regression analyses were performed with the statistical software Joinpoint Trend analysis version 4.9.0.1.
For the mensuration of inequalities of access to seven or more prenatal consultation, we applied the simple and complex measures, namely: I –
Difference: The difference of indicator values between the reference group (12 years and more) and the comparison group (no schooling); II –
Ratio: Quotient of indicator values between the reference group (12 years and more) and the comparison group (no schooling); III –
Concentration Index (CIX): A relative measurement of inequality for ordered stratifiers based on the Lorenz curve.
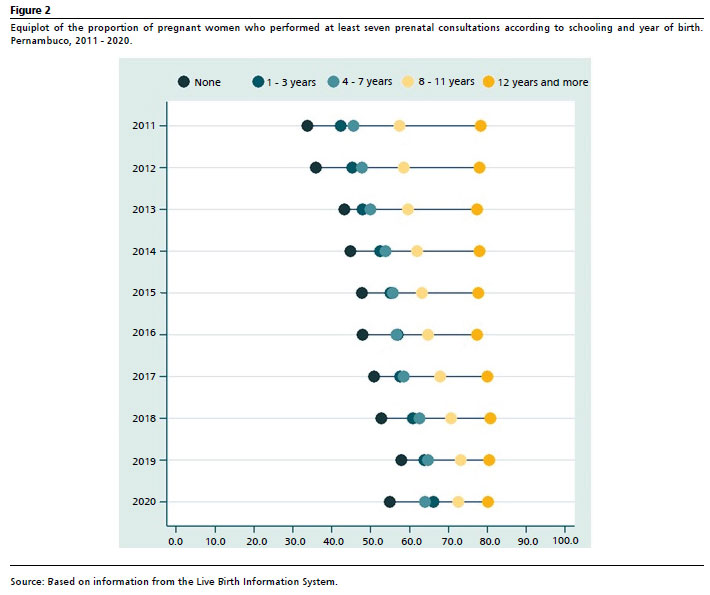
13Moreover, in order to identify inequality standards, the proportion of births to mothers who performed seven or more prenatal consultations was stratified by group of maternal schooling in each year. The equiplot figure, conceived by the International Center for Equity in Health, aiming to assess health inequalities.
14For data analysis and processing, we used the statistical pack of the Stata software, version 16.1.
The study was developed by means of secondary data, of public domain and available free of charge, assuring the confidentiality of personal information. Therefore, according to the Resolution of the National Health Council number 510/2016, the submission to the Research Ethics Committee was not necessary.
ResultsBetween 2011 and 2020, the percentage of pregnant women that attended seven and more prenatal consultation went from 54.2% to 71.8%, a 32.4% increase, with differences by level of maternal schooling. The less prenatal coverage was observed within pregnant women without schooling in the entire period (47.0%), whilst for those women with 12 years of schooling or more, we observed higher coverage (78.8%) (Figure 1).
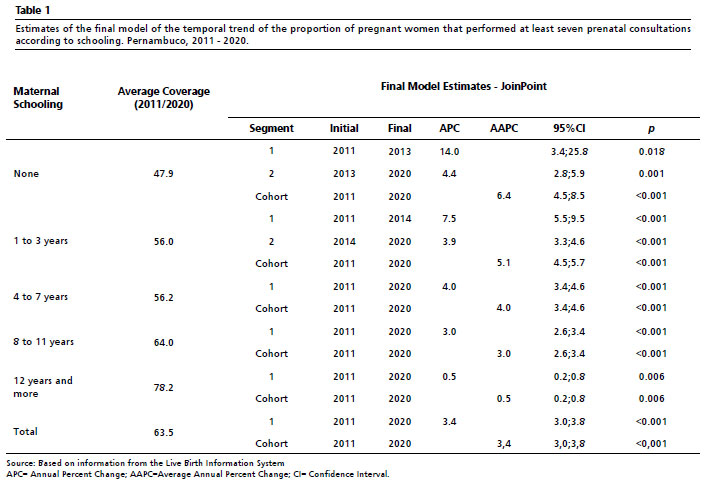
The temporal analysis demonstrated a significant trend in the increase of the attendance of seven or more prenatal consultations in Pernambuco during the assessed period, in all levels of maternal schooling, however in different levels (Table 1).
