ABSTRACT
OBJECTIVES: to analyze the temporal trend in early neonatal mortality among adolescent mothers in Brazil and macroregions between 2000 and 2020.
METHODS: a mixed ecological study, using secondary data publicly available from the Live Birth Information System and the Mortality Information System, from which information was consulted on children born in Brazil, according to macro-region, between 2000 and 2020, descendants of adolescents. Infant mortality rates were calculated for Brazil and its macroregions for each year analyzed. Temporal analysis was performed using the Joinpoint Regression Model.
RESULTS: we observed 101,508 early neonatal deaths. The Northeast region had the highest number of early neonatal deaths (37,919). The temporal trend between 2000 and 2020 in the early neonatal mortality rate among children of adolescent mothers in Brazil showed a decreasing pattern, presenting an average variation for the period (AAPC, Average Annual Percent Change) of -0.90; p<0.001. The greatest decrease was observed in the Southern (AAPC = -2.23; p<0.001) and the lowest in the North, with a general stationary temporal trend (APC = -2.64; p<0.001).
CONCLUSION: the findings showed a decreasing temporal trend in the early neonatal mortality rate among children of adolescent mothers from 2000 to 2020 in Brazil. The greatest reduction was observed in the South, while the North presented a general stationary temporal trend.
Keywords:
Early neonatal mortality, Pregnancy in adolescence, Time series studies, Linear models, Health Inequality monitoring
RESUMO
OBJETIVOS: analisara tendência temporal da mortalidade neonatal precoce entre mães adolescentes no Brasil e regiões, entre 2000 e 2020.
MÉTODOS: estudo ecológico misto, que utilizou dados secundários de acesso público do Sistema de Informações sobre Nascidos Vivos e do Sistema de Informações sobre Mortalidade, dos quais foram consultadas informações sobre crianças nascidas no Brasil, segundo macrorregião, entre 2000 e 2020, descendentes de adolescentes. As taxas de mortalidade infantil foram calculadas para o Brasil e macrorregiões por ano analisado. Na análise temporal aplicou-se o modelo de regressão por pontos de inflexão.
RESULTADOS: incluíram-se101.508 óbitos neonatais precoces. Os óbitos neonatais precoces foram mais numerosos no Nordeste (37.919). A tendência temporal da taxa de mortalidade neonatal precoce no período estudadono Brasil demonstrou padrão decrescente, com variação média do período (AAPC, Average Annual Percent Change) igual a -0,90; p<0,001. A maior tendência de diminuição ocorreu na região Sul (AAPC = -2,23; p<0,001) e a menor no Norte, com tendência temporal geral estacionária (APC = -2,64; p<0,001).
CONCLUSÃO: os achados mostraram uma tendência temporal decrescente da taxa de mortalidade neonatal precoce entre filhos de mães adolescentes no Brasil, no período de 2000 a 2020. A maior redução foi observada na região Sul, enquanto o Norte apresentou uma tendência temporal geral estacionária.
Palavras-chave:
Mortalidade neonatal precoce, Gravidez na adolescência, Estudos de séries temporais, Modelos lineares, Monitoramento das desigualdades em saúde
IntroductionAdolescent pregnancy is a global problem, which may lead to intergenerational cycles of poverty and negative outcomes for newborns.
1 According to estimates of the World Health Organization in 2020, approximately 21 million girls aged between 15 and 19 years become pregnant and about 12 million give birth, each year.
2 Considering the age range of 10 to 14 years, the number is approximately 780 thousand births per year. Most births to adolescent mothers in the world – 95% - occur in developing countries, such as Brazil.
1,2The occurrence of adolescent pregnancy seems to be related to women with lower socioeconomic level and domestic violence (sexual and/or physical).
1,3 Still, it is not uncommon that adolescent pregnancy occurs in an intergenerational standard in which pregnant adolescents are daughters of young mothers that faced social, financial, medical, educational and employment difficulties.
4,5 The stigmatization leads to delays in pregnancy diagnosis and prenatal care. Moreover, adolescents in general possess less psychosocial support than adult women do, in addition, the social disapproval caused by early pregnancy may affect the attendance to prenatal consultations.
6This context leads to maternal and neonatal complications, since adolescent pregnancy is associated with an increased risk of preterm birth, low birth weight, eclampsia, anemia, pregnancy hypertensive disorders, chlamydia and gonorrhea infections and maternal and infant morbidity.
7 Adolescent pregnancy is also related to higher occurrence to fetal growth restriction, premature rupture of membranes, perineal lacerations, episiotomies, Apgar index under seven points in the first and fifth minutes of life and higher risk of hospitalization in intensive care units.
8In order to analyze infant deaths, considering its classification is necessary. Infant mortality refers to deaths of infants under one year of life, subdivided into neonatal mortality (deaths from zero to 27 days of life) and post-neonatal mortality (deaths from 27 to 364 days of life). Neonatal mortality is also divided into two periods, early neonatal (zero to six days of life) and late neonatal (seven to 27 days of life). Nevertheless, neonatal mortality, mainly early neonatal mortality, is the main component of infant deaths since the 1990 decade, corresponding to approximately 70% of the current infant mortality.
9,10The assessment of early neonatal mortality rate associated with adolescent pregnancy is necessary, since it reflects regional socioeconomic conditions, as well as the quality of assistance in prenatal care, delivery, birth and to the newborn.
11 The analysis of the temporal behavior of early neonatal deaths is a useful tool for its assessment, being capable to help measures of public health management and the targeting of assistance public policies. We highlight, thus, the importance of surveys that comprehend the assistance dynamics of adolescent mothers in Brazil and regions of the country. The present study aimed to analyze the temporal trend of early neonatal mortality within adolescent mothers in Brazil and its regions, between 2000 and 2020.
MethodsEcological study with mixed methods, using secondary data of public access available at the Department of Informatics of the Unified Health System (DATASUS – Portuguese acronym). For the consultation of data, performed in February 6, 2023, collected at the Mortality Information System (SIM – Portuguese acronym) and Live Birth Information System (Sinasc – Portuguese acronym), early neonatal deaths were defined as those that occurred in infants between zero to six days of life. Firstly, we selected information on early neonatal deaths per residence in Brazil, of children of young women aged between ten and 19 years, present at SIM. At the same time, data concerning live births in Brazil according to macroregion, between 2000 and 2020, born to mothers with established age, were consulted at Sinasc.
Data were initially tabulated in the Microsoft Excel 2016 software. The analyses were stratified according to the regions of the country: North, Northeast, South, Southeast and Midwest. The variables explored from SIM were analyzed with simple descriptive statistics (absolute and relative frequency) and allocated in three groups: characteristics related to mothers, characteristics related to newborns and characteristics related to birth. In the first group, related to mothers, we categorized the age range (ten to 14 years and 15 to 19 years) and maternal schooling, by years of schooling. In the group related to the newborn, we assessed sex and birth weight. With regard to birth, we clustered data concerning type of gestation (if single, double or triple), way of delivery and gestational age at the moment of birth.
Missing data were registered as “ignored” at the end of each table and were not used in the statistical analysis.
The infant mortality rates, in temporal trends, were calculated for Brazil and its macroregions for each analyzed year, with data consulted at SIM and Sinasc, according to the formula below.
The temporal analysis was performed with the application of the Joinpoint Regression Model. The model analyzed whether a line with multiple segments were more adequate to explain the temporal behavior of data grouping compared to a straight line or with fewer segments. Accordingly, the trend of each indicator is classified into stationary, increasing or decreasing according to the slope of the regression line. With this method, we calculated the Annual Percent Change (APC) and the Average Annual Percent Change (AAPC).
12In the statistical analysis, we adopted the following parameters: i) minimum of zero joins, ii) maximum of four joins, iii) selection of the model by the Monte Carlo computational test (n= 4499 permutations), iv) method of autocorrelation of errors based on the date, v) 95% confidence interval (CI95%) and vi) 5% significance level. Such analyses were performed with the Joinpoint regression program (version 4.9.0.1, National Cancer Institute, Bethesda, MD, US) relating the early neonatal mortality rate within adolescent mothers (dependent variable) to year (independent variable).