Within pregnant women without schooling, although we observed the lowest average coverage (47.9%), it was also observed the most expressive increase, with an APC of 14.0 between 2011 and 2013 (
p=0.018), maintaining significant in the period between 2013 and 2020 (APC = 4.4,
p= 0.001) (Table 1).
We also observed a significant growth in the percentage of, at least, seven prenatal consultations in pregnant women with one to three years of schooling, with an APC increase of 7.5 (
p<0.001) between the years 2011 and 2014 and 3.9 (
p<0.001) in the period between 2014 and 2020. On the other hand, the pregnant women with 12 and more years of schooling, although they demonstrate higher average coverage of seven and more prenatal consultations in the period (78.2%), they also demonstrated the lowest annual increase (APC=0.5,
p=0.006) (Table 1). In Figure 2, it is possible to verify the standard of inequalities on the proportion of pregnant women that performed at least seven prenatal consultations according to maternal schooling and year of birth, in which the highest levels of inequalities of the first year of the study period (2011 and 2012) are observed, with a decrease on the inequality levels from 2013. However, in the year 2020, we observed a discrete increase of inequalities between groups of maternal schooling. Data suggest, also, a standard of inequality nominated bottom inequality, or marginal exclusion.
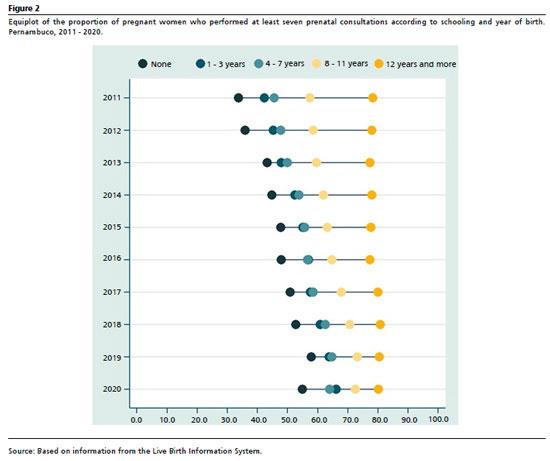
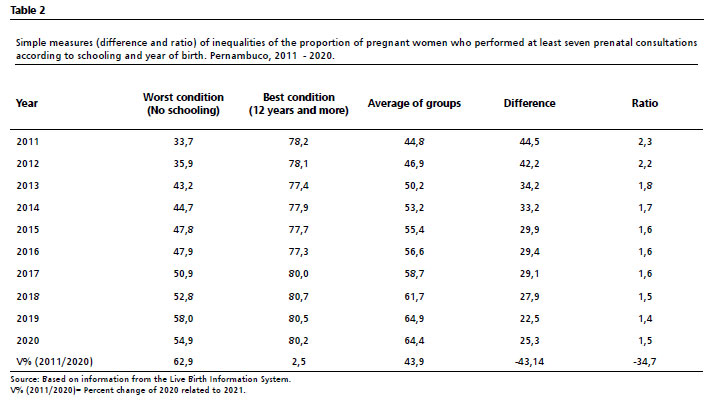
Table 2 demonstrates measurements of inequality for the proportion of pregnant women who performed at least seven prenatal consultations according to schooling and year of birth. We observe that the absolute difference of prenatal coverage between the group with highest schooling compared to that with lowest schooling, in the average of the period, was 31.8, however with a decrease over the years, going from 44.5 in 2011 to 22.5 in 2019 (Table 2).
In the year 2011, we observed that the inequality between the pregnant women without schooling was 2.3 times higher compared to those with 12 years of schooling or more, and a reduction over the years, reaching the value of 1.4 in 2019, a decrease of 39.1%. There was a discrete increase in all inequality measurements in the year 2020 (Table 2).