Since we used public domain data with aggregate information that does not allow individual identification, it was not necessary to submit the research for the approval of the Research Ethics Committee, according to the resolution 466/12 of the National Council of Research Ethics.
ResultsWith regard to the characteristics of early neonatal deaths of children of adolescent mothers: 101,508 early neonatal deaths were included in the present study. The Northeast region presented the highest number of early neonatal deaths (37,919), whilst the Midwest region presented the lowest, with 7911 deaths, as exposed in Table 1. Concerning characteristics related to mothers, in all Brazilian regions, the age range with the highest occurrence was that between 15 and 19 years, which corresponds to 93,949 cases (92.5%), and the most frequent level of maternal schooling was four to seven years of education, with an absolute value of 37,210 (36.6%). However, the Southeast, South and Midwest regions demonstrated more registries of average maternal schooling of eight to 11 years of education, with 11,842 (42.1%), 4424 (41.7%) and 3028 (38.2%) mothers in this level of schooling, respectively.
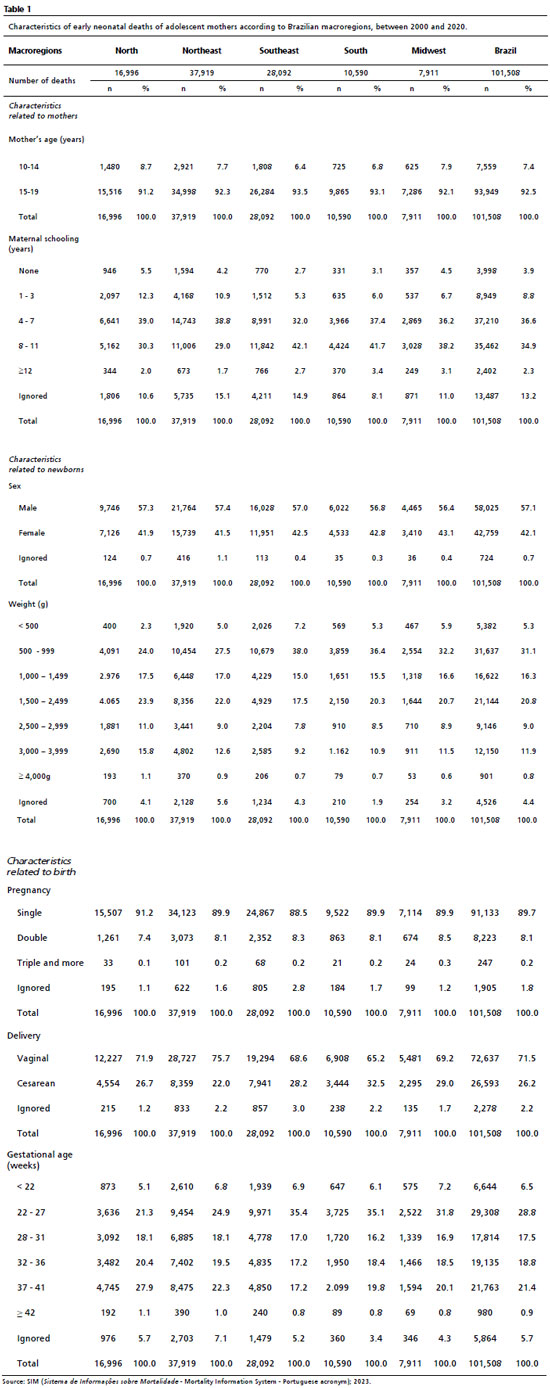
Regarding the characteristics related to newborns, all Brazilian regions demonstrated higher occurrences of the male sex, equivalent to 58,025 (57.1%) neonates. The most frequent birth weight in the national territory varied from 500 to 999 grams, in 31,637 (31.1%) cases, the category of lowest occurrence being that of 4000 grams on, with 901 (0.8%) registries (Table 1).
Concerning the characteristics related to birth, the single pregnancy was the most frequent in all Brazilian regions, comprising 91,133 cases (89.7%), as well as the vaginal way of delivery, with 72,637 (71.5%) registries. With regard to the gestational age, the range from 22 to 27 weeks demonstrated the highest number of registries in the national territory, with 29.308 (28.8%) deaths, except for the North region, where the range from 37 to 41 weeks presented higher occurrence of early neonatal deaths, revealing 4745 cases (27.9%) (Table 1).
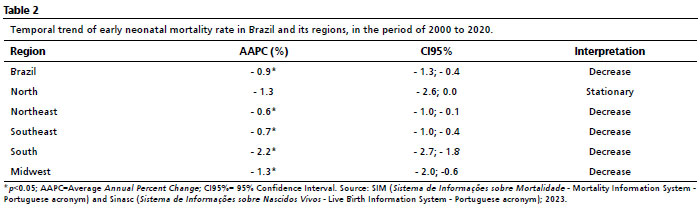
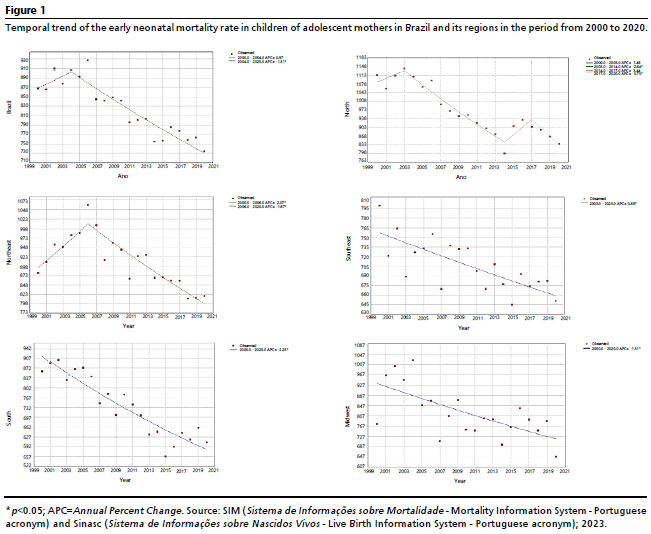
Regarding the temporal trend of the early neonatal mortality rate of adolescent mothers: the lowest early neonatal mortality rates of children of adolescent mothers occurred in the Southeast, followed by the South, Midwest, Northeast and North. The general temporal trend between 2000 and 2020 of the early neonatal mortality rate of children of adolescent mothers in Brazil demonstrated a decreasing standard (AAPC= -0.90;
p<0.001), as shown in Table 2. In the analysis of temporal segments (Figure 1), an inflection point was revealed, with predominating decrease between 2004 and 2020 (APC= -1.31;
p<0.001).
The only region that demonstrated a stationary general temporal trend between 2000 and 2020 was the North. The analysis by inflection points demonstrated three joinpoints and only the temporal segment between 2003 and 2014 was significant (APC= -2.64;
p<0.001). During all the studied period (2000 to 2020), the trend of early neonatal mortality within children of adolescent mothers was decreasing in the Northeast (AAPC = -0.60;
p<0.001). Nevertheless, in the analysis of temporal segments, we observed an increasing trend between 2000 and 2006 (APC = 2.07;
p=0.003) and decreasing trend between 2006 and 2020 (APC= -1.67;
p<0.001) (Figure 1).
The regions South, Southeast and Midwest, however, demonstrated a decreasing trend in all rates during the entire period studied (2000 to 2020). The highest decreasing trend was observed in the South of the country (AAPC= -2.34;
p<0.001), followed by the Midwest region (AAPC = -1.31;
p<0.001) and the Southeast region (AAPC = -0.69;
p<0.001) (Figure 1).
DiscussionThe present study described lower early neonatal mortality rates in the regions South and Southeast and higher rates in the North and Northeast regions. This disparity may suggest that, despite the significant advances, inequalities persist in the access and quality of care in the different regions of the country.