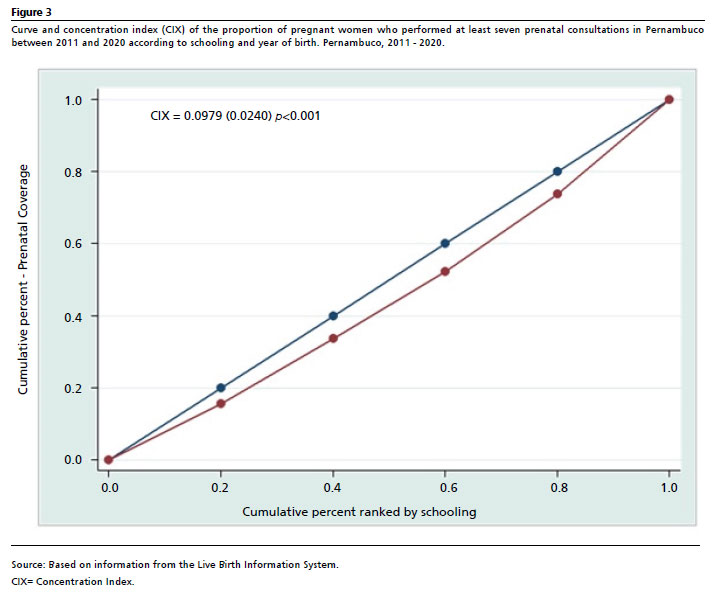
Such inequalities are also reassured by the concentration index (CIX), whose values (0.0979;
p<0.001) suggest that the proportion of at least seven prenatal consultations is concentrated in 9.79% of women with higher levels of schooling (Figure 3).
DiscussionThe results of the present study indicated a significantly increasing trend in the access of women to prenatal care, however, the trend demonstrates different paces of increase and magnitude between groups of maternal schooling. The findings point to the existence of a standard of inequality among pregnant women, in which the highest level of schooling was identified as a enhancing factor of the access, that is, more years of schooling are associated with a higher proportion of pregnant women who attended the recommended number of prenatal consultations.
The development of studies that aim to measure the inequalities attempts to identify the social inequalities, and posteriorly, to explain the causality. Beyond statistical procedures, the measurement of inequalities implies moral values, associated with social justice. The monitoring of health inequalities aims to subsidize the creation of public policies focused on the reduction of social inequalities and for the social justice promotion.
13,15According to Barros and Victoria,
16 the health system has been searching for the implementation of the principle of equity, and due to it, the measurement of social inequities in healthcare is a strategic instrument. The authors indicate the existence of several health indicators that collaborate in the assessment of the socioeconomic position of the population. In the field of mother and child health, maternal schooling is identified as one of the main indicators for the measurement and interpretation of social inequalities.
The study indicates a significant increasing trend in the coverage of prenatal consultation in the state of Pernambuco in all groups of maternal schooling, however, with differing markers between groups. These findings corroborate the results of the national study of Mallman
et al.
3 Although there is a trend of universalization of prenatal coverage in Brazil, there are still sociodemographic and regional inequities in specific aspects of care, in which pregnant women from the North, Northeast and Midwest regions, besides black, indigenous, young, low schooling women, as well as those without partners, demonstrate higher risk of having inadequate prenatal care.
17Studies demonstrate that, generally, the female population with higher degrees of schooling presents better socioeconomic conditions, a fact that may influence the search for healthcare. Moreover, this population has broader access to knowledge concerning their reproductive rights, and consequently, perform the adequate number of prenatal consultations.
3,7Still on the expansion of prenatal coverage in Pernambuco, it is worth highlighting the adherence of the state, in 2012, to the Stork Network strategy, which aimed to contribute to the improvement of the prenatal care in the state and to the increase of the allocation of resources focused on the care provided to pregnant women.