12,13,14 The differences in relation to economic development, financial incentives, employment offer, level of education and expansion of the healthcare network are aspects that influence these indicators.
15,16According to data from Ruschi
et al.,
17 in a study from 2018 carried out in the municipality of Vitória – Espírito Santo, only 13% of pregnant women received, in the period of assessment of the study, adequate care for the advanced level of prenatal, which considers the number of consultations, the onset of prenatal, procedures performed during the prenatal period and laboratory exams. Another study, with data from the National Survey of Health of 2013, indicated that women residing in the North region presented the lowest frequencies of adequate prenatal care, whilst the region Southeast presented the highest,
18 corroborating the regional inequalities registered in the present study. The variations of neonatal mortality coefficients are sensitive to the development conditions of the place in which the survey occurs. African countries, with low development levels, such as Ethiopia, present very high neonatal mortality coefficients (41.0 per 1,000 births). On the other hand, high-income countries possess rates of around 6.0 per 1000 births, according to data from 2017.
19In the present analysis, we found that 7.45% of pregnancies of adolescents occurred in the age range of ten to 14 years old. This rate was even higher in the North region, representing 8.71% of cases. The Law number 12.015/2009 establishes that having sexual intercourse with an individual with less than 14 years old is a sexual crime against vulnerable person, regardless of consent.
20 Reidy
et al.,
21 when analyzing prospectively the temporal relation between the experience of sexual violence and the occurrence of pregnancy, observed that, within the girls, being victim of sexual violence is associated with higher risk of pregnancy during adolescence. The combined sequels of sexual violence and pregnancy in adolescents impair the health and the social and economic development of victims.
In the period analyzed in this study, more than 80% of mothers presented less than 12 years of schooling. Fonseca
et al.,
22 when comparing neonatal mortality with the maternal level of schooling in the state of Rio de Janeiro between 2004 and 2010, found that the mortality rate decreased only for women with intermediate and advanced education. Kale
et al.,
23 when analyzing the evolution of fetal and neonatal mortality in Rio de Janeiro from 2000 to 2018, observed that the group of low schooling was the only to present high and crescent rates, evidencing social inequality in healthcare. Low schooling may compromise the acquisition and comprehension of important information concerning healthcare, particularly, during the prenatal period.
22 Population strategies, without the proper focus on more vulnerable groups, may paradoxically increase disparities; on the other hand, the combination of intersectoral activities, such as in the education area, and the social participation of the population itself are crucial to improve the mortality indicators.
24Adolescents that become pregnant are excessively exposed to complications related to pregnancy and challenge the psychosocial stress associated with pregnancy.
25 The early pregnancy is related to higher incidence of complication such as eclampsia, gestational hypertension, HELLP syndrome, puerperal infections and unnecessary intrapartum interventions.
26 Moreover, maternal age inferior to 19 years is described as being associated with newborns with low birth weight, preterm and small for gestational age.
27 All of these factors are related with a higher maternal and infant morbimortality.
25The present study demonstrated that the birth weight range that predominated in the early neonatal deaths was from 500 and 999 grams. In fact, birth weight is one of the most described risk factors in the literature for neonatal mortality.
23 Low birth weight may have, within its causes, prematurity and intrauterine growth restriction, indicators that reflect the quality of care provided to mothers during pregnancy.
28 Unfavorable socioeconomic conditions and flaws in the prenatal care may also be in the origin of low birth weight.
29The present analysis demonstrated a decreasing trend of the early neonatal mortality in almost the entire national territory, except for the North region, which presented a stationary trend. The observed decrease may be related to the implementation of strategies and assistance public policies, which resulted in the improvement of economic, educational, sanitary and health factors.
13As a limitation of the study, we highlight the use of secondary data in which the typing of deaths and births are performed in a decentralized manner, with potential inconsistencies and missing data. Studies based on secondary data have the disadvantage of the incompleteness of information that is essential for the research. However, the result of other epidemiological studies that used SIM and Sinasc reflects the death and birth profiles in Brazil and the large number of registries contributes to minimizing its possible flaws. Moreover, the present analysis did not consider fetal deaths, since the calculation of the early neonatal mortality rate used data from live births.