17 This way, the process of implementation of the Stork Network in the state may have contributed to the improvement of the access to prenatal care.
A study carried out with the objective of describing indicators of the Program of Improvement of Access and Quality of Basic Care (PMAQ-AB – Portuguese acronym), which refer to prenatal care quality, identified an increase in the access of women to services. However, it observed the persistence of healthcare inequalities such as regional and socioeconomic disparities, in which pregnant women residing in the Southeast Region and with higher income presented a significantly higher coverage.
18Another relevant aspect observed in this study was that, in spite of the high inequalities between the strata of pregnant women by maternal schooling over the entire assessed period, the magnitude of these disparities, expressed more objectively, in simple measures (difference and ration), decreased between 2011 and 2019. In the year 2020, however, the prenatal care coverage presented a discrete reduction, besides a slight increase of inequalities observed.
Nevertheless, it is worth highlighting the onset of COVID-19 pandemic in Brazil, in 2020, which interfered in the access of the population to health services.
19 According to Chisini
et al.,
20 during the year 2020, the COVID-19 pandemic affected the reduction of the execution of procedures carried out at Primary Healthcare (APS – Portuguese acronym), and prenatal care was one of the services affected in Brazilian municipalities.
This study demonstrates that pregnant women with higher schooling over the period present an increase with regard to the prenatal coverage at first, and only posteriorly, the coverage of pregnant women with less schooling advances. These findings reveal the inverse equity principle, according to what Victoria
et al.
6 expose, in which public policies, when implemented, benefit initially the more privileged socioeconomic strata, and only posteriorly reach the less privileged.
6With regard to the improvements and increase in the prenatal coverage, the APS is the strategic service for mother and child care, being a reference for prenatal care.
21 However, in the current context, SUS is facing a progressive dismantling process, characterized, mainly, by the adoption of fiscal austerity measures, being the APS one of the main services affected.
22 According to Paes-Sousa
et al.
23 the fiscal austerity policies lead to negative outcomes to the population and more vulnerable groups, as occurred with indicators related to infant mortality. According to the authors, Brazil is being characterized by several news related to a setback in healthcare, such as the decrease of vaccine coverage and risk of measles outbreak, indicating that the reduction of investments in healthcare is observed mainly in the APS.
Furthermore, Silva
et al.
24 affirm that the implementation of austerity measures, such as cuts in social programs and health services are associated with an increase in infant mortality, and to an aggravation of health inequalities. The research revealed that regions that challenged harsh fiscal adjustments experienced a decrease of quality in health services and a reduction on the access to essential care, which contributed to the increase of infant mortality rates and other negative health indicators within the less privileged population. This study reinforces the need for more balanced policies that protect social services and promote health equity.
Within the limitations of this research, we highlight potential biases related to the quality of information, since this research was based on secondary data. Furthermore, the object of the study was the descriptive analysis of the evolution of access to prenatal care and inequalities in healthcare, without the intention of elucidating causality relationships. This aspect may demand, in further studies, the use of other methodological approaches for a deepening of the subject.
Finally, in spite of the increasing trend of prenatal care coverage, the results of the present study found a persistence of social inequalities, expressed here by the levels of maternal schooling. According to Guimarães
et al.,
21 even though the health investments are not able to revert negative social indicators, the assurance of universal and equitable access to pregnant women may collaborate with the reduction of inequalities, especially for more vulnerable women who need public prenatal care service.
21 Therefore, we highlight the need for strengthening of public policies that consider social determinants in healthcare, aiming to overcome the persistent social inequalities, and consequently, to actualize the guarantee of the equity principle in the SUS. This study advances when it combines the analysis of temporal trend of prenatal consultations coverage with an approach of measurement of inequalities in mother and child healthcare. In a country such as Brazil, specifically in the context of Pernambuco, these inequalities represent a persistent challenge, demanding in-depth debates to base the formulation of effective public policies.