Lastly, we conclude that the North region presented the highest early neonatal mortality rate, whilst the Southeast region presented the lowest. All states presented a decreasing trend of the analyzed rate, except for the North region, which presented a stationary trend. The highest percent change was observed in the South of the country. The findings suggest the need for intersectoral public policies focused on the assistance offered to pregnant adolescents, mainly in the North and Northeast regions.
References1. Mann L, Bateson D, Black KI. Teenage pregnancy. Aust J Gen Pract. 2020 Jun; 49 (6): 310-6.
2. World Health Organization (WHO). Adolescent pregnancy. Geneva: WHO; 2018. [access in 2023 Set 21]. Available from:
http://www.who.int/mediacentre/factsheets/fs364/en/3. Akanbi MA, Ope BW, Adeloye DO, Amoo EO, Iruonagbe TC, Omojola O. Influence of socio-economic factors on prevalence of teenage pregnancy in Nigeria. African J Reprod Health. 2022, 25: 138-46.
4. Maheshwari MV, Khalid N, Patel PD, Alghareeb R, Hussain A. Maternal and Neonatal Outcomes of Adolescent Pregnancy: A Narrative Review. Cureus. 2022 Jun 14; 14 (6): e25921.
5. Govender D, Naidoo S, Taylor M. “I have to provide for another life emotionally, physically and financially”: understanding pregnancy, motherhood and the future aspirations of adolescent mothers in KwaZulu-Natal South, Africa. BMC Pregnancy Childbirth. 2020; 20 (1): 620.
6. Corcoran J. Teenage pregnancy and mental health. Societies. 2016; 6 (21): 1-9.
7. Eliner Y, Gulersen M, Kasar A, Lenchner E, Grünebaum A, Chervenak FA, Bornstein E. Maternal and Neonatal Complications in Teen Pregnancies: A Comprehensive Study of 661,062 Patients. J Adolescent Health. 2022; 70 (6): 922-7.
8. Paller L, Feldman F, Lauria W, Rey G. Obstetric and perinatal outcomes in teenage pregnancy: a literature review. Int J Fam Commun Med. 2021; 5 (1): 179-83.
9. Maheshwari MV, Khalid N, Patel PD, Alghareeb R, Hussain A. Maternal and Neonatal Outcomes of Adolescent Pregnancy: A Narrative Review. Cureus. 2022 Jun 14; 14 (6): e25921.
10. Ministério da Saúde (BR). Manual de Vigilância do Óbito Infantil e Fetal e do Comitê de Prevenção do Óbito Infantil e Fetal. Brasília (DF): Ministério da Saúde; 2009. [access in 2023 Set 21]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/manual_obito_infantil_fetal_2ed.pdf11. Migoto MT, Oliveira RP, Freire MHS. Análise da mortalidade perinatal e seus fatores associados. Rev Baiana Enferm. 2018; 32: e26249.
12. Prezotto KH, Oliveira RR, Pelloso SM, Fernandes CAM. Trend of preventable neonatal mortality in the States of Brazil. Rev Bras Saúde Matern Infant. 2021; 21 (1): 291-9.
13. Costa AÁ da S. Tendência da Taxa de Mortalidade Infantil no Brasil, de 2000 a 2019 [Internet]. repositorio.ufrn.br; 2023 [access in 2024 Jun 30]. Available from:
https://repositorio.ufrn.br/handle/123456789/51882.
14. Mallmann MB, Tomasi YT, Boing AF. Realização dos testes de triagem neonatal no Brasil: prevalências e desigualdades regionais e socioeconômicas. J Pediatr. 2020 Aug; 96: 487-94.
15. Malta DC, Prado RR, Saltarelli RM, Monteiro RA, Souza MF, Almeida MF. Óbitos evitáveis na infância, segundo ações do Sistema Único de Saúde, Brasil. Ver Bras Epidemiol. 2019; 22: e190014.
16. Prezotto KH, Bortolato-Major K, Moreira RC, Oliveira RR, Melo EC, Silva FRT. Mortalidade neonatal precoce e tardia: causas evitáveis e tendências nas regiões brasileiras. Acta Paul Enferm. 2023; 36: eAPE02322.
17. Ruschi GE, Zandonade E, Miranda AE, Antônio FF. Determinantes da qualidade do pré-natal na Atenção Primária à Saúde: o papel do Apoio Matricial na Saúde da Mulher. Cad Saúde Colet. 2018; 26 (2): 131-9.
18. Mario DN, Rigo L, Boclin KL, Malvestio LM, Anziliero D, Horta BL, et al. Qualidade da Assistência pré-natal no Brasil: Pesquisa Nacional de Saúde 2013. Ciên Saúde Colet. 2019; 24 (3): 1223-32.
19. Kamal R, Hudman J, McDermott D. What do we know about infant mortality in the U.S. and comparable countries? [Internet]. Peterson-Kaiser Health System Tracker; 2019. [access in 2023 Set 21]. Available from:
https://www.healthsystemtracker.org/chart-collection/infant-mortality-u-s-compare-countries/#item-perinatal-mortality-u-s-slightly-lower-comparable-countries20. Presidência da República (BR). Lei Federal n. 12.015, de 7 de agosto de 2009. Altera o Título VI da Parte Especial do Decreto-Lei no 2.848, de 7 de dezembro de 1940 - Código Penal, e o art. 1o da Lei no 8.072, de 25 de julho de 1990, que dispõe sobre os crimes hediondos, nos termos do inciso XLIII do art. 5o da Constituição Federal e revoga a Lei no 2.252, de 1o de julho de 1954, que trata de corrupção de menores [Internet]. Brasília (DF); 2009. [access in 2017 May 3]. Available from:
http://www.planalto.gov.br/ccivil_03/_Ato20072010/2009/Lei/L12015.htm21. Reidy DE, Bhochhibhoya S, Baumler ER, Peskin MF, Emery ST, Shegog R, et al. Sexual violence in early adolescence is associated with subsequent teen pregnancy and parenthood. Prev Med. 2023; 171: 107517.
22. Fonseca SC, Flores PVG, Camargo KR Jr, Pinheiro RS, Coeli CM. Maternal education and age: inequalities in neonatal death. Rev Saúde Pública. 2017; 51: 94.
23. Kale PL, Fonseca SC, Oliveira PWM, Brito AS. Fetal and infant mortality trends according to the avoidability of causes of death and maternal education. Rev Bras Epidemiol. 2021; 24 (1).
24. Ruiz JI, Nuhu K, McDaniel JT, Popoff F, Izcovich A, Criniti JM. Inequality as a powerful predictor of infant and maternal mortality around the world. PLoS One. 2015; 10 (10).
25. Lambonmung A, Acheampong CA, Langkulsen U. The Effects of Pregnancy: A Systematic Review of Adolescent Pregnancy in Ghana, Liberia, and Nigeria. Int J Environ Res Public Health. 2022; 20 (1): 605.
26. Trombetta TC, Bentes TK, Silva NL, Queiroz YS, Lira Neto JCG, Ferreira BO. Identificação das condições maternas e fatores de risco da gravidez na adolescência: uma revisão integrativa. Res Soc Dev. 2022; 11(6): e47311629498.
27. Fall CH, Sachdev HS, Osmond C, Restrepo-Mendez MC, Victora C, Martorell R, et al. Association between maternal age at childbirth and child and adult outcomes in the offspring: a prospective study in five low-income and middle-income countries (COHORTS collaboration). Lancet Global Health. 2015; 3 (7): e366-77.
28. Gaiva MPM, Fujimori E, Sato APS. Fatores de risco maternos e infantis associados à mortalidade neonatal. Enferm. 2016; 25 (4): e2290015.
29. Buriol VCS, Hirakata V, Goldani MZ, Silva CH. Temporal evolution of the risk factors associated with low birth weight rates in Brazilian capitals (1996-2011). Popul Health Metr. 2016; 14 (1): 15.