Authors' contribution: Lis DOA: Conceptualization (Equality); Data Curation (equal); Formal Analysis(equal); Research (equal); Methodology (Equality); Project management (Equal); Resources (equal); Software (equal); Supervision (equal); Validation (Equal); Visualization (Equal); Writing – original draft (equal); Writing – review and editing (Equal).
Silva MTA: Supervision (Support); Writing – review and editing (support).
Maia LTS: Methodology (Equality); Software (equal); Supervision (Leader); Writing – review and editing (leader).
All authors approved the final version of the article and declared no conflicts of interest.
References1. Martins IPM, Nakamura CY, Carvalho DR. Variáveis associadas à mortalidade materna e infantil: uma revisão integrativa. Rev Atenção Saúde. 2020; 18 (64): 145-65.
2. Marques BL, Tomasi YT, Saraiva SS, Boing AF, Geremia DS. Orientações às gestantes no pré-natal: a importância do cuidado compartilhado na atenção primária em saúde. Esc Anna Nery. 2021; 25 (1): e20200098.
3. Mallmann MB, Boing AF, Tomasi YT, Anjos JC, Boing AC. Evolução das desigualdades socioeconômicas na realização de consultas de pré-natal entre parturientes brasileiras: análise do período 2000-2015. Epidemiol Serv Saúde. 2018; 27 (4): e2018022.
4. Mario DN, Rigo L, Boclin KLS, Malvestio LMM, Anziliero D, Horta BL,
et al. Qualidade do pré-natal no Brasil: Pesquisa Nacional de Saúde 2013. Ciênc Saúde Colet. 2019; 24 (3): 1223-32.
5. Ministério da Saúde (BR). Portaria nº 1.459, de 24 de Junho de 2011. Institui, no âmbito do Sistema Único de Saúde – SUS – a Rede Cegonha. [access in 2023 Ago 20]. Available from:
http://https://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt1459_24_06_2011.html6. Victoria CG, Vaughan JP, Barros FC, Silva AC, Tomasi E. Explaining trends in inequities: evidence from Brazilian child health studies. Lancet. 2000; 356 (9235): 1093-8.
7. Silvestrin S, Buriol VCS, Silva CH, Goldani MZ. Avaliação da incompletude da variável escolaridade materna nos registros das Declarações de Nascidos Vivos nas capitais brasileiras – 1996 a 2013. Cad Saúde Pública. 2018; 34 (2): e00039217.
8. Fonseca SC, Flores PVG, Camargo KR, Pinheiro RS, Coeli CM. Escolaridade e idade materna: desigualdades no óbito neonatal. Rev Saúde Pública. 2017; 51: 94.
9. Esposti CDD, Santos-Neto ET, Oliveira AE, Travassos C, Pinheiro RS. Desigualdades sociais e geográficas no desempenho da assistência pré-natal de uma região metropolitana do Brasil. Ciênc Saúde Coletiva. 2020; 25 (5): 1735-49.
10. Instituto Brasileiro de Geografia e Estatística (IBGE). Cidades e Estados. [
online]. 2022. [access in 2022 Mar 20]. Available from:
https://www.ibge.gov.br/cidades-e-estados/pe.html11. Ministério da Saúde (BR). Fundação Nacional de Saúde (FUNASA). Manual de instruções para o preenchimento da Declaração de Nascido Vivo. Brasília (DF): FUNASA; 2001. [access in 2022 Mar 20]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/funasa/declaracao_nasc_vivo.pdf12. National Cancer Institute. Joinpoint Trend Analysis Software. [
Internet]. U.S Department of Health & Human Services; 2022. [access in 2022 Abr 22]. Available from:
https://surveillance.cancer.gov/joinpoint/13. Medeiros M. Medidas de desigualdade e pobreza. Brasília (DF): Instituto de Pesquisa Econômica Aplicada (IPEA); 2012. [access in 2024 Set 15]. Available from:
https://econpolrg.com/wp-content/uploads/2013/05/medeiros_2012_medidas_de_desigualdade_e_pobreza.pdf14. International Center for Equity in Health. Equiplot. 2022. [
Internet]. [access in 2022 Mar 29]. Available from:
https://www.equidade.org/equiplot15. Silva ICM, Restrepo-Mendez MC, Costa JC, Ewerlin F, Hellwing F, Ferreira LZ,
et al. Mensuração de desigualdades sociais em saúde: conceitos e abordagens metodológicas no contexto brasileiro. Epidemiol Serv Saúde. 2018; 27 (1): e000100017.