Authors’ contributionCarvalho JMS and Quintiliano JAC: conceptualization and study design, literature review and elaboration of the manuscript. Santos CBM: conceptualization and study design, literature review, data analysis and interpretation and elaboration of the manuscript. Carmo DC and Bonfim LAM: literature review, data acquisition and elaboration of the manuscript. Nogueira MP: intellectual review of the manuscript and final approval of the version submitted to the journal. All authors approve the final version of the manuscript and declare no conflicts of interest.
Received on October 27, 2023
Final version presented on August 25, 2024
Approved on August 30, 2024
Associated Editor: Pricila Mullachery


 ; Claudia Bispo Martins Santos 2
; Claudia Bispo Martins Santos 2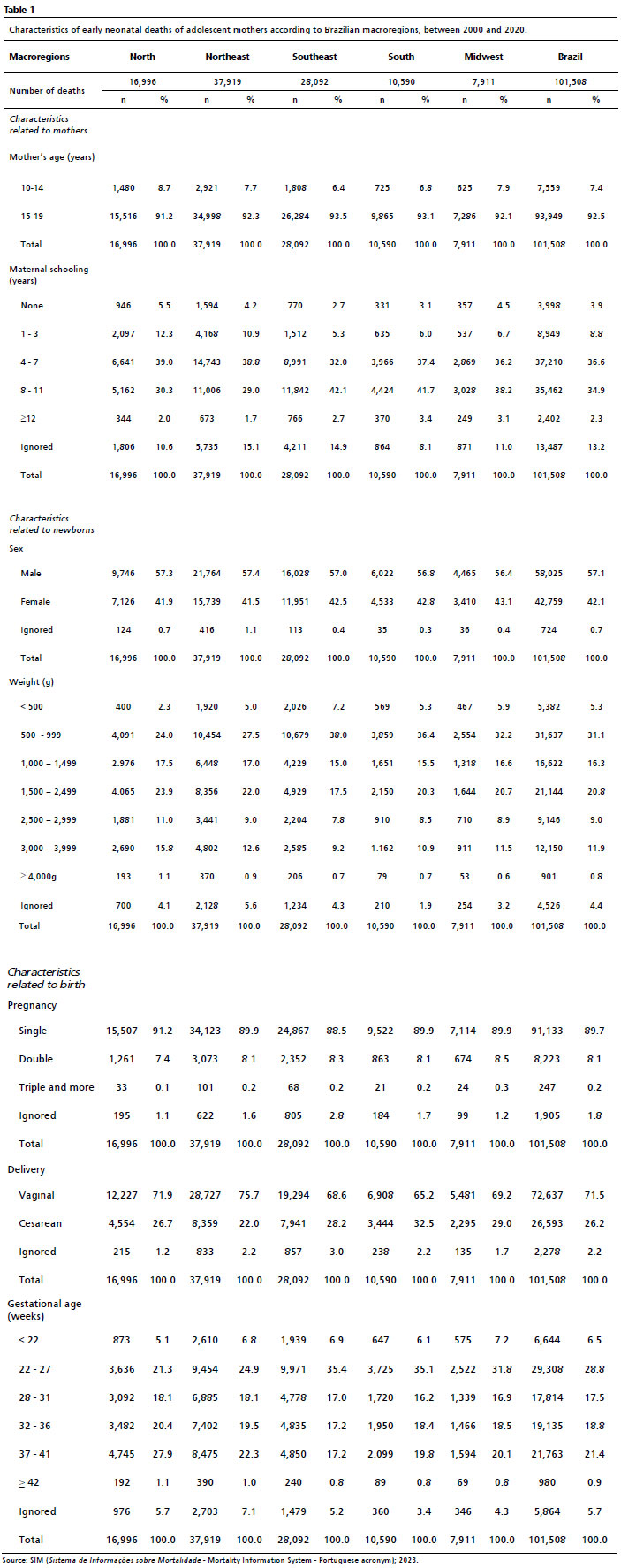






 Ler em português
Ler em português