16. Barros AJD, Victora CG. Measuring Coverage in MNCH: Determining and Interpreting Inequalities in Coverage of Maternal, Newborn, and Child Health Interventions. PLOS Med. 2013; 10 (5): e1001390.
17. Ministério da Saúde (BR). Portaria nº 1.498, de 12 de julho de 2012. Aprova Etapa II do Plano de Ação da Rede Cegonha do Estado de Pernambuco e aloca recursos financeiros para sua implementação. 2012. [access in 2022 Mar 22]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2012/prt1498_12_07_2012.html18. Domingues RMSM, Dias MA, Nakamura-Pereira M, Torres JA, D'Orsi E, Pereira APE,
et al. Adequação da assistência pré-natal segundo as características maternas no Brasil. Rev Panam Salud Pública. 2015; 37: 140-7.
19. Albuquerque MV, Ribeiro LHL. Desigualdade, situação geográfica e sentidos da ação na pandemia da COVID-19 no Brasil. Cad Saúde Pública. 2020; 36 (12): e00208720.
20. Chisini LA, Castilhos ED, Costa FS, D'Avila OP. Impact of the COVID-19 pandemic on prenatal, diabetes and medical appointments in the Brazilian National Health System. Rev Bras Epidemiol. 2021; 24: e210013.
21. Guimarães WS, Parente RCP, Guimarães TLF, Garnelo L. Acesso e qualidade da atenção pré-natal na Estratégia Saúde da Família: infraestrutura, cuidado e gestão. Cad Saúde Pública. 2018; 34 (5): e00110417.
22. Morosini MVGC, Fonseca AF. Revisão da Política Nacional de Atenção Básica numa hora dessas? Cad Saúde Pública. 2017; 33 (1): e00206316.
23. Paes-Sousa R, Rasella D, Carepa-Sousa J. Política econômica e saúde pública: equilíbrio fiscal e bem-estar da população. Saúde Debate. 2018; 42 (3): 172-82.
24. Silva JA, Costa LM, Pereira RF. The impact of fiscal austerity on child mortality and health inequalities: a regional analysis. J Public Health Policy. 2024; 45 (2): 123-39.
Received on July 24, 2023
Final version presented on October 21, 2024
Approved on November 6, 2024
Associated Editor: Aurélio Costa


 ; Maria Tatiane Alves da Silva2
; Maria Tatiane Alves da Silva2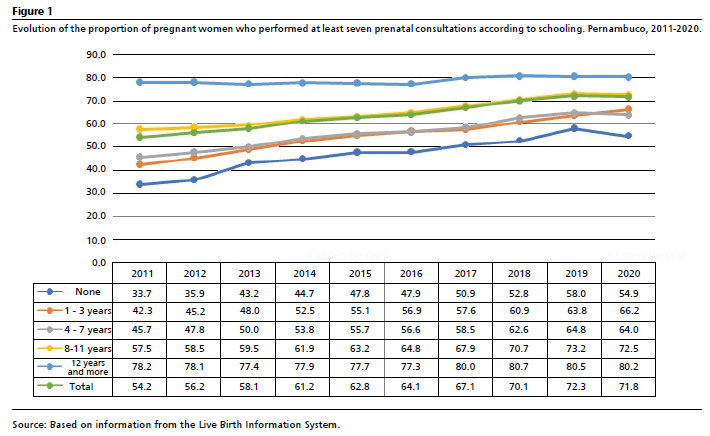






 Ler em português
Ler em português